The Consequences of a Public Health Insurance Option: Evidence From Medicare Part D Prescription Drug Markets
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The Consequences of a Public Health Insurance Option:
Evidence From Medicare Part D Prescription Drug
Markets
Daniel P. Miller
Clemson University
Jungwon Yeo
Singapore Management University∗
November 2011
Abstract
Policy makers in the US have debated the merits of including a government spon-
sored public health insurance option as a part of health care reform. Under the pro-
posed legislation, the government would offer a basic coverage plan with premiums
set at cost that competes against plans offered by private insurers. The government’s
ability to negotiate favorable prices with health care providers and lack of profit taking
could increase competition and perhaps crowd out a significant amount of private com-
petition. We consider the existing Medicare Part D prescription drug market which
resembles the new health insurance exchanges that will be coming online in 2014. We
use data from the 2006-2009 Part D market to estimate a random coefficient discrete
choice demand system and a supply side model for Part D plans. Using our estimates,
we conduct policy counterfactuals that include a public option as proposed by leg-
islators in the 2009 “Medicare Prescription Drug Coverage Improvement Act.” Our
results indicate a small increase in competition if the government plan operates with
a cost structure similar to private plans. But, if the government has up to a 25% cost
advantage over private plans, perhaps achieved through a strong bargaining position
with drug manufacturers, the government plan dominates the market and crowds out
a significant fraction (25%) of private plans’ market share. There are consumer surplus
gains; they increase in the size of the public option’s cost advantage. But, no matter
the cost advantage, all total surplus gains are eliminated after factoring in the decline
in insurer profits and the implicit subsidies in the Part D program.
∗
We thank Leemore Dafny, Amanda Kowalski, Greg Lewis, Claudio Lucarelli, Tom Mroz, Robert Town
and seminar participants at Clemson, University of Georgia, and University of South Carolina for helpful
comments. First Draft February 2011. Author correspondence: dmille7@clemson.edu and jwyeo@smu.edu.sg
11 Introduction
In 2010 US legislators passed a major health insurance reform bill. A controversial provision
that was ultimately struck from the bill is the “Community Health Insurance Option”1 , col-
loquially known as a “Public Option.”2 When fully enacted in 2014, the reformed health care
system will continue to rely on private health insurance markets, but under the “Commu-
nity Option” the government would have offered a zero-profit basic coverage health insurance
plan that sells alongside private plans. The legislation stipulates that the government plan
compete on a level playing field with private plans. It will not be subsidized, is subject to
the same regulations as private plans, has no special mandates on coverage, and negotiates
provider fees without statutory mandate.
There are pros and cons of a public option. Supporters advocate the benefits of more
choice and increased competition. They also hope the government will further drive down
cost by leveraging a strong negotiating position over fees with providers (physicians, hospi-
tals, drug manufacturers). Critics argue that the public option could significantly crowd out
private plan enrollment without any competitive benefits. Moreover, they are concerned that
greater negotiating power will distort providers’ supply-side incentives: for example, phar-
maceutical manufacturers incentives to develop new drugs (Lakdawalla and Sood, 2009).
Although the plan is explicitly budget neutral, there are concerns that the public option
could have an budgetary impact through other subsidies and tax-provisions tied to the re-
form. To another set of critics, who believe that government provision of services is less
cost-efficient than private provision, the government option would simply be a fringe plan
that has little impact on competition.
In this paper, we consider the existing Medicare Part D prescription drug insurance
market—which closely resembles the reformed insurance markets—to quantitatively evaluate
the competitive consequences of introducing a public option. As part of the 2003 “Medicare
Modernization Act” (MMA), Medicare introduced “Part D,” that for the first time would
cover prescription drugs. Unlike the original Medicare program, where the government is
the sole insurer, Part D is a regulated insurance exchange. Senior citizens enroll in plans
subsidized and regulated by the government, but sold by competing private insurers.
The Part D market has never had a public option; we cannot conduct a retrospective
1
House of Representatives Bill H.R. 3590 Section 1323, struck from bill Sec 10104.
2
The language in an earlier bill proposal (H.R. 3962) proposed by Nancy Pelosi, used the term “Public
Health Insurance Option,” which was was changed to “Community Health Insurance Option” in the passed
bill. The descriptions in the two bills are nearly verbatim identical. The key difference is that in the passed
legislation states may opt-out of the community option whereas in the earlier bill states could not opt-out.
2program evaluation. Instead, we estimate an equilibrium supply/demand model for insurance
plans and then conduct a policy counterfactual that recomputes the market equilibrium with
the inclusion of a public option. We assess many competitive outcomes such as the effect on
enrollment for the government plan and private plans, monthly premiums, consumer welfare,
industry profits, and subsidies linked to the Part D program.
Two stylized facts about Part D markets fuel the debate over a public option. On one
hand, individuals have lots of choices. The typical enrollee can choose from over 40 plans
offered by about 20 insurers. On the other hand, it is a concentrated industry. Between
2006 and 2009, the Herfindahl-Hirschman concentration index (HHI) for the average market
is 2376, in the range the Department of Justice labels “moderately concentrated,” just shy of
the “highly concentrated” threshold of 2500. At the national level, the two largest insurers
(United Healthcare, and Humana) together have a 50% market share. Taking these two facts
together, it’s not immediately obvious whether a public option would have a minor or major
impact on competition.
We model plans as differentiated products. Per regulation, private insurers must offer at
least one plan meeting a basic, minimum coverage standard, but they are also allowed to
offer enhanced plans with more generous coverage, the so-called “Cadillac” plans. Coverage
characteristics such as deductibles, drug copays, and drug formularies (the list of covered
drugs) differentiate plans. We use a flexible random coefficients discrete choice model of
plan demand. Our model captures heterogeneity in consumer’s preferences for plans, driven
by factors such as enrollees’ health status and idiosyncratic differences in enrollees’ drug
regimens.
We model the supply of plans as a Bertrand multiproduct firm oligopoly model. We pay
particular attention to the rules regarding premium subsidies. They distort the residual de-
mand elasticities faced by insurers and hence effect insurer markups. Moreover, the subsidies
are the channel by which the public option impacts the government budget.
