Your voice where it matters most in NHS & care services Our draft strategy 2017 2020
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Your voice where it matters most in NHS & care services
Our draft strategy 2017 - 2020
We’re listening to shape,
influence and improve services
in Suffolk
Published June 2017 Published March 2017
www.healthwatchsuffolk.co.uk
www.healthwatchsuffolk.co.uk
P1
Contents
01 P3
P3
Introduction
What is Healthwatch Suffolk?
... Our responsibilities
P4 What do we hope to achieve?
... Our vision and values
02 P6
P6
Our governance
How are we governed?
03
P8 The team
P8 Who delivers our services?
P9 Staff structure
04
P10 Finance
P10 How are we funded?
05
P11 Our core work
P11 The national landscape
P15 The Health and Wellbeing Board
... Our stakeholder survey 2016
06
P18 Our priorities
P18 Local Healthwatch priorities (National)
P20 Our strategic priorities
If you require this document in an alternative format please contact
Healthwatch Suffolk on 01449 703949 or by email to
info@healthwatchsuffolk.co.uk.
P2
01 Introduction
What is Healthwatch Suffolk? We aim to amplify the voice of patients,
service users and the public, as an
We have been operating as a Community independent consumer champion for
Interest Company and Social Enterprise health and social care in Suffolk. Our 2015-
since April 2013. Local healthwatch 16 Annual Report captures much of what
provision was created in 2013 as part we do and aim to achieve on behalf of
of widespread changes to the way in and with the people of Suffolk.
which care is organised in England. The
obligations of a local healthwatch are set We are responsible for gathering the
out in the Regulations subsequent to the views of the people of Suffolk regarding
Health & Social Care Act 2012. the health and social care they receive.
Click to find out more... Watch a video
Look out for these icons
throughout this document. Click Web content
them for more details about our
work and how we can make a Document download
difference.
We then bring such views to the attention service, thereby giving advice to people
of commissioners and providers of health looking for a health or social care
and social care and have statutory powers service to meet their needs. We are also
to hold them to account. responsible for the requirements placed
upon us by the 2012 Act and to exercise
Suffolk has three Clinical Commissioning such powers as we have been granted
Groups (CCGs) with responsibility for under that Act.
commissioning health services. The
responsibility for commissioning social Our powers are that:
care lies with Suffolk County Council.
• We can ask providers for
What are our responsibilities? information which they must make
available to us.
We are responsible to Suffolk County • We can make recommendations to a
Council for realising the requirements of local provider and they are required
the specification which they have agreed to tell us within 20 days what action
with us. As a part of that agreement we are they intend to take or why they
responsible for providing a signposting intend not to take any action.
P3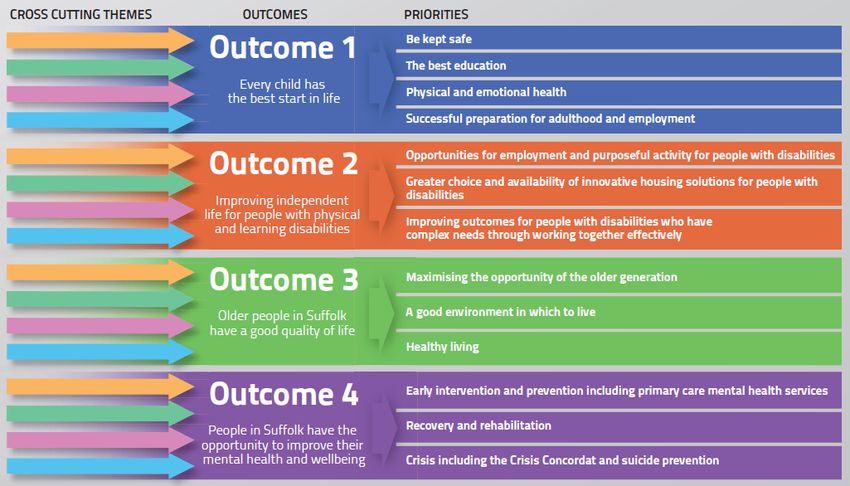
• We have the power to report on Details of outcomes achieved to-date can
health or social care matters to the be found in our outcomes document
local Health Overview and Scrutiny 2013-2016, an online document that we
Committee. They are required to will update roughly every 6 months (see
have regard to any information we additional content on page 5). Page 3
have sent them.
