WELCOME TO ESPN/ERKNet Educational Webinars on Pediatric Nephrology & Rare Kidney Diseases
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

WELCOME TO
ESPN/ERKNet
Educational Webinars on Pediatric
Nephrology & Rare Kidney Diseases
• Date: 01 June 2021
• Topic: Atypical Hemolytic Uremic Syndrome
• Speaker: Marina Noris
• Moderator: Elena Levtchenko
HEMOLYTIC UREMIC SYNDROME
Histology lesions: Swelling and detachment of endothelial cells, accumulation of fluffy material in the
subendothelium, thrombi and obstruction of the vessel lumina.
Ischemia Stenosis
Endothelial injury
subendothelial espansion
Stenosis
Organ dysfunction Thrombosis Shear stress
Thrombocytopenia RBC fragmentation
Ruggenenti and Remuzzi, Kidney Int 2001
2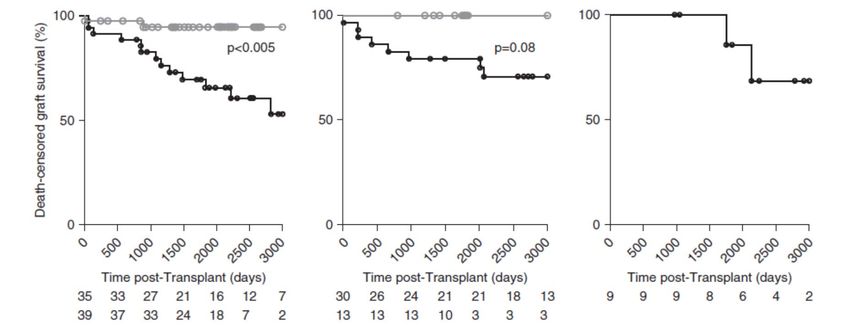
Adhesion molecules and
dHUS STEC P-selectin up-regulation
Comp Gene Defective complement
aHUS mutation regulation
TTP ADAMTS13 UL-VWF multimers
Autoimmune or systemic Complement activating
sHUS diseases, tx, infections
conditions
glomerulopathies,
Microthrombi
3
ATYPICAL HEMOLYTIC UREMIC SYNDROME
100
Patients free of events
Death or ESRD (%)
80
60
aHUS
40
Incidence:
0.5-2/1,000,000/year 20
0
Sex: no difference 0 2 4 6 8 10 12
Follow up (years)
A life threatening multisystem disease of microangiopathic hemolytic anemia, thrombocytopenia, and acute renal failure
4 with predominant but not exclusive renal involvement.
Active after Low grade
trigger constitutively active
Classical pathway Lectin pathway Alternative pathway
IgM, IgG1, IgG3 Mannose residues, tick-over, bacteria,
Immune complexes IgG4 bacterial toxin, LPS
Pathogen Pathogen H2O
C3
Igs Y C4b C2b
MBL
Mannose
CFH
C1q C3a
C1r C1s MASP fB CFI
C3b
C3 CD46
fD
C1inh THBD
C4bp C2b Bb
C4b C3b
C3 convertase C3a C3 convertase
C3b
C5
C3b C3b
C2b Bb
C4b C3b
C5a C6 C7 C8 C9 C5 convertase
C5 convertase
5 C5b-9 CD59
Factor H plays a pivotal role in the regulation of the alternative pathway of complement activation
Produced mainly in the liver as a single peptide glycoprotein, factor H circulates in plasma at a
concentration of 50 mg/dl
Regulatory Recognition
domain doman
C3b proteoglycans C3b proteoglycans
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
P1166L
V1168stop
I1169L
E1172stop
Y1197C
c.1494delA Q950H W1183L , W1183R
C309W S714stop E850K Y951H Q1076E
W1183C
Y118Ifs*4 M823T T956M T1184R
L98F C853Y I970V
C597stop L1189R
W978C L1189F
Q400K c.2303insA D1119G S1191L
Y235C D1119N
R53C S1191W
S58A S890I H893R P1130L G1194D
C630W Y899D V1134G E1195stop
R60G Y1021F
C673Y Y899stop E1135
C66Y C1043R V1197A
C915S Q924stop Q1137L E1198A, E1198K
c.155delAGAA W1037stop
C926F Y1142D F1199S
c.22686del15bp Y1142C V1200L
W1157R R1203W
C1163W G1204E
c.3486delA R1206C
c.3493+1G>A R1210C, S1211P
