The Impact of COVID-19 on the Management of Hepatocellular Carcinoma in the Asia-Pacific
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

The Impact of COVID-19 on the Management of
Hepatocellular Carcinoma in the Asia-Pacific:
Lessons from the 1st Wave
Pierce K. H. Chow FRCSE PhD
Professor, and Program Director, Duke-NUS Medical School
Senior Consultant Surgeon, Singapore General Hospital and National Cancer Centre Singapore
Protocol Chair, The Asia-Pacific Hepatocellular Carcinoma Trials Group
1
Disclosures
Personal financial interests:
• Advisory role: Sirtex Medical, Ipsen, BMS, Oncosil, Bayer, New B Innovation, MSD, BTG
Plc, Guerbet, Roche, AUM Bioscience, L.E.K. Consulting, AstraZeneca, Eisai, Genentech,
IQVIA, Abbott
• Research funding: Sirtex Medical, Ipsen, IQVIA, New B Innovation, AMiLi, Perspectum,
MiRXES, Roche
Leadership roles:
• Founding President, College of Clinician Scientists, Academy of Medicine Singapore
• Protocol Chair, The Asia-Pacific Hepatocellular Carcinoma (AHCC) Trials Group
• Academic Vice-Chair (Research), Surgery Academic Clinical Program, SingHealth-Duke-
NUS
• Chief Medical Officer, AVATAMED PTE LTD
Restricted, Non-Sensitive
2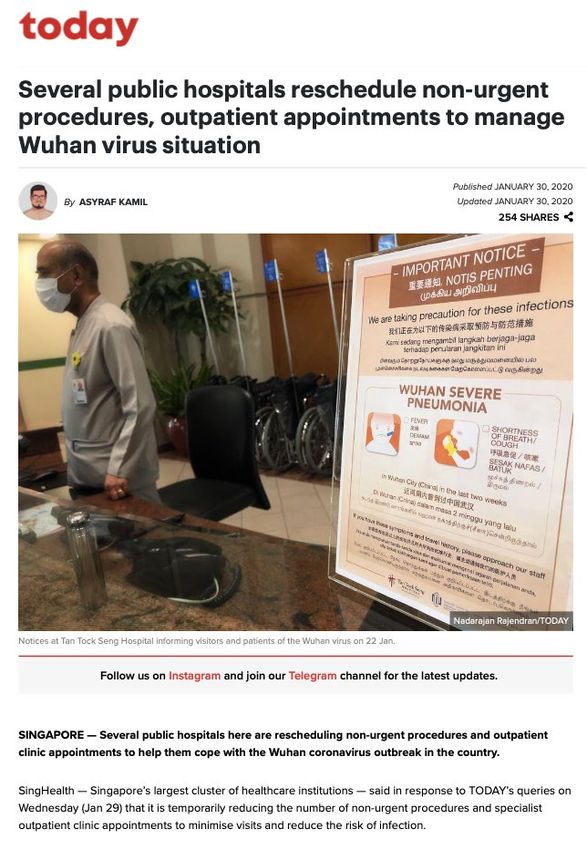
Overview
i. The biology and epidemiology of HCC and its significance in the Asia-Pacific
ii. How we responded to the first wave of the COVID-19 pandemic
iii.The impact of the response to the first wave of COVID-19 on cancer care globally
iv. How the COVID-19 Asia-Pacific HCC survey came about – the Hepatocellular
Carcinoma (HCC) Registry in Asia
v. Results of the Survey – The Impact of COVID-19 on the Management of Hepatocellular
Carcinoma in the Asia-Pacific
vi. Multiple waves of COVID-19 – Lessons Learnt from the First Wave
Restricted, Non-Sensitive
3
Hepatocellular Carcinoma (HCC)
• More than 1 million new cases a Regional variation in the estimated age-standardized
incidence rates of HCC
year, 80% of the disease burden in
the Asia-Pacific, but:
– until recently few efficacious systemic
therapies available
–
Chronic Viral Hepatitis
• Global HBV prevalence: 6%
• Global HCV prevalence: 2% WHO
• HBV is found mostly in the Asia-Pacific
• HBV accounts for > 50% of HCC but there is great
geographical variation
• HBV in HCC – 70% (Korea) 15% (Japan) 3% Sweden
• Modes of Transmission
