What every board member needs to know about improvement and quality assurance - A report from the Good Governance Institute and Perfect Ward
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Good
Governance
Institute
What every board member needs
to know about improvement and
quality assurance
A report from the Good Governance Institute and Perfect Ward
September 2021
What every board member needs to know about improvement and quality assurance
Document name: What every board member needs to know about improvement and quality assurance
Date published: September 2021
Author/s: Chris Smith, Consultant, GGI
Will Grayson,Junior Consultant, GGI
Laura Botea, Director of Corporate Affairs, GGI
Stephen McCulloch, Director of Communications, GGI
Reviewed by: Darren Grayson,Executive Director and Partner, GGI
Joe Roberts,Consultant, GGI
In collaboration with: Perfect Ward
ISBN: 978-1-907610-70-7
This document has been prepared by GGI Development and Research LLP © [2021] GGI Development and Research LLP
Good Governance Institute, (Company number 590301 Registered in the Republic of Ireland) Registered office: The Black Church St. Mary’s Place Dublin 7 D07
P4AX Republic of Ireland; GGI Limited (Company number: 06836117 Registered in England and Wales) Registered Office: Old Horsmans, New Road, Sedle-
scombe, Battle, East Sussex, TN33 0RL, UK; GGI Development and Research LLP (Company number C384196 Registered in England and Wales) Registered
Office: Old Horsmans, New Road, Sedlescombe, Battle, East Sussex, TN33 0RL, UK
For more information contact:
contact@good-governance.org.uk
www.good-governance.org.uk
2
What every board member needs to know about improvement and quality assurance
Executive Summary
What every board member needs to know The report reflects on this important
about improvement and quality assurance development and examines how changes
is a report intended to guide and support to the healthcare environment will impact
boards in developing and maintaining future arrangements.
robust quality assurance and improvement
processes within their organisations. Finally, it explores the acknowledged
enablers and barriers to effective quality
It contains a maturity matrix, a practical tool assurance. The aim is to demonstrate the
to support boards in assessing levels of breadth of factors that can impact quality
maturity within their organisations against assurance, and support board members
key identified criteria and identifying the in identifying which barriers they need to
steps they need to take to progress the tackle and which enablers they need to
maturity of their organisations. The report promote.
also provides best practice examples and
key questions to help boards translate For further information or support in using
theory into practice. the report and associated maturity matrix,
please contact GGI at contact@good-
The report covers key definitions, governance.org.uk or Perfect Ward at
governance principles, roles and info@perfectward.com.
responsibilities (including the role of
regulators and other stakeholders) in
relation to quality assurance and quality
improvement.
Healthcare services around the world
are increasingly adopting integrated
approaches to the delivery of care.
3Good
Governance
What every board member needs to know about improvement and quality assurance Institute
Good Governance Institute Perfect Ward
GGI exists to help create a fairer, better At Perfect Ward, we apply the best digital
world. Our part in this is to support those technology to solve one of healthcare’s most
who run the organisations that will affect important challenges – how to continuously
how humanity uses resources, cares for the improve quality.
sick, educates future generations, develops
our professionals, creates wealth, nurtures Our aim is to bring the mobile user
sporting excellence, inspires through the experience we all know and love on our own
arts, communicates the news, ensures all phones, to the healthcare industry; a sector
have decent homes, transports people and long underserved by technology, and reliant
goods, administers justice and the law, on manual, paper-based processes.
designs and introduces new technologies,
produces and sells the food we eat – in We created our app to empower all health
short, all aspects of being human. and care professionals to do their quality
inspections more quickly and with greater
We work to make sure that organisations accuracy via easy-to-use technology. By
are run by the most talented, skilled and using Perfect Ward quality inspections are
ethical leaders possible and work to fair completed up to 60% quicker, freeing up
systems that consider all, use evidence, time to care and providing instant access to
are guided by ethics and thereby take the critical quality data for our customers.
best decisions. Good governance of all
organisations, from the smallest charity
to the greatest public institution, benefits
society as a whole. It enables organisations www.perfectward.com
to play their part in building a sustainable,
better future for all.
www.good-governance.org.uk
4What every board member needs to know about improvement and quality assurance
1. Introduction
The NHS arguably has one overarching It is equally important that board members
purpose: to provide comprehensive, high and senior managers understand key
quality and universal health care services to principles of quality assurance and
the people of the UK1. improvement and are equipped to apply
these to their decision-making processes.
Boards are fundamental to achieving this
purpose. It is they who set the strategic Given this, and to help board members
direction of the institutions and systems navigate these challenges, Perfect Ward
they lead, and who will need to find and the Good Governance Institute
realistic and practical solutions to the many have partnered on a new programme of
challenges that health and social care work focusing on quality assurance and
providers face, both in the short and longer improvement in health and social care.
term.
This research paper is the first output from
Within this, the value of good governance that programme. It aims to explore some of
should not be underestimated. Indeed, we the key concepts of quality assurance and
know all too well from high-profile incidents improvement and provide best practice
that when governance fails it can quickly examples and tools to support boards to
lead to patient safety issues. translate theory into practice. The report
has been informed by interviews and a
This is why it is so important that roundtable involving senior figures from the
organisations that provide healthcare have health and social care sector.
robust quality assurance and improvement
mechanisms. When implemented We would like to thank everybody who
effectively, these inform and support contributed to this paper, especially the
frontline staff to deliver high-quality and members of the editorial board and those
sustainable care, and managers to make we interviewed. The full list of contributors
more intelligent and effective decisions2. can be found in the appendix.
