The Expansion of Medical Assistance in Dying in the COVID-19 Pandemic Era and Beyond: Implications for Vulnerable Canadians
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Scholarly Reviews and Commentary
The Expansion of Medical Assistance in Dying in the
COVID-19 Pandemic Era and Beyond: Implications
for Vulnerable Canadians
Sera Whitelaw1, Trudo Lemmens2,3, Harriette G.C. Van Spall4,5,6,7
1
Faculty of Medicine and Health Sciences, McGill University, Montreal, Quebec, Canada; 2Faculty of Law, University of
Toronto, Toronto, Ontario, Canada; 3Dalla Lana School of Public Health, University of Toronto, Toronto, Ontario, Canada;
4
Department of Health Research Methods, Evidence, and Impact, McMaster University, Hamilton, Ontario, Canada;
5
Department of Medicine, McMaster University, Hamilton, Ontario, Canada; 6Population Health Research Institute,
Hamilton, Ontario, Canada; 7Research Institute of St. Joseph’s, Hamilton, Ontario, Canada
Corresponding Author: Dr. Harriette Gillian Christine Van Spall: Harriette.VanSpall@phri.ca
Submitted: 22 October 2021; Accepted: 5 January 2022; Published: 30 May 2022
DOI: https://doi.org/10.22374/cjgim.v17i2.586
Abstract
In 2015, the Canadian parliament passed a law permitting adults to request Medical Assistance in Dying
(MAiD) when they have a grievous, irremediable medical condition that causes unbearable suffering and
their natural death is reasonably foreseeable. Following a constitutional challenge, a Quebec lower court, ruled
in the Truchon vs. Canada AG case that the restriction to a reasonably foreseeable death is an unjustifiable
impingement on the right to life, liberty, and security of the person and the right to equality. In response, the
government expanded the MAiD law in March 2021 through Bill C-7 to include those who are not approach-
ing their natural death. Bill C-7 is a potentially harmful approach to justice for vulnerable groups such as the
elderly, disabled, or those with chronic illnesses. The COVID-19 pandemic has highlighted serious problems
with how we care for the vulnerable members of our society. In this article, we explore what has gone wrong
and what has raised serious concerns, while proposing potential options to consider when developing new
laws, systems, and processes to improve societal equity.
Résumé
En 2015, le gouvernement fédéral a adopté une nouvelle loi permettant aux adultes de demander l’aide médi-
cale à mourir (AMM) dans certaines circonstances, notamment les problèmes de santé graves et irrémédia-
bles qui provoquent des souffrances insupportables et dont la mort naturelle est raisonnablement prévisible.
À la suite d’une contestation constitutionnelle, un tribunal de première instance de la province de Québec a
statué, dans l’affaire Truchon c. Procureur général du Canada, que la restriction à une mort raisonnablement
prévisible constitue une atteinte injustifiable au droit à la vie, à la liberté et à la sécurité de la personne. En
réponse à ce verdict, le gouvernement a modifié la loi sur l’AMM en mars 2021 par l’intermédiaire du projet
de loi C-7 pour y inclure les personnes chez qui la mort n’est pas dans un avenir prévisible. Le projet de loi C-7
Canadian Journal of General Internal Medicine Vo l u m e 1 7 , I s s u e 2 , 2 0 2 2 17The expansion of MAiD in the COVID-19 pandemic era
est une approche de la justice potentiellement préjudiciable aux groupes vulnérables, comme les personnes
âgées, handicapées ou atteintes de maladies chroniques. La pandémie de COVID-19 a mis en lumière de
graves problèmes concernant la façon dont on prend soin des membres vulnérables de notre société. Dans
cet article, nous explorons ce qui a mal fonctionné et ce qui a suscité de vives inquiétudes, tout en proposant
des options possibles à envisager lors de l’élaboration de nouvelles lois, de nouveaux systèmes et de nouveaux
processus pour améliorer l’équité sociale.
