The Senior Patient Navigator Program
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

UMASS MEDICAL SCHOOL
The Senior Patient Navigator Program
Building Clinical Skills & Supporting Seniors
Mark Fitzgerald, UMMS 2013
Gary P. Blanchard, MD
Colleen J. Burnham, MBA
2012-2013
STUDENT NAVIGATOR RESOURCE
MANUAL
UMMS Senior Patient Navigator Program© is supported by the Donald W. Reynolds Foundation and sponsored
by the University of Massachusetts Medical School Advancing Geriatrics Education (AGE) initiative
Table of Contents
PROGRAM HISTORY/BACKGROUND/RATIONALE 4
PROGRAM FACULTY AND ADMINISTRATION 6
TRAINING TO BECOME A STUDENT NAVIGATOR 7
TIMELINE OF A NAVIGATOR SESSION 8
HELPFUL TIPS FOR SUCCESSFUL NAVIGATION FROM EXPERT NAVIGATORS 10
OVERALL TIMELINE FOR STUDENT NAVIGATOR TRAINING 11
NOTE-TAKING TEMPLATE 12
NOTE-TAKING TEMPLATE SAMPLE 14
MODULE I: COMMUNICATING WITH OLDER ADULTS 16
Program Objectives 16
Medical, Nursing, Pharmacy, and Interprofessional Geriatric Competencies 17
Module I: Important Concepts 18
Module I: Clinical Pearls of Communication 19
Module I: Guiding Questions 21
Module I: Reading and Reference List 22
MODULE II: GERIATRIC PRESCRIBING 23
Program Objectives 23
Medical, Nursing, Pharmacy, and Interprofessional Geriatric Competencies 24
Module II: Important Concepts 25
Module II: Guiding Questions 26
Module II: Reading and Reference List 27
MODULE III: GERIATRIC SPECIALTY-SPECIFIC CONSIDERATIONS 28
Program Objectives 28
Medical, Nursing, Pharmacy, and Interprofessional Geriatric Competencies 29
Module III: Cardiology Clinical Pearls 31
Module III: Orthopedic Clinical Pearls 33
A Brief Introduction to Third Year & The Hospitalized Patient 35
Module III: Guiding Questions 36
Module III: Reading and Reference List 37
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e |2
MODULE IV: END-OF-LIFE CARE AND CONSIDERATIONS 38
Program Objectives 38
Medical, Nursing, Pharmacy, and Interprofessional Geriatric Competencies 39
Module IV: Guiding Questions 40
Module IV: “On Breaking Bad News and Speaking of Death” 41
Module IV: Reading and Reference List 45
RESOURCES OVERVIEW 46
Program Objectives Addressed in Resources Overview 46
INDEX 47
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e |3
P ROGRAM H ISTORY
The Senior Patient Navigator Program is an original University of Massachusetts Medical School (UMMS)
geriatric curriculum targeting first-year and second-year medical students, graduate nursing students, pharmacy
students. The brainchild of Bonnie Vallie (Class of 2011), the program’s goal was to afford medical students an early
clinical exposure to geriatricians and other specialists who see older patients in the ambulatory setting.
Bonnie Vallie formulated the idea of the Senior Patient Navigator Program during the 2008-2009 academic year. The
pilot of the program took place the following academic year as an extra-curricular student activity for the School of
Medicine implemented and facilitated by Romulo Celli (Class of 2012). Originally based out of the cardiology clinic
on the School of Medicine’s University campus, older adult patients with upcoming cardiology appointments could
call a phone line and request a preclinical medical student to accompany them into their appointments. The students
would transcribe important notes during the visit and debrief with the patient after the appointment. The program was
found to have mutual benefit for students and patients, and received positive feedback from students, physicians,
patients, and caregivers.
While successful, it was felt the program had untapped potential and was not entirely self-sustaining long term. Mark
Fitzgerald (Class of 2013) reengineered the program from the ground up and a new iteration of the Navigator
Program was rolled out during the 2010-2011 academic year. Rather than being clinic based, the program now
centered on pairing each participating student with an older adult patient under the care of a geriatrician. The student
would attend the patient’s appointments across multiple sub-specialties in addition to their primary care appointments,
providing the student with a longitudinal clinical experience. Students were supplied with a manual addressing topics
pertinent to the navigation and care of older adults while small group meetings facilitated by geriatrician faculty were
held throughout the year to discuss the learning modules from the manual. The program also expanded, serving as a
pilot for nursing student participation and interprofessional learning. The program was awarded status as an optional
enrichment elective (OEE) for the school of medicine during the academic year, with fifteen medical and nursing
students participated as the first group of navigators to complete the newly designed elective.
The program continued to develop and grow in popularity the following year. Additional topics for discussion were
added to the student manual, as the program was refined to provide the optimum learning experience.
Effort is being invested to continue fostering the growth of the program. This is illustrated by the further expansion of
the program to include pharmacy students, as well as nurse practitioner and pharmacy mentors in the 2012-2013
academic year. The program is now actively pursuing the goals of building clinical skills, providing longitudinal
experiences, and encouraging interprofessional learning for students, while providing valuable support of older adults
and their caregivers.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e |4
B ACKGROUND /R ATIONALE
The Navigator works by pairing a nursing, pharmacy, MS1, or MS2 student with an older patient, whom they
“navigate” through their various outpatient medical encounters during an academic year to help the patient more fully
understand their health problems and treatments. Through this immersive experience, students will be able to:
Consider the complexity of multiple medical morbidities, polypharmacy, and involvement of family
members when communicating with older persons in the ambulatory setting, and later apply the
experiences during their clinical years.
Receive exposure to basic skills of reconciling a patient’s medications, including prescribed, herbal, and
over-the-counter medications.
Recognize health literacy issues affecting older patients and to develop skills to surmount communication
barriers.
Consider how integrative geriatric care is managed across specialties- particularly in oncology- thanks to
an interprofessional partnership for navigating patients
Weigh standard recommendations for health screenings and treatments with the age, functional status,
and the goals of care for their older patients.
Reflect upon the psychological, social, and spiritual needs of their patients with advanced illness and
patient family members.
