Ultrasonographic Evaluation of Nerves and Their Association with Veins in the Lower Limbs
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
pISSN 1598-6756 eISSN 2765-5628
Annals of Phlebology Vol. 19, No. 1, April, 2021
□ Review Article □
https://doi.org/10.37923/phle.2021.19.1.1
Ultrasonographic Evaluation of Nerves and Their Association with
Veins in the Lower Limbs
1
Division of Vascular Surgery, Department of Surgery, Asan Medical Center, University of Ulsan College of
2
Medicine, Seoul, Korea, Department of Surgery, Stony Brook University Medical Center, New York, USA
Hyangkyoung Kim, M.D., Ph.D.1 and Nicos Labropoulos, Ph.D.2
Peripheral nerves of the lower extremities are often encoun- the outcome immediately, and can be used for follow-up.
tered during preoperative venous ultrasound examination or An appropriate scanning technique is essential for accurate
venous procedures. Nerves are not a region of interest in anatomical confirmation of nerves using US. In this review,
routine practice, but basic knowledge of their course and
we present a brief description of the anatomy of peripheral
sonographic appearance is helpful in evaluating nonsaphenous
reflux or avoiding nerve damage during surgery. Knowledge nerves, their ultrasonographic appearance, and clinical
of the anatomy and scanning technique is required to significance in venous procedures.
accurately detect the location of nerves. In this review, we
present a brief description of the ultrasonographic anatomy MAIN TEXT
of peripheral nerves and the clinical significance of venous
interventions. (Ann Phlebology 2021;19:1-8)
Commonly encountered peripheral nerves of the lower
Key Words: Nerve, Ultrasonography, Venous procedure, extremity in routine clinical practice are the femoral, sciatic,
Venous reflux, Anatomy tibial, common peroneal, sural, and saphenous nerves.
Nonsaphenous reflux is often associated with sciatic or
tibial nerve vein reflux. The common peroneal, sural, and
INTRODUCTION saphenous nerves can be damaged by venous interventions.
The femoral and sciatic nerves can be easily located during
Peripheral nerves of the lower extremities are often encoun- scanning, while blocks of these nerves are performed with
tered during preoperative venous ultrasound examination or US guidance. Injury to the lower extremity nerves can lead
venous procedures. Nerves are not a region of interest in to several complications, such as paresthesia (hypoesthesia-
routine practice for most vascular specialists. However, basic numbness, hyperesthesia – pain), and reduced or even
knowledge of their course and sonographic appearance is abolished motor function.
helpful in evaluating venous pathology and, more importantly, 1) Instrumentation and appearance at US
to avoid nerve damage during venous interventions. Ultrasound
(US) examination is increasingly being used for imaging The peripheral nerves of the lower extremity can be
peripheral nerves. A previous study showed greater sen- scanned using a high-frequency linear array transducer.
sitivity in the detection of peripheral nerve pathology with US Superficial nerves may be scanned with a 12∼17 MHz
than with magnetic resonance imaging (93% vs. 67%) (1). linear-array transducer, while deeper nerves may be scanned
Furthermore, US is noninvasive, well-tolerated by patients, with a 5∼12 MHz transducer. A convex transducer may be
easily repeatable, can guide venous interventions and assess used when scanning the posterior thigh in patients with
obesity.
Nerves are composed of bundled fascicles, and each fiber
is surrounded by the endoneurium (Fig. 1). Each fascicle
Corresponding author:Nicos Labropoulos, Stony Brook, New York
11794, USA, Department of Surgery, Stony is held together and surrounded by the perineurium. The
Brook University Medical Center epineurium is a dense sheath of connective tissue that
Tel: 631-444-2683, Fax: 631-444-8824 covers the outside of the nerve. Nerves often travel along
E-mail: nlabrop@yahoo.com
1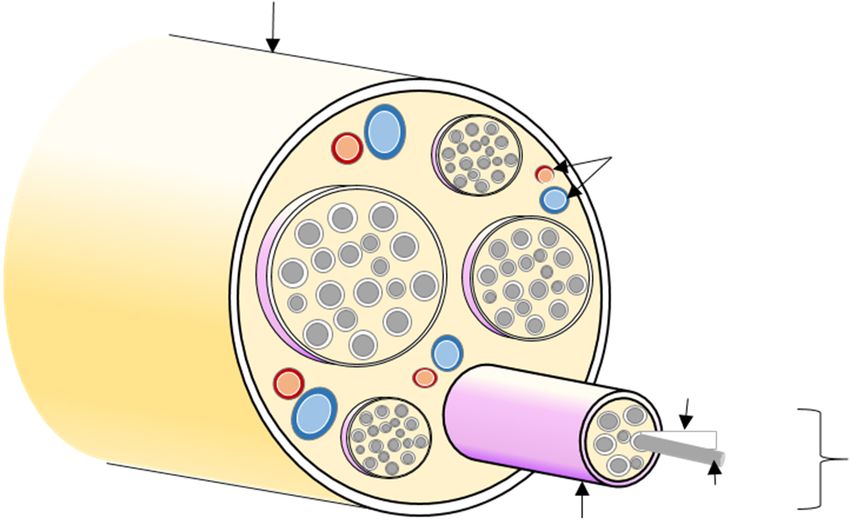
2 Annals of Phlebology:Vol. 19, No. 1, April, 2021
the blood vessels. redundant blood supply from the iliac branch of the iliolumbar
The structure of a nerve has a characteristic “honeycomb” artery, deep circumflex iliac artery, and lateral circumflex
appearance on US in the short axis, representing an unin- femoral artery in the femoral triangle (2). Femoral nerve
terrupted fascicular pattern (Fig. 2). The epineurium, made injuries manifest as an isolated motor or sensory deficit (3).