Keywords: Medical Assistance in Dying, Equity, Equality, COVID-19
Following the landmark Carter vs. Canada case in 2015,
Canadian parliament passed a law permitting capable adults
to request Medical Assistance in Dying (MAiD) when they
have a grievous, irremediable medical condition that causes
unbearable suffering and an irreversible decline of capabil-
ities, with a reasonably foreseeable natural death.1 While
MAiD was originally intended as an exceptional procedure
in situations of intolerable suffering in a broad end-of-life
context, recent trends indicate that the use of MAiD has
steadily increased each year across all Canadian jurisdictions
since the law was passed in 2016 (Figure 1).2 There is evi-
dence that Bill C-7 and future MAiD expansion measures
could increase the vulnerability of people who may benefit Figure 1. Total reported MAiD deaths in Canada by juris-
instead from better access to treatment and palliative care, diction between 2016 and 2019.
better supports while living with chronic disease, and better NL, Newfoundland; PE, Prince Edward Island; NS, Nova
living conditions at home and in long term and chronic care Scotia; NB, New Brunswick; QC, Quebec; ON, Ontario;
institutions. MB, Manitoba; SK, Saskatchewan; AB, Alberta; BC, British
Patients usually seek MAiD in Canada because they Columbia; YT, Yukon Territories; NT, Northwest Territo-
experience debilitating symptoms that diminish their quality ries; NU, Nunavut.
of life,2,3 perceived burden on family members and informal *Data from the Government of Canada.2
caregivers,4–6 and loss of dignity.2,7 The Health Canada first
annual report on MAiD has confirmed reasons that have demand for MAiD. Based on the Health Canada first annual
prompted individuals to choose MAiD (Table 1).2 Among report on MAiD, 10.2% of people who received MAiD did
the 5389 individuals who received MAiD in 2019, the most not have access to disability supports,2 and conflicting
commonly cited reasons for intolerable suffering that caused reports on the availability of these supports exist.2,8,9 The
them to opt for MAiD were inadequate pain control or fear Health Canada first annual report on MAiD stated that
of this in the future (53.9%), the perceived burden on fam- 82.1% of 5389 patients receiving MAiD received palliative
ily or caregivers (53.3%), loss of dignity (34.0%), and isola- care, but as many as 16% received palliative care for the first
tion or loneliness (13.7%).2 Similarly, a retrospective chart time less than 2 weeks before they chose to die.2 A total of
survey of 250 patients, of which 23.7% had an end-organ 18% failed to receive any palliative care prior to receiving
failure due to heart failure and/or lung disease, conducted MAiD.2,10 There may be regional variation in these estimates;
in British Columbia found that illness-related suffering for example, a chart review at the Ottawa Hospital found that
(59.8%), loss of control (52.7%), and fear of future suffering as many as 39.3% of those who requested MAiD had no pal-
(24.1%) were the most common reasons causing individuals liative care involvement.11 This emphasizes concerns over the
to opt for MAiD.7 timeliness and quality of these services, while also raising the
The limited availability of disability supports and access question of whether better access to palliative care may have
to palliative care services may play a significant role in the mitigated the demand for MAiD.