Using data from 2006 to 2009 on aggregate plan enrollment, pricing, and plan character-
istics, we estimate the model using the method in Berry (1994) and Berry, Levinsohn, and
Pakes (1995) (BLP). To evaluate the consequences of introducing a public option, we recom-
pute the model equilibrium under the counterfactual market structure that includes a public
option. As in Petrin (2002), BLP models are tailored for counterfactuals that introduce new
products.
A public option for the Part D market has been under consideration long before the 2010
health insurance reform debates. Every session of congress since the MMA legislation passed
3in 2003 proposed a public option. The proposals detail exactly how the public option would
be introduced.3 The government would only offer a basic plan—no enhanced plans. The plan
competes on a level playing field as if it were just another private plan. Like private plans,
the public option would construct a drug formulary, set copay and coinsurance rates, and
negotiate discounts with drug manufacturers. The negotiating rules are fully flexible; there
are no statutory pricing directives set in law such as reference pricing and the government
(and manufacturers for that matter) may exclude drugs from the formulary.4 Unlike private
plans, it foregoes profits by setting monthly premiums at cost. Thus, the public option is
explicitly budget neutral. But, its introduction will have an indirect effect on the government
budget through the existing Part D subsidy rules.
We construct the public option’s plan characteristics to match the basic benefit structure,
and, as our baseline, assume that it sells at the marginal cost equal to that of the average
private plan. We explore the possibility that the government could offer a more or less
desirable plan by varying the plan’s cost. For instance, the government plan could have
a low cost if it has the ability to negotiate deep discounts with drug manufacturers. We
consider a case where the government plan has a 25% cost advantage, comparable to the
drug discounts negotiated by Canadian provinces and the Veterans Affairs program.5 We
also consider the case that the government has a cost disadvantage, representing either poor
drug price negotiations or inefficient management.
Our results show that if the government plan operates with a cost similar to the average
private plan it becomes an average plan. It ranks as a top 10 to 15 plan (out of about 40) with
a 1.4% market share. It gains most of its share by crowding out private plans’ share. There
is little effect on premiums; private plans lower them by just a couple cents. Nationwide
consumer surplus increases by about $78 million, which is offset by a decrease in industry
profits of $53 million. The competitive effects are more pronounced if the government has
a 25% cost advantage. The government plan is number 1 with a 8.6% market share. Basic
plans–the closest in product space to the government plan—respond with slightly lower
premiums, yet lose 15% of their enrollees. Enhanced plans are affected modestly, losing
3
The 2009 “Medicare Prescription Drug Coverage Improvement Act.” is the most explicit.
4
The proposed Pelosi bill (H.R. 3962) included reference pricing clauses, but the passed law H.R. 3590
does not.
5
Danzon and Furukawa (2008) constructs a price index comparing Canadian and American brand name
drugs and finds 20% to 40% lower prices in Canada. The advocacy group, Families USA, compared Part
D drug prices to the Veterans Affairs (VA) negotiated Federal Supply Schedule (FFS) prices for the top 20
drugs in 2007. They found the VA negotiates a median 58% lower price than the lowest price that a Part D
plan negotiated. source: www.familiesusa.org/assets/pdfs/rhetoric-vs-reality.PDF (accessed 8/12/10).
4about 4% of their enrollees. The different response by basic and enhanced plans is due to the
estimated higher cross price elasticity amongst basic plans, than between basic and enhanced
plans. Nationwide consumer surplus increases $565 million while industry profits fall $311
million. If the government has a 10% cost disadvantage, there is negligible competitive effect.
Despite the government forgoing profits, this result follows because the market is already
highly competitive and has low markups: estimated markups average just 7% to 9% over
cost. If we factor in the subsidies in the Part D program, all total surplus gains are wiped
out (regardless of the government plan’s cost advantage) because more enrollees are brought
in to the highly subsidized Part D program from other options with lower subsidies.
The remainder of the paper is organized as follows. In section 2 we relate our work
to the existing literature. Section 3 provides background and institutional details of the
Medicare part D market. Section 4 introduces the demand and supply model. Section 5
describes the data. Section 6 reports our supply and demand estimates. Section 7 conducts
the counterfactual exercise. Section 8 concludes.
2 Contribution to Existing Literature
There is an emerging literature about the Medicare Part D prescription drug program. Much
of this literature focuses on the behavioral economics of senior citizens choosing plans. In
particular, the literature examines whether senior citizens rationally choose plans. Abaluck
and Gruber (2009) use micro level consumer data on plan choices and drug expenditures
and find that senior citizens don’t necessarily pick the plan that would minimize total out
of pocket expenditures on premiums, deductibles, and copays. Enrollees tend to overvalue
plan characteristics such as the monthly premium and deductible, when in fact there exists
a plan with a higher deductible or premium that results in lower expected out of pocket
expenditures, even after factoring risk consideration. In a series of work Heiss, McFadden,
and Winter (2006, 2010), document cases of sub-optimal plan choice with regards to plan
coverage and a penalty for late enrollment. They find people delay enrollment who, looking
towards future years, would otherwise be better off enrolling despite a short term loss.
Lucarelli, Prince, and Simon (2008) estimate a similar model to ours and run a counterfactual
experiment that limits the number of plans insurers may offer. These papers suggest limiting
plan choice could be welfare improving if enrollees are not fully rational or face high search
costs.
Our study differs in several dimensions. First, we consider an equilibrium model of the
5market. Our focus is not only on consumer demand, but also the supply side of the market.
We are able to analyze both sides of the market because we have enrollment data on the
entire market, not just a selected sample of consumers. We also have the necessary data
on the subsidy rules that allows us to correctly model and estimate the supply side. By
analyzing all sides of the market, we can conduct a comprehensive welfare evaluation of
consumers, insurers, and (as a subsidized market) the government’s budget. Second, we
construct plan characteristics using highly detailed data on drug coverage for the the entire
universe of prescription drugs for every plan. In short, we observe every financially relevant
plan characteristic that consumers observe. Although the micro data available to Abaluck
and Gruber (2009) allows them to estimate a richer demand system, we are nonetheless able
to estimate a very flexible random coefficient demand system. It is robust to the possibility
that enrollees overvalue certain characteristics thus ensuring we get unbiased estimates of
demand elasticities and the supply-side.