R1215G ,R1215Q
T1216stop
• >100 different pathogenic gene variants in 20‐30% of patients C1218R
P1226S
c.3675_3699del
c.3695_3698del
Warwicker et al., Kidney Int , 1998
• 90% are heterozygous, most in the recognition domain Caprioli et al., JASN, 2001
Richards et al., Am J Hum Gen, 2001
Perez‐Caballero et al., Am J Hum Gen, 2001
Dragon‐Durey et al., J Am Soc Nephrol, 2004
Caprioli et al., Blood, 2006
6 Noris et al, CJASN 2010
SOLID-PHASE RESTRICTED COMPLEMENT ACTIVATION IN aHUS
Domain recognition
Mutated CFH via regulatory
C- 20 domain still dissociates Bb from
CFB C3b and favors C3b inactivation
CFH
regulatory
CFI
Alternative pathway activation -N Bb
(spontaneous hydrolysis, iC3b
bacteria, viruses) C3b
regulatory Mutated CFH instead does not bind
C3 -N C3b and glycosaminoglycans on
CFH endothelium and does not regulate
complement on cell surface
CFB
C3b recognition
-C
C3a
C5
Surface bound C3 C5a
CFI convertase
iC3b Bb C5 convertase
C3b C3b
Manuelian et al., JCI, 2003
Sanchez‐Corral et al., Am J Hum Gen, 2002
Heinen et al., JASN, 2007
Noris et al, Blood 2014
Glycosaminoglycans Endothelial cell Merinero HM et al, Kidney Int 2018
7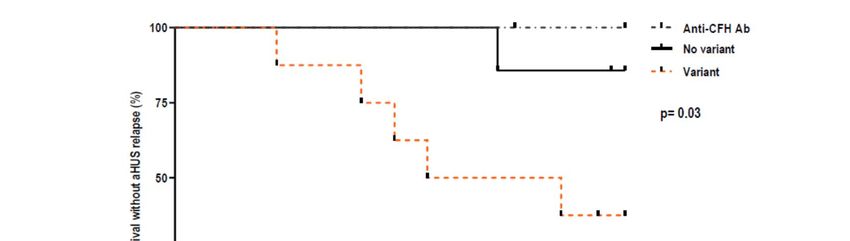
HIGH HOMOLOGY IN THE REGULATORS OF COMPLEMENT ACTIVATION
GENE CLUSTER
CFH/CFHR1 hybrid gene
Venables et al., Plos Medicine, 2006
• High degree of sequence identity between the gene for factor H and the genes for the five
factor H-related proteins (CFHR1 to 5) which favors non-allelic homologous recombinations
giving rise to hybrid genes.
• Copy number variation assays (CGH arrays or MLPA) are required to detect hybrid genes
• Identified in 34/485 aHUS patients (7%).
Piras et al., Frontiers in Medicine, 2020
8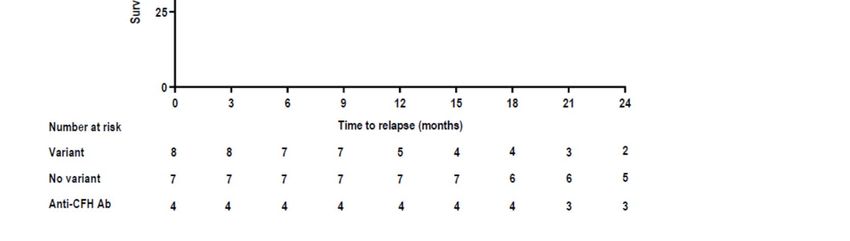
FH/FHR HYBRID PROTEINS FOUND IN PATIENTS WITH aHUS
FH/FHR1 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 4 5
Venables et al., PLoS Med 2006
FH/FHR1 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 5
Valoti et al., JASN, 2015
FH/FHR3 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 1 2 3 4 5
Francis et al., Blood, 2012
FH/FHR3 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 1 2 3 4 5
Challis et al., Blood, 2015
In the FH/FHR hybrid molecules the C-terminal SCRs of CFH are substituted with those of
FHR1 or with the entire FHR3, resulting in decreased complement regulatory activity on
endothelial cell surface
9
ANTI-FH AUTOANTIBODIES IN AHUS
40-80% 100%
FH 1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
80%
1 2 3 4 5
FHR1
8-9% mostly children Dragon-Durey et al JASN 2005
Blanc et al., J Immunol, 2012
● Anti-FH abs mainly target the FH C-terminus
● Most patients with aHUS and FH autoantibodies are homozygous for a deletion of genes encoding FH
related proteins 1 and 3.