Actively participate in interprofessional communication, problem-solving, and education
Upon enrollment, new Student Navigators (SNs) receive the Student Navigator Resource Manual that includes
literature on effective communication with older persons, geriatric prescribing, geriatric specialty-specific
considerations, and end-of-life care. During the academic year, geriatrician, nurse practitioner, and pharmacist faculty
advisors facilitate four small group sessions (offered during fall and spring semesters) with participating SNs to teach
the seven goals mentioned above.
Geriatricians and nurse practitioners involved in the Navigator Program pair SNs with patients in their practice, who
then longitudinally follow those patients to sub-specialist appointments. At appointments, the SN’s responsibilities
include accompanying the older patient into the examination room and taking notes on a standardized template to
document the visit. Immediately afterward, the SN summarizes the information with the patient (and caregiver) and
provides a copy of the encounter form. The student navigator works with the patient to arrange follow-up
appointments with sub-specialists after his or her first office visit with the patient. Students learn to contrast the
different communication styles as well as challenges employed by primary providers and specialists.
Ultimately, we hope the Navigator Program will influence the communication style and outlook of health profession
students toward older patients by offering an early clinical exposure and small group teaching sessions with academic
geriatricians, nurse practitioners, and pharmacists.
Sincerely,
Dr. Gary Blanchard, Dr. Sarah McGee, Dr. Erika Oleson
Geriatrician Faculty Advisors to the Navigator Program
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e |5
Program Faculty and Administration
Gary Blanchard, MD Sarah McGee, MD, MPH
Geriatrician Faculty Advisor Geriatrician Faculty Advisor
508.856.4250 508.334.6251
Gary.Blanchard@umassmed.edu Sarah.McGee@umassmed.edu
Mary Ellen Keough, MPH
Erika Oleson, DO, MS Reynolds/AGE Project Director
Geriatrician Faculty Advisor Director of Educational Programs
508.334.6251 Meyers Primary Care Institute
Erika.Oleson@umassmemorial.org 508.791.7392
MaryEllen.Keough@umassmed.edu
Megan Janes Benjamin Vaughan
Geriatrics Interest Group Co-leader Geriatrics Interest Group Co-leader
UMMS Class of 2015 UMMS Class of 2015
Megan.Janes@umassmed.edu Benjamin.Vaughan@umassmed.edu
Colleen Burnham, MBA Mark Fitzgerald
AGE Curriculum Resources Navigator Consigliore
Office of Educational Affairs SOM, Class of 2013
Colleen.Burnham@umassmed.edu Mark.Fitzgerald@umassmed.edu
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e |6
T RAINING TO B ECOME A S TUDENT N AVIGATOR
Navigator training is presented in two parts, which are most effective when presented sequentially.
Part I
The Student Navigator Leaders provide the Student Navigator Resource Manual to students upon enrollment in the
program. Materials include orientation information, training instructions, blank templates for note-taking and
assessment, relevant articles presented in learning modules, and useful resources for patients and Student Navigators
(SNs). The prospective SN is asked to read the training/orientation section upon receipt of the manual. The
prospective SN is not expected or required to read the entire manual all at once. Throughout the semester, SNs attend
four small group meetings hosted by a faculty advisor. Each small group meeting addresses one of the four learning
modules. Prospective SNs are encouraged to read the corresponding learning module before the meeting in order to
be prepared to discuss the topic. Each module begins with a summary of the included materials, a list of important
concepts; ending with guiding questions for the prospective SN to consider. For each learning module, the
prospective SN is encouraged to think critically about how the content of each section is clinically relevant.
Additionally, prospective SNs are encouraged to click on the following link and become oriented with the information
on the UMMS Advancing Geriatric Education (AGE) website: http://umassmed.edu/AGE/index.aspx.
A presentation by Dr. Gerry Gleich is accessible on the AGE website under the ‘Geriatrics Interclerkship 2010’ tab of
‘UMMS AGE Curriculum Development’. This presentation gives an overview of many of the following learning
modules; it is accessible via the following link: http://onlinetraining.umassmed.edu/p49355707/
Online PowerPoint files included in this manual are timed for 3-5 seconds per slide and do not have audio.
Slideshows are intended as exposure to the material rather than mastery of all the information in them. The SN can
use the pause button on detailed automated presentation slides.
Part II
Two videos of actual Navigator sessions are in development. The Prospective Navigator will view both videos and
take notes on a blank template as if they were actually navigating the patient. Immediately following the appointment,
the SN has the opportunity to compare his or her notes with those taken by the SN in the video. Look for similarities
and differences between the model notes and your own, including details that may be superfluous or missing. The
prospective SN should also note the flow and content of the Student Navigator meeting with the patient prior to the
appointment and afterward as well. The videos are intended as general models to highlight the important particulars,
but each SN will have his or her own personality and method of interacting with the patients they navigate. The
following pages show a completed demonstration template. Keep in mind the content of the notes taken will likely
vary from session to session.
Any questions about the goals and or logistics of patient navigation may be directed to either the current GIG co-
leaders (Ben Vaughan, Meagan Jane), or the geriatrician faculty advisors to the Navigator Program (Dr. Gary
Blanchard, Dr. Sarah McGee, Dr. Erika Oleson).
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e |7
T IMELINE OF A N AVIGATOR S ESSION
15 Minutes Prior to Appointment
Student Navigator (SN) and elder meet outside of physician’s office.
If patient and SN are not previously acquainted, SN will introduce him/herself.
“Hi Mr/s. ______. My name is _____ _________ and I am a nursing/pharmacy/medical student at
UMMS/UMass GSN/MCPHS. I will accompany you in your appointment and take notes based on what the
provider says (about your health, medications, and any instructions s/he wants you to follow).”
If patient is new to program, the SN explains the purpose and goals of the program, as well as the services the
SN provides.
“The Navigator Program is meant to help health profession students learn by working with patients and health
care providers. The hope is the program also helps the patient; you do not have to remember everything the
provider says because I will take notes and give them to you.”
The SN asks if there are any questions or concerns the patient has.
“Are there any questions you have for the doctor that you would like me to remind you about during the
appointment?”
During the Appointment
Accompany the patient into the examination room. Observe the patient-clinician interaction and the physical
exam, taking structured notes using the specially designed template.
At the end of the appointment, ask the provider to look over the notes taken on the template and initial them if
the physician desires.