The US healthcare system has historically relied on the private provision of health insur-
ance. But, when the government becomes a supplier, crowding out of private competition
becomes a concern. Examples include Medicaid, (Cutler and Gruber, 1996), the Supplemen-
tal Children’s Health Insurance Program, (Lo Sasso and Buchmueller, 2004), and Medicaid’s
long-term care insurance (Brown and Finkelstein, 2008). These papers use both program
evaluation and calibration techniques to measure crowd out effects using data from after the
enactment of the government program. In contrast, our structural approach has predictive
power that allows us to make pre-enactment forecasts, and we can evaluate welfare effects,
not just market share outcomes.
This is also one of the first papers to address the competitive consequences of proposals
in the recent health care legislation. Others contributions include Dafny, Ho, and Varela
(2010) that quantifies the benefits of switching from an employer based health insurance
system (with a limited choice of plans) to an individual health insurance exchange (with
broader choice) and Avraham, Dafny, and Schanzenbach (2009) that evaluate the impact of
tort reform on insurance premiums.
Our work is also related to the IO health literature about competition in insurance mar-
kets. A recent example is the reduced form work in Dafny, Duggan, and Ramanarayanan
(2009) that examines the effect of mergers on health insurance premiums. They find consoli-
dation that results in much higher concentration only causes a modest increase in premiums.
There are other papers using that use a structural approach including Dranove, Gron, and
Mazzeo (2003); Ho (2009), who, respectively, estimate the competitive effects product differ-
6entiation in insurance markets and the role of bargaining between insurers and health care
providers.
Our model is static on both the supply and demand side which brings up two qualifica-
tions. On the supply side, we do not model plan’s entry and exit to determine if a government
option would cause plans to exit. We cannot identify this effect in a meaningful way because
there is no entry or exit by major firms in the data. Entry and exit only occurs on the
extreme competitive fringe, and we believe ignoring this churn will have negligible effect on
our results. Second, our model does not account for dynamic features of the demand for
health insurance plans. Carlin and Town (2009) document strong persistence in demand for
health insurance across time. Miller and Yeo (2011) estimate a dynamic demand system for
Part D plans with switching costs.
Finally, our work relates to the adverse selection literature, in particular Lustig (2010).
We do not have micro level data that would allow us to correct for adverse selection, but we
sign the potential bias in our estimates following the intuition in Lustig (2010).
3 Medicare Background
Medicare is the United State’s entitlement program that provides health insurance to all
people over age 65 and to some categories of disabled people. It started in 1965 and is
funded by a payroll tax. The original Medicare programs (Part A and Part B) cover hospital
and doctor services, but lack coverage for prescription drugs. Under Part A and Part B, there
is only 1 insurance plan that is provided by the government. The government negotiates fees
with hospitals and doctors according to rules mandated in legislation.
Medicare reforms have introduced a privatization of insurance. In 1997, Part C, currently
called Medicare Advantage (MA), created a health insurance exchange that gave Medicare
beneficiaries the option to purchase plans offered by competing private insurers. MA plans
set coverage levels and freely negotiate fees with providers. Medicare regulates coverage
standards and provides subsidies. Enrollment in a MA plan is voluntary and substitutes for
Part A and Part B coverage.
As part of the legislation in the 2003 Medicare Modernization Act (MMA), Medicare
introduced Part D to offer prescription drug coverage. Like Part C, Medicare beneficiaries
choose from a menu of plans sold on an insurance exchange by competing private insurers.
Part D plans set coverage levels and freely negotiate drug prices with manufacturers. Medi-
care regulates coverage by setting a minimum standard, and subsidizes monthly premiums.
7Insurers may offer enhanced coverage that exceeds the minimum standards, but the enhance-
ments are not subsidized. Roughly speaking, the subsidy is 2/3 of the average premium set
by the plans. In the model of the supply-side, we elaborate and formally model the subsidy
rules.
Medicare beneficiaries are penalized for not having drug coverage.6 They can obtain
coverage from a Part D plan sold in the exchange, a group policy offered by a current
employer or union, a group policy offered by a former employer or union as part of the
Retiree Drug Subsidy Program (RDS), or another government program such as Veterans
Affair insurance. The policies in the Part D market are sold as either stand-alone plans or
bundled with a MA plan (MA+Part D). We only endogenize the market for stand-alone
Part D plans, but we use enrollment data on MA+Part D plans and the RDS program to
account for the subsidy rules in our supply-side estimates and counterfactuals.
The duration of a Part D contract is one year, beginning January 1st. Once the contract
begins, enrollees are not allowed to switch plans. In November and December there is
an open enrollment period when enrollees are allowed to switch plans for the upcoming
year. Plans cannot adjust premiums or make major changes to coverage characteristics
throughout the year. Enrollees can only select plans offered in their geographic region which
are drawn around state boundaries. Plans must charge a uniform premium to all enrollees
in a region; they cannot engage in 3rd degree price discrimination based on health status or
prior experience.
Enrollees can access many channels to evaluate and select plans. Medicare publishes plan
information online through its “Plan Finder” tool and in print forms distributed through
the mail. Third parties, such as pharmacies and consumer advocacy groups offer assistance.
Insurers are allowed to market their plans through many types of media. Enrollees sign-up by
contacting Medicare or directly with the insurer. These are complicated financial contracts;
these channels are intended to make the plan selection process as transparent as possible.
Low income households are eligible for additional subsidies. All enrollees receive a pre-
mium subsidy, but Medicare pays all premiums and drug copays/coinsurance for households
below 100% of the poverty level. The low income subsidy gradually phases out up until
150% of the poverty level. Low income subsidy enrollees may choose any plan, but they
receive less than 100% premium and copay subsidies for enhanced plans and basic plans
with premiums above a market determined threshold. The lowest income households that
6
For every month a beneficiary lacks coverage, premiums increase by 1% for the rest of the person’s life.
For example, delaying enrollment by 2 years, results in a 24% premium penalty.
8do not actively sign-up are randomly assigned by Medicare to a plan that qualifies for the
full low income subsidy. A large fraction of the Medicare population, over 20%, receives a
low income subsidy.