18 Vo l u m e 1 7 , I s s u e 2 , 2 0 2 2 Canadian Journal of General Internal MedicineWhitelaw S et al.
Table 1. Reported nature of suffering among people who more likely to opt for MAiD. Members of the Canadian
received MAiD in 2019
Association of MAiD Assessors and Providers have reported
No. (%) of 5389
people receiving
that since the onset of the pandemic, more individuals have
Reported nature of suffering MAiD+ inquired about MAiD and that COVID-19 restrictions have
Loss of ability to engage in meaningful 4375 (82.1) accelerated the timelines of individuals’ medically assisted
activities deaths.14 Residents in LTC facilities, which have made up a
Loss of ability to perform activities of 4209 (78.1) majority of all reported COVID-19 deaths in Canada, are
daily living particularly vulnerable.15 LTC homes lacked the basic test-
Inadequate control of symptoms other 3039 (56.4) ing capabilities, hygiene processes, and personal protective
than pain (or concern about it)
equipment needed for infection prevention and mitigation,
Inadequate control of pain (or concern 2905 (53.9)
about it)
even after they were identified as COVID-19 hot spots.16
Before the pandemic, a meta-analysis of 16 cross-sectional
Loss of dignity 2872 (53.3)
studies found that residents of LTC institutions had worse
Perceived burden on family, friends, or 1832 (34.0)
caregivers quality of life than community-dwelling individuals.17 The
Loss of control of bodily functions 1719 (31.9) impact of LTC institutionalization on the quality of life of
Isolation or loneliness 738 (13.7)
individuals has likely only worsened with the isolation and
illness of the pandemic.18 For example, in October 2020, a
Emotional distress/anxiety/fear/ 253 (4.7)
existential suffering 90-year-old woman, who was described as being excep-
Loss of control/autonomy/independence 220 (4.1) tionally social and energetic, elected to receive MAiD as
No/poor/loss of quality of life 199 (3.7) she did not want to suffer through another lockdown in her
Other 32 (0.6)
LTC home.14 These trends during the COVID-19 pandemic
+
More than one could be selected, therefore the total exceeds 100%. should be seen by legislative bodies as an urgent call toward
*Data from the Government of Canada.2 action for improving the quality of care in LTC, reducing the
need for lockdowns, enhancing the quality of life amongst
Existential suffering associated with living environments vulnerable individuals, and providing community support so
and poor health care experiences may also result in individu- individuals can live at home longer.
als opting for MAiD.12–14 An example was a 42-year-old man Expanding access to MAiD outside the end-of-life con-
with VACTERL syndrome, a non-random association of text may increase the proportion of vulnerable Canadians,
birth defects that affects multiple anatomical structures, who, such as those with disabilities, who receive MAiD.. Following
despite having the option to receive physician-recommended a constitutional challenge, a Quebec lower court ruled in the
medical interventions that could keep him alive, declined Truchon vs. Canada AG case that the restriction to reason-
treatment and requested MAiD in 2020 largely due to pre- ably foreseeable death is an unjustifiable infringement on
vious negative healthcare experiences.12 Another recent the right to life, liberty, and security of the person and the
example was a 35-year-old man suffering from Fabry disease right to equality.19,20 Parliament, responded in March 2021
who chose MAiD in January 2021.13 His decision to receive with a new MAiD law that removed the legal safeguard that
MAiD appeared to be associated with the deplorable con- restricted MAiD to those who have a reasonably foreseeable
ditions in the long-term care (LTC) home he resided in.13 death, and introduced a second track access system for per-
These squalid conditions have since caused the Retirement sons who are not approaching their natural death, de facto
Homes Regulatory Authority to revoke the operating licence for persons who have a disability.21–23
of this LTC home along with five others.13 These cases raise An analysis of 1027 Canadians with disabilities found
concerns about the prioritization and provision of MAiD that increased anxiety, stress, and despair were associated
in circumstances without first addressing the failure of care with negative financial effects of COVID-19, increased
standards. Situations such as these also highlight the need for loneliness, and decreased feelings of belonging.24 There is
future research directed towards understanding the gaps in concern that the increased strain on support services and
care amongst people who opt for MAiD. the disproportionate impact on vulnerable populations
The SARS-CoV-2 2019 (COVID-19) pandemic has as a result of COVID-19 may result in even more people
highlighted serious disparities in how we care for vulnera- with disabilities with non-foreseeable deaths opting for
ble members of our society – and such members may be MAiD.
Canadian Journal of General Internal Medicine Vo l u m e 1 7 , I s s u e 2 , 2 0 2 2 19The expansion of MAiD in the COVID-19 pandemic era
people opted for MAiD, and how these underlying reasons
should be addressed with better health care, social supports,
disability services, and other measures that promote dignity
in life, so that individuals do not seek to access a government-
funded and health system-provided assisted death. It is
important that we learn from our experiences in the COVID-
19 pandemic context, while also adjusting our laws, systems,
and processes to improve social justice and protect those who
are in situations of heightened vulnerability.