1
The NHS Constitution for England (updated 1 January 2021): https://www.gov.uk/government/publications/the-nhs-constitution-for-england/
the-nhs-constitution-for-england 5
2
Anna Dixon, Catherine Foot, Tony Harrison, Preparing for the Francis Report, The King’s Fund, 2012 https://www.kingsfund.org.uk/sites/default/
files/field/field_publication_file/preparing-for-the-francis-report-jul2012.pdfWhat every board member needs to know about improvement and quality assurance
2. Context
Health and social care systems across the world collaboratives and place-based governance who have worked commendably throughout,
are grappling with a range of similar problems, arrangements. All of this will have implications to the brink6. The impact on quality of care
including staff recruitment and retention on how care is delivered and assured, with new is hard to quantify but certainly poses a
challenges, developing more integrated care layers of governance required. significant near-term risk to many organisations
systems, achieving financial sustainability, in the sector.
and, of course, ensuring that health and care Other parts of the UK are arguably somewhat
services are accessible and high-quality. further along on the integration journey4. For many NHS organisations, the pandemic
Scotland legislated for integrated care in 2014, represented a period when governance was
In the UK, and in England in particular, health bringing health and social care under the rightly relaxed in order to release precious time
and social care is in a period of considerable management of 31 integrated authorities. Also and capacity to the Covid response. During
change. Ever since the publication of the Five in 2014, Wales introduced integrated health this period, we have seen committees deemed
Year Forward View in 2015, we have seen and social care partnerships consisting of local to be less essential stood down, regulatory
the gradual rolling back of legislation that government, NHS, third and independent intervention significantly reduced, and many
emphasises competition as the main driver sectors, and carer representatives. Whereas services put on hold7. It demonstrated what
of improving quality of care and financial across Northern Ireland there are 17 integrated was possible, particularly with regard to
sustainability, in favour of that which prioritises care partnerships that bring networks of service digital transformation, with increases in virtual
integration, collaboration and partnership. providers together to provide more joined up consultations and remote working.
This has culminated in the recent publication care for local populations.
of NHS England’s Integrated Care Systems: Now, as we come out of the worst of the
Design framework, which sets out how NHS At the same time as we are seeing widespread pandemic, health and social care providers
leaders and organisations will operate with system-level changes introduced and have a rare opportunity to recast quality
their partners in integrated care systems (ICSs) embedded, health and care organisations governance within their organisations. In
from April 20223. These changes will result around the world have also been responding doing so, it will be important that the learning
in the dissolution of clinical commissioning to what has been called an ‘unprecedented from the previous 18 months is embedded
groups as ICSs are formally created around the challenge’ in the COVID-19 pandemic5. This and, where appropriate, paused activities
country, as well as the introduction of provider has pushed many organisations and their staff, reintroduced.
3
NHS, Integrated Care Systems: design framework, version 1, June 2021 https://www.england.nhs.uk/wp-content/uploads/2021/06/B0642-ics-design-framework-june-2021.pdf
4
GGI, Growing pains: integrated care lessons from Scotland and Wales, Illumination series, March 2021 https://www.good-governance.org.uk/publications/insights/growing-pains-integrated-care-lessons-from-scotland-and-wales
5
Ham, C (2020). The challenges facing the NHS in England in 2021
6
GGI, Practical solutions for managing NHS system burnout, Illumination series, April 2021 https://www.good-governance.org.uk/publications/insights/practical-solutions-for-managing-nhs-system-burnout 6
7
GGI, Purposeful quality committees, Illumination series, June 2021, https://www.good-governance.org.uk/publications/insights/purposeful-quality-committeesWhat every board member needs to know about improvement and quality assurance
3. The current state of play
This section will cover what quality assurance out the key principles of quality assurance. In Quality assurance, then, which relates
and quality improvement actually mean and 2001, the Academy of Management voted to the “processes for defining, assuring,
entail, as well as their roles in healthcare this the most influential management book maintaining and improving quality”, is
systems domestically and across the world. of the 20th century. essential to ensuring boards fulfil this duty10.
Implemented effectively, quality assurance
3.1 What is quality assurance The premise of quality assurance is that work should also increase the transparency,
can be codified as a series of instructions relevance and value of information that
and standards. organisations disclose to their market and
Quality assurance is the function of their stakeholders.
setting standards for things, measuring Within this, it is important that organisations,
whether the standards are met and what including board members, understand 3.2 What is quality improvement (QI)
the variation is and trying to iron out the extent of their responsibilities for the
unwarranted variation, principally.” provision of safe and effective care.
It is a mistake, I think, to see QI as the next
– a chief executive at our roundtable In the UK, public and private providers of step on from QA. They’re symbiotic things.
health and social care are subject to the same You need both. I wouldn’t want to have a
The IHI describes six dimensions of quality tests and standards including a duty of quality. blood transfusion that wasn’t very heavily
that must be in place for the delivery of quality assured. I wouldn’t want to set up
high-quality healthcare: safety, effectiveness, “The board has a key role in safeguarding a community outreach service if I hadn’t
patient-centredness, timeliness, efficiency, quality, and therefore needs to give empowered the staff to be perpetually
and equity8. It is up to boards, managers, appropriate scrutiny to the three key facets improving or changing. It’s that.”
and ultimately all staff to ensure that these of quality – effectiveness, patient safety and
dimensions are in place with health and patient experience. – a chief executive at our roundtable
social care organisations through a process
of quality management. Effective scrutiny relies primarily on the ‘Quality improvement’ in healthcare is the
provision of clear, comprehensible summary framework used to systematically improve
The major force behind quality management information to the board, set out for the ways care is delivered to patients,
was Frank Winslow Taylor, whose 1911 book everyone to see, for example, in the form of using characteristics that can be measured,
The Principles of Scientific Management set quality accounts9.” analysed, improved and controlled.