3.1 Plan Characteristics
Plan’s are differentiated along several dimensions of coverage characteristics (deductibles,
coinsurance/copay rates, drug formularies) and other non-pecuniary characteristics. The
regulations set minimum standards for cost sharing rules. Under the minimum Part D
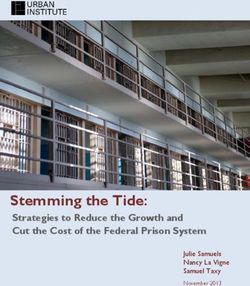
benefit structure enrollees’ out of pocket expenses follow a 5 part tariff. Table 5 and figure 1
depict the benefit structure and the names of the 5 regions of the tariff schedule. Enrollees
pay a premium regardless of their drug expenditures. For the first $250 of drug expenditures
(deductible) they pay 100% of their expenditures, and then between $250 and $2250 they are
in the initial coverage zone and pay 25% of their drug expenditures. Then, between $2250
and $5100 of expenditures they are in the donut hole and pay 100%. Beyond $5100, they are
in the catastrophic range and pay 5%. These are the 2006 thresholds; to keep pace with drug
price inflation and to keep the Part D program on budget, the thresholds have increased in
later years.
Plan’s classified as “basis” satisfy the minimum standard. They can use either coinsur-
ance rates that cover a percentage of drug expenditures or copay rates denominated in fixed
dollar amounts. For example, a plan may set a $30 copay for brand name drugs and $4 for
generic drugs. Across all drugs on the formulary, copay rates must be approved by Medicare
as being “Actuarially Equivalent” to a benefit structure using coinsurance rates. Plans with
more generous coverage are classified as “Enhanced.” They typically offer more generous
coverage by reducing the deductible and/or reducing out of pocket expenditures in the initial
coverage and donut hole regions. The portion of premiums attributable to enhancements
are not subsidized.
On a drug-by-drug basis, plans have a lot of scope selecting drugs for their formulary and
setting copay/coinsurance rates. The regulations require plans to cover at least two drugs
from the major therapeutic classes. Within a class they can pick and choose which drugs to
cover with a few exceptions for protected drugs, such as some cancer treatments, that must
be included on the formulary. Plans can cover “elective” medications, such as prescription
sleep medications, but that coverage is considered an enhancement and not subsidized. En-
rollees receive coverage for any on-formulary drug, but there may be restrictions in the form
9Figure 1: Part D Basic Benefit Structure
10of quantity limits, prior authorizations, and step therapies.7 Off-formulary drugs are not
covered; to purchase an off-formulary drug, an enrollee would have to pay full retail price
or go through an appeals process with the plan. Plans do not have to set 25% cost sharing
rates for every drug on the formulary. They set higher or lower copay/coinsurance rates by
placing drugs on tiers. For example, the tiers might be ranked as preferred, non-preferred,
specialty. Medicare must approve the tiers as being “actuarially equivalent.” Despite this
requirement, we observe a lot variation at the aggregate level, particulary amongst the most
popular drugs.
Drug prices are determined through a bargaining process between insurers, manufac-
turers, wholesalers, and pharmacies. Per regulation, plans are required to pass along all
discounts and rebates to enrollees. Medicare monitors every drug transaction to ensure com-
pliance. Negotiated prices matter for enrollees. Even if plans have identical cost sharing rules,
an enrollee would have a stronger preference for the plan with lower negotiated drug prices.
While the regulations ensure copay/coinsurance rates remain fixed, negotiated drugs prices
fluctuate throughout the year. As shown in Duggan and Scott-Morton (2010), restrictive
formularies, tiered copay/coinsurance rates, and bargaining were important considerations
in the design of the Medicare Part D market.
Plans contract with pharmacies to construct a pharmacy network. Contracts are not
exclusive; pharmacies can accept many plans, and plans can have several pharmacies. Plans
designate network pharmacies as either preferred, non-preferred, or mail-order. Drug prices
and copay/coinsurance tiers may differ across pharmacies, and are usually, but not always,
lower at preferred and mail-order pharmacies.
There are other important non-pecuniary plan characteristics. As in Starc (2010), mar-
keting and advertising activities influences consumer’s choices. As an example, the market
leader United Healthcare pays royalties to AARP to market and endorse their plans. Hu-
mana, the second largest Part D insurer, has a marketing arrangement with Walmart. While
marketing increases an insurer’s visibility, it is also signals to enrollees that they are dealing
with a sound and reputable company. Case in point, Medicare recently terminated the plans
offered by a fringe insurer, Fox Insurance, citing several regulatory violations. Finally, ser-
vice quality characteristics such as the accuracy and ease of understanding documentation,
leniency in appeals procedures, and customer service also differentiate plans.
7
Prior authorization requires the plan’s approval before filling a prescription at the pharmacy. Step
therapy routines requires enrollees to try another drug first, and if it is ineffective then the plan provides
coverage.
114 Model
We model the supply and demand system for plans using the discrete choice framework of
Berry (1994); Berry et al. (1995). We separately introduce the demand and supply side.
4.1 Demand
Every year t, a consumer, indexed by i, can enroll in one prescription drug plan. Con-
sumers choose amongst the j = 1, . . . , Jmt differentiated plans offered in market m in year
t. Markets are geographically separated by Medicare regions drawn around state borders.
Residency requirements and the annual enrollment period admit a very clean market defini-
tion; consumers cannot enroll in plans outside their region, nor switch plans within a year.
They may also choose an outside option, j = 0. Following the convention in the demand
estimation literature, we normalize the utility from the outside option to zero. The outside
option includes going without drug coverage, enrolling in an MA+Part D plan, or getting it
from another source, such as a current employer, another government program, or a Retiree
Drug Subsidy program plan.
Each year, enrollees pay a premium pjmt set by the plan. They derive utility from plan
characteristics and income left over after paying the premium. Define the conditional indirect
utility of person i choosing plan j in market m as:
Ui (Xjmt , pjmt ) = −αi pjmt + X0jmt βi + ξjmt + ijmt (1)
where Xjmt is a vector of observable plan characteristics, ξjmt represents an index of unobserv-
able (to the econometrician) plan characteristics, and ijmt is a term capturing idiosyncratic
differences in consumers’ preferences over plans. The terms αi , and βi are random coefficients
that represent consumer i’s marginal utility over income and over product characteristics.
The random coefficients are distributed iid normal across consumers and markets with mean
ᾱ and β̄ and variance Σ. Consumers choose the plan yielding the highest conditional indirect
utility in equation 1.
After describing the supply-side model, we introduce our measures of plan characteristics
in the data section and further discuss factors driving heterogeneity in preferences.
