The Role of Information and Communications Technology Policies and Infrastructure in Curbing the Spread of the Novel Coronavirus: Cross-country ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
JMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
Original Paper
The Role of Information and Communications Technology Policies
and Infrastructure in Curbing the Spread of the Novel Coronavirus:
Cross-country Comparative Study
Nam Ji Eum, BA; Seung Hyun Kim, BA, MS, PhD
School of Business, Yonsei University, Seoul, Republic of Korea
Corresponding Author:
Seung Hyun Kim, BA, MS, PhD
School of Business
Yonsei University
50 Yonsei-ro, Sinchon-dong
Seodaemun-gu
Seoul, 03722
Republic of Korea
Phone: 82 2 2123 2506
Email: seungkim@yonsei.ac.kr
Abstract
Background: Despite worldwide efforts, control of COVID-19 transmission and its after effects is lagging. As seen from the
cases of SARS-CoV-2 and influenza, worldwide crises associated with infections and their side effects are likely to recur in the
future because of extensive international interactions. Consequently, there is an urgent need to identify the factors that can mitigate
disease spread. We observed that the transmission speed and severity of consequences of COVID-19 varied substantially across
countries, signaling the need for a country-level investigation.
Objective: We aimed to investigate how distancing-enabling information and communications technology (ICT) infrastructure
and medical ICT infrastructure, and related policies have affected the cumulative number of confirmed cases, fatality rate, and
initial speed of transmission across different countries.
Methods: We analyzed the determinants of COVID-19 transmission during the relatively early days of the pandemic by
conducting regression analysis based on our data for country-level characteristics, including demographics, culture, ICT
infrastructure, policies, economic status, and transmission of COVID-19. To gain further insights, we conducted a subsample
analysis for countries with low population density.
Results: Our full sample analysis showed that implied telehealth policy, which refers to the lack of a specific telehealth-related
policy but presence of a general eHealth policy, was associated with lower fatality rates when controlled for cultural characteristics
(P=.004). In particular, the fatality rate for countries with an implied telehealth policy was lower than that for others by 2.7%.
Interestingly, stated telehealth policy, which refers to the existence of a specified telehealth policy, was found to not be associated
with lower fatality rates (P=.30). Furthermore, countries with a government-run health website had 36% fewer confirmed cases
than those without it, when controlled for cultural characteristics (P=.03). Our analysis further revealed that the interaction between
implied telehealth policy and training ICT health was significant (P=.01), suggesting that implied telehealth policy may be more
effective when in-service training on ICT is provided to health professionals. In addition, credit card ownership, as an enabler of
convenient e-commerce transactions and distancing, showed a negative association with fatality rates in the full sample analysis
(P=.04), but not in the subsample analysis (P=.76), highlighting that distancing-enabling ICT is more useful in densely populated
countries.
Conclusions: Our findings demonstrate important relationships between national traits and COVID-19 infections, suggesting
guidelines for policymakers to minimize the negative consequences of pandemics. The findings suggest physicians’ autonomous
use of medical ICT and strategic allocation of distancing-enabling ICT infrastructure in countries with high population density
to maximize efficiency. This study also encourages further research to investigate the role of health policies in combatting
COVID-19 and other pandemics.
(JMIR Public Health Surveill 2022;8(1):e31066) doi: 10.2196/31066
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 1
(page number not for citation purposes)
XSL• FO
RenderXJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
KEYWORDS
health policy; telehealth; physical distancing; disease transmission; COVID-19
on the spread of COVID-19 tended to have narrower scopes,
Introduction such as individuals, several cities, a single country, or a single
First identified in December 2019, the novel COVID-19 continent, rather than a global focus [12-17]. Although there
outbreak has rapidly spread worldwide. As of September 23, are some exceptions, those studies were still limited in the
2021, the World Health Organization (WHO) reported that over number of countries, possibly due to difficulty in data collection,
229.8 million people were infected worldwide, with over 4.7 for investigation [15,16]. For instance, the latest cross-country
million deaths caused by COVID-19 [1]. Furthermore, on study on the effect of threat or coping appraisal on distancing
December 19, 2020, a mutant of COVID-19, labeled B.1.1.7, compliance was conducted by comparing 5 countries only [18].
was found, causing further havoc specifically in European In addition, prior research also focused on how the demographic,
countries. Consequently, the UK Prime Minister Boris Johnson cultural, or political factors of a country affected COVID-19
imposed another lockdown that was even stricter than the infection [19-22], but did not include ICT-related factors.
previous lockdowns [2]. This kind of catastrophic pandemic is To address such a research gap, the primary objective of this
not unprecedented. From 1918 to 1919, the H1N1 influenza A study was to identify what national characteristics have a major
virus emerged and went on to infect approximately 40% of the impact on curtailing contagious diseases during the relatively
global population, with a mortality rate of more than 2% [3]. early days of the pandemic. In particular, we focused on the
The H1N1 flu persists to this date, over 100 years since its first role of distancing-enabling ICT infrastructure (DistancingICT)
appearance, and has undergone significant genetic mutations. and medical ICT infrastructure and policy (MedicalICT) in
Virologists expect COVID-19 to follow a similar pattern [4,5]. containing COVID-19 infection, fatality rates, and transmission
As such, the prevalence of pandemics and genetic mutations is speed.
not a one-off phenomenon. Other outbreaks with disruptive
social and economic consequences are probable [6], demanding Methods
research on how to control the spread of a virus in its early
stages. Data Collection
With this urgent need in mind, it is noteworthy that the infection The main sources of country-level data used in this study
and fatality rates as well as the speed of transmission have varied included the United Nations, the World Bank, the WHO,
widely across countries. Countries, such as Israel, Singapore, Worldometers, Our World in Data (OWID), Ookla, Hofstede
South Korea, and Taiwan, are regarded as relatively successful Insights, and Wikipedia. Among these, Worldometers is a
in curbing transmission [7], whereas European countries and reference site that provides real-time statistics on diverse topics.
the United States experienced an explosive increase in the As a widely used source of research, media, and teaching, OWID
number of confirmed cases [1]. It is known that minimizing is an online scientific publication institute that focuses on global
physical contact between individuals without disturbing their issues such as poverty and disease. Ookla provides analyses of
daily lives and improved medical practices are crucial in internet access performance metrics. Hofstede Insights provides
managing the spread of infectious diseases in general [8]. First, culture scores of each country based on Hofstede’s cultural
as a means of reducing physical contact and enabling social dimension theory [23], and is widely used in academic research.
distancing, national information and communications technology For example, to predict growth of COVID-19 confirmed cases
(ICT) infrastructure, such as e-commerce and high speed internet across several countries, Hofstede dimensions are used to
connection, has played a key role in many countries [8,9]. account for cultural factors [24]. Wikipedia is used only to
Second, the possible importance of medical ICT policies and determine which countries enforced national lockdowns in the
infrastructure has also been recognized. For example, effective early days of COVID-19. The accuracy of enforcement and the
use of telehealth practices has been credited with the successful dates of enforcement were further confirmed through research
management of other infectious diseases, such as severe acute in the media. All the data were collected between July and
respiratory syndrome (SARS) and Middle East respiratory August 2020. This sampling strategy allows us to analyze the
syndrome (MERS), pointing to a possible role for telehealth in determinants of COVID-19 transmission during the early days
controlling pandemics [10]. In addition, other medical ICTs, of the pandemic.
such as computerized physician order entry (CPOE) and We limited our analysis to the countries that reported statistics
e-prescribing, have been acknowledged as drivers of health care related to the spread of COVID-19. For example, countries
improvements in quality and efficiency [11]. Third, countries without accurate statistics on deaths as of July 28, 2020, were
differed significantly across other dimensions, such as excluded. China, the country at the epicenter of COVID-19,
implementation of early lockdown and conformity to was excluded because the patterns of disease spread and
government policies because of their cultural differences, which governmental control differ greatly from those in other countries.