of dense collagen, appears bright on US, whereas the peri- Physical signs may include paresis or flaccid paralysis of
neurium, made of fat cells, appears dark. As nerves are not the quadriceps muscle, diminished or absent extension of the
compressible, higher pressure can be applied with the knee, and reduced or absent patellar reflex. Sensory distur-
transducer to improve imaging when necessary. Tendons bances, including numbness, paresthesia, or hyperesthesia, are
have a fibrillar pattern of parallel hyperechoic lines, such present along the course of the saphenous nerve, over the
as nerves. However, the nerves are very close to the vessels anteromedial aspect of the thigh, and the inner aspect of the
and slide away during compression. calf down to the medial malleolus.
2) Femoral nerve
The femoral nerve is most easily seen within the femoral
triangle lateral to the common or superficial femoral artery
(Fig. 3A). The femoral nerve receives nerve fibers from L2
to L4 and runs between the iliacus and psoas major
muscles. The femoral nerve exits the pelvis into the anterior
thigh compartment. Approximately 2∼4 cm below the
inguinal ligament, the femoral nerve then divides into the
anterior and posterior divisions. It terminates as the saphenous
nerve. Femoral nerve injury is most commonly caused by
traction injury, direct surgical trauma, or compression
injury. Ischemic injury is less common because it receives
Fig. 3. Anatomy (A) and ultrasound image (B) of the femoral
nerve (FN). The FN is found lateral to the common femoral
artery (CFA) (B-left). The nerve is smaller than the CFA and the
artery is smaller than the adjacent common femoral vein (CFV).
Compression with the transducer occludes the CFV leaving the
FN and CFA (B-right). Femoral nerve block is administered with
ultrasound guidance, which is easy to perform and has a low
Fig. 1. Illustration of the anatomy of a typical peripheral nerve. risk of complications.
Fig. 2. Ultrasound appearance of the
nerve. (A) Honeycomb appearance in
the short axis. (B) Hypoechoic struc-
ture that runs longitudinally with the