8
IHI, How Can We Define “Quality” in Health Care?, http://www.ihi.org/education/IHIOpenSchool/resources/Pages/Activities/DefiningQualityAimingforaBetterHealthCareSystem.aspx 7
9
NHS, The Healthy NHS Board: Principles for Good Governance https://www.leadershipacademy.nhs.uk/wp-content/uploads/2012/11/NHSLeadership-TheHealthyNHSBoard.pdf
10
Dixon A, Foot C, & Harrison T, Preparing for the Francis report: How to assure quality in the NHSWhat every board member needs to know about improvement and quality assurance
Quality improvement arose in the 1920s It involves continuous efforts to achieve At the second level are boards who retain
through pioneers such as Juran and Deming stable and predictable results, in essence, ultimate accountability for the quality of
at the Hawthorne Works in Cicero, Illinois. It to reduce process variation and improve care within their institutions. And at the third
is underpinned by the belief that those with the outcomes of these processes both for level are external bodies such as regulatory
the best knowledge of how to improve work patients and the healthcare organisation organisations which are typically responsible
efficiency are those that are actually doing it: and the system it works in12. for assuring the public about the quality of
the teams at the sharp end. care they should expect to receive16.
3.3 Reassurance versus assurance
In healthcare we see this pioneered
through the Institute of Healthcare In governance, great emphasis is placed
Improvement (IHM), for example, with on distinguishing between reassurance
techniques such as LEAN or the ‘Plan-Do- (when someone tells you that all is well) and
Check-Act’ (PDCA) cycle11: assurance (telling you what’s happening
and showing you the evidence so that you
can judge for yourself if all is well), and
boards must be careful to ensure that they
strike the right balance between the two13.
This will allow boards to not be overrun by
statistics and also ensure that they are not
solely reliant on what the executives say is
happening. Those working at each level have a
fundamental role to play in ensuring
In healthcare, it is frequently argued that that healthcare services are safe and
there are ‘three lines of assurance’ or effective. However, this paper is principally
‘three lines of defence’ when it comes concerned with the second level of
to quality1415. At the first level are the assurance: boards and the systems and
healthcare professionals responsible for the processes which support their effective
delivery of patient care. functioning.
11
ASQ, What is the plan-do-check-act (PDCA) cycle? https://asq.org/quality-resources/pdca-cycle
12
Agency for Healthcare Research and Quality, Practice Facilitation Handbook https://www.ahrq.gov/ncepcr/tools/pf-handbook/mod4.htm
13
GGI, Assurance, Reassurance and Performance, Illumination series, May 2021 https://www.good-governance.org.uk/publications/insights/assurance-reassurance-and-performance
14
Agency for Healthcare Research and Quality, Practice Facilitation Handbook https://www.ahrq.gov/ncepcr/tools/pf-handbook/mod4.html 8
15
NHS Providers, Board assurance: a toolkit for health sector organisations
16
Dixon A, Foot C, & Harrison T, Preparing for the Francis report: How to assure quality in the NHSWhat every board member needs to know about improvement and quality assurance
GGI has previously written about how the escalating any areas of concern through the • The board becomes a driving force for
best boards continually question their organisation. A key principle must be that only continuous quality improvement across
own governance17. This includes how the areas of greatest concern are escalated the full range of services.
information is presented and utilised within to the executive, with less concerning issues • Boards are also required to endorse
board and committee meetings to ensure dealt with at the appropriate level. This and sign off declarations of assurance
that board member time and expertise is ensures proper accountability. to regulators in relation to quality,
most effectively utilised. and comply with the registration
3.4 Specific responsibilities of requirements of the quality regulator.20
But how much assurance is the right amount? healthcare organisations
And how can boards truly be confident about with regards to quality of care On the other hand, ensuring accountability
the quality of services being provided?18 in relation to quality is facilitated by more
NHS boards have a statutory duty of quality. than regular scrutiny of information on
It is our view that, at a time when many of In support of this, the Leadership Academy quality, however exemplary it may be.
our colleagues are concerned with capacity suggests the following to exhibit good Research suggests that governance of
and staff health and wellbeing, we should practice: quality can be improved if board members
be wary of returning to the assurance routinely step outside the boardroom to
industry that has historically existed within • All board members need to understand gain first-hand knowledge of the staff and
the management structures of most health their ultimate accountability for quality. patient experience. It is important to ensure
and social care providers – and which is • There is a clear organisational structure that clinical leaders are properly empowered
resource-intensive and often confused with that clarifies responsibility for delivering to lead on issues relating to clinical quality,
good governance. quality performance from the board to as boards benefit from regular opportunities
the point of care and back to the board. both to take advice from clinical leaders and
To resolve this, it is important that boards • Quality is a core part of main board to reflect on innovative practice in relation to
put in place the right systems and processes meetings, both as a standing agenda quality improvement21.
to support staff to report and manage item and an integrated element of all
quality19. This includes the implementation major discussions and decisions. 3.5 Regulation and stakeholders
of digital solutions to help mechanise • Quality performance is discussed in more
assurance process as well as appropriate detail regularly by a quality committee A high-performing quality assurance
escalation routes, with staff at the front with a stable, regularly attending framework helps ensure that healthcare
line dealing with the day-to-day issues, but membership. organisations perform at an optimal level.