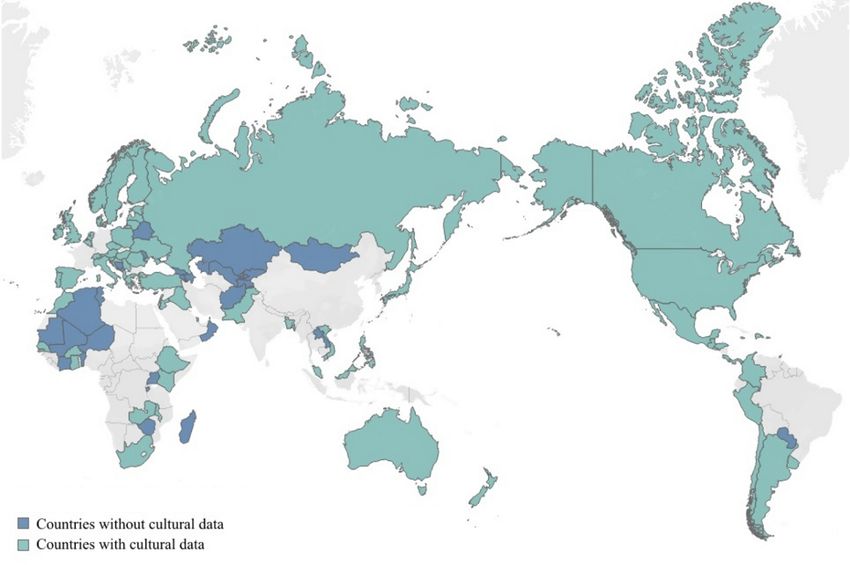
could have affected their success in social distancing. By matching the data for the social, economic, and demographic
Therefore, to gain broader insights, there is a need for statuses of countries, as well as their physical distancing and
country-level analysis of the national-level characteristics that health care–related ICT infrastructure, our final data set
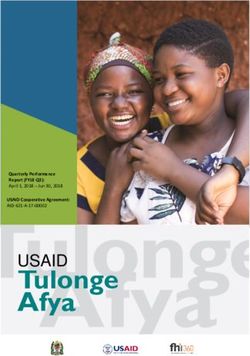
mitigate the spread of COVID-19 through successful distancing consisted of 98 countries. The countries included in our analysis
and improved medical practices. Nevertheless, previous studies are shown in Figure 1.
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 2
(page number not for citation purposes)
XSL• FO
RenderXJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
Figure 1. Map chart of the countries used in the analysis.
We focused on the following 3 dependent variables that stay-at-home orders during COVID-19 [27]. Next, the
represented the early state of the spread of COVID-19 in each MedicalICT variables involved the availability of a national
country: (1) the cumulative number of infections, (2) the fatality telehealth policy or strategy; availability of
rate, and (3) the number of days from initial infection to the government-supported multilingual health internet websites that
1000th infection. The first dependent variable represents the provide information; institutions with health care ICT training;
cumulative number of COVID-19 infections per country as of and national electronic health records (EHRs). These variables
July 28, 2020. The second dependent variable is the fatality represent MedicalICT because the variables relate to either
rate, which is the death toll over the cumulative number of reliable online sharing of medical information (government
infections. The third dependent variable is the transmission health internet sites and national EHRs) or the effective use of
speed of COVID-19 in its initial stage. This is represented for existing medical ICT technology (national telehealth policy and
each country by the number of days from the date of the first health care ICT training).
confirmed case to the date of the 1000th confirmed case. For
In particular, national telehealth policy is divided into the
the third dependent variable, countries with fewer than 1000
following 2 types: implied and stated. An implied telehealth
cases as of July 28, 2020, were excluded due to the difficulty
policy means that a country does not have a specific national
of calculating the speed of transmission.
telehealth policy or strategy, and such a policy is referred to in
The 2 main categories of our main independent variables were the overall national eHealth policy. Australia, Finland, and the
DistancingICT and MedicalICT. For DistancingICT, we chose United States are examples of such countries. The United
the following 2 variables based on findings of previous research: Kingdom and Norway, on the other hand, have separate
rate of credit card ownership and broadband internet speed. telehealth policies. For instance, the Norwegian Ministry of
Research and Markets reported that during the COVID-19 Health commissioned the Norwegian Centre for Telemedicine
pandemic, North America’s online sales surged, and credit cards to foster telehealth services, while assuring “the necessary
were the top payment method for these online sales [25]. actions to secure a successful dissemination of the services”
Previous studies further support the relationship between [28]. As such, countries with a specific national telehealth policy
e-commerce and credit card usage. Meyll and Walter surveyed or strategy, apart from a national eHealth strategy, are accounted
more than 25,000 US households and confirmed that individuals for as “stated” telehealth policy in our model. Although the term
using mobile payments are likely to use credit cards [26]. Given telehealth and eHealth are at times used interchangeably, they
this direct relationship between e-commerce and credit card differ in the purpose of use. While telehealth indicates usage of
usage, we identified credit cards as a major enabler of distancing ICT to promote long-distance care, eHealth indicates usage of
as they serve as alternatives to offline shopping. Broadband ICT for health in general. For example, in the United States,
internet speed also assists individuals to comply with before COVID-19, telehealth was only for people who needed
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 3
(page number not for citation purposes)
XSL• FO
RenderXJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
long-distance care due to limited access to nearby hospitals domestic product (GDP) at purchasing power parity (PPP) and
[29,30], while eHealth was widely applied to patients regardless unemployment rate as controls for the economic statuses of
of hospital accessibility. Accordingly, reimbursement on countries. Moreover, because several studies have indicated
telehealth has not been prioritized or sufficiently instituted, as that high temperatures and humidity may influence the infection
compared to that on general eHealth [30]. As such, telehealth, rate of COVID-19, we included annual rainfall and temperature
comparably, lacked clearly stated guidance before the pandemic. as controls [31]. Similarly, we added other controls, such as the
proportion of senior citizens, early implementation of a national
Our control variables were selected based on the results of prior
lockdown, and population density, to our model, along with 2
research that primarily focused on how the demographic,
culture-related variables, individualism and uncertainty
cultural, or political factors of a country affected COVID-19
avoidance. Overall, we selected additional control variables that
infections [19-22]. The larger the scale of these countries’
are identified as important determinants of the spread of
economies, the greater their potential for economic activities,
contagious viruses in the literature. Detailed explanations of
such as job hunting and international exchanges, that increase
our main variables and additional control variables are
the opportunities for infections. Thus, we included gross
summarized in Table 1.