Following the Appointment
After the visit, the SN and patient “debrief” in a private area of the office to review. Use this time to clarify
key points of the visit, their patient’s vital signs, weight, lab/test results, and any changes to their medication
regimen.
Ex. “Dr. _____ said your blood pressure was good, and your cholesterol was great.”
Ex. “Did you have questions about anything else that the doctor said?”
Use this time to explain any complicated medical terms that may have been unclear.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e |8
***It is necessary to emphasize that Student Navigators should translate medical language used during
the appointment; Student Navigators should not take notes or give advice based on interpretation. It is
also okay to not know an answer to a question asked by the patient.
The SN provides the patient and or family member with a copy of the Navigator notes from the visit, along
with the medication list if feasible.
Work with the patient to schedule any follow-up visits at mutually suitable times for you both. It may be
helpful to bring an academic calendar to check for any conflicts while coordinating the follow-up visit. Keep
in mind that as an elective, class time should take precedence over the Navigator Program and you may not
always be able to plan a follow-up appointment that fits everyone’s schedules. Choosing to skip class time for
navigation commitments should be done at your discretion and judgment.
Each SN will complete an evaluation of their clinical encounters once a semester using either BLS Vista
(Blackboard) or E-Value. Evaluation data is pivotal for improving the program each year, and allow the
faculty to be responsive to SN feedback.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e |9
H ELPFUL T IPS FOR S UCCESSFUL N AVIGATION
FROM E XPERT N AVIGATORS
Bonnie Vallie Romulo Celli
Class of 2011 Class of 2012
Visionaries and Founders of the Navigator Program
A caregiver may accompany elderly patients to their appointments; make sure you are attentive and
responsive to both patient and caregiver.
Elderly patients will have many different levels of cognitive functioning. Try to summarize at a level
appropriate for their understanding.
If you are unsure about the accuracy of a note you recorded (especially any change in medication), double
check with the doctor.
Write neatly and large enough for your notes to be legible even if the patient has some vision loss. The notes
you take serve as a valuable reference for the patient.
If you are unsure of the answer to a question, it is always best to say, “I don’t know”.
Bring extra note-taking templates to appointments. It may be helpful to quickly scribble notes down on one
set during the appointment and then copy them over neatly afterward.
As you get to know the patient over multiple visits, you may find yourself in a position to advocate for the
patient in specific situations. Always be polite and respectful toward the health care provider, and use
common sense to advocate appropriately on behalf of the patient and/or caregiver
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 10O VERALL T IMELINE FOR S TUDENT N AVIGATOR T RAINING
Note that each blocked event only runs ~1-2 hours. Time ranges are blocked for probable time-periods during which
that event may occur.
Date Event (Small Group/ Module) Event (Clinical Estimated Time Commitment
Experience) for Prospective Student
Navigator (PSN)
August Objective: Student Navigator
(Early) Recruitment n/a
Location: Activities Fair
August Objective: Student Navigator Orientation Meeting: ~ 1 hour
(Late) Orientation
Location: TBA
PSN Preparation: Read Training
section of Manual
September ~ Objective: Student Navigator Small Objective: Student- Prep for Small Group: ~1 hour
October Group Meeting #1 Patient Navigator Small Group Meeting: ~2 hours
Location: TBA Session 1 Supervised Navigator Session:
PSN Preparation: Read Module I ~ 1 hour
in Manual
November ~ Objective: Student Navigator Small Objective: Student- Prep for Small Group: ~1 hour
December Group Meeting #2 Patient Navigator Small Group Meeting: ~2 hours
Location: TBA Session 2 Supervised Navigator Session:
PSN Preparation: Read Module II ~ 1 hour
in Manual
January ~ Objective: Student Navigator Small Objective: Student- Prep for Small Group: ~1 hour
February Group Meeting #3 Patient Navigator Small Group Meeting: ~2 hours
Location: TBA Session 3 Supervised Navigator Session:
PSN Preparation: Read Module III ~ 1 hour
in Manual
March ~ Objective: Student Navigator Small Objective: Prep for Small Group: ~1 hour
April Group Meeting #4 Additional Small Group Meeting: ~2 hours
Location: TBA Navigator Sessions Additional Supervised Navigator
PSN Preparation: Read Module IV Session(s):
in Manual ~ 1 hour per session
Total First Year Commitment: ~ 16 - 20 hours
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 11Note-Taking Template
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 12UMMS AGE Senior Patient Navigator Program© Materials included may be subject to copyright protection P a g e | 13
N OTE -T AKING T EMPLATE S AMPLE
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 14UMMS AGE Senior Patient Navigator Program© Materials included may be subject to copyright protection P a g e | 15
M ODULE I: C OMMUNICATING WITH O LDER A DULTS
Summary
This module focuses on communication between health care providers, patients, and caregivers. It explores effective
ways to communicate, as well as barriers that may arise in clinical situations. Module I has three parts: one online
video, a narrated PowerPoint presentation, and a sections of clinical pearls. The video in Part 1 is presented by the
American Medical Association (AMA) and discusses health literacy and can be accessed via the link below. The
PowerPoint covers tips for improving doctor/caregiver communication, studies examining health literacy in older
adults, and how health literacy is tested. It can be accessed via Blackboard Vista. The clinical pearls section is
included in this binder; it discusses common challenges and solutions in communicating with older adults.
Part 1
Health Literacy and Patient Safety: Help Patients Understand American Medical Association
http://www.youtube.com/watch?v=cGtTZ_vxjyA
Part 2
Communication & Health Literacy in Older Adults Fitzgerald
Part 3
Clinical Pearls of Managing Communication Challenges Blanchard
PROGRAM OBJECTIVES ADDRESSED
Consider the complexity of involvement of family members and or caregivers, and possible cognitive
impairment when communicating with older persons in the ambulatory clinical setting.
Develop communication skills for effectively relating to older patients and apply them during their clinical
years.
Recognize health literacy issues affecting older patients.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 16MODULE I: COMMUNICATING WITH OLDER ADULTS: MEDICAL, NURSING, PHARMACY, AND INTERPROFESSIONAL
COMPETENCIES
AACN & JOHN A. HARTFORD FOUNDATION ADULT-GERONTOLOGY PRIMARY CARE NURSE PRACTITIONER COMPETENCIES
Practitioner- Patient Relationship: Provides support through effective communication and therapeutic relationships with
individuals, families, and caregivers facing complex physical and/or psychosocial challenges.