What is our vision? Page 6
• We have the power to Enter and
View providers of publicly funded
Our vision, or purpose, is to: Page 8
health or social care services. Apart
from where they concern social
Page 18to
“Champion the views of local people
care for people under 18 years of
age (these are the responsibility of achieve excellent health and social care
services in Suffolk”. Page 20
OFSTED).
• We can refer matters to the Pagewe
In order to accomplish our vision, 24will:
Care Quality Commission or to
Healthwatch England if it is a matter • Aim to be representativePage
of the36
local
that can best be dealt with on a community we serve;
national level. Page 48
• Engage with health and social care
What high level outcomes do we aspire commissioners, service providers
Page 50
to help bring about? and communities when changes
to service provision are planned or
a. Health and social care services public health issues addressed;
shaped to meet people’s needs and • Engage and represent the
are improved as a result of their community we serve with
experience. particular emphasis on seldom
b. Local people confident in the heard groups;
validity and transparency of health • Commit to collaborate and
and social care bodies’ decision work in partnership with other
making. organisations to ensure maximum
c. Suffolk citizens knowing about, added value, and to avoid
understanding and empowered duplicating each other’s work; and
to access health and wellbeing • Actively listen to the public’s
services that meet their needs. concerns, highlight poor service
d. Local people knowing of and what is working well.
Healthwatch Suffolk and its role,
trusting and respecting it as a What are our values?
credible local champion, making
a difference to services and the We Listen and we are Inclusive;
health and wellbeing of the people Transparent; Accessible; Accountable;
of Suffolk. Responsive; and Proactive.
These are described in more detail
e. Services readily accessible to within Appendix C, Communications &
Suffolk citizens, through wide Engagement Strategy 2016-2019.
ranging and appropriate avenues
and opportunities that comply with
all relevant disability and equality
legislation.
P4
Additional content
What is Healthwatch Suffolk? Our outcomes document
About us
Our Annual Report 2015/16
We are always striving to find new ways to engage people and obtain views about
local services. This includes the launch of new social media platforms, the continued
development of our online Feedback Centre (rate and review) and expanding our
networks to reach local communities.
In 2016/17, we used these networks to talk to people about important issues and
ensured that local views are heard as part of ongoing work to make our local services
sustainable for the future.
Find out more...
www.healthwatchsuffolk.co.uk
P5
02 Our governance
How are we governed? We also support two sub-groups, which
report to our Board of Directors. These
Healthwatch Suffolk is a social enterprise are:
operating as a Community Interest
Company and as such is governed by a • Mental Health Focus Group; and
Board of Directors. The Board oversees • Black and Minority Ethnic (BME)
the strategic and operational activities and Diversity Focus Group
of the Company, including the delivery
of the requirements of Suffolk County Our BME and Diversity sub-group is one
Council’s service specification. The Board of the most productive means through
is also responsible to the membership which we are able to engage diverse
of Healthwatch Suffolk and is led by the communities in Suffolk. It is a forum
Chair of Healthwatch Suffolk, who is also for sharing information, networking,
our representative on the Suffolk Health and gathering feedback from different
& Wellbeing Board. Board documents are communities about local health and care
available online. services.
We conducted a Director recruitment A range of voluntary organisations are
campaign between August and members as well as statutory partners
November 2016, having consulted both including acute hospitals, clinical
staff and members as part of the process. commissioning groups and the mental
health trust. The Group has taken the
Our third Annual General Meeting time to review its Terms of Reference,
(AGM) took place on October 27th 2016. aims and purpose in 2016. The revised
Healthwatch Suffolk AGMs are intended Terms will shape its work for the next
to ensure that a proper representation of couple of years.
our activities is provided to Members. We
currently have two levels of membership Our Mental Health Focus Group
(Friends and Members). Only Members continues to attract a good mix of senior
have voting rights within the organisation. health and social care professionals,
As of January 2017 we will be looking to people who use mental health services,
invite our Friends to become Members, carers and support organisations. It
prior to closing the Friends classification. facilitates a dialogue between mental
health professionals and service users/
Streamlining our governance structure in carers as a means to bring about change
2015/16 saw our Board take the decision in the way mental health services are
to close what was the Operational provided. This Group has also reviewed
Delivery Group. The Group had been its Terms of Reference and agreed
essential at the time that Healthwatch priorities for 2016-17.