– Sexual: sex workers and men who have sex with men are particularly at risk
– Parenteral: IV drug abuse, healthcare workers, contaminated blood transfusion
– Perinatal: new-borns with mothers who are HBeAg positive
Restricted, Non-Sensitive
5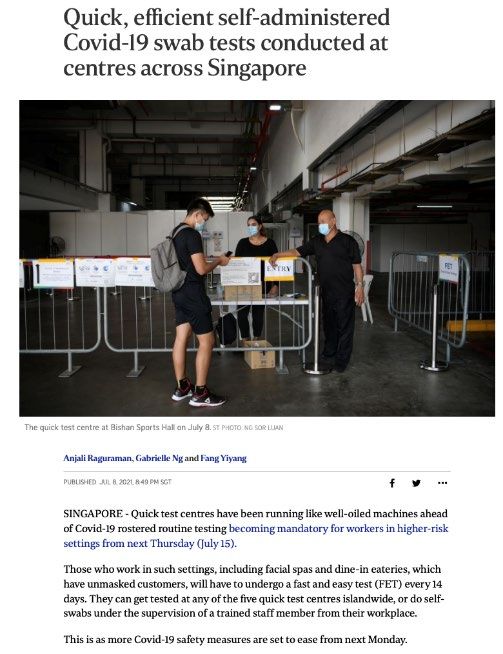
HCC spans a wide range of stages at diagnosis
Data from the Comprehensive Liver Cancer Clinic in NCCS (Chew et al 2021)
Early-stage HCC
• Lesions within the Milan criteria
• Criteria: Early Stage
– Solitary tumour < 5 cm OR < 3 tumours, each < 3 cm 129/578 patients 22.3%
AND no invasion of blood vessels and no distant
spread
Locally-advanced HCC Locally Advanced
• Lesions confined to the liver that are outside of the 266/578 patients 46.0%
Milan criteria with or without vascular invasion intermediate: 24%
• BCLC B + BCLC C without distant metastases with vascular invasion: 22%
Metastatic HCC Metastatic
• With good liver function (Child Pugh A or early B) 183/578 patients
• With poor liver function 31.7%
BCLC, Barcelona Clinic Liver Cancer staging.
Chow PK, et al. Liver Cancer. 2016;5:97–106. * Chew XH, el al. Liver Cancer 2021 DOI:10.1159/000513400
Restricted, Non-Sensitive
6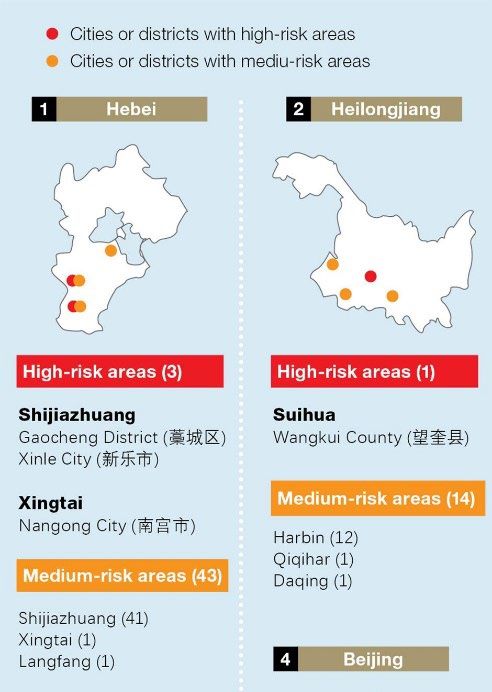
Best treatment outcomes for HCC depend on choice of
treatment modality appropriate for cancer stage
Adapted from
AASLD Guidelines
(2018),
requires in-patient stay ** *IV administration
** **oral administration
* Atezo-bev
*
Restricted, Non-Sensitive
7
COVID-19 and its Impact on the Liver
• Hepatic dysfunction has been seen in
14-53% of patients with COVID-19.
(Jothimani et al., 2020, J. Hepatol.)
• Hepatic involvement could be owing
to:
o Direct cytopathic effect of the virus
(angiotensin-converting enzyme 2 (ACE2)
is also expressed in the gastrointestinal
tract, vascular endothelium and
cholangiocytes of the liver)
o Greater than 30-fold increase in ACE2
expression in the liver of patients with hepatitis
C virus-related cirrhosis compared with healthy
individuals (Paizis G et al., 2005, Gut)
o Uncontrolled immune reaction
o Sepsis
o Drug-induced liver injury
Restricted, Non-Sensitive
8
Research from A*STAR and NCCS: Single-Cell RNA-seq Reveals Angiotensin-Converting Enzyme 2
and Transmembrane Serine Protease 2 Expression in TROP2+ Liver Progenitor Cells: Implications
in Coronavirus Disease 2019-Associated Liver Dysfunction (Seow et al., 2021, Front. Med.)