hyperechoic cover (epineurium) in the
long axis.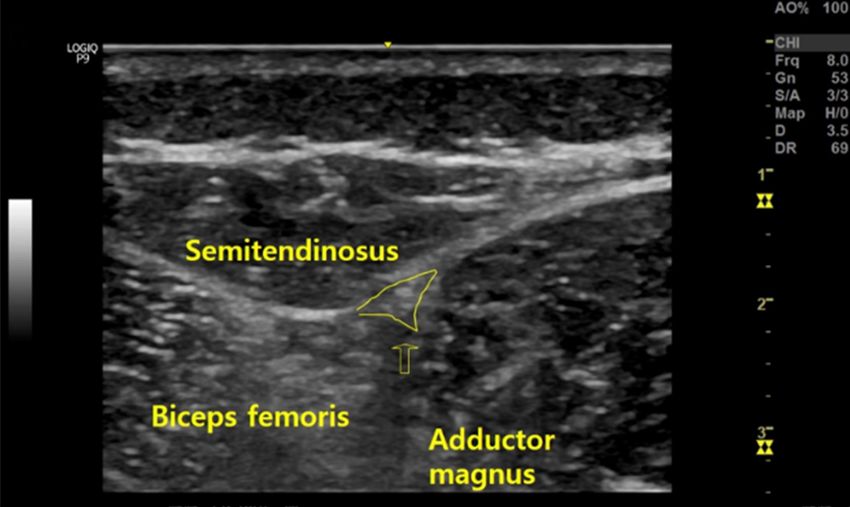
Hyangkyoung Kim and Nicos Labropoulos:Ultrasonographic Evaluation of Leg Nerves 3
A US examination of the femoral nerve was performed
3) Lateral femoral cutaneous nerve (lateral cutaneous
in the supine position, and the femoral vessels were used
nerve of the thigh)
as important anatomic landmarks for locating the femoral
nerve (Fig. 3B). The femoral nerve is often visualized The lateral femoral cutaneous nerve arises from the
during the femoral nerve block. The femoral nerve block dorsal division of L2 and L3. It emerges from the lateral
is usually performed for surgery on the anterior aspect of border of the psoas major approximately at its middle and
the thigh and superficial surgery on the medial aspect of crosses the iliacus muscle obliquely toward the anterior
the leg below the knee, such as saphenous vein stripping superior iliac spine. It then passes under the inguinal
or harvest, femoral endarterectomy, and groin lymph node ligament, through the lacuna musculorum, and then over the
excision. sartorius muscle into the thigh, where it divides into an
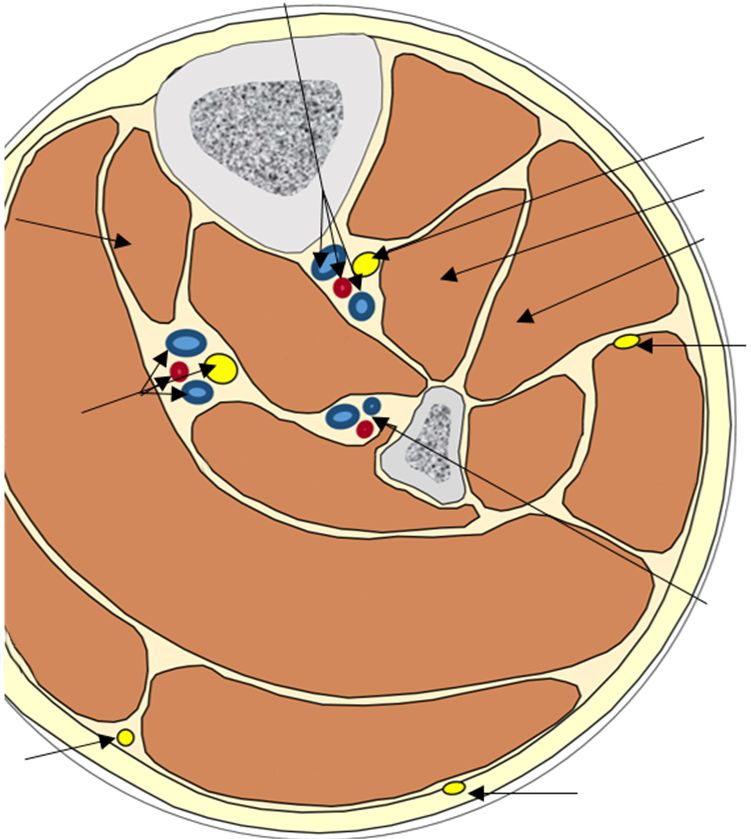
Fig. 4. Anatomy (A) and ultrasound image (B) of the sciatic nerve. The sciatic nerve vein reflux can be documented as a dilated
vein with significant reflux along the sciatic nerve, when the patients have varicosities behind the thigh or knee (C).
Fig. 5. Anatomy (A) and ultrasound image (B) of the tibial nerve (arrow).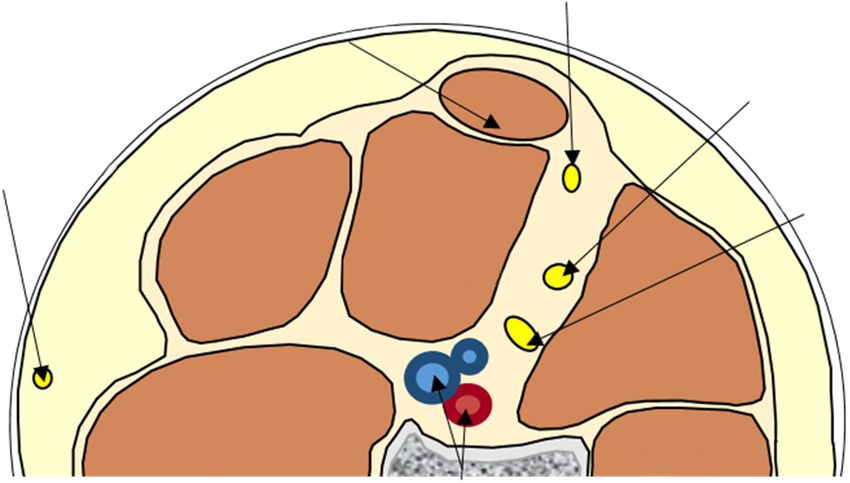
4 Annals of Phlebology:Vol. 19, No. 1, April, 2021
anterior and a posterior branch (Fig. 3A). It can be injured injuries occur less commonly in the midthighs. Symptoms
during ligation, stripping, or avulsion. It supplies sensation and signs of sciatic nerve injury are weakness of the
to the skin of the thigh and causes meralgia paresthetica, affected muscles, including the hamstrings. Sensory loss
characterized by tingling, numbness, and burning pain in the involves the entire peroneal, tibial, and sural territories.