Suffolk was being formed and had
fulfilled its role.
P6
We bring people together to shape and improve local health
and social care services.
Additional content
Videos filmed at our last AGM About membership
Meet the Board
A summary of our last AGM
P7
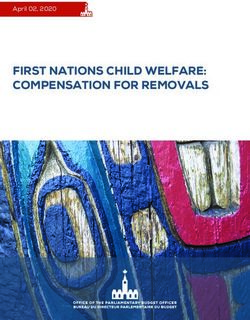
03 The team
Operations Manager
(Amanda Stevens)
Fina
(Yvo
Who delivers our services?
We have a Team of dedicated and
talented individuals who are all
passionate about the work and aims of a Business Development Officer
local Healthwatch. (Simon King)
The Team of roughly 11 FTE (full time
equivalent) staff are also supported by
about 80 committed and knowledgeable
volunteers and together offer broad and Administrator
accessible services; the quality of which (Kevin Marsh)
is enhanced because of our approach
to collaborate and work in partnership
whenever possible.
For details on what our Team and
volunteers do please see our 2016-17
Annual Report. Our Communication &
Engagement Strategy details what our
Team does. The latter is available on
request. As a reference, the chart right
identifies the Staff Structure as of July
2016.
P8
Chief Executive
(Andy Yacoub)
ance Officer Information Services Senior Community
onne Hall) Manager Development Officer
(Michael Ogden) (Gill Jones)
Research and Development Community Development
Officer Officer
(Sarah Jull) (Elizabeth Storer)
Research and Development Community Development
Officer Officer
(Tom Delaney) (Kerry Overton)
Community Development
Information Services Officer
Officer
(Jenny Ward)
(Dan Pennock)
Mentor
Apprentice
Additional content
Our Annual Report 2015/16
Our Communications and engagement strategy
P9
04 Finance
Health and Social Care Act 2012, Section In addition to the funds agreed with
182 placed a duty on local authorities Suffolk County Council, Healthwatch
such as Suffolk County Council to make Suffolk will also endeavour to earn
contractual arrangements with a Local income which will be reinvested
Healthwatch for the involvement of local into local healthwatch projects and
people in the commissioning, monitoring, work programmes. We are therefore
provision and scrutiny of health and introducing a Business Development Plan
social care services. and have in 2016 already begun to create
and benefit from new income streams.
Suffolk County Council is also duty
bound to ensure that adequate
resources are provided to Healthwatch
Suffolk, following Department of
Health guidelines and other key local
decision makers (e.g. the Health and
Wellbeing Board). Healthwatch Suffolk
demonstrates delivery of services
using the principles of value for money;
those being economy, efficiency and
effectiveness.
We were established by an act of
Parliament in 2012, which means a
Local Healthwatch must be funded by
law in every area of England.
P1005 Our core work
Our primary role is to gather experiences 2. Health & Social Care Information and
and views and build an evidence base Access: We will continue to provide
that we can use to help inform health and advice and information about access
social care service improvement. Prior to to local health and care services so
Healthwatch Suffolk CIC’s incorporation choices can be made about how,
and following wide consultation, Suffolk where and when those services are
County Council developed and agreed accessed. Key themes are;
with us strategic outcomes (see page 3) to
support the achievement of our vision. • Signposting & Information
services in general and on the
Nine strategic objectives were identified; Care Act specifically
our core work. We have a detailed • Raising awareness of local
Communications & Engagement healthwatch
Strategy 2016-2019 (Appendix C) that
describes how it is we deliver this core • Suffolk Information Standard
work. We also believe that it is important
to communicate the difference we 3. Research & Analysis: Provides
make and we do this partly through our direction for our activity and will
Key outcomes of our work 2013-2016 continue to use national and local
publication (Appendix D), a document we intelligence/data to inform activity.