● Failure of central and/or peripheral tolerance to FH related 1 and FH?
Zipfel et al, Plos Genetics, 2007
Jozsi et al, Blood, 2008
10 Trojnar et al, Front Immunol, 2017MCP VARIANTS IN aHUS spontaneous hydrolysis,
bacteria, viruses
C35X
C35Y (n=3)
E36X
P50T
R59X (n=4)
C3
1 C64P
K65D
192T>C+193-198del
C99R
2 R103W
SCRs G130V
(96-129)del+G130I+Y132T+L133X
3 Y189D
G204R
C3b
T267fs270X
4 (858-872)del+D277N+P278S
F242C
C3a
STP
TM A353V CFB
Y328X
CT
MCP 10%
CFI
MCP
iC3b C3b
Endothelial cell
Loss of function heterozygous variants: low expression or reduced C3b binding and cofactor activity
Noris et al, Lancet 2003
Richards et al, PNAS 2003
11 Caprioli et al, Blood 2006C3 AND CFB GAIN OF FUNCTION VARIANTS IN aHUS
CFB C3 7-10%
FH
FD CFB: 1-2%
CFI
C3 Bb
iC3b
C3b
C3b
CFB
CFB
C3a
C3
convertase
CFI C5
Bb
C3b iC3b C3b C5 convertase
MCP
Glycosaminoglycans
Endothelial cell
Goicoechea et al., PNAS, 2007
Roumenina et al., Blood, 2009
12 Fremeaux-Bacchi et al, Blood 2008GENETICS OF AHUS: AN EUROPEAN DISCOVERY
CFH
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20
CFH/CFHR1 hybrid
MCP
Newcastle 1
C3 Jena 2
3
~60%
4
anti FH Ab Del CFHR3/CFHR13
Paris
CFI THBD
Bergamo
Madrid
CFB
1 2 3
13THE CASE OF GENE POLYMORPHISMS IN CARRIERS OF PATHOGENETIC VARIANTS
TO EXPLAIN INCOMPLETE DISEASE PENETRANCE
* CFH Glu1172stop
R078 R077 R083 R079 R081 R082 R080 R084
p.Q672Q, SCR11
p.E936D,SCR16
-332C/T
R063
R078 R063 R077 R083 R079 R084
H3 H4 H3 H4 H4 H4 H4 H4 H4 H4 H4 H4
H3: T G T
* * * * *
Caprioli et al., Hum Molec Genet, 2003
•Among 21 families with CFH pathogenetic variants (26 patients with aHUS and 47 unaffected carrier relatives) the
H3 haplotype on wild-type allele was more prevalent in affected (69%) than in unaffected (17%) subjects.
Breno M et al., unpublished
• In 80 pedigrees with a mutation in complement genes (CFH, or MCP or C3 or CFB) aHUS penetrance was 60%
in subjects who also carried the CFH-H3 and the MCPggaac risk haplotypes, while only 18% of mutation carriers
with neither risk haplotypes developed the disease.
Arjona E et al., Blood 2020
14COMBINED COMPLEMENT GENE ABNORMALITIES IN aHUS
795 patients from 4 European cohorts
8.7% 8.2% 10%
22.6% 27%
Combined complement gene abnormaties were found in around 10% of patients with CFH or C3 or CFB
pathogenetic variants, and about 25% of patients with MCP or CFI pathogenetic variants.