Tissue Types ACE2
• Co-expression of angiotensin-
converting enzyme 2 (ACE2) and
transmembrane serine protease 2
(TMPRSS2) in a specific TROP2+
liver progenitor population of
cirrhotic livers
• Indicating SARS-CoV-2 infection
preferentially infect TROP2high TMPRSS2 TROP2
cholangiocyte-based progenitors,
compromising the regenerative
ability of an infected liver and/or
contributing to liver pathology
Restricted, Non-Sensitive
9
How we responded to the first wave of the
COVID-19 pandemic
Restricted, Non-Sensitive
10The world initially reacted to COVID-19 as if it were
SARS or MERS
SARS MERS COVID-19
Nov 2002 – Jul 2003 Apr 2012 – Dec 2019 –
(declared worldwide (re-emerges intermittently) (multiple waves, ongoing)
containment)
8098 cases, 774 deaths 2574 cases, 886 deaths 197 million cases, 4.2 million deaths
no diagnostic kit, no vaccine diagnostic kit available vaccines, diagnostic kits available
global case fatality rate 11% global case fatality rate 34.4% global case fatality rate ~3.4%
Controlled with strict public Controlled with strict public
health measures health measures
Does the strategy that worked for SARS and MERS work in COVID-19?
Restricted, Non-Sensitive
11SARS – The (visceral) SGH Experience
• Cases were initially defined according to syndromic features in the absence of diagnostic
tests. No diagnostic kits – no PCR, Rapid antigen test, no vaccine
• 76% of infections in Singapore were traced to hospitals, and about 42% of the SARS
patients were healthcare workers
o SARS was very deathly (case mortality in Singapore was 13.9%), with HCW colleagues dying from
the disease (strong visceral memories)
o Within the the SGH General Surgery wards, an index case was traced whose infection led to 38
cases of SARS (in healthcare workers, patients and visitors) in wards and another 12 cases across
the rest of the hospital.
• Drastic public health measures were taken which brought
SARS under control within months. No vaccines
• This experience shaped our initial response to the 1st wave
of COVID-19
Chow et al. (2004), Emerg. Infect. Dis.
SARS Investigation Team from DMERI and SGH (2005), Rev. Med. Virol.
Restricted, Non-Sensitive
12Response to COVID-19
Deferring non-urgent hospital visits to reduce footfall and re-
prioritize resources
Jan 2020 May 2021
• Up to 20% of patients
with COVID-19
infections require in-
patient or intensive
care/assisted
ventilation support
Is this sustainable for multiple
waves?
Restricted, Non-Sensitive
13Patients deferred hospital visits due to patient’s own fear of
contracting COVID-19 at healthcare institutions
From a consumer survey conducted by the Society of • Patients with cancer are more
Cardiovascular Angiography & Intervention in May 2020:
susceptible to infection due to the
immunosuppressive state caused
by both anticancer treatment and
surgery.
• A meta-analysis in China revealed
an elevated case-fatality rate of
5.6% for cancer patients. (Wu et al.,
2020, JAMA)
Restricted, Non-Sensitive
14Response to COVID-19
Reduced accessibility to healthcare facilities
• Large countries such as the United States and China Recommendations include:
have imposed statewide/city level restrictions • Set days of quarantine
• Provision of negative RT-PCR test
• Cessation of public transportation network during results
lockdowns • Avoiding non-essential travels
Suspension of all cross-city buses, passenger flights and
trains to medium-/high-risk regions
Restricted, Non-Sensitive
15The impact of the response to the first wave of
COVID-19 on cancer care globally
Restricted, Non-Sensitive
16Response to COVID-19
Postponement of cancer screening services
Based on ACS Guidelines (2020) April 2021: Restarting of cancer
screening with careful
April 2020: No one should consideration of the associated
go to a healthcare facility for risks and benefits of screening,
routine (non-diagnostic and ensuring safety for both
cancer screening) until patients and healthcare
further notification
personnel.
Jan – Jun 2020: Reduction of cancer
screening by 60-99% in the United Based on ASCO
States Guidelines (2020)
August 2020: Continued
postponement of most cancer
screening procedures (e.g. screening
Resulted in a screening deficit and its
mammograms and colonoscopies) to
conserve healthcare resources and downstream consequences
reduce patient contact with healthcare
facilities.
Restricted, Non-Sensitive
17COVID-19 disrupted care for patients with cancer
• Oncologists around the world had resources directed away from them as hospitals battle
COVID-19 and had to balance the delivery of high-quality continuous, unfragmented
cancer care while minimizing patients’ risk of exposure to COVID-19
Jazieh et al. (2020, JCO Glob.
Oncol.) study revealed that an
overwhelming majority of 88% of
the 356 participating sites faced
challenges in providing usual cancer
care to patients.
Restricted, Non-Sensitive
18Delay in initiation of treatment for HCC
• First principle of modification to
clinical practice of HCC is to defer
treatment to reduce the spread of
COVID-19 amongst cancer
patients.
• In Iavarone et al. (2020, Ann.