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 4
(page number not for citation purposes)
XSL• FO
RenderXJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
Table 1. Variable descriptions.
Variable name Description (by country) Source Year measured
Dependent variable
Total casesa Number of individuals infected by COVID-19 Worldometers 2020
Fatality ratea Death rate against the number of confirmed cases (0-100) Worldometers 2020
Number of daysb Number of days elapsed from the first confirmed case to the Our World in Data 2020
1000th confirmed case
Control variable
GDPc PPPd GDP by PPP in billions World Bank 2019
Unemployment rate Unemployment rate (0-100) World Bank 2019
Population density People per square km of land area World Bank 2019
Percent aged 60 or over Percentage of people aged 60 or older United Nations 2019
Annual rainfall Average annual rainfall in mm World Bank 2019
Annual temperature Average annual temperature in °C World Bank 2019
Early lockdown Implementation of a national lockdown within 1 month of the Wikipedia, Press 2020
first confirmed case (dichotomous)
Individualism Cultural dimension score for preference for a loosely knit so- Hofstedee 2015
cial framework in which individuals are expected to take care
of only themselves and their immediate families (0-100)
Uncertainty avoidance Cultural dimension score for degree to which the members of Hofstede 2015
a society feel uncomfortable with uncertainty and ambiguity
(0-100)
ICTf infrastructure enabling
physical distancing
Credit card ownership The percentage of respondents who report having a credit card World Bank 2017
(aged 15+)
Broadband speed Broadband internet speed in Mbps Ookla 2019
Medical ICT infrastructure and
policy
Telehealth policy (stated) Country with a stated telehealth policy or strategy (1: yes, 0: World Health Organization 2015
otherwise)
Telehealth policy (implied) Country with no specific telehealth policy or strategy but is World Health Organization 2015
referred in an overall eHealth policy or strategy (1: yes, 0:
otherwise)
Government health websites Government-supported health internet sites providing informa- World Health Organization 2015
tion (1: available, 0: not available)
Training ICT health Institutions offering in-service training to health professionals World Health Organization 2015
on ICT for health (1: available, 0: not available)
National EHRg Country with a national EHR (1: available, 0: not available) World Health Organization 2015
a
Data collected as of July 28, 2020.
b
Data collected as of August 9, 2020.
c
GDP: gross domestic product.
d
PPP: purchasing power parity.
e
Definitions for Hofstede variables were obtained online [32].
f
ICT: information and communications technology.
g
EHR: electronic health record.
log (Total Casesi) = α1 + β11Controli +
Empirical Analysis
β12DistancingICTi + β13MedicalICTi + ε1i (1)
For each dependent variable, we specified our models as
follows:
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 5
(page number not for citation purposes)
XSL• FO
RenderXJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
Fatality Ratei = α2 + β21Controli + β22DistancingICTi interaction effects between MedicalICT variables. To ensure
+ β23MedicalICTi + ε2i (2) that independent variables in the analysis were not correlated,
we calculated variance inflation factor (VIF). All the
log (Number of Daysi) = α3 + β31Controli +
independent variables had VIF values less than 10, which
β32DistancingICTi + β33MedicalICTi + ε3i (3) indicates no multicollinearity violations [33]. Lastly, robust
where i denotes an individual country. standard errors were used to address any possible
heteroskedastic error.
For simplicity, an ordinary least squares estimator was used to
estimate the coefficients. The variables of main interest were We also conducted a subsample analysis in which we removed
DistancingICT and MedicalICT. The positive coefficient values countries with high population density. A prior study showed
of DistancingICT and MedicalICT in equations 1 and 2 positive correlation between population density and COVID-19
demonstrate that the variables increased the total number of infection [14]. Residents of densely populated countries
confirmed cases and the fatality rate. In contrast, the positive inevitably have interactions and contacts with more people
coefficients of DistancingICT and MedicalICT in equation 3 offline, whereas loosely populated countries can reduce such
represent a slower transmission speed. In all 3 models, we used possibilities when the infrastructure is built up. Moreover, less
the same set of control variables, including GDP PPP, populated countries may not have sufficient localized medical
unemployment rate, population density, elderly population ratio, services, thus requiring more medical ICT infrastructure than
annual rainfall, annual temperature, and early lockdown. For other countries. The needs and utilization of ICT would
normality, we log transformed all the variables, including total significantly vary by population density as well. Thus, to
cases and number of days, that displayed skewed distributions determine if our results might be biased by the inclusion of
and were nonnegative. countries with higher population density, we conducted an
additional analysis with only countries with lower population
For each dependent variable, our baseline model included all
density.
the main independent variables and controls, but without the 2
culture-related variables of individualism and uncertainty
avoidance. In the second model, we added these culture-related
Results
variables to the baseline model. We performed this separate Main Analysis
estimation because the content for the culture-related variables
was not available for all 98 countries. Thus, adding them to the The descriptive statistics for the variables used in this analysis
model reduced the sample size from 98 to 69. In the third model, and their correlations are presented in Table 2 and Multimedia
we added several interaction terms to check for possible Appendix 1, respectively.
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 6
(page number not for citation purposes)
XSL• FO
RenderXJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
Table 2. Summary statistics.
Variable name Mean (SD) value Minimum value Maximum value
Dependent variable
Total cases, n (98 countries) 113,021.2 (464,974.3) 20 4,498,343
Fatality rate, % (95 countries) 3.32 (3.18) 0.05 15.26
Number of days, n (91 countries) 51.02 (29.30) 11 139
Control variables
GDPa PPPb, US $ billions (98 countries) 734.76 (2,290.02) 9.03 21,427.70
Unemployment rate, % (98 countries) 6.55 (4.68) 0.09 28.18
Population density, persons/km2 (98 countries) 256.50 (919.32) 2.11 8737.02
Percentage aged 60 or older, % (98 countries) 15.32 (8.85) 3.19 34.02
Annual rainfall, mm (98 countries) 78.85 (54.56) 1.53 244.87
Annual temperature, °C (98 countries) 16.74 (8.57) −4.97 29.29
Early lockdown, dichotomous (98 countries) 0.36 (0.48) 0 1
Individualism, numeric score (68 countries) 42.85 (23.57) 6 91
Uncertainty avoidance, numeric score (68 countries) 66.97 (22.67) 8 100
Distancing-enabling ICTc infrastructure
Credit card ownership rate, % (98 countries) 21.23 (22.25) 0 83
Broadband speed, Mbps (98 countries) 45.47 (36.40) 4.18 191.93
Medical ICT infrastructure
Telehealth policy (stated), dichotomous (98 countries) 0.22 (0.42) 0 1
Telehealth policy (implied), dichotomous (98 countries) 0.37 (0.49) 0 1
Government health websites, dichotomous (98 countries) 0.61 (0.49) 0 1
Training ICT health, dichotomous (98 countries) 0.82 (0.39) 0 1
National EHRd, dichotomous (98 countries) 0.47 (0.50) 0 1
a
GDP: gross domestic product.
b
PPP: purchasing power parity.
c
ICT: information and communications technology.
d
EHR: electronic health record.