124.2 Supply
We model the supply side by closely following the regulations in the Medicare Modernization
Act of 2003. A set of F multiproduct insurers compete in a Bertrand-Nash fashion. In year
t, each plan j offered in market m submits a bid bjmt to Medicare. Insurers submit separate
bids in each market, even if the plans offered in different markets are otherwise similar. For
each enrollee, the plan receives a monthly payment equal to its bid. Part of that payment is
made by enrollees in the form of the premium pjmt , and the remainder is subsidized by the
government.
We model plan’s marginal costs mcjmt of enrolling a customer as a constant.
As multiproduct firms that can offer plans in many regions, profits for firm f are given
by,
X X
Πf t = Mmt (bjmt − mcjmt )sjmt (2)
mt Jf mt
where Mmt is the number of potential enrollees in market m and Jf mt indexes the set of
plans offered by firm f in market m. The first order conditions with respect to a bid bjmt
are given by,
X ∂sr
sjmt + (br − mcr ) =0 (3)
r∈Jf t
∂bjmt
for all plans across all markets. Notice, we are explicit about summing across all markets;
because of the subsidy rule, the cross derivatives ∂b∂sjmt
r
6= 0 if r is in a different market than
j.
The system of first order conditions can be inverted to solve for marginal cost,
mct = bt + ∆−1 st (4)
where ∆m is a matrix of own and cross price share derivatives appropriately defined for a
∂s ∂s
multiproduct firm. It has elements, ∂bjj for own share derivatives along the diagonals; ∂brj
as off diagonal terms if the same firm offers plans r and j, otherwise zero. The boldface
terms, mcmt and bmt , are vectors of marginal costs and bids. Under the assumption that
the market is in equilibrium, the inversion allows us to estimate marginal cost without any
data on cost. We only need data on bids, market shares, and demand elasticity estimates
from the demand model. Because the demand model is expressed in terms of premiums and
the supply model, in terms of bids, we need to account for the subsidy rules.
The regulation sets the rule for determining the size of the subsidy. The government
13subsidizes a fixed proportion, λt , of the enrollment weighted average bid of all plans in the
country (λt ≈ 65%). The enrollee pays the balance as its premium. Thus, each enrollee gets
the same subsidy amount regardless of plan choice. Enrollees realize savings from choosing
cheaper than average plans, or pay extra to pick one that is more expensive than average.
The determination of the weighted average bid is complicated by the distinction between
basic and enhanced plans. Only the portion of the bid attributable to basic coverage is
included in calculation of the weighted average bid. The portion attributed to enhanced
coverage is not subsidized. A bid bjmt separates into a basic component bbasic
jmt , and enhanced
enhanced
component bjmt ,
bjmt = bbasic enhanced
jmt + bjmt
Plans choose bids but do have discretion allocating between the basic and enhanced compo-
nent. The allocation is based on an actuarial calculation that takes into consideration the
plan’s coverage characteristics. We assume a fixed ratio γjmt between the two components.
benhanced
jmt
γjmt =
bbasic
jmt
For example, γjmt is zero for basic plans and is larger for an enhanced plan that eliminates the
deductible and provides donut hole coverage than for an enhanced plan that only eliminates
the deductible. The formula to map a bid bjmt to a premium pjmt is:
pjmt = bjmt − λt b̄t (5)
The weighted average bid b̄t is based on bids of all stand-alone part D plans and select
MA+part D plans in the entire nation.
X
b̄t = s̃jt−1 bbasic
jt (6)
jt
The weights s̃jt−1 are based on the previous year’s enrollment Ejt−1 ,
Ejt−1
s̃jt−1 = P
jt Ejt−1
The weight is zero for plans that are new entrants to the market. Premiums are bounded
below at zero, but it has never been a binding constraint. In the first year, 2006, the weights
were equal for all plans. The shift from a simple average to the weighted average method
14was gradually phased in through 2008.8
4.3 Supply-Side with Adverse Selection
Adverse selection may bias our marginal cost estimates. Marginal cost depends on the
drug consumption (or risk profile) of a plan’s pool of enrollees; “sicker” consumers are more
costly to enroll than “healthier” ones. Adverse selection occurs because a plan’s risk profile
depends on its premium and coverage characteristics relative to competing plans. Adjusting
bids shuffles the sorting of enrollee risk-profiles across plans. Our model’s constant marginal
cost is implicitly invariant to the risk profile of the pool of enrollees and thus potentially
misspecified.
Medicare uses risk adjustment payments to combat adverse selection. They gather highly
detailed enrollee demographic and health information from Medicare records9 to compensate
plans that attract high risk pools. With perfect risk adjustments, our model of constant
marginal cost is correctly specified; even with less than perfect risk adjustments, the bias
is mitigated. See Fong and Schwarz (2009) and McAdams and Schwarz (2007) for further
discussion. But, it has been documented that Medicare’s risk adjustments are not perfect
(Lustig, 2010), and we believe adverse selection is a legitimate concern.
Without individual level data we cannot account for adverse selection, and thus it is
beyond the scope of this paper. Nonetheless, it is useful to understand how adverse selection
would bias our marginal cost estimates. In the appendix, we expand our supply-side model
and follow the intuition in Lustig (2010) to heuristically sign the bias for basic and enhanced
plans. The bottom line is that our marginal cost estimates for basic plans may be overstated,
and understated for enhanced plans.
4.4 Elasticities with Subsidy Distortion
To perform the inversion that solves for marginal cost, it is necessary to express demand
elasticities in terms of bids, not premiums. For ease of notation, we use a non-random
coefficient specification to illustrate how the subsidy rule distorts insurer’s residual demand
8
The “Medicare Demonstration to Limit Annual Changes in Part D Premiums Due to Beneficiary Choice
of Low-Cost Plans” act, passed in mid-2006, amended the original legislation to phase-in the weighted average
bid calculation method.
9
Healthcare Effectiveness Data and Information Set (HEDIS)
15elasticities. The market share for plan j in region m in year t is given by:
M
sjmt = Pjmt
1 + k Mkmt
where ! !