Oncol.), the HCC treatments for (Chan and Kudo, 2020, Liver
Cancer)
42 patients in Milan were
o Scheduled with a delay of >= 2
months in 11 (26%) patients
o Thermal ablation was carried out
instead of preplanned surgical
resection
Restricted, Non-Sensitive
19Routine Workflow of HCC Management
Adapted from AASLD Guidelines (2018),
DIAGNOSIS TREATMENT
SURVEILLANCE
Surveillance ultrasound Diagnostic imaging for HCC with a
examination and plasma multiphasic CT or MRI
AFP every 6 monthly Negative
Benign lesions (L1-RADS 1 and
2)
If either/both found
to be positive (i.e. Low probability of HCC (L1-
lesions > 1cm RADS 3)
and/or AFP above
upper limit of Probable HCC (L1-RADS 4)
normal (e.g. >=
Depending on the stage of the
20ng/mL) Definitively HCC (L1-RADS 5)
disease, various curative and systemic
therapies are initiated.
20COVID-19 resulted in altered allocation of healthcare resources
that directly impacts on the Workflow in HCC care
• COVID-19 has been a litmus test for the resilience of health systems and societies
around the world.
• With resources reallocated to managing the pandemic, cancer care is deprioritized.
1. Deferring non-urgent hospital visits,
admissions and investigations 4 5
• Decrease footfall in the hospitals
1 2
• Conserve resources
2. Suspension of screening programs
3. Delays in diagnosis/later stages of
cancer at diagnosis 3
4. Delays in initiation of treatment/limited
treatment options owing to late
diagnosis
5. Interruptions to on-going treatment
Restricted, Non-Sensitive
21Disruption to clinical trials
• Due to social distancing policies, protocol deviations are expected to increase owing to
delay in ongoing assessments, implementation of alternative processes etc.
• COVID-19 has reportedly resulted in delays in 16 clinical trials for HCC across Phase I–
III (Pharmaceutical Technology, https://www.pharmaceutical-technology.com/comment/hepatocellular-carcinoma-
covid-19/)
o Most notable being the Phase II/III TACE-3 trial investigating the use of Nivo + TACE for intermediate
HCC patients
• The SingHealth Experience
o Suspension of all new/ongoing studies/trials with
patient/subject contact
o Postponement of follow-up visits and therefore,
biosamples collection
o Suspension of all benchwork, resulting in the delay in
the generation of research data
Adapted from: NCCS Business Continuity Plan dated 30 Mar 2020
Restricted, Non-Sensitive
22Singapore and COVID-19: The First Wave
Apr 20
Highest recorded
1,426 cases in a
Mar 28 single day owing
to dormitory
Dormitories clusters
cluster
Apr 17 Jun 1 Aug 8
Jan 23 Circuit breaker
Circuit breaker is
lifted, Singapore
Closure of the S11
Singapore’s first measures kick in dormitory cluster @
enters Phase 1 of
case, a 66-years old (default working from Punggol (largest
reopening
man from Wuhan is home, disallow dining dormitory cluster)
in)
2020 confirmed
Apr 30 Jul 21
Mar 21 Suspension of Closure of the
Singapore Sungei Tengah
sees its first 2
operations for 18
months at Changi Jun 19 Lodge cluster (2nd
deaths due to Airport Terminal 2 Singapore moves to largest dormitory
the virus Phase 2 of reopening. cluster)
Apr 14 Dining in is permitted
and households can
Mask-wearing receive up to 5 visitors
outside of one’s
house becomes
mandatory
Strict measures to contain COVID-19, reallocation of healthcare resources to address the pandemic
Restricted, Non-Sensitive
23Singapore and COVID-19: Adjusting to the new norm
Dec 28 May 7 Jul 16
Singapore moves into Jurong Fishery
Phase 3 of reopening. JEM/Westgate
port cluster
Households can cluster
receive up to 8
visitors. Dec 30 Feb 22
Introduction of the Commenced May 16 Jun 13 Jul 20
COVID-19 vaccine
for healthcare
vaccination for
seniors aged above
Return to Phase 2 Bukit Merah Return to Phase 2 Aug 24
(Heightened Alert) View cluster (Heightened Alert) Dormitory
workers 70 years old measures measures cluster
2021
Nov 9
Announcement of the Apr 28 Jun 13 Aug 3
efficacy of the Pfizer Lifting of Phase 2 CGH cluster
TTSH cluster
COVID-19 vaccine in (Heightened Alert)
a Phase 3 study measures
Nov 16 May 5
Announcement of the Changi Airport
cluster
Jun 29
efficacy of the KTV cluster
Moderna COVID-19
vaccine in a Phase 3
study
Moving from COVID-19 pandemic to ENDEMIC
Restricted, Non-Sensitive
24More than one wave – COVID-19 Statistics in Singapore
As of 24 Aug 2021,
Active Cases
Vaccination introduced
870
Hospitalised Community Facilities
339 531
Deaths
50
Retrieved from: https://www.worldometers.info/coronavirus/country/singapore/
Restricted, Non-Sensitive
25How the COVID-19 Asia-Pacific HCC Survey came
about?