Practitioner- Patient Relationship: Uses culturally appropriate communication skills adapted to the individual’s cognitive,
developmental, physical, mental and behavioral health status.
Teaching-Coaching Function: Adapts teaching-learning approaches based on physiological and psychological changes, age,
developmental stage, readiness to learn, health literacy, the environment, and resources.
Professional Role: Directs and collaborates with both formal and informal caregivers and professional staff to achieve optimal
care outcomes
ASCP GERIATRIC PHARMACY CURRICULUM GUIDE COMPETENCIES
Communication: Demonstrate skill in communicating drug and adherence information (verbal and written) to senior patients,
their caregivers and the interprofessional care team.
Communication: Demonstrate proficiency to interview and counsel seniors with varying degrees of cognitive and communication
abilities.
Communication: Recognize barriers to effective communication (e.g., cognitive, sensory, cultural, and language).
Education: Utilize educational material appropriate to the specific patient/caregiver.
CORE COMPETENCIES FOR INTERPROFESSIONAL COLLABORATIVE PRACTICE
VE5. Work in cooperation with those who receive care, those who provide care, and others who contribute to or support the
delivery of prevention and health services.
RR1. Communicate one’s roles and responsibilities clearly to patients, families, and other professionals.
CC1. Choose effective communication tools and techniques, including information systems and communication technologies, to
facilitate discussions and interactions that enhance team function.
CC2. Organize and communicate information with patients, families, and healthcare team members in a form that is
understandable, avoiding discipline-specific terminology when possible.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 17MODULE I: COMMUNICATING WITH OLDER ADULTS: IMPORTANT CONCEPTS
Low health literacy is an extremely prevalent problem, with 60% of adults age 65+ at a basic or below basic
health literacy level. The causes of low or declining health literacy are diverse, but they can usually be
organized by identifying with of the three “In’s” (intake, interpret, and interact) the cause is interfering with
(ex. Loss of vision limits a patient’s ‘intake’ ability, while dementia may limit the ability to interpret).
Hypertension, diabetes, and hypercholesterolemia may all lead to cerebrovascular disease and stroke, which
can affect reading ability. Moreover, several studies have shown that individuals who have hypertension are
more likely to have a decline in cognitive function, even in the absence of a stroke.
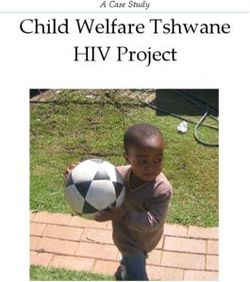
The Short Test of Functional Health Literacy in Adults (S-TOFHLA) has shown health literacy to be closely
inversely correlated with age.
Figure 1. Mean scores on the Short Test of
Functional Health Literacy in Adults for five age
groups, stratified according to years of school
completed: >12 yr (black circle; n = 898), 12 yr
(white circle; n = 998), 9–11 yr (black triangle; n =
526), and 0–8 yr (white triangle; n = 352). The
bars indicate standard errors (Baker, Gazmararian,
Sudano, Patterson, 2000).
A patient with low health literacy may find most patient education materials that are distributed in physicians’
offices to be too complex, written at too high a level, or not organized from the patient perspective.
Having a companion or caregiver with the patient can create a specific type of triadic dialogue that is
uniquely common to geriatrics (some say it is like turning a pediatric triadic interview on its head). It is
important to obtain information from both patient and caregiver without alienating or ignoring either party.
A language barrier can occasionally be a hurdle in effective communication in elderly populations. Often
surmounting this hurdle requires a set communication skills, including experience with a triadic interview and
the ability to break down information so it can be translated.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 18MODULE I: COMMUNICATING WITH OLDER ADULTS: CLINICAL PEARLS OF MANAGING COMMUNICATION
CHALLENGES
MEDIUMS OF COMMUNICATION
Non-verbal Communication
Personal Space: be aware most people prefer 1 1/2 to 3 feet of space around them.
Assess their mood and attitude. Utilize congruent facial expressions.
Use gestures to clarify your point.
Paraverbal Communication
Be aware of how your message is perceived.
Attend to tone: respectful
Assess volume: consider possible hearing impairment
Attend to cadence: keep your rhythm slow and deliberate
Verbal Communication
Use simple, direct statements, enunciate words, avoid terms of endearment or infantilizing.
Utilize Mr. or Mrs., Ms. until granted permission otherwise… Ask!
Always acknowledge the patient directly, address the family member or caregiver afterward. Never ignore the
patient.
Power of Attorney is only an enforced power if the patient becomes incapacitated.
Ask open-ended questions and avoid giving ‘fill in the blank’ responses (unless format is necessary because
of cognitive deficiency).
Do not skirt issues (depression, suicide, alcohol, finances, abuse).
Allow plenty of time for responses.
Empathic Listening
An active process, provide undivided attention. Remember to restate, rephrase and clarify.
Allow for silence.
BARRIERS TO COMMUNICATION
Hearing impaired
Possible Solution: Stand directly in front of the person, make sure you have that individual’s attention and
that you are close enough to the person before you begin speaking to reduce or eliminate background noise.
Possible Solution: Use a portable amplifier system; speak slowly and distinctly.
Visually impaired
Possible Solution: Explain what you are doing as you are doing it. Ask how you may help: increasing the
light, reading the document, and/or describing where things are.
Possible Solution: Write instructions in large font with a dark marker.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 19Dementia
Introduce yourself each time.
Use short simple sentences or questions and give plenty of time for the person to respond.
Maintain a calm demeanor; dementia patients may mirror emotion.
Redirect and distract out of stressful situations.
Dementia: Understanding Behaviors
Dementia can affect areas in the brain that control emotion and behavior. The person’s ability for insight and
judgment may be impaired.
Confusion limits one’s ability to understand their surrounding and or to express themselves conventionally.
Dementia: Further Tips for Communication
Speak slowly using simple sentences. Ask simple questions that require a choice or a yes/no answer.
Use concrete terms and familiar words.
Always introduce yourself, don’t expect the person to know your name no matter how long you have known
them.
Prompt the person with information instead of testing their knowledge.