X bkmt
Mjmt = exp −α bjmt − λt s̃kmt−1 + X0jmt β + ξjmt .
k
1 + γjmt
We substituted bids in for premiums using the subsidy rule given in equation 5. There are
three relevant price elasticities given in equation 7: own price, cross price with a plan offered
in the same market m, and cross price with a plan offered in a different market m0 .10
h i
∂sjmt bjmt λt
ηjjmt = ∂bjmt sjmt
= −αbjmt (1 − sjmt ) − 1+γjmt s̃jmt−1 (1 − s0mt )
h i
∂skmt bjmt
ηkjmt = ∂bjmt skmt
= −αbjmt −sjmt − 1+γλtjmt s̃jmt−1 (1 − s0mt ) (7)
h i
∂skmt bjm0 t λt
ηkjm0 t = ∂bjm0 t skmt
= −αbjm t − 1+γ 0 s̃jm t−1 (1 − s0mt )
0 0
jm t
The second term inside the brackets captures the distortion in residual demand elasticities
cause by the subsidy. The distortion makes own-price elasticities more inelastic and cross
price elasticities larger relative to a market with no subsidy. The intuition is that when plan
j in market m increases it’s bid, the subsidy increases for all plans across the nation. With a
larger subsidy, inside goods become more attractive relative to the outside option. Insurers
internalize the subsidy distortion and will have higher markups, more so for large national
insurers with high enrollments (hence high weights s̃jmt−1 ) that offer plans in many markets.
Also notice the subsidy distortion would be more severe if the subsidy fraction λt were higher
or if Medicare subsidized the enhanced component of bids (γjmt =0 for enhanced plans).
In our results, we quantify the impact of the subsidy rule on markups by comparing our
estimated markups to estimates from a model where insurers treat the subsidy amount as
lump sum.
5 Data
We collected publicly available data from the Center for Medicare and Medicaid Services
(CMS) on plan level enrollment and bids for all stand alone part D plans offered since the
the programs inception in 2006 through 2009. We also purchased detailed data on plan
10
Because the weights s̃jmt−1 are based on lagged enrollment, we could also calculate cross price elasticities
across time. We don’t because our model is static.
16characteristics from CMS. There are four files. The formulary file lists all drugs on a plan’s
formulary, the beneficiary cost file describes cost sharing rules, the pharmacy network file
lists all preferred and non-preferred pharmacies, and the pricing file reports average drug
transaction prices for every drug and plan. The pricing file was first published in 2009, the
other files are available in all years. Specifically, prices are the average transaction price net
of all rebates for a 30 day supply filed at the plan’s preferred pharmacies in Q3 2009.11 They
are used to calculate enrollee drug expenditures. It’s worth noting that enrollees may not
know the exact drug price during the enrollment period because drug prices and rebates vary
throughout the year, and prices reported by the ”Plan Finder” tool on Medicare’s website
are not necessarily accurate.12
5.1 Enrollment and Premiums
Across the four years and 39 regions, 75 insurers offer stand alone Part D plans. The market
penetration of insurers is quite skewed; 18 national firms offer plans in all states,13 while 44
regional insurers offer plans in just one market. Insurers offer an average of 2.5 plans in a
market, with most offering 1, 2, or 3 plans.14 At least one must be a basic plan.
Enrollees have lots of choices. A typical enrollee can choose from over 40 plans offered
by about 20 insurers. Table 6 shows the average number of insurers and plan offerings in a
market. The entries are broken down by year and plan segment: Enhanced and Basic.
Despite the large number of insurers, the Part D market is highly concentrated. Table 7
reports various measures of firm concentration (1-firm concentration, c1, 2-firm c2, 4-firm c4,
and Herfindahl-Hirschman index) averaged across markets. The top firm (United Healthcare
for most markets) commands an average 36% market share, while the top 4 firms, 73%. The
11
Plan’s report all transactions, called Prescription Drug Events (PDE) to CMS. A PDE includes in-
formation on prices and all rebates/discounts with manufacturers, wholesalers, and pharmacies. Rebate
information is proprietary, only the net price is available to researchers. Some pharmacies charge a dispens-
ing fee, on the order of a couple dollars, that may or may not be included in the net drug price. Our data
are based on PDE records.
12
Every two weeks plans are required to submit a separate pricing file to CMS that is used in the plan
finder database. The database is not constructed from PDE records. If the plan never submits a price, the
finder reports a price 30% below the average wholesale price for generic drugs, 10% below for brand name
drugs. Even if a plans submits a price, it may not get updated every 2 weeks, so the prices can be outdated.
Recently, Medicare began reporting survey results that ask enrollees to rate the accuracy of drug prices paid
at the pharmacy compared to price reported on the plan finder. Many plans get very poor ratings.
13
excluding 5 markets for US territories with very small penetration
14
There are a few exceptions where insurers offer more than 3 plans, up to a maximum of 9. The most
notable is in 2006 when United Healthcare, the market leader, offered 5 plans. Two of these plans were
sponsored by Pacificare, which was acquired by United Healthcare. United Healthcare consolidated these 5
plans into 3 in 2007.
17HHI averages 2376, which according to the Department of Justice guidelines falls into the
“moderately concentrated” category.15 Overtime, the markets have become less concentrated
but still fall into moderately concentrated levels.
Table 8 reports national enrollment as a percentage of all eligible Medicare beneficiaries
(≈ 42 million) and monthly premiums. The table divides shares into three categories: stand
alone part D plans, bundled MA+Part D, and stand alone Medicare Advantage plans. Stand
alone Part D enrollment has been stagnant since program inception in 2006, while monthly
premiums have risen dramatically; average premiums rose about 30% between 2006 and
2009. Meanwhile, both stand alone MA and bundled MA+PartD, plans have experienced
an increase in enrollment. Tables 9 reports enrollment and premium statistics separate by
basic and enhanced plans. Basic plans attract about 3 times as many enrollees and charge
30% lower premiums as compared to enhanced plans.
Table 10 reports more detailed summary statistics for both basic and enhanced plans at
the market level. Note the large variation in premiums for both plan segments as well as the
variation and skew in enrollment figures. The average basic plans enrolls 1% of Medicare
beneficiaries, while the largest, upwards of 18%. The average enhanced plan has a smaller
share, .4%, but the distribution also exhibits a large skew.
Every year Medicare announces the official average bid amount b̄basic
t and average pre-
basic basic
mium b̄t − λt b̄t . These figures, along with the calculated subsidy fraction λt , are
reported in table 11.16 Table 12 reports summary statistics on plan bids.