17
GGI, The basics of good governance, Illumination series, May 2021, https://www.good-governance.org.uk/publications/insights/the-basics-of-good-governance
GGI, Assurance, Reassurance and Performance, Illumination series, May 2021 https://www.good-governance.org.uk/publications/insights/assurance-reassurance-and-performance
9
18
19
GGI, Purposeful quality committees, Illumination series, June 2021 https://www.good-governance.org.uk/publications/insights/purposeful-quality-committees
20
NHS, The Healthy NHS Board: Principles for Good Governance https://www.leadershipacademy.nhs.uk/wp-content/uploads/2012/11/NHSLeadership-TheHealthyNHSBoard.pdf
21
IbidWhat every board member needs to know about improvement and quality assurance
Without it, managers would have a less clear can override their decisions. • Australian Institute of Health and
view of how patients are being treated while • The General Medical Council – Welfare
under their care, staff performance levels, responsible for registering doctors when • Council for Health Service
and outcomes for both patients and the they enter the profession, for making Accreditation of Southern Africa
organisation. The demonstration of a robust arrangements for dealing with poorly
quality assurance framework and evidence performing doctors, and, currently, 3.6 Regulatory requirements for
of quality improvement are staples among for introducing a five-yearly system of quality
the expectations of regulatory bodies in revalidation.
the health and social care sector. Failure to • The Nursing and Midwifery Council Under Regulation 12 of the CQC’s
meet these demands is likely to result in – responsible for registering nurses, Guidance for Providers, the following are
dire consequences for any organisation and nursing associates and midwives when listed as essential in terms of providing safe
could warrant further investigation. they enter the profession and for care treatment:
dealing with poorly performing nurses
Many organisations in the UK are involved and midwives. a. assessing the risks to the health and
with quality assurance, the King’s Fund lists, • Health and Care Professions Council safety of service users of receiving the
among others: – responsible for regulating 15 health care or treatment;
and care professions such as dieticians, b. doing all that is reasonably practicable
• The Care Quality Commission – clinical scientists and paramedics in the to mitigate any such risks;
responsible for licensing all providers of UK. c. ensuring that persons providing care
health and social care. It has the power • General Dental Council – the UK-wide or treatment to service users have the
to close services down if they are below statutory regulators of the dental team. qualifications, competence, skills and
standard. experience to do so safely;
• The National Institute for Health and Internationally, the following organisations d. ensuring that the premises used by the
Clinical Excellence – its main function play a role: service provider are safe to use for their
in the present context is to produce intended purpose and are used in a safe
clinical guidelines. It has been charged • Institute for Healthcare Improvement way;
with defining quality standards for the (IHI) e. ensuring that the equipment used by
treatment of a wide range of conditions. • International Society for Quality in the service provider for providing care
• The Commission for Healthcare Health Care (ISQua) or treatment to a service user is safe for
Regulatory Excellence – responsible such use and used in a safe way;
for overseeing all the professional As well as other country-specific bodies f. ensuring the proper and safe
regulators. It reports annually on their such as: management of medicines;
performance and in some circumstances • Health Quality Ontario g. assessing the risk of, and preventing, 10What every board member needs to know about improvement and quality assurance
detecting and controlling the spread • if there is a robust overview of the care report incidents
of, infections, including those that are that is being provided22. b. involves the workforce and consumers in
healthcare associated; the review of incidents
In a similar fashion, the Australian c. uses the information from the analysis of
The quality assurance system within an Commission on Safety and Quality in Health incidents to improve safety and quality
organisation should ensure that such Care stipulate requirements that include: d. regularly reviews and acts to improve the
standards are monitored and maintained. effectiveness of the incident management
• That health service organisation uses and investigation systems.24
However, failure to meet these standards organisation-wide quality improvement
is likely to warrant further action from the systems that: • That health service organisations:
CQC upon inspection, either in the form
of a demand for improvement or direct a. identify safety and quality measures, and a. have processes to seek regular feedback
intervention. monitor and report performance and from patients, carers and families about
outcomes their experiences and outcomes of care
The CQC is likely to check: b. identify areas for improvement in safety b. have processes to regularly seek
and quality feedback from the workforce on their
• if policies are relevant, up-to-date and c. implement and monitor safety and quality understanding and use of the safety and
accessible improvement strategies quality systems
• if operations are patient-centred d. involve consumers and the workforce c. use this information to improve safety
• risk assessments in the review of safety and quality and quality systems.25
• staff satisfaction surveys performance and system23.
• if important documents are stored in a
safe and secure place • That health service organisation has
• documented evidence of improvement organisation-wide incident management
• improvement action plans and investigation systems, and:
• culture
• ISO accreditation a. supports the workforce to recognise and
22
Citation, Quality assurance and good governance: how to be outstanding https://www.citation.co.uk/news/care/quality-assurance-good-governance-outstanding/
23
Australian Commission on Safety and Quality in Healthcare, Patient safety and quality systems, Action 108 https://www.safetyandquality.gov.au/standards/nsqhs-standards/clinical-governance-standard/
patient-safety-and-quality-systems/action-108
24
Australian Commission on Safety and Quality in Healthcare, Patient safety and quality systems, Action 111 https://www.safetyandquality.gov.au/standards/nsqhs-standards/clinical-governance-standard/
patient-safety-and-quality-systems/action-111
Australian Commission on Safety and Quality in Healthcare, Patient safety and quality systems, Action 113 https://www.safetyandquality.gov.au/standards/nsqhs-standards/clinical-governance-standard/
11
25
patient-safety-and-quality-systems/action-113What every board member needs to know about improvement and quality assurance
It is important to mention that within the 2. Practices for Improving Quality and
independent sector, regulatory requirements Safety: making quality and safety of
deemed fit for national health systems may care a priority of the board’s business
not translate well to independent healthcare 3. Partnerships for Improving Quality
providers. Nuffield Health had the following and Safety: developing strong
to say on the matter: collaborative partnerships with staff,
service users and the wider community
“The progress has not always been easy, as 4. Methods for Improving Quality and
much of the existing best practice guidance Safety: support the provider in applying
relates to NHS services and does not a quality improvement methodology
necessarily translate across to the situation 5. Measurement for Improving Quality
in the independent sector. And initially it and Safety: selecting board measures
took time to work with CQC to ensure they to monitor and demonstrate an
understood exactly how our services were improvement in the delivery of care.
configured.”26 6. Risk Management and Assurance:
ensure that all risks to service user
Beyond regulatory matters, management quality and safety are addressed in a
also needs to be able to demonstrate robust and structured way.
a sound understanding of quality 7. Planning for Improving Quality and
assurance systems from the top down. Safety: championing and overseeing
HealthMangagement.org has outlined the development, implementation and
seven leading practices in relation to the monitoring of a plan for improving
board and its role in regards to quality quality and safety.27
assurance:
1. Leadership for Improving Quality
and Safety: actively demonstrating a
commitment to seeking assurance and
driving improvement.
