VA SIERRA NEVADA HEALTH CARE SYSTEM | RENO, NV
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The American Legion
SYSTEM WORTH SAVING
VA SIERRA NEVADA HEALTH CARE SYSTEM | RENO, NV
Date: March 9 – 10, 2016
Health Administration Committee Member: Jeanette Rea
Deputy Director of Veterans Affairs and Rehabilitation Division: Roscoe Butler
Deputy Director of Employment and Education: Mark Walker
Assistant Director Operation Comfort Warrior: Bruce Drake
Overview tient Care Services/Nurse Executive were in attendance.
Human Resources Department
As of February 22, 2016, the VASNHCS indicated they have ap-
proximately 1,400 employees. Of this number, the VASNHCS
reported 190 vacancies.
Workforce trends continue to be largely influenced by the cur-
rent economic climate which has led to an increased number of
applicants for most vacant administrative positions. Physician
and specialty registered nurse positions remain a recruitment
challenge. Of paramount concern is the age of their workforce.
Over 11% of their current workforce is eligible to retire, and
many eligible employees fill leadership roles or other critical
positions.
For example, one of the three members of their executive lead-
The VA Sierra Nevada Health Care System (VASNHCS) is an in- ership is eligible to retire now. In addition, 46% of their nurse
tegrated system providing health care across Northern Nevada managers and 21% of their physician leaders are eligible for im-
and Northeastern California. VASNHCS includes a level 1-C mediate retirement in fiscal 2016. VASNHCS is actively devel-
VA Medical facility that provides primary and secondary care oping their current workforce to address this gap and intends
to 20 counties in northern Nevada and northeastern California. to implement the new Phased Retirement Program when avail-
Services include general medicine, mental health, gynecology, able.
orthopedics, ophthalmology, urology, vascular, cardiac cath-
eterization, emergency department, intensive care, diagnostic Employee Surveys
imaging and nuclear medicine, pharmacy, surgical services, Like the broader American workforce, VASNHCS employees
telehealth, primary care, dental clinic, and eye clinic. Pediatric span four generations, each with unique generational person-
and obstetric services are not currently offered. alities and expectations related to their work environment, ca-
The VASNHCS operates four Community Based Outpatient reers, and personal social backgrounds. VASNHCS continues
Clinics (CBOCs) that are located in Auburn, CA; Gardnerville, to identify and address these differences through tools such as
NV; Susanville, CA; and Fallon, NV. Hours of Operation: Mon- “True Colors,” the All Employee Survey, and team-building ef-
day through Friday 8:00 am to 5:00 pm. Shuttle van service from forts focused on the identification of recruitment barriers and
Auburn to Reno daily - departs at 7:30 am. The clinics provide using job satisfiers and techniques.
primary care, mental health therapy (individual and group),
and social services. No Pharmacy or Emergency Clinic. Fee ba- Employee Safety
sis contracts for Laboratory and Radiology. Summary of VASNHCS scores
Executive Leadership Briefing Employee Safety Barometer: Barometer Survey scores
from 2012 (13%) to 2015 (24%). Scores by Program Category
On March 9, 2016, the SWS team met with the executive lead-
were high for Supervisor Participation, Safety Support Ac-
ership to discuss the previous night’s town hall meeting and to
tivities, and Safety Support Climate Activities. Management