The results for regressions with robust standard error are shown higher than that for Fatality Ratei and Number of Daysi,
in Tables 3-5. For each dependent variable (number of indicating that the national characteristic variable used in the
confirmed cases [Table 3], fatality rate [Table 4], and analysis explains the cumulative number of infected better than
transmission speed [Table 5]), model 1 was the baseline model, the 2 other dependent variables. For Total Casesi, the R2 values
while model 2 added culture-related variables as controls. Model
for the 3 models were 61.5%, 73.3%, and 75.4%, respectively.
3 included all the control variables as well as the interaction
effects between distancing ICT and medical ICT variables Considering that the R2 averages of Fatality Ratei and Number
(DistancingICTi × MedicalICTi). As mentioned above, in the of Daysi were 44.5% and 37.0%, respectively, the overall
case of Number of Daysi, countries with no reported cases of explanatory power of the models for Total Casesi exceeded that
the 1000th infection as of July 28, 2020, were excluded from of the 2 others. Therefore, national characteristics account for
the analysis. As for the goodness of fit, R2 for Total Casesi was a significant portion of the differences in the cumulative number
of confirmed cases by country.
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 7
(page number not for citation purposes)
XSL• FO
RenderXJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
Table 3. Main regression results for the full sample with the dependent variable log (total cases).
Variable Model 1a (baseline P value Model 2b (including P value Model 3c (interaction P value
model), regression co- culture), regression effects), regression
efficient (SE) coefficient (SE) coefficient (SE)
General variable
log (GDPd PPPe) 1.136 (0.116)JMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
Table 4. Main regression results for the full sample with the dependent variable fatality rate.
Variable Model 1a (baseline P value Model 2b (including P value Model 3c (interaction P value
model), regression co- culture), regression effects), regression
efficient (SE) coefficient (SE) coefficient (SE)
General variable
log (GDPd PPPe) 1.635 (0.571) .005 1.573 (0.670) .02 1.993 (0.711) .007
Unemployment rate −0.042 (0.077) .59 −0.019 (0.095) .84 0.043 (0.099) .67
log (population density) 0.036 (0.623) .95 1.579 (0.805) .06 1.962 (0.843) .03
Percentage aged 60 or older 0.143 (0.07) .04 0.045 (0.101) .66 0.025 (0.103) .81
log (annual rainfall) 0.198 (0.835) .81 2.373 (1.325) .08 2.224 (1.346) .11
Annual temperature −0.011 (0.058) .85 −0.033 (0.082) .69 −0.041 (0.082) .62
Early lockdown −0.617 (0.737) .41 −1.000 (0.860) .25 −0.535 (0.931) .57
Individualism N/Af N/A 0.138 (0.031)JMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
Table 5. Main regression results for the full sample with the dependent variable log (number of days).
Variable Model 1a (baseline P value Model 2b (including P value Model 3c (interaction P value
model), regression co- culture), regression effects), regression
efficient (SE) coefficient (SE) coefficient (SE)
General variable
log (GDPd PPPe) −0.130 (0.044) .005 −0.08 (0.055) .15 −0.061 (0.058) .29
Unemployment rate −0.001 (0.006) .84 −0.001 (0.007) .87 0.004 (0.008) .61
log (population density) −0.068 (0.047) .16 −0.089 (0.064) .17 −0.079 (0.066) .24
Percentage aged 60 or older 0.005 (0.005) .30 0.01 (0.008) .23 0.003 (0.008) .71
log (annual rainfall) 0.032 (0.063) .62 −0.05 (0.104) .63 −0.057 (0.105) .59
Annual temperature 0.010 (0.005) .03 0.008 (0.007) .21 0.006 (0.007) .36
Early lockdown −0.096 (0.055) .09 −0.118 (0.069) .09 −0.118 (0.075) .13
Individualism N/Af N/A −0.002 (0.002) .46 −0.002 (0.002) .46
Uncertainty avoidance N/A N/A −0.003 (0.002) .17 −0.002 (0.002) .26
Distancing-enabling ICTg infrastructure
Credit card ownership rate −0.0003 (0.002) .88 −0.001 (0.002) .56 0.0004 (0.002) .88
log (broadband speed) −0.125 (0.113) .27 −0.208 (0.140) .14 −0.260 (0.146) .08
Medical ICT infrastructure
Telehealth policy (stated) 0.002 (0.066) .98 0.009 (0.081) .91 −0.328 (0.260) .21
Telehealth policy (implied) 0.001 (0.055) .99 0.042 (0.071) .56 −0.357 (0.183) .06
Government health websites 0.017 (0.061) .78 0.047 (0.085) .59 0.067 (0.117) .57
Training ICT health 0.055 (0.070) .44 0.042 (0.091) .65 −0.203 (0.128) .12
National EHRh −0.029 (0.049) .55 0.018 (0.062) .77 0.038 (0.096) .70
Interaction
Telehealth policy (stated)×government N/A N/A N/A N/A −0.015 (0.183) .94
health websites
Telehealth policy (implied)×government N/A N/A N/A N/A 0.02 (0.144) .89
health websites
Telehealth policy (stated)×training ICT N/A N/A N/A N/A 0.415 (0.304) .18
health
Telehealth policy (implied)×training ICT N/A N/A N/A N/A 0.506 (0.188) .01
health
Telehealth policy (stated)×national EHR N/A N/A N/A N/A −0.013 (0.178) .94
Telehealth policy (implied)×national N/A N/A N/A N/A −0.107 (0.159) .50
EHR
Constant 3.131 (0.520)JMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
the coefficient for the rate of credit card ownership was −0.057 sample. The results of the further analysis are shown in Tables
and significant (P=.04) (Table 4), suggesting that credit card S1-3 in Multimedia Appendix 2.
usage could have lessened the fatality rate. However, broadband
The key results are not remarkably different. Telehealth policy,
internet speed was not associated with any of the 3 measures
rather than technology itself, may promote efficient management
of transmission of COVID-19. Lastly, the presence of a
of COVID-19’s aftermath regardless of population density.
government-run health website showed a negative and
Unlike other national traits, the presence of telehealth policy
significant relationship with the total number of confirmed cases
(stated and implied) showed a negative association with the
(β=−0.440; P=.03) (Table 3). This implies that countries with
fatality rate when we omitted countries in the top 30% of
government-run health websites had 36% fewer confirmed cases
population density from our sample. These consistent results
than those without it.
highlight the importance of telehealth policy development in
The effects of DistancingICT and MedicalICT on the infection containment. However, it is noteworthy that credit
transmission speed of COVID-19 were not statistically card ownership was no longer significant. It is conceivable that
significant. For the interaction terms, although most coefficients countries with lower population density also have lesser rates
were insignificant, the interaction between implied telehealth of offline physical interaction, thus lowering the need for credit
policy and training ICT health was significant (β=0.506; P=.01) cards and online shopping.