26
Nuffield Health, Working with the Care Quality Commission, 2018, https://www.nuffieldhealth.com/article/working-with-the-care-quality-
commission-cqc 12
27
HealthManagement, Volume 18 Issue 2, Quality and Safety: The Role of The Board, 2018, https://healthmanagement.org/c/healthmanage-
ment/issuearticle/quality-and-safety-the-role-of-the-boardWhat every board member needs to know about improvement and quality assurance
4. Changes to the healthcare environment and the impact on quality assurance and improvement
As highlighted earlier in this report, The Framework also makes plain that Further afield, Australia’s long-term health
health care services around the world from their establishment in April 2022, plan sets out the vision for the country over
are increasingly adopting integrated ICSs will be expected to have specific the next 10 years. It focuses on developing
approaches to the delivery of care. responsibilities for delivering safe and high- a system that is more integrated, efficient,
quality services.28 In particular, the ICS NHS focused on patients, and equitable. Six
In the UK, health and social care in England body will be the accountable body for the integrated care programmes and initiatives
is currently going through a period of realisation of this, underpinned by effective have been developed that focus on
fundamental change. This will result in the governance and strong local leadership.29 improving population outcomes:
introduction of ICSs, provider collaboratives
and other place-based arrangements which In tandem, other home and international • Planned Care for Better Health
will, at least in the short term, complicate countries are seeing a similar focus on • ED to Community
quality governance and assurance. more joined-up and integrated care. For • Residential Aged Care
example, since the passing of the 2014 • Paediatrics Network
The recently published Integrated Care Public Bodies (Joint Working) (Scotland) • Specialist Outreach to Primary Care
Systems: Design Framework, consolidates Act, Scotland has required local authorities • Vulnerable Families.31
NHSEI’s thinking around ICSs and and health boards to work together to plan
particularly focuses on the governance of and deliver adult community health and Similarly, in Canada, provinces such as
these new bodies. It proposes a two-board social care services, including services for Ontario have piloted a range of integrated
model consisting of: older people.30 care initiatives such as integrated funding
models (IFMs) that required collaboration
• ICS NHS body, which is comprised of Integration Joint Boards have been and coordination across acute and post-
NHS organisations and is responsible for introduced to facilitate this process, acute care sectors. These are reported
the day-to-day running of the ICS commissioning health and care services for to have had a positive impact on care
• ICS Partnership Body that brings specific regions and consisting of councillors, coordination across healthcare settings.32
together a wider array of stakeholders NHS NEDs, non-voting NHS professionals,
including social care and public health the third sector and service users. Those we spoke to broadly agreed with
the move towards integrated care systems
28
GGI, ICS oversight - good governance arrangements will be key, Illumination series, July 2021 https://www.good-governance.org.uk/publications/insights/ics-oversight-good-governance-arrangements-will-be-key
29
GGI, ICS design: good governance will be key, Illumination series, June 2021, https://www.good-governance.org.uk/publications/insights/ics-design-good-governance-will-be-key
30
GGI, Growing pains: integrated care lessons from Scotland and Wales, Illumination series, March 2021 https://www.good-governance.org.uk/publications/insights/growing-pains-integrated-care-lessons-from-scotland-
and-wales 13
31
NSW Government, Australia’s Long-Term Health Plan, 2019, https://www.health.nsw.gov.au/integratedcare/Pages/australias-long-term-health-plan.aspx
32
Gayathri Embuldeniya, Jennifer Gutberg, Walter P.Wodchis, The reimagination of sustainable integrated care in Ontario, Canada, January 2021, https://www.sciencedirect.com/science/article/pii/S0168851020302736What every board member needs to know about improvement and quality assurance
and the opportunities that this presented In speaking to colleagues from around the is the principle of subsidiarity.33 This is the
for improving quality. This includes improved world, several highlighted the importance concept that decisions and accountability
relationships and coordinated care across of the following in ensuring that health and are best delivered with the greatest impact
areas, opportunities for sharing and learning social care integration programmes have a as close to the front line in a system or
from best practice, staff movement, and more positive impact on quality and safety: organisation as possible.
standardised and aligned measurement.
• clear lines of responsibility and It is an approach that has long been adopted
Despite this, some of those we spoke to in accountability between organisations, in the EU, which has a formal principle
preparing this report suggested that some underpinned by robust joint governance of subsidiarity in policymaking, and is
lingering issues persist. In England this (see below on the principle of subsidiarity) increasingly gaining traction in the NHS.34 For
includes: • strong relationships and mutual trust example, the Health and Social Care Select
between organisations and individuals Committee has argued that systems:
• concerns that ICSs will be too acute • consistent and clear reporting around
focused with historical issues remaining quality across organisations …should be encouraged to adopt a principle
around parity of esteem for mental health • a transparent and open culture which of subsidiarity in which decisions are made at
trusts and others around the system supports staff and organisations to the most appropriate local level.”35
including adult social care services learn from their mistakes coupled with
• the risk that new arrangements will add mechanisms to share this learning across The principle of subsidiarity particularly
layers of bureaucracy and governance and systems. makes sense with regards to quality
increase duplication assurance and improvement which require
• the need for regulation will need to adapt 4.1 The principle of subsidiarity the impetus and initiative of front-line staff
as ICSs and place-based arrangements to work effectively. It requires organisations
increasingly come into being. to clarify those quality incidents that require
To embed innovation, you need to give escalating to board level and those that can
Some of these issues will be addressed staff permission to try and come up with and should be resolved at the front line or as
through the introduction of clearer their own solutions” close to it as possible.
governance and accountability as ICSs are
brought into being on a statutory footing. – a chief executive at our roundtable It also requires greater levels of trust from
However, strong leadership will also be leadership teams and accountability among
required if quality of care is not to be Key to clearer and more effective governance staff teams, as well as engagement across
impacted during the transition. across ICSs and place-based arrangements sectors and services.