go over additional questions. Lisa Howard, Medical Center Di-
Participation and Employee Participation scores were low, but
rector; Dr. Steven Brilliant, Chief of Staff; Joan Bucker, Acting
compared to 2012 scores
Associate Director; and Rachel Crossley, Associate Director, Pa-
Patient Safety: 2014 Patient Safety Culture Survey administered
The American Legion | SYSTEM WORTH SAVING REPORT 1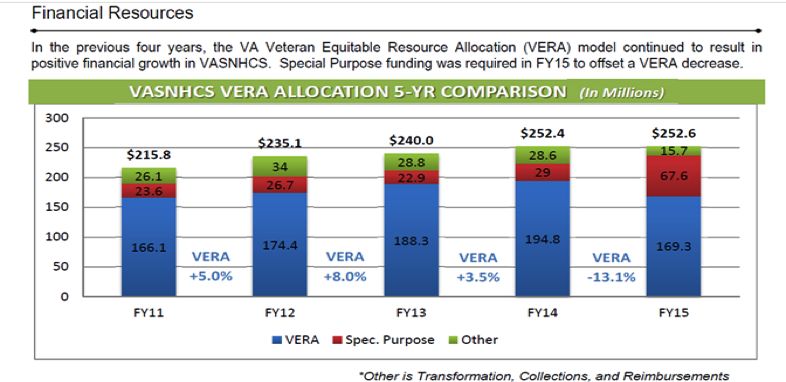
The American Legion
SYSTEM WORTH SAVING
to staff showed 15 of 15 dimensions below Veterans Health Ad- Fiscal Fiscal Fiscal Fiscal Fiscal
ministration (VHA) averages, with two dimensions scoring two Group Type
2010 2011 2012 2013 2014
standard deviations below. This is an improvement however
Enrollees 45,765 41,593 40,800 42,092 43,008
from 2011 when there were four dimensions that were two stan-
dard deviations below national average. Small sample size made Uniques 28,630 30,020 30,562 31,797 32,435
generalizations difficult. So low scores, but improving. Highly Rural 2,828 2,951 2,998 3,064 3,122
Integrated Ethics: 25% of questions were the lowest of any fa- Rural 11,709 12,180 11,315 11,736 12,037
cility in VA Sierra Pacific Network (VISN 21). 53% were at or Urban 14,087 14,766 16,243 16,827 17,115
below the 30th percentile for all National, CO, VO, and VISN
Female 1,956 2,258 2,287 2,448 2,341
questions. There was a 27.3% response rate as compared to
16.2% for 2012 Operation
Enduring Free-
RN Satisfaction: Overall nursing satisfaction scores in fiscal dom (OEF)/
2014 are improved relative to fiscal 2012 with better than na- Operation
tional gains in Participation, Quality of Care, Registered Nurse 1,522 1,705 2,038 2,341 2,540
Iraqi Freedom
Manager and Staffing categories. (OIF)/Op-
eration New
Financial Management Dawn (OND)
Homeless 780 1,005 1,126 1,837 1,802
Business Office
The Business office provided the following statistics on the
VASNHCS:
• Fiscal 2015 Admissions - 3,380
• Average Daily Census for each inpatient program – 49
• Fiscal 2015 Outpatient visits - 448,715
• Fiscal 2016 Projected Outpatient visits - 542,419
Historical Workload
Veteran Demographics
Fiscal Fiscal Fiscal Fiscal Fiscal
The VASNHCS catchment area expands to Alpine, El Dorado, Services Type
2010 2011 2012 2013 2014
Lassen, Modoc, Mono, Nevada, Placer, Plumas and Sierra coun-
Outpatient Encounters 48,5139 52,5412 54,6348 59,8534 60,8900
ties in California. Carson City, Churchill, Douglas, Esmeralda,
Eureka, Humbolt, Lander, Lyon, Mineral, Pershing, Storey, and Community Discharges 295 272 294 377 311
Living Cen-
Washoe counties in Nevada are also served by VASNHCS. Bed Days 20,705 20,841 20,628 19,984 20,753
ter (CLC)
VASNHCS provides care to a diverse group of veterans. Below is Discharges 2605 2,860 2,841 2549 2,500
a breakdown of the groups that they serve. Medicine
Bed Days 12,352 12,782 11,121 10,569 10,726
Discharges 646 709 682 581 614
Psychiatry
Bed Days 3,978 3,542 3,634 3,957 4,170
Discharges 564 590 577 590 557
Surgery
Bed Days 2,859 2,915 2,961 2,984 2,953
The American Legion | SYSTEM WORTH SAVING REPORT 2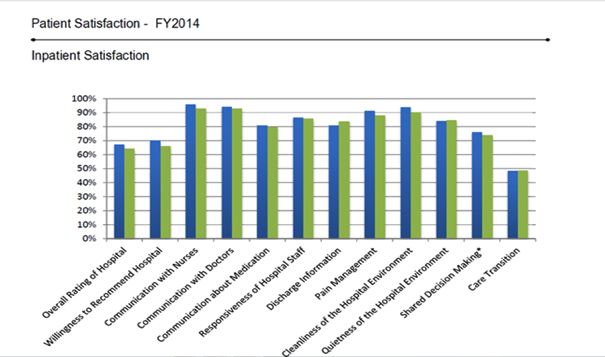
The American Legion
SYSTEM WORTH SAVING
Non-Va Coordinated Care Program (NVCC) MONTHLY SUMMARY OF FEE CONSULT REQUESTS
NVCC budget for the following: FISCAL 2015
Type Oct Nov Dec Jan Feb Mar Total
Authorized Care
Physical
• Fiscal 2013 - $19,236,000 221 169 180 91 28 30 719
Therapy
• Fiscal 2014 - $27,446,900 Ultrasound 154 136 142 27 1 0 480
• Fiscal 2015 - $25,074,500 (Authorized and Unauthorized, not Neurosurgery