(Table 5). Therefore, an implied telehealth policy may be more
effective when in-service training on ICT is provided to health Discussion
professionals (β=−0.357+0.506=0.149).
Principal Findings
Despite this not being the main focus of the study, it would be
meaningful to examine the effects of other control variables in In this study, we conducted exploratory research on the role of
light of the lack of country-level empirical studies on the spread national characteristics, especially in regard to ICT and medical
of COVID-19. Interestingly, early lockdowns, contrary to ICT infrastructure and concomitant policies that enable physical
expectations, were statistically uncorrelated with the total distancing, in the cumulative number of confirmed cases, fatality
number of infections and the fatality rate. Moreover, the rates, and initial transmission speed of COVID-19. The findings
coefficients for GDP with the total number of confirmed cases suggested that medical ICT policies, especially when in-service
and the fatality rate were 1.136 (PJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
Otherwise, prompt and precise communication attempts by the [21], but we used COVID-19 transmission data until July 28,
government could enhance information transparency and build 2020. It is challenging to refrain from public gatherings for
trust among the public, increasing the likelihood of public several months; the impact of uncertainty avoidance would be
compliance with suggested guidelines including vaccine weakened eventually.
acceptance [39].
The analysis result indicates that GDP is positively related to
Second, our findings suggest that possession of a credit card, a the number of total cases and the fatality rate. It is plausible that
widely used payment method for e-commerce [25,26], is related economically active countries, as represented by higher GDP,
to a lower fatality rate. The results varied when countries with involve more interactions between individuals, causing an
higher population density were omitted; this could happen inevitable increase in the number of infections. Alternatively,
because of either uneven development of contact-free systems in larger economies, the number of confirmed cases may reflect
in areas of lower density or prevention of crowding through better testing because these countries have the economic
widespread interventions such as contact tracing [40]. capacity to conduct more tests. Lastly, a higher proportion of
Nonetheless, such a finding denotes how credit card ownership the elderly population was correlated with a fewer number of
facilitates distancing compliance via online commerce. infections in total. The perceived risk of infection among elders
Alternatively, credit cards could have advanced financial might have influenced stay-at-home compliance, thus reducing
inclusion and cushioned the financial burden even in challenging physical contact and infections.
times. For instance, cardholders, especially those with a low
income, have benefited from financial assistance programs,
Implications for Research and Practice
including deferred payments, waived late fees, and even skipped The results of this study have several implications. Theoretically,
payments, from credit card issuers [41]. With financial the findings contribute to the effect of ICT infrastructure and
assistance, perceived burden would have been decreased, policy in epidemics. Prior studies have examined ICT adoption
fostering adherence to suggested guidelines [42]. intention of health care workers or how ICT use improves public
health or physical wellness in general [49-52]. Moreover, past
Third, we had interesting findings from the control variables research on ICT and health have paid attention to how ICT
on the spread of COVID-19 and its aftermath. Early lockdown mitigates various health-related challenges by providing access
enforcement displayed no relationship with COVID-19 to health-related information and fostering communication
transmission, although policymakers intuitively assumed that between patients and physicians [53-55]. For example, previous
compulsory restriction of contacts would be helpful in research found that telephone usage for health care lowered
diminishing the total number of infections, fatality rate, and depression rates [53] and increased immunization rates [54].
speed of transmission. Such intuitions are inferred from their However, they rarely showed interest for ICT use in the context
actions to tighten stay-at-home restrictions [27]. Our result is of epidemics, possibly due to its unlikelihood. Similarly,
consistent with the outcome of a preceding analysis that stated previous research on ICT policy in health care mainly focused
infection control was apparently effective before the mandate, on the “limitations concerning design and implementation of
and thus, voluntary social behavior, rather than legal policies” of public health improvement. Considering that ICT,
enforcement, is more crucial in combating a pandemic [43,44]. by its nature, enables faster communication to the public, it is
Stronger individualistic culture exhibited a higher fatality rate, surprising that the effect of ICT on epidemics, which are
whereas uncertainty avoidance showed no association with the widespread and abrupt, was not investigated sufficiently. In this
fatality rate. Related to individualism, a recent study clarified study, we have addressed this void by examining the relationship
the role of individualism-collectivism on the perceived risk of of ICT policy with total cases, fatality rate, and transmission
COVID-19 and sense of responsibility [45]. In essence, speed under the pandemic circumstance. Therefore, by
individuals with strong collectivistic orientation perceived expanding the scope of the role of ICT on people’s health, this
greater fear because of their higher physical and social study contributes to the literature on ICT and health-related
interconnection with others [45]. Moreover, challenges.
collectivism-oriented people, due to their strong sense of Practically, this study advocates autonomous use of medical
integrity and responsibility within the society, were willing to ICT, rather than playing it by the book. Contrary to the
follow containment guidelines, whereas individualism-oriented assumption that detailed and rigorous policy statements limit
people were not willing to follow guidelines [46]. This finding or prevent a wide range of health threats, such as smoking habits
is in line with preceding research that identified a relationship and cardiovascular diseases [56,57], the findings indicate that
between pathogen risk and societal individualism [47]. Societal stated medical ICT policy is in fact less likely to taper the
collectivism, which is more prevalent in Eastern cultures, did fatality rate than implied medical ICT policy. It is plausible that
“[serve] as a natural guard against disease transmission” [48]. relatively less restrictions are helpful for better medical services
A previous study also revealed that countries with relatively because for jobs with high variety tasks, such as medical
high uncertainty avoidance were less likely to engage in public practice, increased autonomy boosts the job performance of
gathering, potentially decreasing the number of infections and workers [58]. This finding is relevant in the broader context of
the fatality rate [21]. However, in this study, such an effect was the digital health field and provides significant empirical insights
not observed. The discrepancy could stem from different data that could improve the outcome of long-distance medical care
collection periods. Huynh conducted an analysis at the initial and guide future clinical decision support system (CDSS)-related
stage of COVID-19, from February 16, 2020, to March 29, 2020 strategies. This finding is aligned with WHO guidelines, which
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 12
(page number not for citation purposes)
XSL• FO
RenderXJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
suggest that “health workers may deviate from the lowered while modern medical care seeking behavior increased
recommendations” of a CDSS based on physicians’ own after kiosks were implemented and used for some years [59].
rationale [36], although an algorithm-based CDSS is In addition, although we included broadband speed in the model,
conventionally perceived as competent. As such, policymakers broadband coverage may also play a distinct role. For instance,
need to consider the independent and flexible decision-making high broadband speed offers fast communication online,
of physicians in the context of medical ICT usage. advocating real-time information sharing in dire situations such
as COVID-19 [9]. On the other hand, broadband coverage
Regarding distancing-enabling infrastructure, this study showed
enables seamless internet connectivity with personal devices;
that the government should prioritize providing ICT
when individuals get out of the service range at some point,
infrastructure that enables physical distancing in densely
they would not get broadband access. While lack of decent
populated areas. As the budget for ICT infrastructure is limited,
broadband coverage indicates inability to use the internet, lack
the government should strategically allocate funds to achieve
of decent broadband speed denotes unattainability of prompt
the greatest benefit. Especially, strategic budgeting is vital in
communication with others. Nevertheless, the correlation
developing countries where tax revenue is relatively insufficient.
between broadband coverage and speed was high
Because our findings show that differences in population density
(correlation=0.79). Accordingly, only one of them was used for
yield different outcomes of ICT implementation, governors can
our analysis to avoid a multicollinearity problem. Moreover,
consider investing in populous areas first, in order to maximize
there are other potential confounders, such as mask adherence,
the benefit with limited resources.
that were not included in our study. However, we believe that
Conclusions our culture-related variables, such as individualism and
Despite our findings on the relationship between national uncertainty avoidance, may account for such confounders [60].
characteristics and disease dispersion, our study is not without Lastly, because the COVID-19 pandemic has not ended, the
limitations. Although we included most established countries, long-term effect of ICT infrastructure and ICT policies could
we were not able to include all countries in our analysis. not be examined.