Author Contributions
HGCV conceived the work, reviewed the literature, and
wrote and edited the manuscript. SW reviewed the litera-
ture and wrote and edited the manuscript. TL reviewed the
literature and wrote and edited the manuscript. All authors
approved the manuscript for submission.
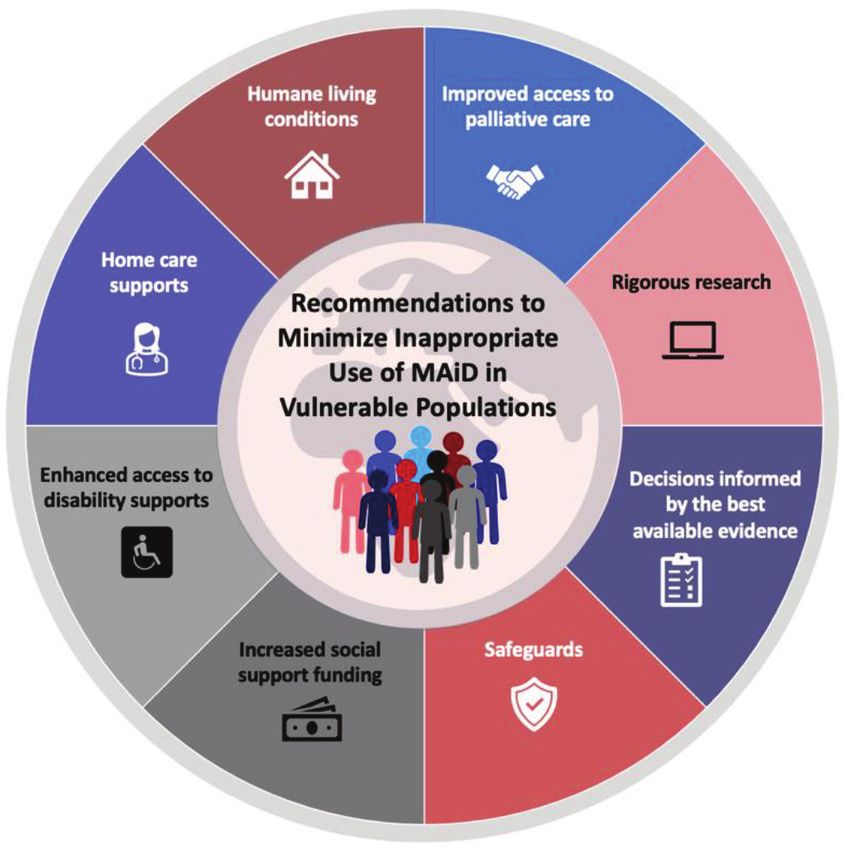
Figure 2. Central Illustration. Recommendations to mini- Conflicts of Interest
mize inappropriate use of MAiD in vulnerable populations.
The authors declare no competing interests.
In light of the legal expansion of MAiD eligibility, the
legislative branches of government and health systems need Funding
to understand and support vulnerable populations (Figure 2,
Central Illustration). We have to conduct research to bet- HGCV received research funding from the Canadian
ter understand gaps in care, support, and services. We must Institutes of Health Research and the Heart and Stroke
realize that Canada has significantly underfunded social sup- Foundation of Canada.
port spending compared to other economically similar coun-
tries, which was recently shown in the 2020 Organization for
Economic Cooperation and Development Social Spending References
update,25 and acknowledge this impact on health outcomes.