outer thigh when injured. The sciatic nerve can be observed when a nonsaphenous
vein reflux is suspected, which is defined as the reflux in
4) Sciatic nerve
the superficial veins that are not part of the great or small
The sciatic nerve is the longest and thickest peripheral saphenous systems (Fig. 4C) (6). The sciatic nerve vein
nerve in the body. It can reach a diameter of up to 2 cm. insufficiency was found in 10% of the cases of nonsa-
It is formed by the L4∼S3 nerve roots and exits the lesser phenous superficial vein reflux (7). In these patients, the
pelvis via the greater sciatic foramen, emerging from most common presenting symptom was pain along the
beneath the piriformis muscle in most cases with some sciatic nerve that was worse while sitting, usually improved
anatomical variants. At this level, it is difficult to locate the with walking and standing, and was reproducible with point
nerve with US (4). Below the piriformis muscle, the sciatic pressure in the area of tenderness where varices disappear
nerve courses posteriorly around the posterior acetabulum (8,9). Similar to the saphenous reflux test, the sciatic nerve
and beneath the gluteus maximus muscle. The sciatic nerve vein is examined in a standing position through distal
descends posteriorly in the fascial plane deep to the biceps augmentation. Sciatic nerve vein reflux can be treated with
femoris and superficial to the adductor magnus muscle, and phlebectomy or ultrasound-guided sclerotherapy with excellent
it is surrounded by a large amount of connective and results (8,10). A more extensive surgical approach should
adipose tissue (5). In the mid-thigh, it is usually visible be avoided because of the high risk of nerve injury (9).
through US in the groove between the semimembranosus
5) Tibial nerve
and biceps femoris muscles (Fig. 4A, B). At the apex of
the popliteal fossa, the sciatic nerve is usually divided into The tibial nerve is the thicker terminal branch of the sciatic
the peroneal and tibial nerves. When it is difficult to nerve and predominantly contains fibers from the L5∼S3
identify, the tibial nerve can be located first and then tracked roots. The tibial nerve travels through the middle of the
proximally along its course. However, the bifurcation level popliteal fossa, along the dorsal surface of the popliteus
is variable (4). muscle, between the popliteal vessels surrounded by abundant
Trauma, fracture, or hip surgery are the most common connective and adipose tissue (Fig. 5A). It then passes
causes of sciatic nerve injuries. Sciatic nerve injury between the two heads of the gastrocnemius muscle. The
commonly occurs in patients with lower weight on hard tibial nerve is sometimes referred to as the posterior tibial
tables during surgery. Stretch, compression, and ischemia nerve at a level below the characteristic fibrous arch of the
are the primary mechanisms. Injury to the nerve can occur soleus muscle. It is accompanied by the posterior tibial
in the frog leg position in vertebral surgeries and in artery and vein, initially on the anterior side, but more
prolonged surgeries in the sitting position. Sciatic nerve distally medial. Thereafter, the term tibial nerve is used
Fig. 6. Female patient with 2 preg-
nancies presented with tingling sen-
sation and posterior calf varico-
sities. She had sciatic (A) and tibial
nerve varicose veins (B). The yellow
line indicates the width of the sci-
atic nerve. The tibial nerve is in
contact with the popliteal vein seen
below it.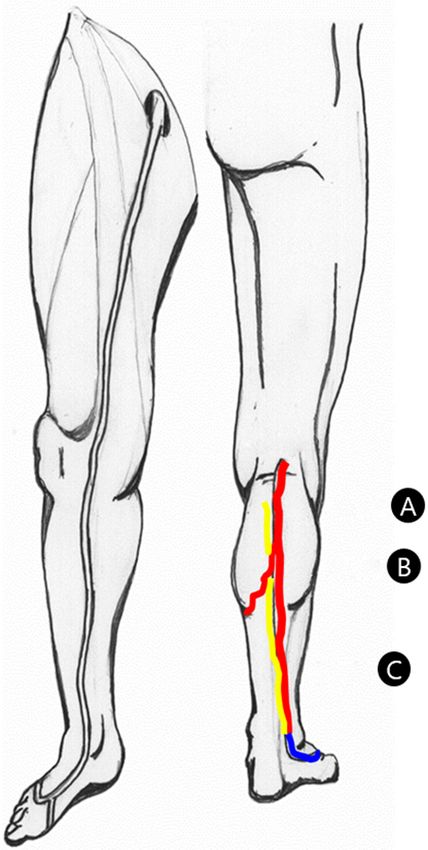
Hyangkyoung Kim and Nicos Labropoulos:Ultrasonographic Evaluation of Leg Nerves 5
throughout the course of the nerve. The tibial nerve gives landmark, the tibial nerve below the knee can be identified
off an anastomotic branch to form the sural nerve. slightly medial to the long axis of the fibula in the
Tibial nerve injury may occur due to compression below transverse view.
the flexor retinaculum of the ankle (tarsal tunnel syndrome), The tibial nerve can be observed if a nonsaphenous vein
trauma, posterior dislocation of the knee, and fracture. reflux is suspected at the posteromedial calf. The prevalence
Injury to the tibial nerve can cause motor and sensory of tibial nerve vein reflux is reported to be lower than that
deficits in the calf and foot, depending on the site of of sciatic nerve vein reflux (8). Reflux in the tibial nerve
involvement. veins has been observed together with that of the sciatic
Because of its large diameter, linear course, and accom- nerve (Fig. 6), and symptoms from compression of the
panying neurovascular bundle, the tibial nerve is an easy nerve have been reported alone or in combination with the
target for US assessment. On US, the tibial nerve accom- popliteal vein compression (11).