33
GGI, Place in integrated care: the noble aim of subsidiarity, Illumination series, July 2021 https://www.good-governance.org.uk/publications/insights/place-in-integrated-care-the-noble-aim-of-subsidiarity 14
34
The Strategy Unit, What could NHS policy makers learn from the European Union? 2019 https://www.strategyunitwm.nhs.uk/news/what-can-nhs-learn-eu
35
www.parliament.uk, Health and Social Care Select Committee, 2018, https://publications.parliament.uk/pa/cm201719/cmselect/cmhealth/650/65017.htmWhat every board member needs to know about improvement and quality assurance
High quality and real-time data and
electronic decision-making tools can
support this principle in health and social
care settings by giving staff the tools to
identify and resolve potential quality issues
as they are developing.
Health and social care boards should
ask themselves the following questions
with regard to quality assurance and
subsidiarity36:
• Where does quality assurance currently
sit in our organisation? Does this
support the principle of subsidiarity?
• How does technology and data
support decision-making across our
organisation?
• Does the leadership team champion
data?
• Do staff understand data as a decision-
making tool to improve organisational
culture or as something which is used
punitively?
15
36
GGI, People in Place, 2021, p.15What every board member needs to know about improvement and quality assurance
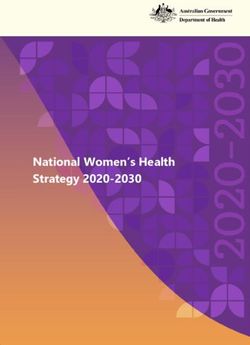
Essential characteristics of subsidiarity
Support
Clear vision • More senior staff taking responsibility for the providing
• A clear shared vision that is understood at all levels within resources and training necessary for lower levels to
an organisation or system discharge their functions
• More senior staff providing opportunities for learning
Trust and growth when mistakes are made and not reverting to
• Genuine trust and commitment from all levels to all the centralised approaches if errors occur
principles of subsidiarity and a respective appreciation of
the functions exercised at various levels Power
• The principle of subsidiarity means giving real power to
Culture lower groups for them to work towards shared aims
• All levels of the organisation are not only respected but • Senior groups should not prevent or absorb any
also required to assume responsibility and accountability responsibilities that can be discharged by a lower level
for whatever they are able to do on their own initiative
• Application on subsidiarity based on the context and Circumstances
circumstances of a particular capacity, decision or place • Subsidiarity needs to be applied in each case through
• Autonomy to work towards shared objectives consideration of all relevant circumstances or a particular
• Flexibility to move capacity down levels if those below place or decision, meaning the way it is applied in practice
could perform certain functions may differ widely from one situation to another
Initiative Data transfers
• Employees and less senior groups must assume • These approaches need to be supported by effective
responsibility and accountability for doing whatever they transfers of information from one level to the next, allowing
can on their own, by taking the initiative and developing senior levels to support where necessary and to create
an entrepreneurial spirit open communication across various levels to cultivate trust
• The scope, limit and reach of each individual, team or and strong relationships
service’s sphere of influence is recognised
16What every board member needs to know about improvement and quality assurance
4.2 Regulation joint inspections of some services since
2013.41 Whilst in Wales, The Healthcare
The future of regulation is less clear. We Inspectorate Wales and Care Inspectorate
have already highlighted how regulation is Wales have conducted joint inspections of
a key element of quality assurance. care for people with learning disabilities
and community mental health teams.42
NHS Providers has recently raised concerns
from its members that ‘the existing Interviewees were clear that regulatory
regulatory frameworks do not sufficiently changes must support quality improvement
reflect the context in which they are now and assurance initiatives not stifle them. In
providing care or their organisation’s order to do this, it has been suggested that
contribution to the wider health care the following will be key:
system.’37
• not creating additional regulatory
Indeed, the CQC has acknowledged that its burdens for individual organisations
regulatory framework will need to change through system and regulatory
and has experimented with place-based accountability
reviews and a new well-led framework.3839 • focusing on quality improvement rather
NHSE has also highlighted how it expects than punitive interventions
the system oversight to work with ICS NHS • ensuring greater transparency around
Body responsible for local oversight and methods and reporting
assurance.40 • not adopting a one-size fits all
approach.43
This is an approach that has been followed
in the other home nations for some time.