Bresin et al, JASN 2013
15Trigger
C3
Eculizumab
A humanized monoclonal antibody
that binds to C5 PMP
CD40L
C3a
C3b
Coagulation
CFB
Platelet
CFI C3 C3 aggregation
C5 C5a
convertase
convertase
Bb C5b-9
C5
C3b Bb C5b
C3b
MCP C3b
C3b VWF
Endothelial cell Endothelial cell
Modified from Noris and Remuzzi, NEJM, 2009LONG TERM OUTCOME OF aHUS PATIENTS
100
MCP mutation
80
Patients free of events
Death or ESRD (%)
60
THBD mutation
40
C3 mutation
No mutation
CFI mutation
20
CFH mutation
0
0 2 4 6 8 10 12
Follow up (years) Noris et al CJASN 2010Platelet count Estimated GFR
mean change from baseline mean change from baseline
140 60
120
45
100
(x10-9/liter)
30
80
(ml/min)
60 15
40
0
20
0 -15
0 2 4 6 8 10 12 14 16 18 20 22 24 26 0 2 4 6 8 10 12 14 16 18 20 22 24 26
Months of Eculizumab treatment Months of Eculizumab treatment
Treatment effect was sustained for up to 26 months
Licht et al., Kidney Int, 2015THE RISK OF POST-TRANSPLANT RECURRENCE DEPENDS ON THE
GENETIC ABNORMALITY
Yes recurrence NO recurrence
FH
FH
MCP
MCP
transplant transplant
FH mutatedECULIZUMAB TREATMENT TAILORING BASED ON THE RISK STRATIFICATION
IMPROVED GRAFT SURVIVAL IN THE HIGH RISK GROUP
• High risk: recurrence in a previous graft, and/or pathogenic variants of CFH/C3/CFB
• Moderate risk: negative complement screening results or a pathogenic variant in CFI
• Low risk: isolated variants in MCP or anti-CFH autoantibody no longer detected at the time of transplantation
Zuber et al., JASN, 2019•A 26-year old male presents with suspicion of TMA after 1 week of vomiting and
progressive asthenia:
•Platelets: 39 x103/µL
•LDH: 1900 IU/L
•Hemoglobin: 8.2 g/dL
•Creatinine: 2.7 mg/dL
•ADAMTS13: >10%
•STEC tests: negative
•Serum C3, and C4 levels: normal
•Plasma C5b-9 levels: normal
•Can this be aHUS?
•No, because circulating complement parameters are normal
•Yes, could be, but further tests are neededBoth during the acute phase of the disease and at remission about half of
aHUS patients had normal serum C3 and plasma sC5b-9 levels
22EX VIVO C5b-9 ENDOTHELIAL DEPOSITION IN A LARGE COHORT OF aHUS PATIENTS
- Serum from controls (n=30) - anti-C5b-9 Ab staining
or untreated aHUS patients (n=121) - Confocal microscopy
Resting or ADP
activation
HMEC-1 Static incubation C5b-9 deposition
10 min 2-4 hours
Resting Activated
600 600
C5b-9 formed (% of control)
C5b-9 formed (% of control)
500 500
400 400
300 300
200 200
100 Normal range 100 Normal range
0 0
Acute Remission Acute Remission
(n=49) (n=59) (n=46) (n=32)
Resting : disease activity (sensitivity 100%, specificity 97%)
Activated: complement dysregulation (sensitivity 100 %)
23 Galbusera et al, Am J Kidney Dis, 2019ECULIZUMAB TREATMENT IN aHUS PATIENTS FULLY NORMALIZED EX
VIVO SERUM-INDUCED FORMATION OF C5b-9 ON HMEC-1
C5b-9 formed (% of control) 1200 1000
Plasma sC5b-9 levels (ng/ml)
1000
*PThe assay must be reproduced by other specialized laboratories so that clinicians
could consider using it
25SERUM FROM PATIENTS WITH HYPERTENSION-ASSOCIATED HUS INDUCED C5b-9
DEPOSITS ON HMEC-1
• Compared with serum from healthy controls (HC), serum from patients with aHUS or hypertension-
associated HUS induced abnormal C5b-9 formation on HMEC-1. C5b-9 deposits normalized after
eculizumab treatment. Timmermans S et al JASN, 2018
• Either serum or activated plasma from patients with acute aHUS induced more C5b-9 deposition on
HMEC-1 than control sera.
• C5b-9 deposits were at control levels or lower with activated-plasma from aHUS patients treated with
eculizumab Palomo M et al, CJASN, 2019
26Every 15 days forever?
How to monitor and
possibly tapering?