Additionally, all decisions pertaining to MAiD should be made 1. CanLII. Carter v. Canada (Attorney General), 2015 SCC 5,
in consultation with the best available evidence, while ensur- [2015] 1 S.C.R 331 [cited 2021 Apr 21]. Available from: https://
www.canlii.org/en/ca/scc/doc/2015/2015scc5/2015scc5.html
ing that proper safeguards are in place to protect our vulner-
2. Government of Canada. First annual report on medical assis-
able populations. Lack of rigorous research, inadequate social tance in dying in Canada 2019. [cited 2021 Apr 21]. Available
support funding, poor living conditions, and inadequate access from: https://www.canada.ca/content/dam/hc-sc/documents/
to care and support will continue to put individuals at risk. services/medical-assistance-dying-annual-report-2019/maid-
Consequently, if we fail to act promptly, we may find more peo- annual-report-eng.pdf
ple, particularly society’s most vulnerable, opting for MAiD. 3. Nuhn A, Homes S, Kelly M, Just A, Shaw J, Wiebe E. Experiences
The COVID-19 pandemic has exemplified how dispar- and perspectives of people who pursued medical assistance in
ities and despair could be alleviated with adequate support dying: Qualitative study in Vancouver, BC. Can Fam Physician.
2018;64:e380–6. PMC6135118.
and services. As the MAiD practice continues to grow, we
4. Li M, Shapiro GK, Klein R, Barbeau A, Rydall A, Bell JAH, et al.
need to insist that our legislative branches of government and Medical assistance in dying in patients with advanced cancer
health systems critically evaluate opportunities for improved and their caregivers: A mixed methods longitudinal study pro-
services rather than further expanding MAiD. This should tocol. BMC Palliat Care. 2021;20:117. http://dx.doi.org/10.1186/
include a detailed assessment of the underlying reasons why s12904-021-00793-4
20 Vo l u m e 1 7 , I s s u e 2 , 2 0 2 2 Canadian Journal of General Internal MedicineWhitelaw S et al.
5. Thangarasa T, Hales S, Tong E, An E, Selby D, Isenberg- 16. Holroyd-Leduc JM, Laupacis A. Continuing care and COVID-
Grzeda E, et al. A race to the end: Family caregivers’ experience 19: A Canadian tragedy that must not be allowed to happen
of medical assistance in dying (MAiD) – A qualitative study. again. CMAJ. 2020;192:E632–3. http://dx.doi.org/10.1503/cmaj.
J Gen Intern Med. 2022;37:809–815. http://dx.doi.org/10.1007/ 201017
s11606-021-07012-z 17. De Medeiros MMD, Carletti TM, Magno MB, Maia LC,
6. Frolic AN, Swinton M, Murray L, Oliphant A. Double-edged Cavalcanti YW, Rodrigues-Garcia RCM. Does the institution-
MAiD death family legacy: A qualitative descriptive study. alization influence elderly’s quality of life? A systematic review
BMJ Support Palliat Care. 2020. http://dx.doi.org/10.1136/ and meta-analysis. BMC Geriatr. 2020;20:44. http://dx.doi.
bmjspcare-2020-002648 org/10.1186/s12877-020-1452-0
7. Wiebe E, Shaw J, Green S, Trouton K, Kelly M. Reasons for 18. Altarum Institute. Experiences of nursing home residents
requesting medical assistance in dying. Can Fam Physician. during the pandemic. [cited 2021 Apr 21]. Available from:
2018;64:674–9. PMID: 30209101. https://altarum.org/sites/default/files/uploaded-publica-
8. Freeman S, Smith TF, Neufeld E, Fisher K, Ebihara S. The tion-files/Nursing-Home-Resident-Survey_Altarum-Special-
wish to die among home care clients in Ontario, Canada: A Report_FINAL.pdf
cross-sectional study. BMC Palliat Care. 2016;15:24. http://dx. 19. CanLII. Truchon c. Procureur general du Canada, 2019 QCCS
doi.org/10.1186/s12904-016-0093-8 3792. [cited 2021 Apr 21]. Available from: https://www.canlii.
