The Mini Clinical Evaluation Exercise (mini-CEX)
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Practical
Assessment
The Mini Clinical
Evaluation Exercise
(mini-CEX)
John J. Norcini, Foundation for Advancement of International Medical Education and
Research (FAIMER)
INTRODUCTION interact with a patient in any of a process. By 1972, the problems of The CEX
variety of settings including the assessing thousands of doctors evaluates the
T
he mini Clinical Evaluation hospital, outpatient clinic, and annually had become so great
A&E. The trainee conducts a that the oral examination was
trainee’s
Exercise or mini-CEX is a
method for simultaneously focused history and physical discontinued. In its place, the performance
assessing the clinical skills of examination and after the Board asked training programme with a real
trainees and offering them feed- encounter provides a diagnosis directors to assess the clinical patient
back on their performance. It is a and treatment plan. The faculty competence of candidates for
simple modification of the tradi- member scores the performance certification and recommended
tional bedside oral examination using a structured document and the use of a clinical evaluation
and because of that, it relies on then provides educational feed- exercise, or CEX, for trainees in
the use of real patients and the back. The encounters are intended their first postgraduate year.
judgments of skilled clinician to be relatively short, about 15
educators. This article describes minutes, and to occur as a routine The CEX was based on the
the mini-CEX, recounts how it was part of the training programme. bedside oral examination that was
developed, and then illustrates its Each trainee should be evaluated part of the certification process. A
use in the Modernising Medical on several different occasions by single faculty member evaluated
Careers (MMC) Foundation Pro- different faculty examiners. the trainee as he or she performed
gramme Assessment. a complete history and physical
Development of the mini-CEX examination on a pre-selected
BACKGROUND For the first four decades of its patient in the hospital. Trainees
existence, the American Board of were then expected to reach diag-
How the mini-CEX works Internal Medicine administered a nostic and therapeutic conclu-
In the mini-CEX, a single faculty traditional bedside oral examina- sions, present their findings, and
member observes the trainee tion as part of its certification produce a written report of the
June 2005 | Volume 2 | No 1| www.theclinicalteacher.com THE CLINICAL TEACHER 25
The CEX
presents
trainees with a
complete and
realistic clinical
challenge
patient. The faculty member then with real patients who exhibit ings, create a management
assessed the trainee’s performance the full range of conditions plan, and communicate this in
along several dimensions. The CEX seen in the clinical setting. both oral and written form.
took about two hours and by the
• The trainee is observed by a Despite its strengths, a grow-
early 1990s the vast majority of
skilled clinician-educator who ing research literature through
first year internal medicine train-
both assesses the performance the 1980s and 1990s showed that
ees in the United States were being
and provides educational the results of CEX were not likely
assessed by this method.
feedback. This enhances the to generalise very far beyond the
validity of the results and single encounter that was ob-
The CEX has at least three
ensures that the trainee served. This conclusion was based
important strengths.
receives the type of on numerous studies of the
• It evaluates the trainee’s per- constructive criticism that assessment of doctors.
formance with a real patient. should result in a reduction of
• The research showed that
In medical school, the Objec- errors and an improvement in
trainees’ performances with
tive Structured Clinical Exam- quality of care.
one patient were not a very
ination (OSCE) is often used
• The CEX presents trainees with good predictor of their per-
and it does an excellent job of
a complete and realistic clin- formances with other patients.
assessing clinical skills. As
ical challenge. They have to get Consequently, they needed to
trainees approach entry to
all of the relevant information be observed on different
practice, however, their edu-
from the patient, structure the occasions with different
cation and assessment needs
problem, synthesise their find- patients before drawing
to be based on performance
26 THE CLINICAL TEACHER June 2005 | Volume 2 | No 1| www.theclinicalteacher.com
reliable conclusions about the overall assessment of each encounters are much shorter The assessor
their competence. Observing trainee. This was also useful than two hours so the CEX and trainee
each trainee with several from the perspective of edu- does not assess the trainee’s
patients was also desirable cation, since trainees received ability to focus and prioritise
must agree to
from an educational perspec- feedback from different asses- diagnosis and management. and record an
tive, since different patients sors, each with their own educational
The mini-CEX is a response to
require different skills from specialties, strengths, and plan of action
some of the shortcomings of the
trainees and this significantly perspectives.