330.000
euro per patient per year
(in child)RISK OF AHUS RELAPSE AFTER ECULIZUMAB DISCONTINUATION: A
PROSPECTIVE NATIONAL MULTICENTRIC OPEN-LABEL STUDY
55 patients (19 children and 36 adults) discontinued eculizumab (mean duration of treatment, 16,5 months)
Children
During follow-up 13 (23%) patients experienced aHUS relapse. In multivariable analysis,
the presence of a rare complement gene variant was associated with an increased risk of
relapse (OR 16.20 [1.78-147.72]).
Fakhouri et al, Blood, 2020
28EX VIVO AHUS SERUM-INDUCED C5b-9 FORMATION ON RESTING HMEC-1
DURING ECULIZUMAB TAPERING/DISCONTINUATION
300
Induction and Tapering Discontinuation
maintenance
C5b-9 formed on resting cells : relapse
(% of control) 200
100 Normal range
0
healthy ≤14d 4w – 6w ≥7w
controls
● The large majority of patients taking eculizumab at extended interdose intervals retained normal
serum-induced C5b-9 deposits on unstimulated endothelium
● All five patients (colored dots) manifesting relapses showed elevated C5b-9 deposition on resting
endothelial cells, in concomitance with or before worsening of clinical parameters (sensitivity for
disease relapse 100%)
29 Galbusera et al., Am J Kidney Dis, 201942 year old woman
heterozygous CFI mutation (p.R187Q)
• During a recurrence the patient was treated with eculizumab resulting in disease remission
• After 7 months of eculizumab every 2 weeks, the interval between doses was increased till discontinuation
• Six months after eculizumab cessation, C5b-9 deposits on resting HMEC-1 rose above normal levels
• One month later the patient developed a disease relapse
Eculizumab
Plt 94 212 142 154 141 115 175
Hb 7.2 7.2 12.8 12.3 10.7 11.6 12.3
LDH 869 401 446 451 525 679 446
Apto ‐ ‐ 85 34 57 ‐ ‐
Creat 4.5 2 1.40 1.50 1.70 1.80 1.20
C5b-9 formed on resting HMEC
500
400
(% of control)
300
200
100 Normal range
0
recurrence 2wk 4wk 10wk 6 mo 7mo 2wk
30 Time from previous eculizumab dose
Galbusera et al., Am J Kidney Dis, 201916 year old girl
‐ recurrent aHUS (onset at 14 years of age)
‐ no identified complement gene abnormalities
• During a recurrence the patient was treated with eculizumab resulting in disease remission
• After 2 year eculizumab every 2 weeks, the interval between doses was progressively increased
• Hematological and renal parameters and C5b‐9 deposits on resting HMEC‐1 remained stably normal
Plt 180 147 190 181 203 175 172
Hb 9 11 11.7 11.4 11.6 11.3 10.6
LDH - 301 349 341 378 313 408
Apto - 50 82 49 74 83 55
Creat 1.3 0.74 0.81 0.8 0.79 0.66 0.67
500
on resting HMEC-1
400
C5b-9 formed
(% of control)
300
200
100 Normal range
0
acute 2w
2wkpost 3w
3wkpost 4w post 5w post
5wk 6w post
6wk 8w post
recurrence 4wk 8wk
Galbusera et al., Am J Kidney Dis, 2019
31CH50 DID NOT EFFICIENTLY DETECT RELAPSE DURING ECULIZUMAB
TAPERING/DISCONTINUATION
300 Induction and Tapering Discontinuation
maintenence
: relapse
Serum CH50Eq 200
(UEq/ml)
Normal range
100
0
healthy ≤14d 4w – 6w ≥7w
controls
● At 5-week or longer intervals between eculizumab doses, total complement activity (CH50) levels
did not differ between patients who had relapse (coloured dots,132±92 UEq/ml) and those who did
not (grey dots,113±72 UEq/ml).