panies the popliteal vein through the popliteal fossa and
6) Common peroneal nerve (CPN)
then continues distally within the posterior tibial neuro-
vascular bundle (Fig. 5B). Using the tibial vessel as a The CPN is the smaller terminal branch of the sciatic
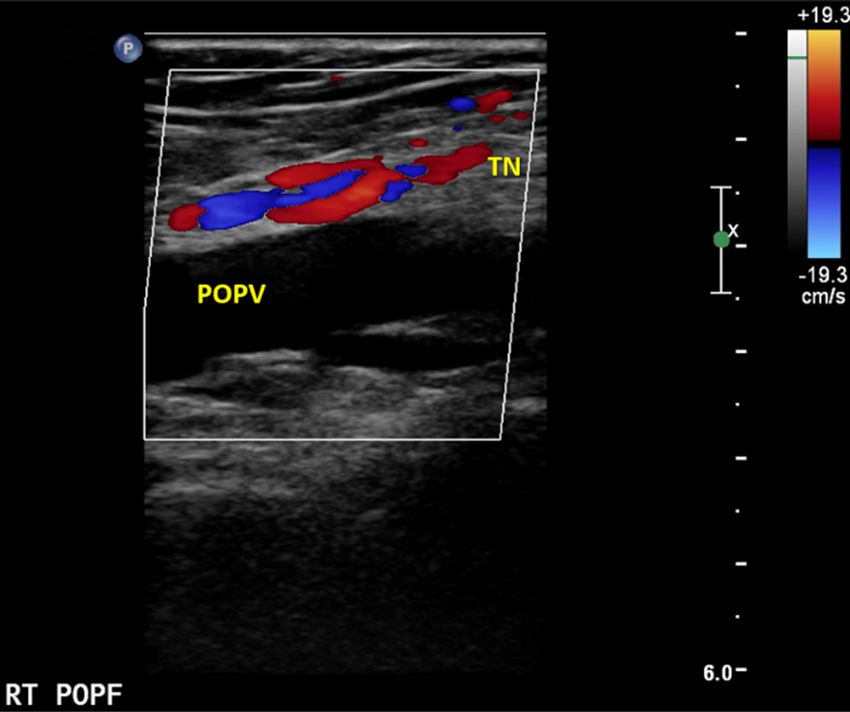
Fig. 7. Anatomy at the popliteal fossa (A) and upper calf (B), and ultrasound image (C) of the common peroneal nerve (CPN)
and the tibial nerve (TN). The CPN and TN are close to the vein of popliteal fossa (VPOPF) at its union with the popliteal
vein (POPV). The nerves are seen just below their branching off from the sciatic nerve. Further down, the tibial nerve lies over
the POPV. The CPN will run lateral and split into superficial and deep peroneal nerves. In this patient the VPOPF was very
dilated and had reflux. Because of its proximity to the nerves, ligation of this vein could lead to potential nerve damage.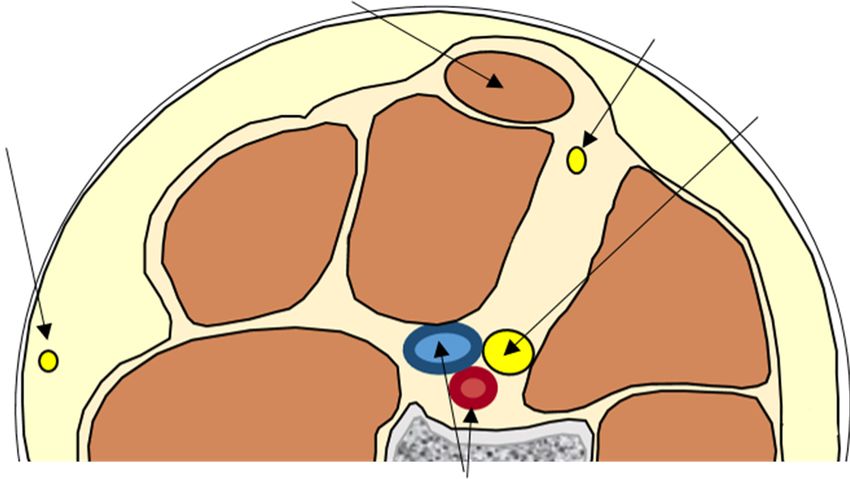
6 Annals of Phlebology:Vol. 19, No. 1, April, 2021
nerve and originates from the L4∼S2 nerve roots. In the The sural nerve is well visualized on US examination
popliteal fossa, it runs deep to the biceps femoris and then because of its superficial course. Using probe compression
descends obliquely around the fibular head (Fig. 7A). It of the SSV, the sural nerve can be visualized in the
courses in the subcutaneous fat and enters the fibular tunnel, subcutaneous fat lateral to the SSV.