9. Pesut B, Thorne S, Wright DK, Schiller C, Huggins M, org/en/qc/qccs/doc/2019/2019qccs3792/2019qccs3792.html
Puurveen G, et al. Navigating medical assistance in dying from 20. Lemmens T, Jacobs L. The latest medical assistance in dying
Bill C-14, to Bill C-7: A qualitative study. BMC Health Serv Res. decision needs to be appealed: Here’s why. The Conversation;
2021;21:1195. http://dx.doi.org/10.1186/s12913-021-07222-5 9 October 2019. [cited 2022 Jan 26]. Available from: https://
10. Gallagher R. Lack of palliative care is a failure in too many MAiD theconversation.com/the-latest-medical-assistance-in-dying-
requests. [cited 2021 Oct 07]. Available from: https://policy- decision-needs-to-be-appealed-heres-why-124955
options.irpp.org/magazines/october-2020/lack-of-palliative- 21. Parliament of Canada. An act to amend the criminal code
care-is-a-failure-in-too-many-maid-requests/ (medical assistance in dying). [cited 2021 Apr 21]. Available
11. Munro C, Romanova A, Webber C, Kekewich M, Richard R, from: https://parl.ca/DocumentViewer/en/43-2/bill/C-7/royal-
Tanuseputro P. Involvement of palliative care in patients assent
requesting medical assistance in dying. Can Fam Physician. 22. Lemmens T, Shariff M, Herx L. How Bill C-7 will sacrifice
2020;66:833–42. PMID: 33208428. the medical profession’s Standard of Care Policy Options (11
12. Yuan S, Oechslin EN, Li M, Osten M, Roche L. Medical assis- February 2021). [cited 2022 Jan 26]. Available from: https://
tance in dying (MAID) in adult congenital heart disease policyoptions.irpp.org/magazines/february-2021/how-bill-c7-
(ACHD). J Am Coll Cardiol. 2020;75:3444. http://dx.doi.org/ will-sacrifice-the-medical-professions-standard-of-care/
10.1016/S0735-1097(20)34071-7 23. Quinn G, Mahler G, Deschutter O. Mandates of the spe-
13. Global News. Hamilton man dies amid ‘disturbing’ living con- cial rapporteur on the rights of persons with disabilities; the
ditions at Niagara Falls home, says family. [cited 2021 Apr 21]. independent expert on the enjoyment of all human rights by
Available from: https://globalnews.ca/news/7608179/ham- older persons; and the special rapporteur on extreme pov-
ilton-man-dies-disturbing-living-conditions-niagara-falls- erty and human rights. [cited 2022 Jan 26]. Available from:
home/ https://spcommreports.ohchr.org/TMResultsBase/DownLoad
14. CTV News. Facing another retirement home lockdown, PublicCommunicationFile?gId=26002
90-year-old chooses medically assisted death. [cited 2021 Apr 24. Pettinicchio D, Maroto M, Chai L, Lukk M. Findings from
21]. Available from: https://www.ctvnews.ca/health/facing-an- an online survey on the mental health effects of COVID-19
other-retirement-home-lockdown-90-year-old-chooses-medi- on Canadians with disabilities and chronic health conditions.
cally-assisted-death-1.5197140 Disabil Health J. 2021:14;101085. http://dx.doi.org/10.31235/
15. Canadian Institute for Health Information. Pandemic experi- osf.io/9d5j4
ence in the long-term care sector: How does Canada compare 25. Organization for Economic Cooperation and Development.
with other countries? [cited 2021 Apr 21]. Available from: Social spending makes up 20% of OECD GDP. [cited 2021 Dec
https://www.cihi.ca/sites/default/files/document/covid-19-rap- 22]. Available from: https://www.oecd.org/els/soc/OECD2020-
id-response-long-term-care-snapshot-en.pdf Social-Expenditure-SOCX-Update.pdf
Canadian Journal of General Internal Medicine Vo l u m e 1 7 , I s s u e 2 , 2 0 2 2 21You can also read