Consequently, the sample size for regression was small. In By conducting an analysis at the country level, we ensured the
addition, the data for medical ICT infrastructure and the rate of generalizability of our work and developed tentative guidelines
credit card ownership were not up-to-date. Therefore, their to control the spread of infectious diseases. We have especially
impacts during the observation period may not have been emphasized the importance of medical telehealth policies that
accurately estimated. However, it is important to note that ICT contribute to reduce the consequences of COVID-19. By
policy and infrastructure have a delayed “lag” effect on collecting updated COVID-19 data, future research can clarify
country-level outcomes because people need to adopt, trust, and the long-term effects of the aforementioned national traits. We
alter their behaviors in line with new technologies and policies hope that this study will broaden the scope of research on the
[59]. For instance, a recent study on the role of ICT in women’s impact of ICT infrastructure and policies, and give guidance
health outcomes showed that the maternal fatality rate was for better policy-making in the health care domain.
Acknowledgments
This work is partially supported by the Barun ICT Research Center at Yonsei University. This research was supported by the
Yonsei University Research Fund of 2019 (2019-22-0051). This research was also supported by the Yonsei Signature Research
Cluster Program of 2021 (2021-22-0006).
Conflicts of Interest
None declared.
Multimedia Appendix 1
Pairwise correlations (N=98).
[DOCX File , 21 KB-Multimedia Appendix 1]
Multimedia Appendix 2
Regression results for the sample with less population density (lower 70%).
[DOCX File , 40 KB-Multimedia Appendix 2]
References
1. WHO Coronavirus (COVID-19) Dashboard. World Health Organization. URL: https://covid19.who.int/ [accessed 2021-09-23]
2. Kupferschmidt K. Mutant coronavirus in the United Kingdom sets off alarms, but its importance remains unclear. Science.
2020 Dec. URL: https://www.sciencemag.org/news/2020/12/
mutant-coronavirus-united-kingdom-sets-alarms-its-importance-remains-unclear [accessed 2021-01-19]
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 13
(page number not for citation purposes)
XSL• FO
RenderXJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
3. Carter RW, Sanford JC. A new look at an old virus: patterns of mutation accumulation in the human H1N1 influenza virus
since 1918. Theor Biol Med Model 2012 Oct 12;9(1):42 [FREE Full text] [doi: 10.1186/1742-4682-9-42] [Medline:
23062055]
4. Grubaugh ND, Hanage WP, Rasmussen AL. Making Sense of Mutation: What D614G Means for the COVID-19 Pandemic
Remains Unclear. Cell 2020 Aug 20;182(4):794-795 [FREE Full text] [doi: 10.1016/j.cell.2020.06.040] [Medline: 32697970]
5. Jin X, Lian J, Hu J, Gao J, Zheng L, Zhang Y, et al. Epidemiological, clinical and virological characteristics of 74 cases of
coronavirus-infected disease 2019 (COVID-19) with gastrointestinal symptoms. Gut 2020 Jun 24;69(6):1002-1009 [FREE
Full text] [doi: 10.1136/gutjnl-2020-320926] [Medline: 32213556]
6. Socio-economic impact of COVID-19. United Nations Development Programme. 2020. URL: https://www.undp.org/
coronavirus/socio-economic-impact-covid-19 [accessed 2021-01-02]
7. Ghose A, Li B, Macha M, Sun C, Foutz NZ. Trading Privacy for the Greater Social Good: How Did America React During
COVID-19? SSRN Journal 2020:1-84. [doi: 10.2139/ssrn.3624069]
8. Coronavirus: Access to the internet can be a matter of life and death during a pandemic. Article 19. 2020. URL: https:/
/www.article19.org/resources/access-to-the-internet-can-be-a-matter-of-life-and-death-during-the-coronavirus-pandemic/
[accessed 2021-02-17]
9. Chiou L, Tucker C. Social distancing, internet access and inequality. National Bureau of Economic Research. 2020. URL:
https://www.nber.org/system/files/working_papers/w26982/w26982.pdf [accessed 2021-12-20]
10. Keshvardoost S, Bahaadinbeigy K, Fatehi F. Role of Telehealth in the Management of COVID-19: Lessons Learned from
Previous SARS, MERS, and Ebola Outbreaks. Telemed J E Health 2020 Jul 01;26(7):850-852. [doi: 10.1089/tmj.2020.0105]
[Medline: 32329659]
11. Draft OECD guide to measuring ICTs in the health sector. Organisation for Economic Co-operation and Development
(OECD). 2015. URL: https://www.oecd.org/health/health-systems/Draft-oecd-guide-to-measuring-icts-in-the-health-sector.