For example, in Scotland, Healthcare
Improvement Scotland and the Care
Inspectorate have been conducting
37
NHS Providers, NHS regulation: a shifting focus, 2019 https://nhsproviders.org/news-blogs/blogs/nhs-regulation-a-shifting-focus
38
Care Quality Commission, An update on CQC’s regulatory approach, 2021 https://www.cqc.org.uk/news/stories/update-cqcs-regulatory-approach
39
Care Quality Commission, Our reviews of local health and social care systems, 2019 https://www.cqc.org.uk/local-systems-review
40
NHS, Integrated Care Systems : design framework, June 2021 https://www.england.nhs.uk/wp-content/uploads/2021/06/B0642-ics-design-framework-june-2021.pdf
41
York Health Services and Delivery Research, January 2020 https://www.york.ac.uk/media/crd/Protocol-reg-inspec-integrated-care.pdf 17
42
Ibid, https://www.york.ac.uk/media/crd/Protocol-reg-inspec-integrated-care.pdf
43
NHS Providers, NHS Regulation: a shifting focus, 2019 https://nhsproviders.org/news-blogs/blogs/nhs-regulation-a-shifting-focusWhat every board member needs to know about improvement and quality assurance
5. Acknowledged enablers and barriers
This section considers some of the key provided by their organisation. It is were told that this can sometimes create
current enablers and barriers to effective therefore vital that they have a good an imbalance within boards and, in turn,
quality assurance, as highlighted by our understanding of quality, supported by a reduced understanding and challenge
NHS, independent sector and international robust governance systems and processes. around quality and quality assurance issues.
colleagues in interviews. The board should set the tone and be Regulators recommend that at least one
the driving force for continuous quality non-executive director in NHS trusts has
This is not intended as an exhaustive improvement across the organisation.44 a clinical background.46 Many of those
list but it is presented as a means of we spoke to felt it was important that
demonstrating the breadth of factors NHS boards in the UK adopt a unitary board members had a ‘lived experience’
that can impact on quality assurance and model, whereby executive and non- of healthcare, either through personal or
in order to support board members in executive directors jointly serve on the vicarious experience, to keep the board
the implementation of effective quality same board. In this mode, both executive focused on trying to do the right thing for
assurance systems and processes. and non-executive board members bear as many people as possible.
equal accountability for the quality of
This section will cover: services provided by the trust. In Europe, In the past, this has been counteracted
the unitary board model also exists in, for by initiatives like site visits; however, for
• board member expertise example, The Netherlands, Norway and obvious reasons, these have been drastically
• governance Sweden.45 reduced during the last 18 months. So
• culture boards have had to become more reliant
• workforce - specifically, capacity and In interviews, we were told that a on what they hear from regulators and
leadership significant proportion of health and social stakeholders to scrutinise and challenge
• digital technology and data literacy and care NEDs have a non-healthcare, often the narrative presented at committee and
• engagement. commercial or financial background. While board meetings without visiting or speaking
it is obviously important that boards are with frontline staff, as they would have pre-
5.1 Board member expertise diverse and incorporate a range of skill sets COVID.47 Those we spoke to were clear that
and, indeed, NEDs are often specifically such initiatives were vital to board quality
All board members are ultimately appointed to bring a skill or perspective assurance and should be stepped back up
accountable for the quality of services not currently available to the board, we as soon as possible.
44
NHS, The Healthy NHS Board: Principles for Good Governance https://www.leadershipacademy.nhs.uk/wp-content/uploads/2012/11/NHSLeadership-TheHealthyNHSBoard.pdf
Peter C Smith, Anders Anell, Reinhard Busse, Luca Crivelli, Judith Healy, Anne Karin Lindahl, Gert Westert, Tobechukwu Kene, Leadership and governance in seven developed health systems, 18
45
2021, https://pubmed.ncbi.nlm.nih.gov/22265340/
46
Monitor, 2014, The NHS Foundation Trust Code of Governance
47
GGI, Assurance, reassurance and performance, Illumination series, May 2021 (https://www.good-governance.org.uk/publications/insights/assurance-reassurance-and-performance)What every board member needs to know about improvement and quality assurance
Others also highlighted that non-clinical provider serves. We were told that, about the need for organisations to clear
NEDs can rapidly be brought up to where these governors had no clinical the significant elective backlog while also
speed through involvement in quality background, they often struggled to being told that, in order to achieve financial
committees and quality-related activities. engage with quality items and were more targets, they must close beds. Boards
We are aware that many health and reliant on reassurance from management of organisations have to make difficult
social care organisations actively appoint that services were high-quality and decisions and need to ensure that these are
non-specialist NED chairs for their sub- effective. dictated, at all stages, by reference to their
committees (i.e. a NED without a clinical mission and values, linked to their strategic
background to chair the quality committee) In each instance, board member induction intent.
in order to prevent operational and and development were highlighted as vital
assurance functions becoming blurred, to quality assurance. It was suggested that
as well as to provide a different lens and both newly appointed board members,
challenge to issues. as well as those from non-clinical
backgrounds, would benefit from coaching
Furthermore, while it is important to ensure or mentorship to help them understand
an appropriate balance of skills at board both what ‘good’ (and preferably
level (including in relation to clinical and ‘excellent’) looks like and what to look for
non-clinical skills) it is equally important when carrying out specific duties such as
for the board to ensure that the clinical site visits. In particular, it was suggested
leadership of the organisation is effectively that board members needed to have a
empowered to lead on quality governance, sound grip on complex topics, such as
and provide the appropriate assurance of health acuity, in a way that many currently
how this duty is being discharged, to the do not.
board.48
These challenges also somewhat extend
Similar issues were highlighted in our to executive directors. Those we spoke
interviews with international colleagues. to highlighted that silo working persisted
Canadian healthcare providers, for in many organisations, compounded by
example, have a board consisting of often contradictory messages from the
independent governors intended to centre. A particular example was provided
represent the communities that the around conflicting advice being given
19
48
NHS, The Healthy NHS Board Principles for Good Governance, p.12What every board member needs to know about improvement and quality assurance
5.2 Governance
Key questions for board members:
I find as an executive, it’s very easy to
give too much detail, but if you give too • Do we have sufficient quality expertise on our board to ensure adequate
much detail, non-execs will – and I’m sure scrutiny and challenge around quality issues?