Offer choices when possible (e.g., Do you live at home or with family?).
Use gestures and visual cues to get your message across.
Speak in a warm, easy-going, pleasant manner. Use humor and cheerfulness when possible.
If the person is hard of hearing, speak into their ear instead of yelling louder. Consider the use of hearing aids
or a headset amplifier.
Assist the patient in note-taking, marking things on a calendar.
Ask family to assist by providing reminders, and to consider use of a medical alert system for safety and
medication prompting.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 20MODULE I: COMMUNICATING WITH OLDER ADULTS: GUIDING QUESTIONS
Why is it difficult to communicate with older adults? Compared to other students at your level in training, do
you feel you are below average, average, or above average in your ability to communicate with older adults?
What are the potential benefits and possible pitfalls to having a caregiver or companion accompanying the
patient to an appointment?
Why is health literacy especially a concern in older adult populations? What other populations might be at
risk for low health literacy?
What are the three components of health literacy (mentioned in the video)? What problems can arise if a
patient has low health literacy?
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 21MODULE I: COMMUNICATING WITH OLDER ADULTS: READING AND REFERENCE LIST
Baker D, Gazmararian J., Sudano J, Patterson M. The association between age and health literacy among elderly
persons. Journal of Gerontology: SOCIAL SCIENCES 2000; 55B(6): S368-S374.
Health literacy in clinical practice. Retrieved http://cme.medscape.com/viewarticle/566053_5 June 18, 2012.
National Family Caregivers Association. Improving doctor/caregiver communications. www.nfcacares.org.
Parker R, Baker D, Williams M, Nurss J. The test of functional health literacy in adults: A new instrument for
measuring patients’ literacy skills. Jounal of General Internal Medicine; 10(10) October 1995: 537-541.
S-TOHFLA Retrieved November 8, 2011: http://www.nmmra.org/resources/Physician/152_1485.pdf.
Weiss BD. Assessing health literacy in clinical practice. Medscape 2007.
http://sme.medscape.com/viewarticle/566053. Accessed August 25, 2012 [requires free registration to
MedScape CME site to view]
ADDITIONAL RESOURCES FOR FURTHER LEARNING
American College of Physicians Health Literacy Resources
http://foundation.acponline.org/hl/hlresources.htm
American College of Physicians Ethics and Human Rights Committee: Family caregivers, patients and physicians:
ethical guidance to optimize relationships.
http://www.springerlink.cin.ioebyrk.asp?genre=article&id=doi: 10.1007/s11606-009-1206-3.
Strategies to Improve Communication Between Pharmacy Staff and Patients: A training Program for Pharmacy Staff
http://www.ahrq.gov/qual/pharmlit/pharmtrain.htm
TOFHLA Teaching Version. Available for purchase from Peppercorn Books
http://www.peppercornbooks.com.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 22M ODULE II: G ERIATRIC P RESCRIBING
Summary
This module focuses on the complexity of managing multiple medications in older adults with regard to proper
dosing, prescribing cascades, and adverse drug reactions. Module I has four parts: two PowerPoint presentations for
students to scroll through, a third narrated PowerPoint presentation, and a link to the AGS Beer Criteria Printable
Pocket Card. The first two presentations are accessed online via the links provided; the slides do not have audio and
are intended for exposure to the material rather than mastery of all the information contained on them. Students
should progress through the PowerPoints at their own pace; for more detailed slides, it is possible to pause the
presentation. Some of the important concepts are repeated among the presentations. The narrated PowerPoint
presentation can be accessed via Blackboard Vista; it provides a review of important topics from the first two
presentations, describes some clinical pearls for geriatric prescribing, and offers an introduction to anticoagulation in
the older adult. Students are encouraged to print out the AGS Beer Criteria Printable Pocket Card for reference and
discussion in regards to its usefulness and purpose.
Part 1
Making Medication Use Safer in Older Adults Tjia
http://onlinetraining.umassmed.edu/p35814819/
Part 2
Drug Therapy in the Elderly Gurwitz
http://onlinetraining.umassmed.edu/drug_therapy/
Part 3
Geriatric Prescribing Parts I & II Fitzgerald
Part 4
AGS Beers Criteria Printable Pocket Card American Geriatrics Society
http://www.americangeriatrics.org/files/documents/beers/PrintableBeersPocketCard.pdf
PROGRAM OBJECTIVES ADDRESSED
Consider the complexity of multiple medical co-morbidities and polypharmacy when communicating
with older persons in the ambulatory clinical setting.
Increase awareness of medication reconciliation, including prescribed, herbal, and over-the-counter
medications.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 23MODULE II: GERIATRIC PRESCRIBING: MEDICAL, NURSING, PHARMACY, AND INTERPROFESSIONAL
COMPETENCIES
AAMC & JOHN A. HARTFORD FOUNDATION GERIATRIC COMPETENCIES FOR MEDICAL STUDENTS
Medication Management: Explain impact of age-related changes on drug selection and dose based on knowledge of age-related
changes in renal and hepatic function, body composition, and Central Nervous System sensitivity.
Identify medications, including anticholinergic, psychoactive, anticoagulant, analgesic, hypoglycemic, and cardiovascular drugs
that should be avoided or used with caution in older adults and explain the potential problems associated with each.
Medication Management: Document a patient’s complete medication list, including prescribed, herbal and over-the-counter
medications, and for each medication provide the dose, frequency, indication, benefit, side effects, and an assessment of
adherence.
AACN & JOHN A. HARTFORD FOUNDATION ADULT-GERONTOLOGY PRIMARY CARE NURSE PRACTITIONER COMPETENCIES
Management of Patient Health/Illness: Conducts a pharmacologic assessment addressing polypharmacy; drug interactions and
other adverse events; over-the-counter; complementary alternatives; and the ability to obtain, purchase, self administer, and store
medications safely and correctly.
Management of Patient Health/Illness: Prescribes medications with particular attention to high potential for adverse drug
outcomes and polypharmacy in vulnerable populations, including women of childbearing age, adults with co-morbidities, and
older adults.
ASCP GERIATRIC PHARMACY CURRICULUM GUIDE COMPETENCIES
Biology of Aging: Discuss the physiologic changes associated with aging and how they impact medication therapy.
Biology of Aging: Apply the knowledge of aging physiology to the clinical use of medications.