formed between the origin of the peroneus longus muscle Because of its proximity to the SSV, it is at risk during
and the fibular head. The CPN wraps around the proximal harvest or ablation of the SSV, as well as dissection of the
fibula and then trifurcates into the deep peroneal nerve, SPJ. Ablation of the SSV may cause sural nerve injury in
superficial peroneal nerve (SPN), and recurrent articular up to 4% of patients (18). When the sural nerve is injured,
branch (Fig. 7B). The trifurcation most commonly occurs burning pain and sensory alterations, including hyperesthesia
at or distal to the fibular neck. The deep peroneal nerve or paresthesia over the posterolateral aspect of the distal
continues distally, accompanied by the anterior tibial artery third of the leg and lateral aspect of the foot, heel, and
on the interosseous membrane. The SPN descends in the ankle. Sural nerve injury from ablation procedures can be
lateral compartment, between the peroneus longus and reduced by using a tumescent solution or nonthermal technique
brevis muscles in approximately 70% of cases or in the (19,20).
anterior compartment in the remaining cases (12).
8) Saphenous nerve
Common peroneal neuropathy is the most common
mononeuropathy in the lower extremity (13), which may The saphenous nerve is a terminal cutaneous branch of
occur due to nerve injury following the surgical removal of the posterior division of the femoral nerve, originating from
the small saphenous vein (SSV) in cases of high location the L2∼L4 nerve roots. It provides pure sensory innervation
of the saphenopopliteal junction (SPJ) above the popliteal to the anterior and medial aspect of the distal thigh, as well
skin crease or having a more lateral course (Fig. 7C) (14). as the anteromedial knee and medial lower leg. The
Injury of CPN in patients with reflux in the vein of the
popliteal fossa can occur during ligation as this vein unites
with the popliteal vein at a higher level and lateral to the
SPJ (15). Furthermore, because the CPN courses around the
neck of the fibula distally, injury could occur after
phlebectomy in that area. Injuries to the CPN can cause
numbness, tingling, pain, extensor weakness, and a gait
problem called foot drop. Entrapment of the SPN is not
uncommon and it can cause pain in the sensory distribution
of the dorsum of the foot with or without paresthesia (16).
The SPN block is useful when edema or infection
contraindicate a more distal ankle block.
7) Sural nerve
The sural nerve is a pure sensory nerve that is formed
by the union of the medial sural cutaneous nerve (which
originates from the tibial nerve at the popliteal fossa) and
the lateral sural cutaneous nerve (which originates from the
CPN). It provides sensory innervation to the posterolateral
aspects of the distal third of the lower leg and the lateral Fig. 8. Ultrasound image of a female patient with small saphenous
aspect of the ankle and foot. The sural nerve usually vein (SSV) reflux. The patient had SSV reflux from the
descends in the posterior midline between the two heads of saphenopopliteal junction (SPJ) to the lateral malleolus (red
color in the drawing) with long duration as seen in the upper
the gastrocnemius muscle and penetrates the deep fascia in
calf (A). The sural nerve (yellow line in the drawing) is not
the proximal calf, with a high rate of anatomical variation close to the SSV in the mid-calf (B) but is in contact with
(17). It runs alongside the SSV in the subcutaneous fat of the SSV at the lower calf (yellow arrow) (C). The perimeter
the posterior calf (Fig. 8). of the nerve has been marked with a yellow dashed line.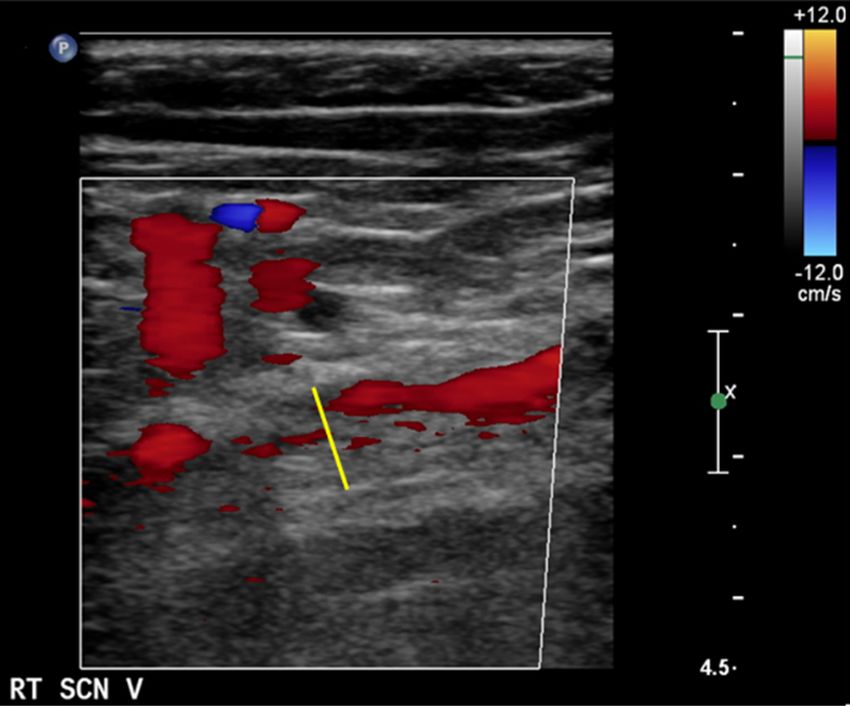
Hyangkyoung Kim and Nicos Labropoulos:Ultrasonographic Evaluation of Leg Nerves 7
Fig. 9. Ultrasound image of the sa-
phenous nerve at the lower third of
the calf in contact with the great
saphenous vein. (A) Cross sectional
view, (B) longitudinal view.