5.2 Plan Characteristics
Our primary plan characteristic variables measure the generosity of plans coverage. Our
first variable is the deductible. The second and third are intended to measure the generosity
of coverage in the initial coverage and donut hole regions. The challenge is taking our rich
drug-level data and converting it into a meaningful plan-level characteristic.
We construct price indices for the top 100 most popular drugs ranked by prescriptions
15
A market with a HHI between 1800 and 2500 is considered moderately concentrated.
16
The official average bid and average premium are reported by Medicare. We also observe the basic
and enhanced component of the bid for all stand alone Part D plans. We do not have complete data on
MA+Part D bids due to further complications in the rules for subsidizing MA+Part D plans. Instead, we
use enrollment figures from MA+Part D plans and the subsidy formula (equation 6) to calculate an average
basic bid for MA+Part D plans. Since MA+Part D plans are included in the outside option, the average
bid is a sufficient statistic for us to properly calculate marginal cost and perform counterfactuals. Because
of the phase-in of the weighted average bid method, we are missing data that would allow us to calculate
marginal cost in 2006 through 2008.
18filled.17 Our first price index reflects the out of pocket cost for an enrollee to fill a 30 day
supply for a basket of the 100 drugs when they are in the initial coverage zone. Our second
price index reflects out of pocket costs in the donut hole. The basket of drugs evenly weights
each drug (1/100th). While there may be drug-by-drug idiosyncratic variation in a plan’s out
of pocket prescription drug cost, this measure captures a plan’s average cost across drugs.
Constructing out of pocket costs is straightforward for drugs covered by a copay. For drugs
covered by coinsurance, it is necessary to know the price of the drug. We use the 2009 pricing
file. For off-formulary drugs, enrollees do not receive coverage, therefore the out of pocket
cost is the full retail price. We set the retail price to the average price in the region.18 We do
not construct a price index for the catastrophic region because there is virtually no variation
across plans.19
There are three sources of variation in the price indices: copay and coinsurance rates,
negotiated drug prices, and formulary composition. Table 14 reports statistics on out of
pocket price indices for the top 100 drugs and separate indices for brand and generic. Most
of the variation in the donut hole is between enhanced plans that fill the donut hole and
basic plans with no coverage. There is more variation in the initial coverage zone than in the
donut hole. The source of this variation comes from differences in copay rates. Comparing
brand and generic drugs, the variation is larger for brand name drugs. Its also interesting to
note trends across time. Average donut hole prices remain steady, while out of pocket prices
in the initial coverage zone fall across years.
Figure 3 shows a histogram of negotiated prices for all drugs in 2009. To compare across
drugs, we record prices as percent deviations from the drug’s average price. Notice there is a
lot of price dispersion; it contributes to the variation in our price indices. To give a sense of
magnitude, 10% of drugs are priced 25% below the average, and 10% are priced 15% above
average. The dispersion is quite remarkable considering these are perfectly homogenous
17
CMS published a report ranking the top 100 drugs by number of prescriptions filled by Part D enrollees
in 2006. Rankings by cost are quite different. For example, the generic drug FUROSEMIDE is number 1 by
prescriptions filled and 98 by cost.
18
Since the base price includes rebates and discounts, we are probably understating retail prices by using
negotiated prices. We use the average national price in rare cases where a region price does not exists. For
the years 2006 to 2008 we construct the price indices in the same manner using 2009 prices. For plans that
did not exists in 2009, we use average regional prices. Drug prices, coinsurance rates, and copays differ
across preferred, non-preferred, and mail order pharmacies. All of our calculations are based on preferred
pharmacies.
19
The Part D regulations do not allow plans to use a tiered copay/coinsurance structure in the catastrophic
region. Out of pocket payments are capped at $5 per prescription or 5% of drug cost. There is little variation
across plans. Moreover, few enrollees, only 8% in 2006 reached the final tier, and of that group, they are
over-represented by the low income subsidy enrollees who pay zero in the catastrophic region.
19products.
We measure formulary comprehensiveness by counting the number of top 100 drugs in-
cluded on a formulary. We also break this list down by brand and generic medication; there
are 42 brand name medications and 58 generic. Table 13 reports statistics on formulary
comprehensive. On average plans cover most of the drugs (more than 90%), but there is
significant variation that appears to have grown over the years, indicating the plans are more
differentiated now than in 2006. There is little difference between enhanced and basic plans.
Insurers typically share formularies for their plans. Across all four years and regions there
are 6679 plans and 400 formularies. Th only intended to illustrate a source of variation in
the price index; we do not includes these drug counts as a separate plan characteristic.
Across the universe of Part D drugs, over 5400, there is a lot of idiosyncratic variation in
formularies. Figure 2 depicts a snapshot of formularies in 2009. Gaps in the formularies show
that less comprehensive formularies are not strict subsets of more comprehensive formularies.
With so many non-overlapping formularies, each enrollee is likely to find a plan tailored his
individual drug regimen. This suggests enrollees sacrifice very little in terms of choice when
plans use formulary restrictions as a bargaining chip with drug manufacturers.
From our data on pharmacy networks, we construct a measure of network coverage by
counting the number of in-region network pharmacies per eligible Medicare beneficiary in
the region. We group preferred and non-preferred pharmacies because many plans do not
make a distinction.
5.3 Basic vs Enhanced Plan Characteristics
Figures 4, 5, and 6 display side-by-side histograms of coverage characteristics for basic and
enhanced plans in 2009. They illustrate the relative location in characteristic space for the
two categories. The differences are relevant because they drive the substitution patterns
in our counterfactual that introduces a basic government option. The plans are highly
differentiated with respect to the monthly deductible. Most basic plans have the maximum
deductible ($295 in 2009), while most enhanced plans have a $0 deductible. No systematic
difference emerges in the histograms for the price index in the initial coverage zone, but there
are differences in the donut hole price index. Almost no basic plans have a price index below
100, while about 50% of the enhanced plans fall below the $100 thresholds. The price index
is lower for these enhanced plans because they provide some coverage in the donut hole.
205.4 Heterogeneity in Preferences: Random Coefficients
Our most flexible demand specification includes random coefficients on the monthly premium,
deductible, and out of pocket price indices. As in a typical demand system, the random
coefficient αi captures heterogeneity in consumers’ marginal utility over income, driven by
differences in income and price sensitivity. Two other factors affect the distribution of αi :
the low income subsidy and late enrollment penalty. The low income subsidy truncates αi .