The Hepatocellular Carcinoma Registry in Asia
(AHCC08)
Restricted, Non-Sensitive
26Leveraging on current member sites of the AHCC Trials Group
Nov 2019 1st Wave 2nd Wave
COVID-19
AHCC08 HCC
Registry in
Jun 2016 Dec 2020
Asia
Restricted, Non-Sensitive
27Participating Centres for AHCC08 – HCC Asia Registry
Status: 2,533 patients from 33 sites recruited and follow-up to 30 Jun 2020
China (1,078 patients/6 sites) Australia (114 patients/2 sites)
• Nanjing Bayi Hospital, NJB • Royal Prince Alfred Hospital, RPA
• Zhongshan Hospital, Fudan University • Royal Adelaide Hospital, RAH
Shanghai, ZSH South Korea (239 patients/8 sites)
• Beijing Cancer Hospital, BCH • Samsung Medical Center, SSM
• Guangxi Medical University Cancer Centre, • Ajou University Hospital, AUH
GXM • Asan Medical Centre, AMK
• Second Affiliated Hospital Zhejiang University • Anam Hospital, KUA
School of Medicine, SAH • Seoul National University Bundang Hospital,
• Harbin Medical University Cancer Hospital, SNU
HMU • Severance Hospital, Yonsei University College
Thailand (50 patients/2 sites) of Medicine, SYH St Mary's Hospital, SMH
• Siriraj Hospital, Mahidol University, SHM • St Vincent Hospital, Catholic University
• National Cancer Institute, NCI Taiwan (374 patients/5 sites) Medical College, SVH
Hong Kong (94 patients/1 site) • National Taiwan University Hospital, NTU Japan (347 patients/5 sites)
• Queen Mary Hospital • Taipei Veterans General Hospital, TVG • Kyorin University School of Medicine, KUM
Singapore (189 patients/3 sites) • Chang Gung Memorial Hospital – KS, CGM • University of Tokyo, UTJ
• National Cancer Centre, NCS • China Medical University Hospital, CMU • Kinkai University Hospital, KKU
• Singapore General Hospital, SGH • National Cheng Kung University Hospital, • National Cancer Centre, NCJ
• National University Hospital, NUH NCK • National Center of Global Health and
New Zealand (48 patients/1 site) Medicine, NCM
• Auckland City Hospital, ACH
Restricted, Non-Sensitive
28Multi-Center Clinical Trials of the AHCC
AHCC01: NCT00003424. Randomised Trial of Tamoxifen Versus Placebo for the Treatment of Inoperable 1997 – 2000
Hepatocellular Carcinoma. NMRC
AHCC02: NCT00041275. Randomized Double Blind Trial Of Megestrol Acetate Versus Placebo For The 2002 – 2007
Treatment Of Inoperable Hepatocellular Carcinoma. NCC,
SingHealth
AHCC03: NCT00027768. Randomised Trial of Adjuvant Hepatic Intra-Arterial Iodine-131-Lipiodol Following 2002 – 2008
Curative Resection of Hepatocellular Carcinoma NMRC
AHCC04: NCT00247260. Phase II dose escalation trial of intra-tumoral Brachysil® in inoperable HCC 2005 – 2006
PSiOncology
AHCC05: NCT00712790. Phase I/II Study of SIR-Spheres Plus Sorafenib as First Line Treatment in Patients 2008 – 2009
With Non-Resectable Primary Hepatocellular Carcinoma NMRC, Bayer,
Sirtex
AHCC06: NCT01135056. Phase III Multi-Centre Open-Label Randomized Controlled Trial of Selective Internal 2010 – 2015
Radiation Therapy (SIRT) Versus Sorafenib in Locally Advanced Hepatocellular Carcinoma NMRC, Sirtex
(SIRveNIB)
AHCC07: NCT03267641. Precision Medicine in Liver Cancer across an Asia-Pacific Network (PLANet Study) 2016 – 2021
NMRC
Restricted, Non-Sensitive
29Ongoing/Upcoming Clinical Trials of the AHCC
AHCC09: A multi-national, double-blind, placebo-control, randomised phase II trial to compare the safety 2022 –
and efficacy of SIR-Spheres (Y-90 resin microspheres) followed by atezolizumab plus A*STaR, Roche,
bevacizumab verses SIR-Spheres in patients with locally advanced hepatocellular carcinoma SIRTex,
(STRATUM)
AHCC10: NCT04965259. Early Detection of Hepatocellular Carcinoma (HCC): miRNA, Microbiome and 2021 – 2025
Imaging Biomarkers in the Evolution of Chronic Liver Disease in a High-risk Prospective A*STaR, MIRXES,
Cohort (ELEGANCE) AMILI, Perspectum
AHCC11: Prospective Cohort Study of Changes in Circulatory microRNA after Surgical Resection of 2021 – 2025
Hepatocellular Carcinoma (PROSECT) A*STaR, MIRXES
Restricted, Non-Sensitive
30Rationale for the AHCC08 –
Hepatocellular Carcinoma (HCC) Registry in Asia
• Most previous studies do not represent real world data as they were collected from
randomized controlled trials and case series from tertiary clinical centers.