saphenous nerve descends in the subfascial plane of the ultrasound and MRI. Neurology. 2013;80(18):1634-1640.
femoral canal and accompanies the superficial femoral 2) Boontje AH, Haaxma R. Femoral neuropathy as a com-
artery. It then courses from the femoral vessels penetrating plication of aortic surgery. J Cardiovasc Surg (Torino).
1987;28(3):286-289.
the superficial fascia toward the medial subcutaneous tissue
3) Celebrezze JP, Jr., Pidala MJ, Porter JA, Slezak FA.
and joins the greater saphenous vein approximately 10 cm
Femoral neuropathy: an infrequently reported postoperative
proximal to the knee. Below the level of the knee, the
complication. Report of four cases. Dis Colon Rectum.
saphenous nerve descends along the medial border of the 2000;43(3):419-422.
tibia, accompanying the greater saphenous vein. 4) Yablon CM, Hammer MR, Morag Y, Brandon CJ, Fessell
A US examination of the saphenous nerve is performed DP, Jacobson JA. US of the Peripheral Nerves of the
in the supine position with slight flexion and external Lower Extremity: A Landmark Approach. Radiographics
rotation of the knee in the same position as when scanning : a review publication of the Radiological Society of North
the lower extremity veins. At the joining point 10 cm America, Inc. 2016;36(2):464-478.
5) Kowalska B, Sudoł-Szopińska I. Normal and sonographic
proximal to the knee, the saphenous nerve can be identified
anatomy of selected peripheral nerves. Part III: Peripheral
by compressing the greater saphenous vein as a landmark
nerves of the lower limb. Journal of Ultrasonography.
(Fig. 9).
2012;12(49):148-163.
The saphenous nerve can be injured during thermal or 6) Labropoulos N, Tiongson J, Pryor L, et al. Nonsaphenous
surgical saphenous vein procedures or saphenous vein superficial vein reflux. Journal of Vascular Surgery.
harvesting involving the medial knee, because of its 2001;34(5):872-877.
proximity to the greater saphenous vein (15,21). When 7) Labropoulos N, Tiongson J, Pryor L, et al. Nonsaphenous
injured, patients present with saphenous neuropathy with superficial vein reflux. J Vasc Surg. 2001;34(5):872-877.
paresthesia or numbness of the medial calf or medial foot 8) Labropoulos N, Tassiopoulos AK, Gasparis AP, Phillips B,
Pappas PJ. Veins along the course of the sciatic nerve. J
depending on the level of injury (15,22).
Vasc Surg. 2009;49(3):690-696.
9) Ricci S. Ultrasound Observation of the Sciatic Nerve and its
CONCLUSION Branches at the Popliteal Fossa: Always Visible, Never Seen.
European Journal of Vascular and Endovascular Surgery.
Most nerves run together with vessels having a standard 2005;30(6):659-663.
location with only a few important variations and are 10) Ricci S, Georgiev M, Jawien A, Zamboni P. Sciatic Nerve
therefore easy to identify. Vascular specialists who are Varices. European Journal of Vascular and Endovascular
accustomed to the ultrasonographic appearance of vessels Surgery. 2005;29(1):83-87.
need to become familiar with the nerves. This will help in 11) Sanchez JE, Conkling N, Labropoulos N. Compression
syndromes of the popliteal neurovascular bundle due to
treatment planning and reducing the complication rates.
Baker cyst. J Vasc Surg. 2011;54(6):1821-1829.
12) Relvas-Silva M, Pinho AR, Lopes JG, et al. Anatomy of the
REFERENCES superficial peroneal nerve: Can we predict nerve location
and minimize iatrogenic lesion? Morphologie. 2021.