pdf [accessed 2021-12-19]
12. Mossong J, Hens N, Jit M, Beutels P, Auranen K, Mikolajczyk R, et al. Social contacts and mixing patterns relevant to the
spread of infectious diseases. PLoS Med 2008 Mar 25;5(3):e74 [FREE Full text] [doi: 10.1371/journal.pmed.0050074]
[Medline: 18366252]
13. Leung K, Jit M, Lau EHY, Wu JT. Social contact patterns relevant to the spread of respiratory infectious diseases in Hong
Kong. Sci Rep 2017 Aug 11;7(1):7974 [FREE Full text] [doi: 10.1038/s41598-017-08241-1] [Medline: 28801623]
14. Coccia M. Factors determining the diffusion of COVID-19 and suggested strategy to prevent future accelerated viral
infectivity similar to COVID. Sci Total Environ 2020 Aug 10;729:138474 [FREE Full text] [doi:
10.1016/j.scitotenv.2020.138474] [Medline: 32498152]
15. Denis E, Telle O, Benkimoun S. Mapping the lockdown effects in India: how geographers can contribute to tackle Covid-19
diffusion. The Conversation. 2020. URL: https://theconversation.com/
mapping-the-lockdown-effects-in-india-how-geographers-can-contribute-to-tackle-covid-19-diffusion-136323 [accessed
2021-12-19]
16. Bontempi E. First data analysis about possible COVID-19 virus airborne diffusion due to air particulate matter (PM): The
case of Lombardy (Italy). Environ Res 2020 Jul;186:109639 [FREE Full text] [doi: 10.1016/j.envres.2020.109639] [Medline:
32668559]
17. Al-Hasan A, Khuntia J, Yim D. Threat, Coping, and Social Distance Adherence During COVID-19: Cross-Continental
Comparison Using an Online Cross-Sectional Survey. J Med Internet Res 2020 Nov 18;22(11):e23019 [FREE Full text]
[doi: 10.2196/23019] [Medline: 33119538]
18. Altmann S, Milsom L, Zillessen H, Blasone R, Gerdon F, Bach R, et al. Acceptability of App-Based Contact Tracing for
COVID-19: Cross-Country Survey Study. JMIR Mhealth Uhealth 2020 Aug 28;8(8):e19857 [FREE Full text] [doi:
10.2196/19857] [Medline: 32759102]
19. Sebhatu A, Wennberg K, Arora-Jonsson S, Lindberg SI. Explaining the homogeneous diffusion of COVID-19
nonpharmaceutical interventions across heterogeneous countries. Proc Natl Acad Sci U S A 2020 Sep 01;117(35):21201-21208
[FREE Full text] [doi: 10.1073/pnas.2010625117] [Medline: 32788356]
20. Jinjarak Y, Ahmed R, Nair-Desai S, Xin W, Aizenman J. Accounting for Global COVID-19 Diffusion Patterns, January-April
2020. Econ Disaster Clim Chang 2020 Sep 04;4(3):1-45 [FREE Full text] [doi: 10.1007/s41885-020-00071-2] [Medline:
32901228]
21. Huynh TLD. Does culture matter social distancing under the COVID-19 pandemic? Saf Sci 2020 Oct;130:104872 [FREE
Full text] [doi: 10.1016/j.ssci.2020.104872] [Medline: 32550745]
22. Atalan A. Is the lockdown important to prevent the COVID-19 pandemic? Effects on psychology, environment and
economy-perspective. Annals of Medicine and Surgery 2020 Aug;56:38-42. [doi: 10.1016/j.amsu.2020.06.010]
23. Hofstede G. Culture's Consequences: International Differences in Work-Related Values. Beverly Hills, CA: SAGE; 1984.
24. Yeung AY, Roewer-Despres F, Rosella L, Rudzicz F. Machine Learning-Based Prediction of Growth in Confirmed
COVID-19 Infection Cases in 114 Countries Using Metrics of Nonpharmaceutical Interventions and Cultural Dimensions:
Model Development and Validation. J Med Internet Res 2021 Apr 23;23(4):e26628 [FREE Full text] [doi: 10.2196/26628]
[Medline: 33844636]
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 14
(page number not for citation purposes)
XSL• FO
RenderXJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
25. B2C e-Commerce and Payments in North America: An Assessment of COVID-19's Impact on the Industry. GlobeNewswire.
2020. URL: https://www.globenewswire.com/news-release/2020/07/06/2057872/0/en/
B2C-e-Commerce-and-Payments-in-North-America-An-Assessment-of-COVID-19-s-Impact-on-the-Industry.html [accessed
2021-02-17]
26. Meyll T, Walter A. Tapping and waving to debt: Mobile payments and credit card behavior. Finance Research Letters 2019
Mar;28:381-387. [doi: 10.1016/j.frl.2018.06.009]
27. Fancourt D. People started breaking Covid rules when they saw those with privilege ignore them. The Guardian. 2021.
URL: https://www.theguardian.com/commentisfree/2021/jan/02/follow-covid-restrictions-break-rules-compliance [accessed
2021-02-20]
28. Zanaboni P, Knarvik U, Wootton R. Adoption of routine telemedicine in Norway: the current picture. Glob Health Action
2014 Jan 09;7(1):22801 [FREE Full text] [doi: 10.3402/gha.v7.22801] [Medline: 24433942]
29. Jetty A, Moore MA, Coffman M, Petterson S, Bazemore A. Rural Family Physicians Are Twice as Likely to Use Telehealth
as Urban Family Physicians. Telemed J E Health 2018 Apr;24(4):268-276. [doi: 10.1089/tmj.2017.0161] [Medline:
28805545]
30. Kircher S, Mulcahy M, Kalyan A, Weldon C, Trosman J, Benson A. Telemedicine in Oncology and Reimbursement Policy
During COVID-19 and Beyond. J Natl Compr Canc Netw 2020 Sep 30:1-7. [doi: 10.6004/jnccn.2020.7639] [Medline:
32998106]
31. Wang J, Tang K, Feng K, Lv W, Chen K, Wang F. Impact of Temperature and Relative Humidity on the Transmission of
COVID-19: A Modeling Study in China and the United States. arXiv. 2020. URL: https://arxiv.org/abs/2003.05003 [accessed
2021-12-20]
32. National Culture. Hofstede Insights. URL: https://hi.hofstede-insights.com/national-culture [accessed 2021-12-17]
33. Hair J, Black W, Babin B. Multivariate Data Analysis. New York, NY: Pearson; 2009.
34. Jarvis CI, Van Zandvoort K, Gimma A, Prem K, CMMID COVID-19 working group, Klepac P, et al. Quantifying the
impact of physical distance measures on the transmission of COVID-19 in the UK. BMC Med 2020 May 07;18(1):124
[FREE Full text] [doi: 10.1186/s12916-020-01597-8] [Medline: 32375776]
35. Nancarrow SA. Six principles to enhance health workforce flexibility. Hum Resour Health 2015 Apr 07;13(1):9 [FREE
Full text] [doi: 10.1186/1478-4491-13-9] [Medline: 26264184]
36. WHO guideline: recommendations on digital interventions for health system strengthening. World Health Organization.
2019. URL: https://www.who.int/publications/i/item/9789241550505 [accessed 2021-12-20]
37. Komenda M, Bulhart V, Karolyi M, Jarkovský J, Mužík J, Májek O, et al. Complex Reporting of the COVID-19 Epidemic
in the Czech Republic: Use of an Interactive Web-Based App in Practice. J Med Internet Res 2020 May 27;22(5):e19367
[FREE Full text] [doi: 10.2196/19367] [Medline: 32412422]
38. Ngai CSB, Singh RG, Lu W, Koon AC. Grappling With the COVID-19 Health Crisis: Content Analysis of Communication
Strategies and Their Effects on Public Engagement on Social Media. J Med Internet Res 2020 Aug 24;22(8):e21360 [FREE
Full text] [doi: 10.2196/21360] [Medline: 32750013]
39. Marlow LA, Waller J, Wardle J. Trust and experience as predictors of HPV vaccine acceptance. Hum Vaccin 2007 Oct
27;3(5):171-175. [doi: 10.4161/hv.3.5.4310] [Medline: 17622801]
40. Hsu J. Population density does not doom cities to pandemic dangers. Scientific American. 2020. URL: https://www.
scientificamerican.com/article/population-density-does-not-doom-cities-to-pandemic-dangers/ [accessed 2021-02-23]
41. White A. Here’s our most up-to-date list of credit card financial assistance programs during coronavirus. CNBC. 2021.