• Real World Data on the presentation, clinical trajectory and management of HCC in Asia-
Pacific must be prospectively collected for the development of effective public health
strategies and to inform the development of therapeutics.
• In this study, patients are treated, managed and followed up according to local clinical
practice.
• Patient-reported outcomes are collected using paper questionnaires during routine visits.
Restricted, Non-Sensitive
31Leveraging on the AHCC Trials Group
Nov 2019 1st Wave Subsequent Waves
COVID-19
Survey
Feb 2019 May 2019 Feb 2020 May 2020
AHCC08 HCC
Registry in
Jun 2016 Dec 2020
Asia
Restricted, Non-Sensitive
32The Impact of COVID-19 on the Management of Hepatocellular
Carcinoma in Asia Pacific Survey
Purpose: Study Design:
To evaluate the impact of the pandemic on • Of the 55 hospitals invited, we received
the diagnosis, treatment and consultation gathered responses from 27 hospitals in 14
Asia-Pacific countries and obtained data
methods for patients with HCC during the
from a corresponding pre-pandemic period
initial wave of the COVID-19 pandemic. (Feb – May 2019) and from the 1st wave of
the pandemic (Feb – May 2020).
Outcomes: • Information collected included delays in
Gandhi M, Ling WH, Chen CH, Lee JH, Kudo M, diagnosis and treatment, changes in
Chanwat R, Strasser SI, Xu Z, Lai SH, Chow PKH treatment modalities and complication rates,
(2021) Impact of COVID-19 on Hepatocellular changes in patient enrollment in clinical trials
Carcinoma Management: A Multi-country and Region and modes of patient consultation.
Study, J. Hepatocellular Carcinoma, 8:1159-67.
https://doi.org/10.2147/JHC.S329018
• Information collected was stratified by BCLC
staging
(IF: 5.828)
Restricted, Non-Sensitive
33Best treatment outcomes depend on choice of treatment
modality appropriate for cancer stage
Adapted from
AASLD Guidelines
(2018),
requires in-patient stay ** *IV administration
** **oral administration
* Atezo-bev
*
Restricted, Non-Sensitive
34Data Collected (2019 vs 2020)
Diagnosis Outcomes
• Delays in diagnosis • Peace vs Wartime (COVID-19)
• Reasons for delays • Decease in outpatients
• Length of delay • Mortality
• % of patients who experienced delay • Staging at presentation
• % of patients where there was no impact • Patients lost to follow up – Registry data % of
Treatment patients who missed follow-up visits during
• Delays in treatment Jan-Mar 20 and Mar-Jun 20
• Reasons for delays • Inpatient due to HCC related
• Length of delay • HCC patients contracted COVID
• % of patients who experienced delay Pandemic Control
• % of patients where there was no impact • Health care system
• Change in treatment • Policy to control pandemic
• Cancellation in treatment • Past experience and preparedness to
pandemic
Restricted, Non-Sensitive
35Participating Centres for the Survey
Status: Of the 55 sites that the survey was sent out to, 27 sites from 14 countries responded (49.1%),
and provided data on 2,789 (pre-pandemic) and 2,045 (1st wave of the pandemic) patients
Australia Japan Singapore
• Royal Prince Alfred Hospital • Kindai University Hospital • Khoo Teck Puat Hospital
Brunei • The University of Tokyo • National Cancer Centre Singapore
• Jerudong Park Medical Centre • National Centre for Global Health South Korea
China and Medicine • Korea University Anam Hospital
• Guangxi Medical University Malaysia • Seoul National University Bundang
Cancer Centre • Hospital Selayang Hospital
• Zhejiang University School of Mongolia • Catholic University Medical College
Medicine • National Cancer Centre of Mongolia Taiwan
Hong Kong Myanmar • China Medical University Hospital
• Queen Mary Hospital • Yangon GI & Liver Centre • National Taiwan University Hospital
Indonesia Philippines • Taipei Veterans General Hospital
• Medistra Hospital • Davao Doctors’ Hospital • National Cheng Kung University
• Makati Medical Centre Hospital
• St Luke’s Medical Centre Thailand
• The Medical City • Chulabhorn Hospital
• National Cancer Institute
Restricted, Non-Sensitive
36Results of the Survey – The Impact of COVID-19
on the Management of Hepatocellular Carcinoma
in the Asia-Pacific
Restricted, Non-Sensitive
37Reduction in the number of new patients diagnosed with HCC
Decline of average 27.6 patients
Greatest reduction in per institution from the pre-
Myanmar, Indonesia, pandemic period (103.2
Philippines and Hong patients/institution to 75.6
Kong patients/institution)
Suspension/de-
prioritization of cancer
screening programs and
appointments
Increase in Malaysia and
no change for Brunei
Restricted, Non-Sensitive
38Delays in diagnosis of new HCC cases
No delay Delay
On average, 48.3% of the institutions reported delays in diagnosis of new HCC cases
owing to COVID-19 across all stages.