I’d be the same – will go down rabbit • Have we provided NEDs with sufficient induction and developmental
warrens and miss the point. Our job is to support to ensure that they are comfortable contributing to discussions
make sure they have the right picture to around quality issues?
have confidence in what’s happening so • How do our board and committee reports support discussion and debate
they can make the right decisions and ask around quality issues?
the right questions.”
- a chief nursing officer at our roundtable devoted to significant quality issues.
Other key characteristics that have been This can be achieved through effective
Boards need to ensure that they are highlighted through our engagement agenda management and reporting.
effective in setting the right standards and include: Boards need to achieve this through the
gaining assurance that those standards principle of delegation and can choose
are being met. Indeed, one of the key • the board assurance framework (BAF) to establish quality committees to help
responsibilities of the board is around should assure the board what is the board understand quality issues and
assurance ‘that the organisation does what happening across the organisation, effectively fulfil its role around quality
it says it will do and behaves in the manner balancing the need to provide enough governance.50
it has agreed’.49 detail to inform but not overload with
information In addition to ensuring the key elements
Interviewees from organisations across UK • effectively sharing best practice internally, above are fit for purpose, we suggest
healthcare have all identified the need for with and between other organisations that boards routinely consider a series of
boards and organisations to see quality and systems key questions (developed through our
assurance, enabled by good governance, • having the right governance systems and conversations with interviewees) in assessing
as a holistic approach through which processes in place including committee whether governance is delivering the right
integrated reporting can be central. structure and associated reporting on outcomes for the organisation or entity and
quality, integrated reporting and the ultimately the population it serves.
appropriate amount of board time
49
GGI, Good Governance Handbook, 2015, p.7
20
50
GGI, Purposeful quality committees, 2021What every board member needs to know about improvement and quality assurance
It is also paramount that healthcare
organisations have forums at all levels where
staff can share learning from both good and Patient safety summit example from Barking, Havering and Redbridge
bad practice with colleagues. We heard University Hospitals NHS Trust
an example of one health and social care
provider implementing a system called The patient safety summit is a meeting attended by all staff disciplines (doctors,
Greatix (reporting examples of great work) to nurses, managers, students, allied health professionals, administrators, and a
sit alongside their Datix (incident reporting patient partner). It focuses on a serious or notable incident that has recently
system) with examples routinely shared at taken place at the trust. The meeting is chaired by either the medical director or
board and the quality committee. Others director of nursing, and is open to wider staff attendance.
highlighted how each sub-committee and
management forum had best practice as an
agenda item as a means of sharing lessons
learned and positive work.
Key questions for board members:
Patient safety summits are another
mechanism through which this can be • Does the board have the right systems in place to ensure it receives and
achieved, and we provide an example below utilises high quality data?
how this might be introduced. • Does the board use a range of improvement methods and are they fit for
purpose?
• Does the board consider trend data for quality metrics?
• Does the organisation allow for open discussions around the lessons from
incidents or near misses?
• Is the board sighted on and have confidence in timescales for further
improvement?
• Has the board put in place specific actions (that are regularly reviewed) to
ensure that, where the data indicates something is amiss, there is a closing of
the loop?
21What every board member needs to know about improvement and quality assurance
5.3 Culture • knowing how to ask the right questions Where boards are not effectively asking
and what the right questions are these sorts of questions and monitoring
• providing and fostering the right organisational culture, the results are often
We’ve got to create a culture where environment through which individuals dire. The failings at Mid Staffordshire NHS
people feel safe to raise issues before can answer truthfully Foundation Trust are perhaps the most
they become a real problem.” • having challenging conversations high-profile example in recent times, where
• providing a safe space and environment an estimated 400 to 1,200 people died
– a chief nursing officer at our roundtable that allows staff to speak up, or a unnecessarily as a consequence of poor
‘blame-free culture’ quality of care and a culture that enabled
The importance of culture was consistently • holding listening and action events this.
highlighted by those we spoke to as central • looking at trends, not just information,
to effective patient care, safety and quality around complaints and compliments Other examples include the failure to
assurance. • testing against key cultural indicators provide appropriate care in the provision
around the provision of safe and of mental health services53 and maternity
What do we mean by ‘organisational effective care services where a ‘culture of blame’ has
culture’? • challenging sub-cultures when these shown to impact on the safety of the care
function and influence in a manner that provided.54
This is a phrase that can often be difficult is contrary to the overall organisational
to pin down. It has been described as: mission and vision. We suggest that boards routinely undertake
‘the way things are done around here’ by simple diagnostic exercises in relation to
Watkins (2013), the attitudes, beliefs and In order to foster an organisation or testing staff confidence in organisational
behaviours of groups of people within entity that has an open and transparent governance, as well as undertaking whole
organisations (Schien, 1985), or ‘the vision, culture, boards of healthcare organisations organisation culture and mindset surveys -
values and behaviours of an organisation and systems need to consistently ask in order for organisations to check-in and
and the people within it’.51 themselves whether the right environment test against key elements of organisational
exists or has been created.52 Deciding culture.
Key characteristics of organisations that by which metrics an organisation
embody a culture that allow for effective can be assessed as having an ‘open
quality assurance, include speaking up and and transparent’ culture is, however,
listening, or: challenging.
51
Nightingale, Adele (2018) Developing the organisational culture in a healthcare setting. Nursing Standard, 32 (21), p. 4-5
52
GGI, Creating the right culture for integrated care, Illumination series, July 2021 https://www.good-governance.org.uk/publications/insights/creating-the-right-culture-for-integrated-care
53
The Observer, Coroners warned of mental health care failings in dozens of inquests, September 2021 https://www.theguardian.com/society/2021/sep/05/coroners-warned-of-mental-health-
22
care-failings-in-dozens-of-inquests
54
BBC, Culture of blame holding back maternity safety, report finds, July 2021, https://www.bbc.co.uk/news/health-57725263You can also read