URL: https://www.cnbc.com/select/credit-card-issuers-offer-customer-assistance-amid-coronavirus-financial-hardship/
[accessed 2021-07-16]
42. Kim E, Gupta S, Bolge S, Chen C, Whitehead R, Bates JA. Adherence and outcomes associated with copayment burden
in schizophrenia: a cross-sectional survey. J Med Econ 2010 Mar 17;13(2):185-192. [doi: 10.3111/13696991003723023]
[Medline: 20235753]
43. Kepp K, Bjornskov C. Lockdown Effects on Sars-CoV-2 Transmission – The evidence from Northern Jutland. medRxiv
2021:1. [doi: 10.1101/2020.12.28.20248936]
44. Gupta S, Nguyen T, Rojas F, Raman S, Lee B, Bento A, et al. Tracking public and private responses to the COVID-19
epidemic: Evidence from state and local government actions. National Bureau of Economic Research. 2020. URL: https:/
/www.nber.org/system/files/working_papers/w27027/w27027.pdf [accessed 2021-12-20]
45. Germani A, Buratta L, Delvecchio E, Mazzeschi C. Emerging Adults and COVID-19: The Role of Individualism-Collectivism
on Perceived Risks and Psychological Maladjustment. Int J Environ Res Public Health 2020 May 17;17(10):3497 [FREE
Full text] [doi: 10.3390/ijerph17103497] [Medline: 32429536]
46. Carvalho LDF, Pianowski G, Gonçalves AP. Personality differences and COVID-19: are extroversion and conscientiousness
personality traits associated with engagement with containment measures? Trends Psychiatry Psychother 2020
Jun;42(2):179-184 [FREE Full text] [doi: 10.1590/2237-6089-2020-0029] [Medline: 32294713]
47. Fincher CL, Thornhill R, Murray DR, Schaller M. Pathogen prevalence predicts human cross-cultural variability in
individualism/collectivism. Proc Biol Sci 2008 Jun 07;275(1640):1279-1285 [FREE Full text] [doi: 10.1098/rspb.2008.0094]
[Medline: 18302996]
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 15
(page number not for citation purposes)
XSL• FO
RenderXJMIR PUBLIC HEALTH AND SURVEILLANCE Eum & Kim
48. Travers M. Cultural Psychology Research Suggests The U.S. May Be Less Individualistic After Coronavirus Pandemic.
Forbes. 2020. URL: https://www.forbes.com/sites/traversmark/2020/03/23/
what-will-the-post-covid-19-world-look-like-lessons-from-cultural-psychology/?sh=69f540563f58 [accessed 2021-02-18]
49. Melas CD, Zampetakis LA, Dimopoulou A, Moustakis V. Modeling the acceptance of clinical information systems among
hospital medical staff: an extended TAM model. J Biomed Inform 2011 Aug;44(4):553-564 [FREE Full text] [doi:
10.1016/j.jbi.2011.01.009] [Medline: 21292029]
50. Jimoh L, Pate MA, Lin L, Schulman KA. A model for the adoption of ICT by health workers in Africa. Int J Med Inform
2012 Nov;81(11):773-781. [doi: 10.1016/j.ijmedinf.2012.08.005] [Medline: 22986218]
51. Ganju KK, Pavlou PA, Banker RD. Does Information and Communication Technology Lead to the Well-Being of Nations?
A Country-Level Empirical Investigation. MISQ 2016 Feb 2;40(2):417-430. [doi: 10.25300/misq/2016/40.2.07]
52. Venkatesh V, Rai A, Sykes TA, Aljafari R. Combating Infant Mortality in Rural India: Evidence from a Field Study of
eHealth Kiosk Implementations. MISQ 2016 Feb 2;40(2):353-380. [doi: 10.25300/misq/2016/40.2.04]
53. Simon GE, Ludman EJ, Tutty S, Operskalski B, Von Korff M. Telephone psychotherapy and telephone care management
for primary care patients starting antidepressant treatment: a randomized controlled trial. JAMA 2004 Aug 25;292(8):935-942.
[doi: 10.1001/jama.292.8.935] [Medline: 15328325]
54. Kaplan WA. Can the ubiquitous power of mobile phones be used to improve health outcomes in developing countries?
Global Health 2006 May 23;2(1):9-14 [FREE Full text] [doi: 10.1186/1744-8603-2-9] [Medline: 16719925]
55. Tan SS, Goonawardene N. Internet Health Information Seeking and the Patient-Physician Relationship: A Systematic
Review. J Med Internet Res 2017 Jan 19;19(1):e9 [FREE Full text] [doi: 10.2196/jmir.5729] [Medline: 28104579]
56. Busse R, Blümel M, Scheller-Kreinsen D, Zentner A. Tackling Chronic Disease in Europe: Strategies, Interventions and
Challenges. Geneva, Switzerland: World Health Organization; 2010.
57. Heidenreich PA, Trogdon JG, Khavjou OA, Butler J, Dracup K, Ezekowitz MD, et al. Forecasting the Future of
Cardiovascular Disease in the United States. Circulation 2011 Mar;123(8):933-944. [doi: 10.1161/cir.0b013e31820a55f5]
58. Dodd NG, Ganster DC. The interactive effects of variety, autonomy, and feedback on attitudes and performance. J. Organiz.
Behav 1996 Jul;17(4):329-347. [doi: 10.1002/(sici)1099-1379(199607)17:43.0.co;2-b]
59. Venkatesh V, Sykes TA, Zhang X. ICT for Development in Rural India: A Longitudinal Study of Women’s Health Outcomes.
MISQ 2020 Jun 1;44(2):605-629. [doi: 10.25300/misq/2020/12342]
60. Nørgaard M, Ehrenstein V, Vandenbroucke JP. CLEP 2017 Mar;Volume 9:185-193. [doi: 10.2147/clep.s129879]
Abbreviations
CDSS: clinical decision support system
DistancingICT: distancing-enabling ICT infrastructure
EHR: electronic health record
GDP: gross domestic product
ICT: information and communications technology
MedicalICT: medical ICT infrastructure and policy
OWID: Our World in Data
PPP: purchasing power parity
VIF: variance inflation factor
WHO: World Health Organization
Edited by G Eysenbach; submitted 08.06.21; peer-reviewed by J Khuntia, P Mechael, W Al-Chetachi; comments to author 01.07.21;
revised version received 25.08.21; accepted 23.11.21; published 07.01.22
Please cite as:
Eum NJ, Kim SH
The Role of Information and Communications Technology Policies and Infrastructure in Curbing the Spread of the Novel Coronavirus:
Cross-country Comparative Study
JMIR Public Health Surveill 2022;8(1):e31066
URL: https://publichealth.jmir.org/2022/1/e31066
doi: 10.2196/31066
PMID: 34817392
©Nam Ji Eum, Seung Hyun Kim. Originally published in JMIR Public Health and Surveillance (https://publichealth.jmir.org),
07.01.2022. This is an open-access article distributed under the terms of the Creative Commons Attribution License
(https://creativecommons.org/licenses/by/4.0/), which permits unrestricted use, distribution, and reproduction in any medium,
https://publichealth.jmir.org/2022/1/e31066 JMIR Public Health Surveill 2022 | vol. 8 | iss. 1 | e31066 | p. 16
(page number not for citation purposes)
XSL• FO
RenderXYou can also read