Communication: Demonstrate skill in communicating drug and adherence information (verbal and written) to senior patients,
their caregivers and the interprofessional care team.
Communication: Demonstrate proficiency to interview and counsel seniors with varying degrees of cognitive and communication
abilities.
Communication: Recognize barriers to effective communication (e.g., cognitive, sensory, cultural, and language).
Pathophysiology: Recognize medication-induced disease.
Geriatric Assessment: Obtain and interpret the medication history in relation to patient's current health status.
Geriatric Assessment: Recognize the relationship between geriatric syndromes/diseases and medication-related problems.
Education: Ensure understanding of medication use and its role in the overall treatment plan.
CORE COMPETENCIES FOR INTERPROFESSIONAL COLLABORATIVE PRACTICE
RR3:
Engage
diverse
healthcare
professionals
who
complement
one’s
own
professional
expertise,
as
well
as
associated
resources,
to
develop
strategies
to
meet
specific
patient
care
needs.
TT3: Engage other health professionals- appropriate to the specific care situation- in shared patient-centered problem-solving
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 24MODULE II: GERIATRIC PRESCRIBING: IMPORTANT CONCEPTS
The amount of medication use in the elderly is much higher, compared to younger populations. 40% of
people >65 years old use >5 medications, while 12% of the elderly population uses >10 medications.
Nearly 1/3rd (1.9 million) of Adverse Drug Events are preventable. Of the most serious, life-threatening
ADEs, over 40% are preventable.
Body composition changes with age: muscle mass decreases while lipid storage increases. This can
profoundly affect the half-life of lipid soluble drugs. Decrease in kidney function can also affect the half-life
of medications as well.
Older adults have slower metabolism, excretion of drug as well as increase sensitivity. The saying, “start low,
go slow” is used to refer to medication dosing
The types of medications most commonly involved in adverse drug events relate closely to those most
frequently prescribed in the ambulatory setting, with cardiovascular drugs and antibiotics/anti-infectives are
the most frequently used and implicated drug categories.
Some of the common problems with Polypharmacy are more adverse drug reactions, decreased adherence to
drug regimens, poor quality of life, high rate of ADEs and or side effects, and (unnecessary) drug expense.
Factors contributing to polypharmacy are underreporting symptoms, use of multiple providers, use of others’
medications, limited time for discussion, limited knowledge of geriatric pharmacology (clinician), and low
health literacy leading to poor understanding of purpose of medications (patient)
Factors contributing to non-adherence are a high number of medications, expense of medications, complex or
frequently-changing dosing schedule(s), adverse reactions, confusion about brand /trade name, difficult-to-
open containers, rectal/vaginal/SQ (unpopular) modes of administration, and limited patient health literacy
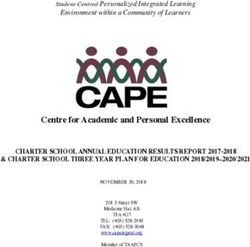
General Model of a ‘prescribing cascade’
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 25MODULE II: GERIATRIC PRESCRIBING: GUIDING QUESTIONS
What have been your experiences regarding medication use in older adults? Do you have parents or
grandparents on multiple medications? Do you know any family members who are been hospitalized because
of an adverse drug event? What sort of medications does the patient you navigate take?
What is Medication Reconciliation? What is the purpose of medication reconciliation and what are the
essential steps in the process?
Why are elderly patients at a high risk for ‘prescribing cascades’? What are 2-3 clinical examples of instances
where prescribing cascades can develop?
What are some effective ways to reduce the number and cost of medications for an elderly patient?
What 4 factors of pharmacokinetics change with aging? What organ systems undergo normal age-related
physiologic changes that influence how to prescribe medications for older adults?
Discuss anticoagulation in older adults. What concerns, considerations, and challenges occur?
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 26MODULE II: GERIATRIC PRESCRIBING: READING AND REFERENCE LIST
American Geriatrics Society. AGS Beers Pocket Card. Accessed
http://www.americangeriatrics.org/files/documents/beers/PrintableBeersPocketCard.pdf August 25, 2012.
Gurwitz J. Drug Therapy in the Elderly. PowerPoint presentation at the Chief Resident Immersion Training. Accessed
http://onlinetraining.umassmed.edu/drug_therapy/ August 25, 2012.
Gurwitz J, Field T, Harrold L, Rothschild J, Debellis K, Seger A, Cadoret C, Fish L, Garber L, Kelleher M, Bates D.
Incidence and preventability of adverse drug events among older persons in the ambulatory setting. JAMA: March 5,
2003; 289(9): 1107-1096.
Rochon P, Gurwitz J. Optimizing drug treatment for elderly people: the prescribing cascade. BMJ 1997; 315: 1096-
1099 (25 October).
Tjia J. Making medication use safer in older adults. PowerPoint presentation at the University of Massachusetts
Medical School. Accessed http://onlinetraining.umassmed.edu/p35814819/ August 25, 2012
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 27M ODULE III: G ERIATRIC S PECIALTY -S PECIFIC E XPERIENCES & C ONSIDERATIONS
Summary
This module explores how integrative geriatric care for a medically complex patient is managed across specialties.
This module is intended to supplement clinical experiences unique to each student navigator, so therefore it is not
expected that you- the student navigator- read the entire module. Instead, read the introductory article “The Way
We Age Now” by Atul Gawande and Part 8: The Hospitalized Patient. Additionally, select one or two sections from
Parts 2 through 7 based on experiences in clinical navigation sessions. If a navigation session took place in a specialty
not listed here, alternatively a student navigator may choose to look up information regarding geriatric considerations
for that specialty. The small group session that accompanies this module will be mostly focused on student navigators
sharing impressions of their specialty navigation sessions.