update roughly once every 6 months. Key themes are;
The nine strategic objectives are: • Research projects which meet
our priorities
1. Community Engagement: We will • Commissioned projects
continue to develop individual and
community relationships, promoting 4. Stakeholder Relationship
and supporting the involvement Management: Ensures the voice of
of local people and listening to local people is heard and that their
individual stories. Key themes are; views influence service provision. Key
themes are;
• Children & Young People
• BME Communities County wide • Enter & View
• Enter & View • 20 day response requests
• Vulnerable Groups – including • Escalation
homeless, looked after children • Partnership strategy e.g. private
& veterans sector & Congress/voluntary &
community sector
• Commissioner relations and
influence
P11• Full membership engagement 9. Financial Management & Revenue
Generation: Key themes are;
5. Statutory Power & Influence: Key
themes are; • Prudent management of our
finances
• Healthwatch England • Continuing to seek
• Suffolk Health & Wellbeing commissioned work
Board • Investigate both grant funding
• Care Quality Commission and contract work
• Health Scrutiny & Overview
Committee How are we and our local health and
care system influenced by the national
6. Marketing & Promotion of and local landscape?
Healthwatch Suffolk: Key themes are;
Both NHS and social care budgets are
• Communication & Engagement under pressure nationally. Demand for
Strategy such services continues to increase at a
rate that outstrips investment into them,
• Enhancing the Healthwatch much of which is due to the combination
Suffolk “Brand” of an ageing population whose life
• Raising our profile locally, with expectancy is rising sharply, and
commissioners/providers, the advancements in medical care leading
public and with Healthwatch to a wider range of medical interventions
England being available. NHS England issued its
Five Year Forward View in order to try
7. People & Volunteer Management: Key and address this situation.
themes are;
This national Forward View will, in
• The provision of training essence, aim to do the following:
necessary for their roles
• Bring about a radical upgrade in
• Role descriptions as required
prevention and public health;
• Support and guidance
• When people need health services,
patients will gain far greater control
8. Systems & Information Management:
of their own care;
Key themes are;
• The NHS will take steps to break
• Continued development of our down the barriers in how care is
signposting role provided between family doctors
and hospitals, between physical and
• Updating our Feedback centre
mental health and between health
• Source hardware suitable to our and social care;
needs
• Local health communities will be
• Obtain software to meet our supported by the NHS’ national
growing ambitions e.g. advanced leadership to choose from amongst
statistical software and Adobe a small number of new care delivery
In-design options;
P12• Across the NHS, urgent and more awareness of their increasing
emergency care services will be emotional wellbeing and mental health
redesigned to better integrate needs, while cardiovascular and stroke
between A&E departments, GP remain the major causes of premature
out-of-hours services, urgent care death. The Clinical Commissioning
centres, NHS 111, and ambulance Groups monitor health statistics and also
services. the performance of the system, such as
Delayed Transfers of care from hospitals.
These priorities are now being rolled out
across the NHS through the Sustainability National and local expectations of a local
and Transformation Plans (STPs). healthwatch are therefore extremely
Healthwatch Suffolk is concerned with wide ranging, with virtually every aspect
two of the 44 STPs: of publicly or part publicly funded health
and social care in scope. In our formative
• North East Essex, West & East years as Healthwatch Suffolk we have
Suffolk, locally named “Local Plan attempted to address most of the issues
for Health & Care”; and and concerns that have either been
• Norfolk & Waveney, locally named raised with us, by service users/patients/
“In Good Health”. carers/professionals, or by us through
our own fact finding and analysis. Such
Healthwatch Suffolk is mindful of the an approach was deemed important at a
strategic importance of these Plans, time when we were a new organisation;
which rightly involve other sectors this coincided with our efforts to establish
such as social care and housing, and is ourselves as an independent watchdog
therefore prioritising every opportunity and in marketing/publicising the services
to be engaged in the process of we provide.
developing them. We are doing so from
the perspective of an independent In preparation for the introduction of a
voice, amongst what are otherwise three year strategy we have taken several
commissioners and the larger providers steps in order to be as well informed as
of health and care services. We are possible, before setting out the objectives,
working alongside and in collaboration priorities and the outcomes we aspire to
with Healthwatch Essex and Healthwatch achieve.
Norfolk.
Information considered will be sourced
There is extensive information about from the following:
the health and the health needs of local
people that is already known through 1. Statutory requirements of a Local
for example the Joint Strategic Needs Healthwatch (Care Act 2012);
Assessment (JSNA) and other sources 2. Suffolk County Council service
of published intelligence and data. The specifications attributed to
growing numbers of older people locally Healthwatch Suffolk;
and nationally mean the numbers 3. Healthwatch Suffolk Annual Report
of people living with long term and 2015-16;
increasingly complex conditions is rising.