tracked separately in Fiscal 2015) 59 58 73 76 94 75 435
Evaluation
Unauthorized Care Mammogram
Female Screen- 63 41 33 55 34 68 294
• Fiscal 2013 - $1,314,500
ing
• Fiscal 2014 - $3,423,000
Radiol-
Service-Connected (SC) Emergency Care/Mill Bill Emergen- ogy / Magnetic
55 83 60 35 24 29 286
cy Care1 Resonance
Imaging (MRI)
• Fiscal 2013 - $22,760,500
Home Base
• Fiscal 2014 - $31,959,900 Primary Care 117 27 38 8 27 21 238
• Fiscal 2015 - $28,448,400 Skilled Nursing
Home Based
Primary Care
105 41 21 6 14 23 210
Home Health
Services
Colonoscopy 29 27 38 20 7 29 150
Neurosurgery
25 14 21 17 25 30 132
Procedure
Radiology /
Computerized
13 60 46 7 1 126 286
Tomography
(CT) Scan
Dental Spe-
20 14 21 17 21 18 111
cialty Services
Radiation
Therapy Evalu- 22 16 24 17 11 20 110
ation
Radiation
Therapy Treat- 18 18 20 16 12 22 106
ment
1 Emergency Care is not broken out separately.
The American Legion | SYSTEM WORTH SAVING REPORT 3
The American Legion
SYSTEM WORTH SAVING
There were many more patients sent out last year with the im- Projected Veteran Utilization
plementation of the Accelerating Care Initiative (ACI). The first VASNHCS has experienced steady growth in both enrollees
three months of fiscal 2015 still reflected some of that volume. and users over the past several years despite declining veteran
The Choice program, implemented in November is reducing population. Looking forward, the Veterans Health Administra-
the number of NVCC consults. tion (VHA) expects to see increases in outpatient utilization and
reductions in inpatient utilization over the next 10-20 years.
Fiscal Fiscal 5-Year Fiscal 10-Year Fiscal 20-Year
Service
2013 2018 Gap % 2023 Gap % 2033 Gap %
Acute Inpatient Medicine 13,877 11,978 -14% 10,633 -23% 8,252 -41%
Acute Inpatient Mental
3,978 3,900 -2% 3,331 -16% 2,443 -39%
Health
Acute Inpatient Surgery 7,442 6,629 -11% 5,751 -23% 4,129 -45%
Ambulatory: Dental Clinic 21,173 26,597 26% 28,568 35% 28,170 33%
Ambulatory: Laboratory
10,7231 118,214 10% 125,902 17% 127,251 19%
and Pathology
Ambulatory: LTSS Home
39,416 44,373 13% 48,768 24% 60,904 55%
and Community Based
Ambulatory: Medical &
Other Non-Surgical Spe- 83,413 92,209 11% 97,959 17% 127,251 29%
cialties
Ambulatory: Mental
62,812 75,214 20% 77,653 24% 80,325 28%
Health Programs
Ambulatory: Primary
Care-Geriatrics-Urgent 138,744 150,861 9% 157,799 14% 160,740 16%
Care
Ambulatory: Radiology
47,207 51,422 9% 55,749 18% 58,208 23%
and Nuclear Medicine
Ambulatory: Surgical
52,934 58,215 10% 62,026 17% 62,901 19%
Specialties
Blind Rehab 420 627 49% 704 68% 723 72%
Inpatient Residential
Rehab Mental Health 212 3,688 15% 3,240 1% 2,437 -24%
Programs
Long-Term Services and
29,395 36,386 24% 39,414 33% 41,785 42%
Supports Inpatient
Spinal Cord Injury 587 635 8% 574 -2% 449 -24%
Pharmacy 1,461,366 1,569,619 7% 1,724,228 18% 2,004,757 37%
The American Legion | SYSTEM WORTH SAVING REPORT 4The American Legion
SYSTEM WORTH SAVING
Quality Management VASNHCS Strategic Priorities:
• Access: Improvements to increase capacity will better avail pa-
tients of quality care within medically appropriate timeframes.
• Workforce Development: Leadership that is forward-looking,
agile, adaptive, high performing, rewarding innovation and
supporting teamwork will proactively recruit, train, develop,
reward, motivate, and inspire our workforce.
• Veteran Engagement: A system that is actively gathering vet-
eran feedback and will appropriately tailor our processes to
address veteran need will be developed.