Restricted, Non-Sensitive
39Delay in initiating HCC treatment
No delay Delay
On average, 62.1% of the institutions reported delays in the initiation of HCC treatment
owing to COVID-19 across all stages.
Restricted, Non-Sensitive
40Changes in treatment modalities
No change Change
31% of the institutions reported changes in treatment modalities for patients of BCLC 0/A and
B stages, while 17.2% of the institutions reported changes in treatment modalities for BCLC
C patients (BCLC C is treated with either oral or IV systemic therapy)
Restricted, Non-Sensitive
41Best treatment outcomes depend on choice of treatment
modality appropriate for cancer stage
Adapted from
AASLD Guidelines
(2018)
requires in-patient stay ** *IV administration
** **oral administration
* Atezo-bev
*
Restricted, Non-Sensitive
42Changes in treatment modalities for BCLC 0/A and B patients
No Yes
Decreased proportion
treated with elective surgery
Increased proportion treated
with oral HCC therapy
(usually treated with inpatient loco-
regional therapy)
On average, 46.6% of the institutions reported a decrease in proportion of patients of BCLC
0/A/B stages treated with elective surgery during COVID-19.
(surgical resection is potentially curative in BCLC 0/A)
Restricted, Non-Sensitive
43Changes in treatment modalities
Clinical trial Randomized patients mOS, months
Sorafenib1(oral) population at baseline, % (95% CI)
2007 (SHARP trial)
Advanced-stage HCC sorafenib 10.7 (9.4-13.3)
BCLC stage A: 0
2008 Child-Pugh class A-B BCLC stage B: 17 placebo 7.9 (6.8-9.1)
BCLC stage C: 82
ECOG PS ≤2 BCLC stage D:Changes in treatment modalities for BCLC 0/A and B patients
No Yes
Decreased proportion
treated with elective surgery
Increased proportion treated
with oral HCC therapy
(usually treated with inpatient loco-
regional therapy)
41.4% reported an increase in the proportion of patients with BCLC B stage being treated with
oral systemic therapy.
(oral systemic therapy is not first line therapy in BCLC B)
Restricted, Non-Sensitive
45Increase in HCC treatment complications
No Yes
On average, 13.8% of the institutions reported an increase in HCC treatment
complications owing to COVID-19 across all stages.
Restricted, Non-Sensitive
46No growth in HCC clinical trials enrollments
Decreased enrollment Increased enrollment
86.3% of the institutions reported a decrease in patient enrollment into HCC clinical studies
owing to COVID-19 for patients of BCLC 0/A and B and 31% reported a similar decrease in
enrollment for patients of BCLC C.
Restricted, Non-Sensitive
47Conversion to teleconsulting
On average, Reduction of face-to-
face consultation by 27%
Due to restrictions such as
Highest adoption of social distancing, home
teleconsulting in the confinement and complete
Philippines, Australia and
Myanmar
lockdowns (in some
countries)
Restricted, Non-Sensitive
48Correlations with findings outside of the Asia-Pacific
Muñoz-Martínez et al. (2021, Dinmohamed et al. (2020, IJzerman M. and Emery J. (2020)
JHEP Rep.) Lancet Oncol.) https://pursuit.unimelb.edu.au/article
A Multi-national study
27% s/is-a-delayed-cancer-diagnosis-a-
consequence-of-covid-19
87% Decrease in cancer incidence
in the Netherlands Cancer 75%
Modified clinical practices Registry Decrease in referrals for
81% Kaufman et al. (2020, JAMA
suspected cancers in the
United Kingdom
Deferred screening programs Netw. Open)
50% 46%
Decrease in weekly cancer
Cancelled curative and/or diagnosis in the United States
palliative treatments
Restricted, Non-Sensitive
49Comparison for HCC between Europe and Asia-Pacific
Multi-national study (76 centers)
Muñoz-Martínez et al. (2021, JHEP Rep.) ASIA-PACIFIC (27 centers)
Europe (73.7%), South America (17.1%), North America (5.3%), Ghandi et al (2021, in press)
Asia (2.6%), Africa (1.3%) Our COVID-19 survey
Modified 31% (BCLC 0/A and B)
87%
Changes in
clinical treatment
practices modalities 17.2% (BCLC C)
Delay in
81%
Deferred
screening
programs
diagnosis of
new HCC cases
48.3%
Treatment with elective surgery 46.6% (BCLC 0/A and B)
50%
Cancelled
41.4% (BCLC C)
curative and/or Treatment with oral therapy
palliative
62.1%
treatments
Delay in initiation of HCC treatment
Restricted, Non-Sensitive
50Limitations
• Potential for systemic differences in patient profiles to be
overlooked due to the aggregated nature of data collection
• Small number of specialist clinics/institutions may under-represent
country or regional demographics
• Survey provided mainly qualitative data and there was no
granular data on individual patients
Restricted, Non-Sensitive
51Multiple Waves of COVID-19:
Lessons Learnt from the First Wave
Restricted, Non-Sensitive
52“History tells that this will not be the last pandemic, and
epidemics are a fact of life.”