There are also rises in the numbers of 4. Suffolk Health & Wellbeing Strategy
young people with learning difficulties, 2016-19 refresh;
P135. Healthwatch Suffolk combined skills and competencies;
Communication and Engagement 10. Healthwatch Suffolk Stakeholder
Strategy; Insight Survey 2016, incorporating
6. National Healthwatch trends and the views of both non-professional
themes that are relevant to Suffolk; and professional stakeholders;
7. Sustainability & Transformation 11. Healthwatch Suffolk Annual
Plans; [financial] Accounts 2015-16 and
8. Outcomes of Healthwatch forecasts for 2016-17. Suffolk County
Suffolk’s use of business analysis Council has to-date set the funding
and self-reflection tools, namely of its Local Healthwatch on a year-
a SWOT (Strengths Weaknesses to-year basis; and
Opportunities Threats) and 12. Healthwatch Suffolk Risk Register
PESTLE (Political Economic 2016.
Sociological Technological Legal
Environmental);
9. A recognition of developments and
continued investment in the Team’s
Additional content
The Suffolk and North East Essex STP
In Good Health: Norfolk and Waveney STP
The Suffolk Information Standard
Suffolk Information Standard video
Healthwatch England
Our Feedback Centre
Our Annual Report 2015/16
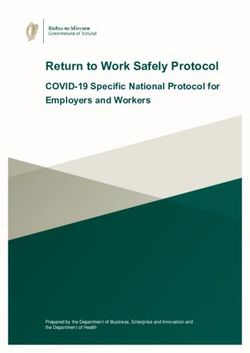
P14What principle outcomes are being sought by Suffolk’s Health & Wellbeing Board?
All four outcomes are relevant to the work of a local healthwatch, as are the cross-
cutting themes of stronger/resilient communities, embedding prevention, addressing
inequalities, and health and care integration. The graphic below has been exported
from the Suffolk Health & Wellbeing Strategy 2016-19
What did our stakeholder Insight Survey bodies involved in health and care. Most
2016 tell us? importantly, we wish to do all we can to
deliver on our commitments, and the
We are by our very nature a listening consumer value they offer, for the people
organisation. We therefore continuously of Suffolk.
invite stakeholders, both organisations
and members of the public alike, to It is a challenging time for the health and
offer views, observations, experiences, social care, and for those who rely on
comments, compliments and complaints us, but by working together towards a
to help us to use our variety of resources shared future we see an opportunity for
efficiently. Healthwatch Suffolk to promote the voice
of the public and improve health and
The Stakeholder Insight Survey is about social care services for all. Our survey
looking to the future i.e. to ensure that reflected the following:
we are evolving in line with the views
of the public and other stakeholders. By • Almost three-quarters of
stakeholders we include patients, service respondents agreed or strongly
users and carers, alongside health and agreed that the work of Healthwatch
care professionals within commissioning Suffolk is based on the views and
and provision organisations, and of experiences of local people.
course voluntary & community sector
P15• Over two-thirds of health and • Almost 9 in 10 respondents agreed
social care professionals agreed or or strongly agreed that Healthwatch
strongly agreed that Healthwatch Suffolk makes it clear that people
Suffolk builds collaborative can be involved in several ways.
relationships with key local decision
makers. Our stakeholder survey plans will be
• Three-quarters of respondents expanded from 2017, incorporating
agreed or strongly agreed that further Healthwatch Suffolk member
Healthwatch Suffolk challenges key engagement, and use of an increasingly
health and care decision makers, if beneficial relationship with voluntary
they are not listening to local people and community sector organisations.
or if care isn’t working the way it We will naturally continue to use every
should. media opportunity to raise awareness of
our work.
• 6 in 10 of respondents agreed or
strongly agreed that Healthwatch
Suffolk has a clear approach to
reaching all communities and
involving them in its work.
Additional content
Healthy Suffolk (Health and Wellbeing Board Information)
P16This page is intentionally blank
If you require this document in an alternative format please contact
Healthwatch Suffolk on 01449 703949 or by email to
info@healthwatchsuffolk.co.uk.
P1706 Our priorities
Why do we need strategic priorities? one for the second year running whilst
social care rises up the list, with particular
April 1st 2017 will be our 4th anniversary. focus on care in people’s homes.