Part 1: Introduction
The Way We Age Now Gawande
http://www.newyorker.com/reporting/2007/04/30/070430fa_fact_gawande
Part 2: Geriatric Psychiatry
3D Geriatrics: Dementia, Delirium, and Depression Gleich
http://onlinetraining.umassmed.edu/p97121950/
The 3D’s Continued: Clinical Pearls Fitzgerald
Part 3: Geriatric Cardiology
Cardiology Clinical Pearls Blanchard
Heart Disease in Older Adults Fitzgerald
Part 4: Geriatric Orthopedics
Orthopedic Clinical Pearls Blanchard
Considerations Treating Older Adults in Orthopedics Fitzgerald
Part 5: Geriatric Oncology
The Older Adult with Cancer: Considerations and Pearls for Treatment Fitzgerald
Part 6: Pain Management
Clinical Pearls of Managing Persistent Pain in the Older Adult Fitzgerald
Part 7: Rheumatologic Diseases
Geriatric Rheumatology Nakasato
http://www.ouhsc.edu/geriatricmedicine/Education/GeriatricRheumatology/index.htm
Part 8: The Hospitalized Patient
What to do when your Patient is Hospitalized & A Brief Introduction to Third Year Fitzgerald
PROGRAM OBJECTIVES ADDRESSED
Consider the complexity of multiple medical co-morbidities and possible cognitive impairment when
communicating with older persons in the ambulatory clinical setting.
Weigh standard recommendations for health screenings and treatments with the age, functional status, and the
goals of care for older patients.
Reflection upon the psychological, social, and spiritual needs of patients with advanced illness and their
family members.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 28MODULE III: GERIATRIC SPECIALTY-SPECIFIC CONSIDERATIONS: MEDICAL, NURSING, PHARMACY, AND
INTERPROFESSIONAL COMPETENCIES
AAMC & JOHN A. HARTFORD FOUNDATION GERIATRIC COMPETENCIES FOR MEDICAL STUDENTS
Cognitive and Behavioral Disorders: Define and distinguish among the clinical presentations of delirium, dementia, and
depression
Cognitive and Behavioral Disorders: Perform and interpret a cognitive assessment in older patients for whom there are concerns
regarding memory or function.
Health Care Planning and Promotion: Define and differentiate among types of code status, health care proxies, and advanced
directives in the state where one is training.
Health Care Planning and Promotion: Accurately identify clinical situations where life expectancy, functional status, patient
preference or goals of care should override standard recommendations for screening tests in older adults.
Health Care Planning and Promotion: Accurately identify clinical situations where life expectancy, functional status, patient
preference or goals of care should override standard recommendations for treatment in older adults.
Palliative Care: Assess and provide initial management of pain and key non-pain symptoms based on patient’s goals of care.
Hospital Care for Elders: Identify potential hazards of hospitalization for all older adult patients (including immobility, delirium,
medication side effects, malnutrition, pressure ulcers, procedures, peri and post operative periods, and hospital acquired
infections) and identify potential prevention strategies.
AACN & JOHN A. HARTFORD FOUNDATION ADULT-GERONTOLOGY PRIMARY CARE NURSE PRACTITIONER COMPETENCIES
Management of Patient Health/Illness: Assesses individuals with complex health issues and co-morbidities, including the
interaction with acute and chronic physical and mental health problems.
Management of Patient Health/Illness: Recognizes the presence of co-morbidities, their impact on presenting health problems,
and the risk for iatrogenesis.
Management of Patient Health/Illness: Treats and manages complications of chronic and/or multi-system health problems.
Professional Role: Coordinates comprehensive care in and across care settings.
ASCP GERIATRIC PHARMACY CURRICULUM GUIDE COMPETENCIES
Continuum of Care: Participate in interprofessional decisions regarding appropriate levels of care for individual patients.
Continuum of Care: Facilitate medication reconciliation across the continuum of care.
Prioritizing Care Needs: Develop a problem list and prioritize care based upon severity of illness, patient preference,
quality of life, and time to benefit.
Prioritizing Care Needs: Identify patients who need referrals to other health and non-health professionals.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 29CORE COMPETENCIES FOR INTERPROFESSIONAL COLLABORATIVE PRACTICE
RR3: Engage diverse healthcare professionals who complement one’s own professional expertise, as well as associated resources,
to develop strategies to meet specific patient care needs.
RR4:
Explain
the
roles
and
responsibilities
of
other
care
providers
and
how
the
team
works
together
to
provide
care.
RR5: Use the full scope of knowledge, skills, and abilities of available health professionals and healthcare workers to provide
care that is safe, timely, efficient, effective, and equitable.
RR7. Forge interdependent relationships with other professions to improve care and advance learning.
TT3.
Engage
other
health
professionals—appropriate
to
the
specific
care
situation—in
shared
patient-‐centered
problem-‐
solving.
TT4. Integrate the knowledge and experience of other professions— appropriate to the specific care situation—to inform care
decisions, while respecting patient and community values and priorities/ preferences for care.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 30GERIATRIC CARDIOLOGY CLINICAL PEARLS
Medications commonly taken by older patients seeing a cardiologist
Coumadin (warfarin) – a potent blood thinner, one of the most effective medication available for preventing
ischemic stroke in older at-risk patients (those with hypertension, congestive heart failure, atrial fibrillation,
diabetes).
o Special considerations in older patients: review complete list of medications (both prescription and
over-the-counter) for potential drug-drug interactions with warfarin that might excessively thin a
patient’s blood (increased risk of bleeding).
Beta-blockers (atenolol, metoprolol [Lopressor, Toprol], carvediol) – lower heart rate and blood pressure by
persistently blunting adrenergic response; significantly decrease mortality following a heart attack and in
those with heart disease; slow the progression of chronic heart failure (improve exercise tolerance and
functional status).
o Special considerations in older patients: check orthostatic blood pressures (lying, sitting, standing) to
ensure that blood pressure does not drop too much (increased risk of falls). Due to the aging of the
sino-atrial node, older patients on beta-blockers tend to have lowered heart rates. May cause
depression and anxiety.
Digoxin – increases contractility of the heart muscle; decreases frequency of hospitalizations for congestive
heart failure but does not lower mortality.
o Special considerations in older patients: potential for toxicity is higher in older patients given narrow
therapeutic drug window and decreased kidney function associated with aging. Monitor levels more
frequently in those with renal failure as toxicity can lead to significant heart arrhythmias.
Normal aging changes to the older heart
Muscle is less able to relax between heart beats and becomes stiffer over time (especially in those with
longstanding high blood pressure).
Less able to increase the strength of contraction (and thereby becomes harder to offload more oxygen to the
heart muscle during exercise).
The walls of coronary blood vessels become less elastic over time.