CEX and it is based on the educa-
broadens the range and rich-
• In terms of the method itself, tional interactions faculty rou-
ness of feedback they receive.
the CEX focused on the trai- tinely have with trainees during
• The research showed that the nee’s ability to be thorough teaching rounds. As in the CEX, one
assessors did not agree with with a single new patient in a faculty member observes a trainee-
each other even when they hospital setting that is unin- patient encounter. However, the
were observing exactly the fluenced by time constraints. encounter is focused, lasts roughly
same performance. Training of In contrast, different patients 15 minutes, and several encoun-
assessors is helpful to some pose different challenges and ters are included in the overall
degree but much larger the tasks or competencies assessment of a trainee. The
improvements in the reliabil- required of doctors vary con- encounters will portray a broader
ity and validity of the ratings siderably depending on the range of challenges because they
was achieved by including setting in which care is ren- can occur in a variety of settings
different faculty members in dered. Further, most patient (i.e., ambulatory/out-patient,
June 2005 | Volume 2 | No 1| www.theclinicalteacher.com THE CLINICAL TEACHER 27
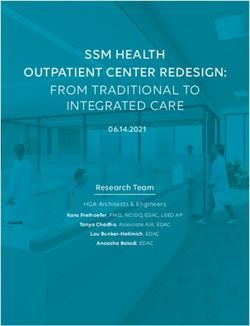
Routine Table 1
What must the assessors do?
discussion The assessor must ensure that the
Competence Descriptor of a Satisfactory Trainee patient is aware of the mini-CEX
among faculty and is typical of the trainee’s
History Taking Facilitates patient’s telling of story, effectively
will improve the uses appropriate questions to obtain accurate, workload. After observing the
quality of the adequate information, responds appropriately to encounter, the assessor completes
assessments verbal and non-verbal cues. the form in Table 1. As can be
seen, all of the competencies are
Physical Exam Follows efficient, logical sequence; examination
appropriate to clinical problem, explains to rated on a six-point scale where 1
patient; sensitive to patient’s comfort, modesty. and 2 are ‘below expectations’, 3
is ‘borderline’, 4 is ‘meets expec-
Professionalism Shows respect, compassion, empathy, establishes tations’, and 5 and 6 are ‘above
trust; Attends to patient’s needs of comfort,
expectations’ for the end of the
respect, confidentiality. Behaves in an ethical
manner, awareness of relevant legal frameworks.
second foundation year.
Aware of limitations.
The assessor is also required
Clinical Judgment Makes appropriate diagnosis and formulates a to give the trainee feedback
suitable management plan. Selectively orders/
immediately following the
performs appropriate diagnostic studies,
assessment. He or she must note
considers risks, benefits.
particular strengths and sugges-
Communication skill Explores patient’s perspective, jargon free, open tions for development on the
and honest, empathetic, agrees management form. In addition, the assessor
plan/therapy with patient. and trainee must agree to and
Organisation/Efficiency Prioritises; is timely. Succinct. Summarises. record an educational plan of
Overall Clinical Care Demonstrates satisfactory clinical judgment,
action. This feedback structure
synthesis, caring, effectiveness. Efficiency, is in line with evidence-based
appropriate use of resources, balances risks and good practice.
benefits, awareness of own limitations.
The assessor is also respon-
primary care, A&E department, competencies assessed and sible for recording information
and inpatient). The fact that descriptions of them can be seen about the encounter itself. This
several encounters are observed in Table 1. information ensures that there is
increases the quality of both the sufficient coverage of the curri-
assessment and the educational What must the trainees do? culum, provides some notion of
feedback. It also offers the oppor- Over the period of a year, the the nature and complexity of the
tunity to include different faculty trainees must get at least six patient’s problems, and provides
members in any one trainee’s different doctors (SpRs, Specialist information on mini-CEX know-
evaluation. Associate/Staff Grades, consult- ledge and experience. There is
ants, GPs) to assess them towards also research indicating that some
Foundation Programme the end of their rotation through of these factors are related to
Assessment different posts. For example, performance on the mini-CEX. For
The mini-CEX has been used in a trainees could ask a doctor to example, previous work has shown
variety of countries, specialties, observe them with the last that assessors tend to overcom-
clinical settings, and levels of patient on a ward round or the pensate by giving higher grades
training. It is currently being next patient coming to the GP when the patients’ problems are
evaluated as part of the National surgery. They should be perform- more complicated.
Health Service’s Modernising ing a task routinely expected of
Medical Careers Foundation them (e.g. clerking a new patient) What guidance is given?