• Community Engagement: Communication with our com-
munity stakeholders is essential to enriching our role as a part-
ner and resource in the neighborhoods and districts we serve.
• Stewardship: As stewards, we must effectively align resources
to provide quality care and deliver sustained value to veterans
and taxpayers alike.
Strategic Priorities for Fiscal 2015 and 2016:
• Inpatient Care: A system-wide approach to improving how
patients move through our inpatient flow, from admission to
discharge. Several workgroups will investigate each piece of
the flow to strategize improvements.
• Memory Care: Develop a plan to provide an appropriate en-
vironment for individuals diagnosed with dementia who are
awaiting long-term placement and improve patient care and
safety.
• Daily Management System: Improve communication related
to the management of daily operations, ensuring proper eleva-
tion of critical information and provide opportunities to rem-
edy challenges at the lowest level.
• New Employee Onboarding: To address the extended time it
Strategic Plan takes to complete employee onboarding, this workgroup will
address the hiring process phases and establish timeline goals
The VASNHCS released their fiscal 2015 Strategic Plan on June and create a centralized process to help expedite the onboard-
29, 2015. Their plan, called Strategy for Excellence, begins with ing process.
the following VA Strategic Goals:
• The VASNHCS achieved Health & Human Service’s Gold Rec-
• Empower Veterans to Improve Their Well-being ognition for its participation in the National Hospital Organ
• Enhance and Develop Trusted Partnerships Donation Campaign.
• Manage and Improve VA Operations to Deliver Seamless and • The VASNHCS earned the Gold Standard for its participation
Integrated Support in the National Center for Patient Safety Program.
VASNHCS Mission: Provide World Class Care and Services to • The Office of the Inspector General conducted a scheduled
America’s Heroes. audit in March 2015. Several areas of care were reviewed with
recommendations and follow-up action plans submitted. Ac-
VASNCHS Strategic Goal: Provide veterans personalized pro-
tion plan implementation and staff education are ongoing.
active, and patient-driven health care.
• In May 2014, the Joint Commission conducted an unan-
The American Legion | SYSTEM WORTH SAVING REPORT 5The American Legion
SYSTEM WORTH SAVING
nounced two-day survey covering several areas of patient care. Outreach Events
Patient access to care was thoroughly reviewed and no recom-
mendations for improvement were identified. VASNHCS 2016 OUTREACH CALENDAR
• The VASNHCS hosted both veteran and community town hall Confirmed
Date Time Location
meetings to facilitate outreach and communication. Event
Women Veter- 1:00 p.m. to
03/18/2016 Main Campus
Women Veterans ans Memorial 3:30 p.m.
A total of 1,978 women veterans receive care from the VASN- Vietnam Veter- 12:00 p.m. to
03/25/2016 Main Campus
HCS Women’s Clinic. The Women Veterans Program Manager ans Standown 3:00 p.m.
projects that over the next five years this number will increase to Senior Spec-
12:00 p.m. to
3,773. The Women’s Clinic has on staff one gynecologist and two trum Baldini’s 05/03/2016 Baldini’s
5:00 p.m.
primary care providers at the Reno facility. There is one primary Health Fair
care provider at the Carson Valley CBOC. Korean War
10:00 a.m. to
Veteran’s As- 05/05/2016 Sparks
The VASNHCS typically hosts 12 events annually to include Go 12:30 p.m.
sociation
Red for Women Health and Pink Out for Breast Cancer. The
medical center hosted a Women Veterans Town Hall on March Crossroads of
05/21/2016- To Be Deter- Convention
18, 2016. the West Gun
05/22/2016 mined Center
Show
VASNHCS Women Veterans Statistics 05/16/16- 11:00 a.m. to Livestock
Reno Rodeo
• Fiscal 2014 – 41,593 05/25/2016 9:00 p.m. Arena
Native Ameri-
• Treated Fiscal 2014 – 31,938 3:00 p.m. to
can Veterans 06/23/2016 Main Campus
4:30 p.m.