32 Galbusera et al., Am J Kidney Dis, 2019EX VIVO C5b-9 DEPOSITION HIGHLIGHTS COMPLEMENT DYSREGULATION
AND DISEASE RELAPSES WHILE THE OTHER BIOMARKERS DO NOT
Acute aHUS Remission aHUS Eculizumab discontinuation
No therapy Eculizumab No relapse Relapse
Plasma sC5b-9 N/ N/ N/ N/ N/
CH50 N N N N
C5b-9 deposition on:
- resting HMEC N N N
• Plasma sC5b-9 levels did not differ between acute aHUS and remission and did not consistently
change during eculizumab treatment or after discontinuation
• CH50 was normal in aHUS, was suppressed by eculizumab and returned to normal after
discontinuation, independently from disease relapses
• C5b-9 deposits on resting HMEC were elevated only in patients with acute aHUS and in those with
signs of relapses during eculizumab discontinuation
33 Galbusera et al., Am J Kidney Dis, 2019Take Home Messages In Atypical HUS local complement activation on endothelial surface (rather than fluid phase) plays a pathogenic role. Genetic abnormalities (mainly heterozygous) causing loss of function of AP complement regulators or gain of function of the components of the AP C3 convertase predispose to aHUS. Both gene mutations and risk polymorphism concur to determine disease penetrance. C5-inhibition efficiently induces disease remission in aHUS and prevents disease recurrences The presence of a pathogenetic complement gene variant increases the risk of relapse upon anti-C5 therapy discontinuation, however relapses are still difficult to predict and early and reliable markers are required
ATYPICAL HEMOLYTIC UREMIC SYNDROME: A DISEASE IN A DISH Diagnosis Monitoring
Thanks!
Caterina Mele
Roberta Donadelli Santiago Rodriguez de Cordoba
Elisabetta Valoti Tim Goodship
Rossella Piras Veronique-Fremeaux Bacchi
Marta Alberti Peter Zipfel
Lucia Liguori Marina Botto
Matteo Breno Matthew Pickering
Miriam Galbusera John Atkinson
Sara Gastoldi Richard Smith
REGISTRO INTERNAZIONALE
Erica Daina SEU/PTT
Centri partecipanti 190 Svizzera
28 casi
Danimarca
3 casi Germania
20 casi
Estonia
1 caso
Cina
2 casi
R. Ceca
Zoltan Prohaska
11 casi
Pazienti SEU/PTT 1481
Elena Bresin
12/2018
Marie-Agnes Dragon Durey
Trento
Varese Bergamo
Brescia Treviso
Bielorussia
2 casi
Monza Polonia Serbia
15 casi 5 casi
Milano Vicenza
Paraskevas Iatropoulos Lubka Roumenina
Torino Padova
Genova Pavia Parma
UK Austria Corea del Sud Filippine
9 casi
Sara Gamba
1 caso Croazia
Fadi Fakhouri
1 caso 3 casi Grecia Russia
2 casi 4 casi 6 casi
Firenze
Italia Roma
1037 casi
Miriam Rigoldi David Kavanagh
Romania
3 casi
Egitto
Belgio Cipro Foggia Turchia Arabia S.
1 caso 1 caso 4 casi
3 casi 9 casi
Sassari Salerno
Bari
Spagna
6 casi
Singapore
1 caso
Josh Thurman
Cagliari Israele
17 casi
Ariela Benigni Portogallo
Bulgaria
1 caso
Brasile
3 casi
Lituania
1 caso
Palermo
Reggio Calabria
Augustin Tortajada
11 casi
IRAN
51 casi
Giuseppe Remuzzi Canada
9 casi
USA Argentina Cile
4 casi
Emirati Arabi Sud Africa
58 casi 23 casi 1 caso 2 casi
http://www.marionegri.it
India
11 casi
Australia
14 casi
Giappone
2 casi
Malesia
2 casi 36Next Webinars
• ESPN/ERKNet Educational Webinars on Pediatric Nephrology &
Rare Kidney Diseases
• Date: 15 June 2021
• Speaker: Rosa Vargas Poussou
• Topic: Dent Disease
• ERKNet/ERA-EDTA Advanced Webinars on Rare Kidney
Disorders
• Date: 29 June 2021
• Speaker: Jürgen Floege
• Topic: Update on KDIGO on Immune Glomerulopathies
• ESPN/ERKNet Educational Webinars on Pediatric Nephrology &
Rare Kidney Diseases
• Date: 07 September 2021
• Speaker: Dieter Haffner
• Topic: Renal hypophosphatemia
Subscribe the ERKNet and IPNA Newsletter and don‘t miss Webinars!You can also read