Specific considerations for older patients seeing a cardiologist
Patients with heart failure but a preserved ejection fraction – diastolic dysfunction – frequently have a
comparable prognosis to those with heart failure and reduced ejection fraction (systolic dysfunction). A better
prognostic marker for patients with heart failure is to assess their functional capacity, i.e., how limited on a
daily basis they are by their shortness of breath.
Treating hypertension in patients in their 80s and 90s is still of paramount importance – with resultant risk
reduction of stroke and heart failure. You need to be more cognizant, though, of inducing orthostatic
hypotension in older patients on multiple blood pressure-lowering agents (especially alpha-blockers and
ACE-inhibitors). Beta-blockers are not optimal blood pressure agents when used in isolation.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 31Anticoagulation with warfarin is currently considered the most effective way to prevent stroke in older
patients with atrial fibrillation. Carefully consider a patient’s goals of care when weighing a patient’s risk of
anticoagulation with the possible benefits of stroke prevention when starting warfarin.
Loop diuretics (furosemide, or, Lasix) are effective for symptomatic relief of congestive heart failure
symptoms – but have many side effects in older persons that need to be closely monitored (electrolyte
abnormalities).
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 32GERIATRIC ORTHOPEDICS: CLINICAL PEARLS
With the first baby boomer set to turn 65 on January 1, 2011, there will be more older patients visiting orthopedic
doctors than ever before. The focus of an orthopedic visit for an older patient is to consider treatments designed to
maintain mobility and alleviate musculoskeletal pain that can lead to a loss of daily function. Advanced minimally
invasive surgical procedures have decreased the frequency of complications associated with surgery, making surgical
intervention a viable option for many older patients. The following are examples of common problems an older
patient may encounter:
Hip and Femur
Hip fractures are the most frequent orthopedic injury suffered by older patients. A patient whose hip fracture is not
treated urgently (within 48 hours) is at greater risk of ultimately losing their mobility and independence – which can,
unfortunately, lead to long-term care placement. Unless treated urgently, hip fractures are also the orthopedic injury
with the highest mortality rate – both immediately following the fracture as well as 6 and 12 months later. There are
four patterns of hip fracture frequently seen: femoral head fracture, femoral neck fracture, intertrochanteric fracture,
and subtrochanteric (shaft) fracture. Interdisciplinary care is vital for successful treatment. The most important
preventative treatment for hip fractures in older patients is fall prevention, focusing on promoting exercise,
maintaining balance, and minimizing potentially hazardous medications. Older patients should be screened for
osteoporosis (see below); those with hip fractures should almost always be treated for osteoporosis.
Knee
The knee is a major site for a list of debilitating pathologies, including bursitis, ligament tearing, and highly prevalent
arthritic diseases. Knee surgery and even total knee replacement are becoming popular procedures for older patients
as new technologies offer a faster recuperation and higher likelihood of recovering full mobility.
Foot and Ankle
Bunions, tendon rupture, and nerve damage are some foot/ankle problems that can significantly disrupt gait and
balance. The foot and ankle is generally divided into three sections - forefoot, midfoot, and hindfoot (including the
ankle) - with each area having its own diverse pathology. A comprehensive article about geriatric ankle/foot surgery
can be found at the following link: Foot & Ankle Surgery: Considerations for the Geriatric Patient
http://www.medscape.com/viewarticle/710374 (Lee & Mulder, 2009)
Spine
Older patients can experience a number of pathologies that affect the integrity of their vertebral column. The diagram
at right lists a number of common issues that can cause back pain. Note that the range of problems includes skeletal,
vascular, nervous, cancerous, and joint components
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 33SPECIFIC CONSIDERATIONS FOR OLDER PATIENTS SEEING AN ORTHOPEDIST
Osteoporosis
Osteoporosis is a very common medical condition, affecting roughly 10 million older patients. Osteoporosis is
marked by bone loss and compromised bone strength, leading to a greater risk of fracture with minimal (or even no)
trauma. Hip fractures pose perhaps the greatest risk to an older patient’s independence. Osteoporotic vertebral
fractures can lead to chronic pain and loss of function. Treatment of osteoporosis has become much more feasible
with the advent of bisphosphonates – namely, alendronate (Fosamax), ibandronate (Boniva), risedronate (Actonel),
and zoledronic acid (Reclast). Preventative measures such as calcium and vitamin D supplementation can also help
ward off disease progression significantly and even prevent falls.
Arthritis: osteoarthritis and rheumatoid arthritis
Arthritis is a major issue in older patients, spanning a clinical spectrum from totally asymptomatic to debilitating and
incapacitating. Osteoarthritis can be more difficult to treat with medication because its pathology is ‘wear and tear’
aging rather than immune-mediated like rheumatoid arthritis. Exercise, especially in the water (where joints are
buoyant), is invaluable. If medications prove ineffective and compromise a patient’s daily functioning, then surgery
may be entertained as an option to reduce pain and restore joint function. Rheumatoid arthritis is an inflammatory
arthritis that can be treated through the use of anti-inflammatory and immunosuppressant drugs.
Cancer
Various types of cancer can cause debilitating problems. Sarcomas (and soft tissue sarcomas) can infiltrate bone and
muscle, devastating normal tissue architecture and functionality. Cancer with metastisis to bone can be a source of
pain and potential disability. Blood cancers such as multiple myeloma will also frequently manifest in part through
bone lesions. The risk of fracture is greatly increased in any number of cancers.
Frailty and Immobility
The elderly population is extremely heterogeneous; at any age there will be patients who are frail and in poor
health as well as others who are quite healthy and physically robust. (To a geriatrician, a patient’s chronologic
age is far less important than their overall functional age.) Recovery from surgery needs to take into account a
patient’s baseline activity level. It is often necessary that surgical recuperation occurs in an inpatient
rehabilitation facility, or skilled nursing facility.
Regardless of frailty, one of the most pressing issues in older patients is extended immobility. Immobility can
quickly lead to a severe decline in health, due to problems such as pressure ulcers, infection, muscle/bone
atrophy, and heart failure. A main goal of orthopedic surgery in elderly patients should be to maximize
mobility as prevention for the problems of immobility.
UMMS AGE Senior Patient Navigator Program©
Materials included may be subject to copyright protection P a g e | 34You can also read