• Total Women Veterans in VASNHCS catchment area – 7,619 Town Hall
• Total number enrolled – 2,618 Hot August 08/02/2016- 10:00 a.m. to Grand Sierra
Night 08/07/2016 9:00 p.m. Resort
• Total number receiving care with the HCS – 1,978
Senior Spec-
• Market penetration fiscal 2014 for enrolled women – 0.34 To Be Deter-
trum Senior 09/06/2016 Old Town Hall
mined
• Market penetration fiscal 2014 for women receive care – 0.25 Fest
• Projected enrollment in five years – 3,773 Reno Bighorns 12:00 p.m. to Reno Event
Multiple Dates
Legal Clinic 3:30 p.m. Center
• Projected enrollment in 10 years – 4,241
VASNHCS 2016 OUTREACH CALENDAR
Unconfirmed
Date Time Location
Event
Grass Valley Grass Valley,
Summer 2016 TBD
Outreach Fair CA
Reno Sparks
Late Spring
Indian Colony TBD TBD
2016
Outreach
Street Vibrations 06/21/2016 TBD Reno/Sparks
Herlong Army
TBD TBD Herlong, CA
Depot
Reno Aces Mili- Aces Ball-
TBD TBD
tary & Vet Games park
Lovelock Frontier 07/29/16- Lovelock,
TBD
Days 07/31/2016 NV
OEF/OIF
August /
Welcome Home TBD Reno
September
Event
The American Legion | SYSTEM WORTH SAVING REPORT 6The American Legion
SYSTEM WORTH SAVING
Data Breaches Construction Project:
Over the last three fiscal years, the VASNHCS reported 219 data
breaches. Veterans Health Administration (VHA) defines a data Project Name 1st Fund
breach violation as “the loss, theft, or other unauthorized access, Renovate and Rightsized Operating Rooms 2017
other than those incidentals to the scope of employment, to data
Execute New North Campus lease to provide Patient Aligned Care
containing sensitive personal information (SPI), in electronic 2017
Team Clinic
or printed form, that results in the potential compromise of the
Renovate and Expand Operating Room Support Areas 2018
confidentiality or integrity of the data.” To reduce the number of
data breaches, employees are required to undergo Privacy and Expand/Renovate Magnetic Resonance Imaging Space 2018
HIPAA training in person or through VA’s Talent Management Renovate Space Adjacent to the Intensive Care Unit Wing B3 of
2018
System (TMS). Building 12
Convert Facility to Electronic Proximity Care Locking System 2018
Procure Land for Campus and Parking Expansion to increase
2018
Security Setbacks
Expand Emergency Power Capacity at the Boiler Plant 2018
Replace damaged piping in clinical Building 1D 2018
Repair critical electrical deficiencies in Clinical Building 1D 2018
Execute New South Campus lease to Provide Patient Aligned Care
2018
Team Clinic
Provide emergency Water Tank Supply 2019
Provide Bird Protection for Patient Safety and Infection Control 2019
Replace Air Handling Units Serving Building 12 2019
Provide Sewer Storage Tanks for Emergency Management 2019
Construct Solar Plane Array on New Parking Garage 2019
Install New Energy Efficient Chiller and Cooling Tower 2019
Construct Parking Garage 2019
Correct Seismic Bracing for Non Structural Components & Equip-
2019
ment in Critical Patient Care Areas
Renovate Wing B4 of Building 12 for Single Patient Rooms 2019
Renovate Sterile Processing Service 2020
Construct New Community Living Center Building (Pod 3) 2020
Repair Exterior Walls for building throughout campus 2020
Renovate Vacant Primary Care for Pharmacy 2020
Realign Center Cores of Wings B4 and B5 in Building 12 2021
Construct New Wellness Center 2021
Construct Solar Panel Array on Second New Facility Parking Garage 2021
Extend Elevators to Roof for Improved Maintenance Access 2022
Construct New Community Living Center Building (Pod 1) 2022
Construct Third Parking Garage 2023
Construct New Inpatient Mental Health Ward 2023
The American Legion | SYSTEM WORTH SAVING REPORT 7The American Legion
SYSTEM WORTH SAVING
Town Hall on various VASNHCS services offered to women veterans. Ms.
Howard spoke of VASNHCS’ commitment to outreach and ser-
On March 8, 2016, a town hall meeting was held at 7:00 pm at
vice to women veterans and offered that in an area adjacent to
the American Legion Post One at 877 Ralston Street, Reno, Ne-
the town hall, the Veterans Benefits Administration (VBA) was
vada, to hear firsthand from veterans and family members about
available to work with veterans with specific claims issues. She
their VA health care experience. In addition to veterans and their
also announced that the Joint Commission had conducted a tri-
family members, the following American Legion Department of
annual survey that week, and that surveyors were complimen-
Nevada officials were in attendance: Lionel Motta, Department
tary of the services that VASNHCS provides.