We are now an established and reputable
independent health and social care The full list of top five priorities nationally
watchdog, with an ever-growing portfolio are as follows (expressed by the number
of positive outcomes (see Appendix D). of local healthwatch that have raised each
Our core work is still wide ranging but we theme):
now need to prioritise our efforts and the
prudent use of our limited resources. 1. Mental Health - including mental
health services for children and
What are the views of patients, service young people (101 local healthwatch)
users and carers, as represented by local 2. Social care – including care homes
healthwatch nationally? and services provided in peoples’
homes (78 local healthwatch)
Analysis by Healthwatch England in
December 2016, this being an annual 3. Primary care – including GP services
survey involving all local healthwatch, (51 local healthwatch)
identified the key issues the public 4. Children and young people’s
want to see policy makers and health experiences of health and social
professionals focus on over the next 12 care (42 local healthwatch)
months. Mental health remains at number
This section is all about
our priorities. Please read
it and let us know if you
agree with our choices...
P185. The experiences of seldom heard of concerns heard by local Healthwatch
groups, including black & minority include people not knowing which
ethnic (BME) communities carer would visit them or at what time,
communities (23 local healthwatch) leaving them feeling vulnerable, and care
workers feeling rushed and without the
Access to, and the quality of, mental right information, which meant they had
health services topped the list last year insufficient knowledge of service user
and retains the top spot, with two thirds needs.
of the Healthwatch network reporting
that their communities want it to be a According to Healthwatch England,
core focus for improvement. Rising to “Spending time in the community
second on 2017’s priority list is social care, visiting users of these services, as well as
with almost half of local Healthwatch working with carers, local Healthwatch
picking up on concerns, including are uniquely placed to gather and share
questions around the quality of some intelligence about people’s experiences
local care homes and issues concerning and ensure concerns are addressed”.
access for some care home residents to
other health services, like NHS dentistry. The fifth most common local
healthwatch priority (seldom heard
Digging deeper into the rise of social groups such as black & minority ethnic
care, Healthwatch England found that communities) is now a core area of work
concerns around care services delivered at Healthwatch Suffolk, ostensibly led
in people’s homes, such as help with via our BME & Diversity Focus Group.
washing, dressing and support to take Marginalised and vulnerable people are
medication, contributed significantly included within the scope of this Focus
with 1 in 5 local Healthwatch now citing Group. The top four national priorities
domiciliary care as a priority, double the are in fact all reflected in the Healthwatch
number who raised it last year. The sorts Suffolk priorities we are proposing.
Are you onboard?
For them to be effective, our priorities must
be shaped by you. We need to know whether
the things we have chosen are the most important areas for you and your
community. Visit
www.surveymonkey.com/r/HWSStrategy or call 01449 703949
This survey will close on 30th April 2017.
After this, it is still possible to have your say on our work by becoming a member or
volunteer. Alternatively, you can leave feedback about local services. We will use it to
guide our activity and make choices about how we can improve local care.
Visit: www.healthwatchsuffolk.co.uk/services
P19Our strategic priorities
What are our proposed strategic These priorities are to our mind all
priorities? interconnected to some degree and
would be reviewed on an annual basis.
We have used our knowledge of national
and local trends, data and research,
alongside what people have been telling
us over the past three years, in order to
identify six proposed strategic priorities
for the period 2017-20.
Table A (see Appendix E) lists the sources
of information that influence our choice
of priorities; namely the strategies, legal
requirements, plans, surveys, local
intelligence, reports and the previously
mentioned national priorities.
Our ongoing commitment to the
aforementioned Sustainability and
Transformation Plan processs, as the local
independent health and care advisor, will
be informed by our core work and that
concerning our strategic priorities.
Mental health and wellbeing:
In identifying mental health and emotional wellbeing as a
Suffolk priority, we have, in addition to the Healthwatch England
survey, taken into account two other key reasons. Parity of
esteem is a critical national issue that clearly impacts on the
local workforce, volunteers and in particular the experiences
of service users, patients and carers. We are also mindful of
the fact that the mental health trust delivering services in
Suffolk is rated as requiring improvement by CQC. Healthwatch
Suffolk continues to press for a co-production approach to the
development, monitoring, implementation and reviewing of the
mental health strategy, along the lines of learning disability co-
production in Suffolk.