1) Zaidman CM, Seelig MJ, Baker JC, Mackinnon SE, Pestronk 13) Donovan A, Rosenberg ZS, Cavalcanti CF. MR imaging
A. Detection of peripheral nerve pathology: comparison of of entrapment neuropathies of the lower extremity. Part 2.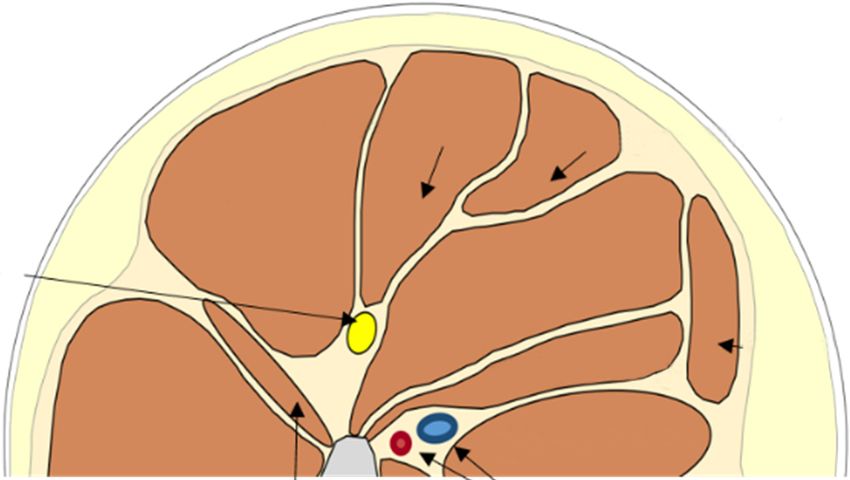
8 Annals of Phlebology:Vol. 19, No. 1, April, 2021
The knee, leg, ankle, and foot. Radiographics: a review saphenous vein: efficacy and complications. J Vasc Surg.
publication of the Radiological Society of North America, 2007;45(4):795-801; discussion 801-793.
Inc. 2010;30(4):1001-1019. 19) Baccellieri D, Apruzzi L, Ardita V, et al. Early results of
14) Atkin GK, Round T, Vattipally VR, Das SK. Common mechanochemical ablation for small saphenous vein
peroneal nerve injury as a complication of short saphenous incompetency using 2% polidocanol. J Vasc Surg Venous
vein surgery. Phlebology. 2007;22(1):3-7. Lymphat Disord. 2020.
15) Sam RC, Silverman SH, Bradbury AW. Nerve injuries and 20) Min RJ, Khilnani N, Zimmet SE. Endovenous laser
varicose vein surgery. Eur J Vasc Endovasc Surg. 2004; treatment of saphenous vein reflux: long-term results. J
27(2):113-120. Vasc Interv Radiol. 2003;14(8):991-996.
16) Allam AE, Mansour ER. Superficial Peroneal Nerve Block. 21) Moawad MR, Masannat YA, Alhamdani A, Gibbons CP.
In: StatPearls. Treasure Island (FL): StatPearls Publishing Nerve injury in lower limb vascular surgery. Surgeon.
Copyright © 2021, StatPearls Publishing LLC.; 2021. 2008;6(1):32-35.
17) Pyun SB, Kwon HK. The effect of anatomical variation 22) Milone M, Di Minno MN, Maietta P, Shatalova O,
of the sural nerve on nerve conduction studies. Am J Phys Musella M, Milone F. Great saphenous vein stripping and
Med Rehabil. 2008;87(6):438-442. nerve injury: the role of stripping direction. Int Angiol.
18) Gibson KD, Ferris BL, Polissar N, Neradilek B, Pepper 2015;34(3):238-242.
D. Endovenous laser treatment of the small [corrected]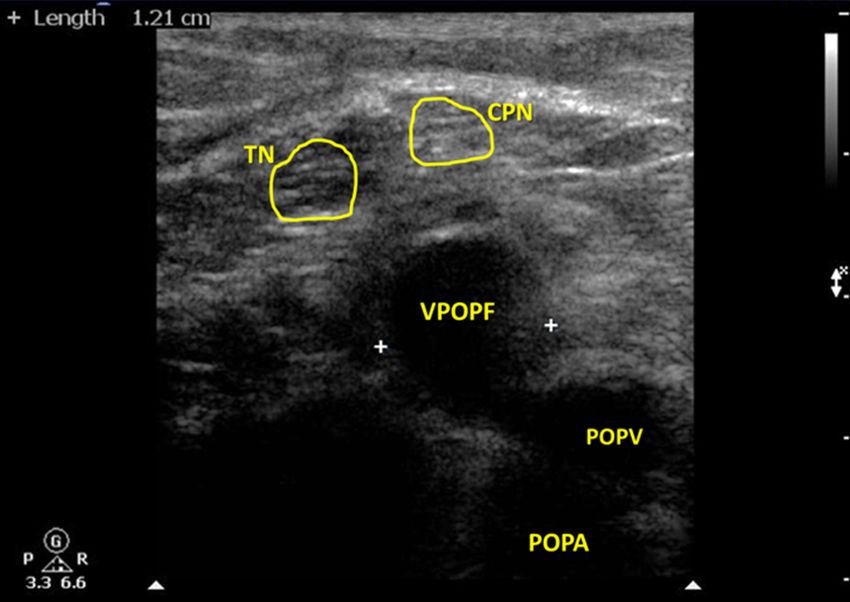
You can also read

















