Adjutant; David S. Evans, Department Commander; John War-
den, Alternate National Executive Committeeman (NEC); and There were approximately 20-30 people in attendance and the
Jack Edstrom, Post One Commander. Glenna Smith, Regional comments were mostly positive. Acting Women Veterans Pro-
Representative, Senator Dean Heller’s Office; and Tracy Soliday, gram Manager Christie Lambert discussed community outreach
Constituent Service Representative, Congressman Mark Amo- and the facility’s efforts to revive the Women Veterans Commit-
dei represented the local Congressional field offices. Lisa How- tee. Ms. Howard asked the room for assistance in spreading the
ard, Medical Center Director, represented VASNHCS. word about the services VASNHCS offers women veterans.
Following are the concerns that were raised during the town hall Afterwards, participants strolled outside to attend a Women Vet-
meeting. erans Memorial Garden with formal ceremony including Con-
gressional, State Government, and Governor Representatives,
• Barbara from Las Vegas VAMC reported that she was referred
VSO’s, veterans and community members. The keynote address
to California for dental care. Veterans are upset that they are
was Kat Miller, Director of the Nevada Department of Veterans
not being seen at VA and want an explanation.
Services. The ceremony included the University of Nevada, Reno
• Danny commented that he is proud to have been a VA patient Army ROTC (UNR ROTC) Women Cadet Color Guard, a tra-
for 28 years and has had only had one problem with specialty ditional Native blessing, and a Military Enlistment Ceremony.
care.
• Ben said he used My HealtheVet and got immediate appoint- Operation Comfort Warrior (OCW)
ments for audiology & eye care. Clinics are open weekends to The American Legion Operation Comfort Warrior (OCW) in
accommodate the needs of veterans. conjunction with the Department of Nevada American Legion
• A male veteran who needs cataract surgery says he does not Reno Post #1, presented the VASNHCS an OWC grant of $5,700
qualify for Choice since the CBOC is within a few miles of his which was used to purchase comfort and recreation items for
home. The shuttle from Minden to Reno only has three seats hospitalized patients. These items were delivered to the medical
and fill quickly. He sought help from the Patient Advocate and center on March 10, 2016, and presented to Stephanie Torian,
was dissatisfied with the resolution provided. He cannot drive Chief of Voluntary Service.
home from the procedure and has no other transportation.
The veteran is in need of hearing aids but has surpassed the Homeless Shelter
means test threshold. On Thursday, March 10; Mark Walker, Deputy Director VE&E
• A female veteran disclosed that when she needed pacemaker Division; Roscoe Butler, Deputy Director VA&R Division; along
and cataract surgery she was referred to a California VA in- with the System Worth Saving Team (Department of Nevada);
stead of a local community provider. met with Elizabeth Pope, Coordinator/Supervisor Health Care
for Homeless Veteran (HCHV) Program, to discuss their pro-
• David said he has received care at Washington, D.C. VAMC grams and services as well as their plan to eliminate veteran
and that Reno VAMC is the better of the two. homelessness in the Reno area. The HCHV Program assists
• The director would like to discontinue appointment cards as veterans with connecting them to VA and community services.
they frequently provide incorrect information. Services include: Transitional and permanent housing; Medical
care; Mental health referrals; Drop-in services for laundry and
On March 18, 2016, the VASNHCS conducted a separate Wom-
showers; and other resources to improve the quality of life for
en Veterans Town Hall. Ms. Lisa Howard, VASNHCS Direc-
veterans.
tor, opened the town hall and introduced a panel comprised of
Dr. Elizabeth Hill, Associate Chief of Staff, Research; Dr. Amy Currently, there are 187 homeless veterans (11 in the rural area)
Sanguinetti, Associate Chief of Staff, Ambulatory Care; and Dr. in Reno. Please note – this number comes from the most recent
Steven Brilliant, Chief of Staff. Each panel member presented Point-in-Time Count, which means that it is an estimate of the
The American Legion | SYSTEM WORTH SAVING REPORT 8The American Legion
SYSTEM WORTH SAVING
area’s homeless veteran population. Reno has been awarded 450 wait time is 1.24 days.