P20Children and young people:
In identifying services related to children and young
people with a particular interest in emotional wellbeing (e.g.
EWB2020), we have, in addition to the Healthwatch England
survey, taken into account two other key reasons. The voice
of children and young people is seldom heard in consistent
and in large numbers, whilst the shortcomings of Suffolk
services such as those relating to Special Educational Needs
have also recently been highlighted by a joint Ofsted and CQC
report.
Primary care:
Primary Care is the first point of contact for health care
for most people. It is mainly provided by GPs (general
practitioners) who handle 90% of NHS patient contact. Other
primary care services include community pharmacists,
opticians, dentists, midwives, health visitors and a variety of
allied health professionals such as physiotherapists.
Changes to GP services are becoming the norm because of
increased demand, recruitment challenges and financial
pressures. For these reasons alone, and in recognition of the
national outlook, primary care is considered a priority by us.
Social care (care homes/domiciliary care)
Social care is the second most prevalent priority for the network.
We use our power of Enter of View to address some home
care matters, whilst also recognising good practice when it is
brought to our notice. We do however struggle to reach service
users of home based care, and we are also aware of the impact
of diminishing resources that for example lead to delayed or
unqualified assessments of service users. This is a challenge
that is faced by almost every local Healthwatch and is therefore
considered a priority for us until we discover more about the
experiences of these vulnerable and often isolated service users.
P21Co-Production
Co-production was first conceptualised by an academic team
at Indiana University in the 1970s and described the lack of
recognition of service users in service delivery. In the UK during
the 1980s, the then director of health policy at the King’s Fund,
introduced the concept of co-production as a way to understand
the relationship between clinicians and patients in health
services. At Healthwatch Suffolk we believe that Co-Production
(or Co-Design) should at times be considered as the best option
for engaging and consulting service users, patients and carers.
It does however require a significant cultural shift on the part
of commissioners and the agencies they represent, alongside a
commitment to and from the service users, patients and carers
involved.
Suffolk’s Learning Disability Strategy and Implementation Plan
remains the most prominent and true current co-production
example, where change is sought, maintained, monitored and
reviewed from a collective standpoint and from the earliest
possible stage. The term co-production is also too often used to
describe approaches that are actually about consultation and
engagement, which are in themselves sound ways of gaging the
views of the public. These are the reasons why Healthwatch
Suffolk has prioritised work on the subject of co-production.
What was the consultation process for A three year implementation plan that
our Strategy? will deliver against our core work and that
of our priorities will be published later in
We consulted our stakeholders over the 2017.
period February to April 2017. In doing so,
we fine-tuned our commitments to the
population of Suffolk for the period 2017-
20.
The key amendment made concerned
our proposed strategic priorities was that
our original six priorities were reduced
to five, because we were advised that
Sustainability and Transformation
Plans actually cover a wide range of
subject matters, already addressed by
our commitments to core work and the
remaining five priorities.
P22Find out more...
www.healthwatchsuffolk.co.uk
P23Appendix A:
SWOT Analysis of Healthwatch Suffolk (revised December 2016)
Strengths Weaknesses
• Backed by Health and Social • Over reliance on a single
Care Act 2012 source of funding
• Cross party support both • The sheer size of the health
Nationally and Locally and social care brings
• Increased statutory functions challenges to prioritisation
over LINk • Growing number of calls to
• Reasonable level of funding signposting with ever more
• Increasingly well integrated complex cases
with local health and social care • Need for more Directors and
organisations greater diversity
• Able to refer to the Care Quality
Commission and Healthwatch
England
• Public accountability
• Communications team now
reach over 130,000 households
of Suffolk
• Credible research and reporting
Opportunities Threats
• Potential for increasing income • Political change as a result of
generation elections to Government –
• Need to engage with other local this could lead to changes in
healthwatch to share learning legislation and funding
• Greater partnership/ • Greater call on signposting as
collaboration with other a result of the Care Act, and
agencies e.g. Voluntary & service integration
Community Sector • Many of the public not clear
• Partnerships/collaboration with about our role and call on
statutory stakeholders us for health care not just
• Increasing involvement in signposting
contracting and selection
activities with partners
• Potential engagement with MPs
and Councillors
• Improving credibility with the
public and stakeholders
P244.