Dr Tedros Adhanom Ghebreyesus (WHO Director-General)
First International Day of Epidemic Preparedness, Dec 2020
Restricted, Non-Sensitive
53Lessons Learnt from the 1st Wave
• Impact of indiscriminate postponement of clinical services
can lead to drastically poorer outcomes, especially for cancer
care
oThe current backlog of screening services will impact healthcare systems
considerably (Tan KK and Lau J, 2020, Eur. J. Surg. Oncol.)
oCosts of managing HCC increases exponentially with later stages at
diagnosis, with decreasing treatment efficacy.
oRisk-benefit ratios should be constantly explored to ensure there is a
balance between considerations of currently available HCC management
and the level of exposure to COVID-19
Restricted, Non-Sensitive
54Lessons Learnt from the 1st Wave (the SGH Surgery experience)
• Calibrated reduction and not total de-prioritization of elective
procedures is an achievable goal
o Policy of not postponing cancer surgery. Consultant grade surgeons decides on
postponement of non-cancer surgery based on ASA scores and co-morbidities
o In SGH, the calibrated postponement enabled 6,640 doctor man-hours to be
reallocated to support COVID-19 containment efforts without significant increase in
emergency surgeries. (Chow et al., under review)
Volume of cancer
Decrease in the surgeries largely
monthly volume remained unchanged
of surgeries
Restricted, Non-Sensitive
55Lessons on the management of HCC from the
1st Wave of COVD-19 (1)
• The COVID-19 HCC survey provides data that can guide
healthcare systems on the continual reassessments of the impact
of policies on the diagnosis and treatment of HCC
• COVID-19 is not going to be over soon – there will continue to
be further waves.
• drastic short term measures that succeeded in SARS are not tenable
in COVID-19
• There should be consideration of a calibrated response to
postponing cancer care rather than the total cancellations seen
in some places.
Restricted, Non-Sensitive
56Lessons on the management of HCC from the
1st Wave of COVD-19 (2)
• Results of the survey should increase awareness of poor clinical
outcomes in HCC with restrictive measures:
• delayed diagnosis
• delayed initiation of treatment
• changing more efficacious in-patients therapies for less
efficacious oral therapies
• There should be increased use of digital communication for
consultations
• possible even in 3rd world countries e.g. Myanmar, Philippines
Restricted, Non-Sensitive
57Differences between two pandemics
Development of
SARS COVID-19 COVID-19 vaccines
As of 23 Aug 2021,
Nov 2002 – Jul 2003 (declared Dec 2019 – Total Doses Administered
8,605,217
worldwide containment)
8098 cases, 774 deaths 197 million cases, 4.2 million deaths
Completed Full Vaccination
Cases largely from the healthcare Cases largely from the community Regime
institutions and affected HCWs
Genomic sequence was publicly 4,251,555
shared within a month
Restricted, Non-Sensitive
58Differences between two pandemics
SARS COVID-19 Development of PCR,
rapid-antigen tests
Nov 2002 – Jul 2003 (declared Dec 2019 – As of 23 Aug 2021,
worldwide containment) Total Swabs Tested
8098 cases, 774 deaths
Cases largely found in the healthcare
197 million cases, 4.2 million deaths
Cases largely found in the
17,338,504
setting community setting
Genomic sequence was publicly
shared within a month
Restricted, Non-Sensitive
59Summary
• The COVID-19 pandemic has resulted in multiple waves of infection
and the pandemic will not be over soon
• The strict public health measures that were so effective in controlling
SARS within a short period of a few months will not be tenable in
COVID-19.
• The first wave of the COVID-19 pandemic brought many lessons
useful for the management of subsequent waves:
• a calibrated response to cancer care will be more useful
• there will be a backlog of cases with late diagnosis
• the substitution of standard-of-care therapies for less efficacious outpatient
therapies will lead to poorer clinical outcomes
• there should be increased use of digital communication for consultations
Restricted, Non-Sensitive
60Thank You! Acknowledgement: 1. The study was funded by Duke-NUS, the “Estate of Tan Sri Khoo Teck Puat”, SingHealth Duke-NUS Global Health Institute Research Grant, Duke-NUS Medical School (Duke-NUS/SDGHI_RGA(Khoo)/2020/0005) and NCCS Cancer Fund. 2. Sim Yu Ki B.Eng (Hons) for creation of slides
You can also read

















