(Housing and Urban Development) HUD-Veterans Affairs Sup- • Clinic Practice Management (CPM) - The establishment of a
portive Housing (HUD-VASH) vouchers. HUD-VASH vouchers clinic practice management team with reporting structure has
provide permanent housing for chronically homeless veterans been critical to VASNHCS’ success in improving access, qual-
who may have mental illness and substance abuse disorders. The ity of care, and communication. The basic structure includes
program is supported by the VA and HUD. VA staff provide out- a group practice manager (GPM) who reports to the chief of
reach, clinical care and intensive ongoing case management ser- staff (COS), and a weekly CPM model meeting. The GPM,
vices. At this moment the Mayor of Reno, Hillary Schieve, has COS, CPM team, and an ad hoc guest all attend.
not signed onto the Mayors Challenge to End Veteran Home-
lessness. Through the Mayors Challenge mayors and other state Average Wait Time in Days
and local leaders across the country have marshaled federal, lo- Completed Appointments as of 12/30/ 2015:
cal, and nonprofit efforts to end veteran homelessness in their
»» Primary Care: 3.81
communities. Ending veteran homelessness means reaching the
point where there are no veterans sleeping on America’s streets »» Specialty Care: 7.26
and every veteran has access to permanent housing. Should »» Mental Health: .40
veterans become homeless or be at-risk of becoming homeless,
communities will have the capacity to quickly connect them to • My Life, My Story captures veterans’ stories of their life and
the help they need to achieve housing stability. The Department experiences for the inclusion of a 2-page summary in VA’s
of Nevada will be contacting Mayor Schieve’s office to discuss the electronic medical record. The VA Sierra Nevada Health Care
potential of her signing onto the Mayor’s Challenge. System was selected as a pilot location for an excellent proj-
ect to enhance the experience of our veterans and Honor their
Additionally, the team visited a shelter in downtown Reno. Vol- Service. This program allows the clinical team an opportunity
unteers of America has contracted beds within the shelter for to know more about the whole veteran, not just their medical
homeless veterans. The shelter provides housing as well as sup- history.
port services and referrals for permanent housing, health care,
education and career opportunities. Lastly, the VA, service pro- • The facility’s Honors Escort Program provides a formal trans-
viders, and other stakeholders are moving in the direction of fer of a recently deceased veteran from their hospital room to
better coordination in order to properly help homeless veterans the facility morgue. A special gurney with a frame is used and
and their families. To end veteran homeless within a community, an American flag is draped over the gurney. Specially trained
there needs to be consistent communication, accountability and staff and volunteers serve as escorts. Employees and visitors
leadership with all involved. who are in hallways when the procession passes stand to the
side and salute or place a hand over the heart. After the proces-
Vet Center sion, family members are provided the opportunity to assist
with folding the flag. An article describing this unique way of
On Thursday, March 10, Deputy Director Roscoe Butler, VA&R paying tribute to veterans was featured in the October–No-
Division Deputy Director Mark Walker, Vocational Rehabilita- vember 2014 issue of VAnguard, a VA employee magazine.
tion and Employment (VR&E), and the Department of Nevada
System Worth Saving Team met with Scott Drew who Team • VA Voices uses the power of storytelling to build connections
Lead at the Reno Vet Center. Mr. Drew apprised the group on between employees, veterans, and the community. These rela-
the role of the Reno Vet Center and gave a tour of the facility as tionships foster empathy, build trust, and create effective part-
well as the Vet Center Mobile Van. nerships in healthcare. During the VA Voices experience, em-
ployees hear personal stories from the local leadership team,
Best Practices participate in team building activities, and learn strategies to
share their story to build stronger connections in support of
The VASNHCS identified the following best practices: the mission of serving veterans.
• Access Best Practice – In early 2014, the average wait time for
a first primary care appointment was 42 days. A Rapid Process Conclusion
Improvement Workshop was held, and a robust new enrollee 1. Staffing: Staffing at VASNHCS remains a challenge as they
patient process was developed. As a direct result of this effort, compete for scarce healthcare resources. Nevada is in the
96% of new veteran enrollees are seen on the same day. The process of opening a medical school in Las Vegas that may
remaining four percent had average wait time was down to 3 serve as a source of future applicants. However, the VA as a
days within just two months of implementation. The current
The American Legion | SYSTEM WORTH SAVING REPORT 9The American Legion
SYSTEM WORTH SAVING
whole continues to struggle to fill vacant positions with ex- minor projects underway for the next several fiscal years to
perienced staff. Over 11% of VASNHCS current workforce redesign inpatient units and the OR. As referenced above,
is eligible to retire; many eligible employees fill leadership additional outpatient sites of care are in leasing.