For example, it is zero for those receiving a 100% subsidy and half of what it would otherwise
be for an individual receiving a 50% subsidy. For an enrollee subject to the late enrollment,
penalty—1% per month not enrolled— αi increases in proportion to the duration of late
enrollment. Combined, the low income subsidy and late enrollment penalty increase the
variance on the distribution of αi . They may also skew the distribution, but we lack data
on these populations to estimate higher order moments of the distribution.
Heterogeneity in preferences for the deductible and out of pocket price indices are driven
by heterogeneity in enrollee’s health status and risk aversion. All enrollees (weakly) prefer
a lower deductible, but “Healthy” enrollees have a relatively low (in magnitude) marginal
utility with respect to the deductible because their drug expenditures are unlikely to exceed
the deductible. “Sick” enrollees have a higher marginal utility because they would expect to
spend through the deductible with certainty. By the same reasoning, health status affects
preferences over out of pocket prices in the initial coverage and donut hole regions. It’s
worth noting, enrollees care not only about the cost sharing rates in the marginal tier of the
tariff schedule they fall into (deductible, initial coverage, donut hole, or catastrophic), but
also tiers they surpassed. Marginal utility only diminishes for the higher tiers that they are
unlikely to enter. More risk averse enrollees place a higher preference on the deductible and
price indices. Like the premium, the low income subsidy truncates the distributions towards
zero.
We use a parsimonious Normal distribution over the random coefficients with a block
diagonal covariance matrix. However, this distribution may not be appropriate for three
reasons. First, in a model of demand for drugs with a kinked tariff schedule, the distribution
of drug expenditures will exhibit bunching and gaps around the kinks (Marsh, 2010). In
our model of plan demand, this translate into gaps and mass points in the distribution of
random coefficients. Second, we would expect correlation in the random coefficients across
the tiers of the tariff schedule because they all relate to expenditures of money. For a risk
neutral enrollee, a dollar spent on the premium is worth exactly the same as an (expected)
dollar spent in the later tiers. This implies an enrollee’s marginal utility over characteristics
21monotonically decreases moving down the tariff schedule. The premium should have the
highest coefficient because it is paid with certainty, and the donut hole should have the
lowest coefficient since it is not necessarily reached with certainty. Third, if consumers are
risk averse, a risk premium is built into their preferences which further complicates the
correlation structure of random coefficients. The distribution over the marginal tier that
an enrollee enters matters for the risk premium. For example, a consumer that exceeds the
deductible with certainty places a risk premium on the coefficient in later tiers and no risk
premium on the deductible coefficient. For estimation, we experimented with specifications
that accommodate these three qualifications (correlation in random coefficients, discrete type
models (Berry and Jia, 2010), and mixtures models with Normal and discrete distributions)
but could not obtain sensible results. In principle these richer models may be identified
with aggregate data (?), but accessing consumer level data, as in Abaluck and Gruber
(2009), would help with identification. We leave this as future work. Nonetheless, the
focus of this paper is on the the supply-side for which the demand model is a means to
obtain reasonable price elasticity estimates. With our more parsimonious random coefficient
model, we estimate sensible elasticities and ameliorate the standard criticisms of non-random
coefficient discrete choice models.
5.5 Heterogeneity in Preferences: Idiosyncratic Preferences
The idiosyncratic logit error terms, ij , reflect unobserved heterogeneity in preferences that
are not otherwise captured by random coefficients. There are several reasons we believe they
should enter our demand specification. Drug purchasing patterns are likely the primary
source of idiosyncratic preferences. Enrollees have stronger preferences for plans that cover
their specific drug regimen at low out of pocket prices. Thus, drug-by-drug idiosyncratic dif-
ferences in formulary composition and copay/coinsurance rates generate idiosyncratic pref-
erences. Figure 2 illustrates idiosyncratic differences in formulary composition; a similar
visual representation of copay/coinsurance rates shows the same pattern. Marketing activ-
ities and pharmacy networks may also contribute to idiosyncratic preferences. Using the
examples from before, AARP members might have stronger preferences for AARP endorsed
plans, and Walmart customers might prefer plans that contract with Walmart. It is also
worth noting low income subsidy enrollees who accept random assignment to plans. Their
behavior can be rationalized in our model by attributing the random assignment to draws
from the distribution of ij .
22? and Berry and Pakes (2007) have critiqued this model because the dimensionality
of ij increases as products are added. The added term ensures consumers benefit from
the introduction of a public option, even if it has a high premium, undesirable average
characteristics, and there is no competitive response by existing plans. We justify the extra
ij term for the government plan by assuming its formulary and copay/coinsurance rates
will exhibit the same sort of idiosyncratic differences found amongst the privately offered
plans. These difference are a likely outcome because the legislation permits the government
to bargain with drug manufacturers using restrictive formularies and tiered copays, just like
private plans.
6 Estimation
In this section, we report our demand and supply-side marginal cost estimates.
Our most flexible demand specification includes random coefficients on the monthly pre-
mium, deductible, and out of pocket price indices. We also report estimates for non-random
coefficients specifications estimated by OLS and IV, and a more parsimonious random coef-
ficient specifications.
We include formulary fixed effects. They control for unobserved differences in the mean
quality of formularies that would otherwise be difficult to measure with a few observable
coverage characteristics. Formulary fixed effects have two advantages. First, they capture
the desirability of the entire formulary, not just the top 100 drugs that are included in the
out of pocket price indices. Second, without fixed effects, the price index variables may be
correlated with mean unobserved quality in ξ. Specifically, the price index could be high
because the formulary composition includes many high-cost, high quality drugs. Formulary
fixed effects purge this correlation. The remaining characteristics in ξ reflect marketing
activities and service characteristics.
We use the instruments proposed in BLP to instrument for the endogenous premium
variable: the sum of the other exogenous observable product characteristics offered by rival
firms and by the firm’s other plans. It is necessary to justify the validity of the instruments:
that is, the exogeneity of the characteristics. The price index variables are exogenous for
several reasons. First, the benefit design is regulated by Medicare, not chosen by plans.
Second, the underlying drug prices are set by pharmaceutical manufacturers, not insurers.
Part D enrollment may affect insurers’ bargaining power in drug price negotiations which
brings into question the validity of the instruments. In defense, enrollment does not change
23You can also read