Appendix B:
PESTLE analysis of Healthwatch Suffolk (completed January 2016)
Factor Key influences Team
rating
Political Suffolk County Council (SCC) i.e. commissioning changes, 22
relationship and finance
Health & Wellbeing Board 9
National policy influencing Healthwatch England 9
Economic Diversification i.e. due to more expected of Healthwatch for less 20
Working smarter because of potential cuts in public expenditure 20
Social Reliance on health & social care integration (neighbourhood teams 15
and networks)
Challenging providers and commissioners 14
Ensuring Healthwatch services are accessible to all communities 10
Technological Information sharing between organisations 24
Data security sharing/confidentiality 9
Intellectual property 7
Application of technology to Healthwatch processes 7
Legal Implications of Care Act on signposting, engagement and SCC com- 21
missioning priorities
Growing integration of health & social care e.g. Suffolk Connect and 9
funding to follow service users
Gaining research approval via partnerships with hospitals, SCC and 8
academic establishments
Environmental Rurality of Suffolk i.e. isolation, lack of service reach, transport, cost 19
of travel, fuel poverty & employment
Office environment i.e. facilities, lighting and policies/procedures 18
Working from home i.e. benefits, drawbacks and cost 14
P25Appendix C
We have presented how our choice of priorities is influenced in a simple matrix table
(see overleaf). This matrix does not include an exhaustive list of strategic influences
and so we naturally also pay a great deal of attention to ‘live’ sources of information
emanating from our own diverse list of Members, service user and carer forums, the
Care Quality Commission, nearby local healthwatch colleagues, health and care com-
missioners and local providers.
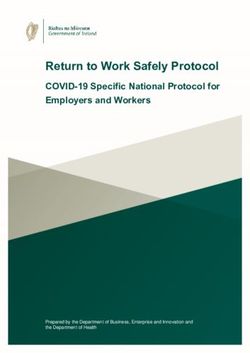
Table A; Rationale behind proposed strategic priorities; presented as a matrix
Strategic influence Mental Children Primary Social care Co-
health and and young care production
emotional people
wellbeing
Care act x x x x
Service specs x x x x x
HWS annual report x x x x x
Suffolk H&WB strategy x x x x
HWS C&E strategy x x x x x
National LHW priorities ‘16 x x x x
STPs x x x x
HWS Team skillset x x x x x
HWS survey 2016 x x x x x
HWS finances
HWS risk register Limits what HWS can take on, deliver & achieve
Index: HWS (Healthwatch Suffolk); H&WB (Health & Wellbeing Board); LHW (local
healthwatch); CDO (Community Development Officers)
P26Getting in touch
The Healthwatch Suffolk office is locted in Claydon (Mid Suffolk). You can contact us
8.30am until 5pm (Monday to Friday). Emails, letters and voice messages will be
responded to as soon as possible (generally within 24 to 48 hours).
Address Freepost RTTY-CEUT-LCRH
Healthwatch Suffolk
Unit 14, Hill View Business Park
Old Ipswich Road
Claydon
Ipswich
IP6 0AJ
Telephone 01449 703949 / 08004488234 (Freephone for Signposting Ser-
vice)
Email info@healthwatchsuffolk.co.uk
Website www.healthwatchsuffolk.co.uk
Twitter @HWSuffolk
Facebook www.facebook.com/HealthwatchSuffolk
To share views on our priorities...
Visit www.surveymonkey.com/r/HWSStrategy or call 01449 703949
This survey will close on 30th April 2017. After this, it is still possible to have your
say on our work by becoming a member or volunteer. Alternatively, you can leave
feedback about local services. We will use it to guide our activity and make choices
about how we can improve local care.
Visit: www.healthwatchsuffolk.co.uk/services
P27This document is available to download Healthwatch Suffolk uses the
from the Healthwatch Suffolk website. It Healthwatch Trademark (which covers
has been made available to the bodies the logo and Healthwatch brand) when
responsible for arranging and delivering undertaking work on our statutory
diabetic care services and anyone that activities as covered by the licence
may be interested in our organisation. agreement.
Report layout and infographics created
by the Healthwatch Suffolk Information
Team. For a free design quotation please
contact 01449 703949.
@HWSuffolk - Follow Healthwatch Suffolk
If you require this document in an alternative format please contact
Healthwatch Suffolk on 01449 703949 or by email to
info@healthwatchsuffolk.co.uk.
P28You can also read