roles or other critical positions. For example, one of the 8. Choice First/Tri-West: Communication with Tri-West is
three members of VASNHCS executive leadership is eligible the greatest challenge for both veterans and VA staff. Sched-
to retire now. Also, 46% of their Nurse Managers and 21% uling takes more than five days as directed by contract, and
of their physician leaders were eligible for immediate retire- most community appointments are made outside the 30-day
ment in fiscal 2015. time frame. Patients are scheduled with the wrong specialty
2. Centralization of HR: When asked if consolidation of HR providers and sometimes with no input from the veteran.
would have a positive or adverse effect on the hiring and re- Secondary Authorization requests (SARs), which are re-
cruitment process, the SWS team was advised that it would quests for extensions or additional treatment, do not get to
be a disaster and would take away any local control and the VASNHCS within two days as directed by contract. Cur-
oversight from medical center Directors. The centralization rently, they are down to a 10-day delay, but at the time of our
of Prosthetics and Procurement Services nationwide was site visit, Tri-West was months behind. Continuity of care is
cited as an example of unsuccessful implementation. negatively impacted when documents are not returned from
3. The catchment area is large and very rural: The catchment outside providers within the contracted time frame.
area for the VASNHCS is the 2nd largest rural district in the 9. Weather (wintertime): Winter weather is known to se-
country. It is comprised of 110,000 square miles of territory verely hamper or shut down commutes via Donner Pass and
in northern Nevada and California. Veteran populations are Summit, in the Sierra Nevada Mountains between Reno and
scattered across a multitude of small rural towns in 20 coun- Northern California. This can and does affect a large per-
ties. centage of the veterans who travel to the main campus for
4. Considerable driving distance for veteran: Many veterans care.
travel upwards of 3.5 hours one-way to access care at the 10. Signage: During a tour of the medical center, a veteran
VASNCHS. The furthest eastern edge of their catchment pointed out issues with the directional signage posted by
area, for example, is 253 miles away on I-80. They have the elevators throughout the medical center. Concern was
placed CBOCs in many sectors, including a part-time out- raised that the signage was difficult to follow and did not
reach clinic. VASNHCS opened another primary care site in provide veterans with a positive experience.
Reno and will open an additional PC site in North Valleys 11. Medical Record Documentation for Non-VA Care: Com-
Reno in fiscal 2016. munity providers do not have federal level encryption for
5. Communication: The rural nature of the catchment area records to be transmitted electronically, which has delayed
in Nevada makes for limited communication options with payments to the provider. When it was explained that there
regards to notifying veterans. Reno itself has a tiny media is a national proposal to uncouple the medical record from
market. There are only three Network Television stations the payment process, the SWS team was informed that if that
and one regional newspaper. The proliferation of web-based happens, VA may never get the records. It was furthered
platforms such as social networking have expanded options explained that by decoupling the medical record from the
somewhat, but many older veterans do not utilize these re- payment, VHA will have no leverage over the provider.
sources. 12. Beneficiary Travel: When the VASNHCS transfers an in-
6. Lack of in-house resources: During the Clinical Service patient to another VA Medical Center (VAMC) for a higher
Chiefs meeting with The American Legion, the topic of level of care, the receiving VAMC routinely discharges the
inpatient beds was discussed. VASNHCS has a multi-year patient to home afterwards. The veteran is responsible for
Value Stream addressing inpatient bed flow and monitors providing their transportation home if they do not meet
the cumulative census to identify opportunities to increase the eligibility requirements for beneficiary travel. This has
the bed count. VASNHCS has six beds that could be acti- posed a challenge for veterans who are referred to a distant
vated that are also being considered for memory care needs. VAMC.
7. Space: Space is a challenge as the VASNHCS is landlocked
in a residential neighborhood with insufficient parking.
Recommendations
VASNHCS is in design for a Major Project, which will pro- 1. Signage: The VASNHCS Executive Leadership should up-
vide for modern outpatient delivery. There are also many date the directional signage throughout the medical center
The American Legion | SYSTEM WORTH SAVING REPORT 10The American Legion
SYSTEM WORTH SAVING
to ensure it is easily understood, so that veterans and visitors
will leave the center with a positive VA experience.
2. Medical Record Documentation for Non-VA Care: Since
VA nationally has decoupled the medical record documen-
tation from the payment process, nationwide VA must en-
sure the time requirements specified in the national con-
tract are being met. When the requirements are not met, VA
must execute its contractual option to hold the contractor
accountable.
3. Beneficiary Travel: The American Legion Department of
Nevada should work with the VASNHCS in drafting a leg-
islative resolution to authorize VA to pay an inpatient veter-
ans’ beneficiary travel expenses when transferred from one
VAMC to another, if upon completion of the medical care if;
a. The veteran is discharged to home as an outpatient, and
b. The veteran is not otherwise eligible, and thus finan-
cially unable to pay the cost of travel to return home.
The American Legion | SYSTEM WORTH SAVING REPORT 11You can also read