Assessment Programme and its and the six encounters must cover Written guidance is given to both
use in this programme illustrates the main areas of the curriculum the trainees and the assessors. A
many of the issues involved in (http://www.mmc.nhs.uk/ description of the Foundation
implementing the mini-CEX. curriculum). After the encounter, Assessment Programme can be
trainees keep one copy of the found at http://www.mmc.
What does the mini-CEX assess? structured evaluation form for nhs.uk/. Trainees are provided
Consistent with the quality their portfolios, give one to their with a description of the mini-
improvement model used in the educational supervisor, and one CEX, advised about whom they
Foundation Programme, the mini- goes to the Trust Foundation should invite to be the assessor,
CEX is intended to identify areas Coordinator for forwarding to the what they should be assessed
of strength and weakness. The central administrative centre. doing, when it should be used,
28 THE CLINICAL TEACHER June 2005 | Volume 2 | No 1| www.theclinicalteacher.comMini-Clinical Evaluation Exercise (CEX). Courtesy of Department of Health, England.
and how it should work. They are Assessors are also given writ- the method, its purpose, and its
given copies of the forms that ten guidance that contains a place in the overall Foundation
need to be completed and description of the mini-CEX and programme. The competences to
responsibility for having them how it works. They receive infor- be assessed are listed and des-
done in a timely fashion. mation about the development of cribed for the satisfactory trainee
June 2005 | Volume 2 | No 1| www.theclinicalteacher.com THE CLINICAL TEACHER 29results will be incorporated into
an overall assessment profile for
each trainee.
CONCLUSION
The mini-CEX is a way of simulta-
neously assessing the clinical
skills of trainees and offering
them feedback intended to en-
hance their future performance.
Its validity and reliability derives
from the fact that trainees are
observed while engaged with a
series of real patients in different
practice setting and judgments
about the quality of those
encounters are made by skilled
educator-clinicians. Its educa-
tional effect is based on a signi-
ficant increase in the number of
occasions on which trainees are
directly observed with patients
and offered feedback on their
performance.
FURTHER READING
Norcini JJ, Blank LL, Arnold GK, Kimball
HR. The Mini-CEX (Clinical Evaluation
Exercise): A preliminary investigation.
Ann Intern Med 1995; 123: 795–99.
Norcini JJ, Blank LL, Duffy FD, Fortna G.
The mini-CEX: A method for assessing
clinical skills. Ann Intern Med
2003;138:476–481.
Day SC, Grosso LG, Norcini JJ, Blank LL,
Swanson DB, Horne MH. Residents’ per-
ceptions of evaluation procedures used
by their training program. J Gen Intern
Med 1990;5:421–426.
and special stress is placed on the • Improving the accuracy of
feedback to be given to trainees. ratings Elstein AS, Shulman LS, Sprafka SA.
Medical problem solving: An analysis of
Details of the administration are
• Improving the detection and clinical reasoning. Cambridge, MA: Har-
also provided. vard University Press, 1978.
recall of performance
Noel GL, Herbers JE, Caplow MP, Cooper
Although exhaustive training A number of national training GS, Pangaro LN, Harvey J. How well do
of the assessors is unlikely to be days have been provided and internal medicine faculty members
productive, a workshop to start further training is planned. evaluate the clinical skills of residents?
the process and routine discus- Ann Intern Med 1992;117:757–765.
sion among faculty will improve What happens with the results? Holmboe ES. The importance of faculty
the quality of the assessments Each of the rating forms is observation of trainees’ clinical skills.
and the feedback. Evidence-based returned to a central location and Acad Med 2004; 79: 16–22.
training should focus on four the data are entered into the Holmboe ES, Hawkins RE, Huot SJ. Direct
aspects of the process. computer. When six encounters observation of competence training: a
have been completed, the data randomized controlled trial. Ann Intern
• Reducing common errors (e.g. Med 2004; 140: 874–81.
are collated for the whole year
being too severe or too Holmboe ES, Yepes M, Williams F, Hout
and returned to the trainee via
lenient) SJ. Feedback and the mini clinical eval-
his/her programme director. The
uation exercise. J Gen Intern Med 2004;
• Understanding the dimensions educational supervisor will dis- 19(5 Pt 2): 558–61.
being assessed and the cuss the feedback with the trai-
standard of assessment nee. In addition, the mini-CEX
30 THE CLINICAL TEACHER June 2005 | Volume 2 | No 1| www.theclinicalteacher.comYou can also read