The Canadian Epilepsy Database and Registry - Cambridge ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
The Canadian Epilepsy Database
and Registry
R.S. McLachlan
ABSTRACT: Epilepsy encompasses medical, psychological, social and demographic factors which are
best studied in large populations. The Canadian Epilepsy Database and Registry (CEDAR) is a compre-
hensive English language, multicentre epilepsy database which has been developed to study the impact of
these and other factors on epilepsy in Canada. In addition, it can be used locally in the clinic for office
record keeping, automated printout of a referral letter or graphing seizures and other data over time. The
data in CEDAR are similar to what is found in the patient's chart. There are 20 participating centres
across Canada which have entered data on over 8000 adult and pediatric epilepsy patients. The informa-
tion in CEDAR will be available for research purposes to centres entering data as well as to academic
researchers, the pharmaceutical industry and government agencies.
RESUME: La Banque de donnees et le Registre canadien de I'epilepsie. L'epilepsie comprend des facteurs medi-
caux, psychologiques, sociaux et demographiques qu'on peut mieux etudier dans des grandes populations. La Banque
de donnees et le Registre canadien de I'epilepsie (BRCE) est une banque de donnees 6tendue, multicentre, en anglais,
sur I'epilepsie qui a ete developpee pour etudier l'impact de ces facteurs et d'autres facteurs sur l'6pilepsie au Canada.
De plus, elle peut etre utilisee localement en clinique pour la tenue de dossiers, pour imprimer automatiquement une
lettre, pour referer un patient ou pour dessiner un graphique des crises ou d'autres donnees dans le temps. Les donnees
dans BRCE sont semblables a ce qu'on retrouve dans le dossier du patient. Les 20 centres participants a travers le
Canada ont entre des donnees sur plus de 8000 adultes et enfants epileptique. L'infoimation dans BRCE sera mis a la
disposition des chercheurs des centres qui entrent des donnees, des chercheurs du milieu acadeinique, de 1'industrie
pharmaceutique et des agences gouvernementales, a des fins de recherche.
Can. J. Neurol. Sci. 1998; 25: S27-S31
The astounding impact of computerization on medical prac- under the leadership of Dr. Joe Dooley from Halifax with start-
tice and research over recent years can be illustrated by many up funding from Parke Davis. One of the goals of this consor-
examples. Imaging of the human body using computer tech- tium was to develop and implement a pediatric epilepsy
niques for diagnosis and clinical research is commonplace. No database. In 1995, Dr. Dooley and 1 discussed including epilep-
secretary would be without a powerful word processor which sy of all ages in the database which could then be used by both
has replaced the electric typewriter used in most offices only 15 adult and pediatric neurologists on a national basis. The original
years ago. Not surprisingly, computers designed to store, orga- concept was to have two databases, one for pediatrics and one
nize and retrieve large amounts of information are also emerg- for adult epilepsy, but it quickly became apparent that the
ing as important tools for clinical database development and degree of overlap was so great that one combined database
management. The purpose of this article is to briefly describe would be most appropriate. Thus, CEDAR was born under the
the recent development and potential usefulness of a Canadian auspices of the Canadian League Against Epilepsy (CLAE) with
epilepsy database. financial support from Burroughs Wellcome followed by Glaxo
Over the past 10 years, more and more individual physicians Wellcome.
have attempted to develop working clinical databases for their The main purpose of CEDAR is to assist in the establishment
own offices or clinics with varying degrees of success. Early of a disease specific research network to enhance epilepsy
software platforms for database development were cumbersome research in Canada. The information in CEDAR is of potential
and many physicians did not appreciate the time and effort use to academic researchers, the pharmaceutical industry and
required to establish a useable database. It was on this back- government agencies. CEDAR can provide detailed information
ground that the Canadian Epilepsy Database and Registry from large numbers of patients on epidemiology, genetics,
(CEDAR) was designed as the first English language national seizure types, epilepsy syndromes, antiepileptiec drug doses or
epilepsy database in the world and one of the first widely used,
disease oriented software programs.1 The only other country to
have developed a successful multicentre, comprehensive epilep- From the London Health Sciences Centre, University of Western Ontario, London.
sy database is Italy.2 Based on a lecture given at Glaxo Wellcome in Mississauga in September 1997.
Reprint requests to: Richard S. McLachlan, M.D., University of Western Ontario, Lon-
The concept for a national epilepsy database took form in don Health Sciences Centre, University Campus, 339 Windermere Road., London,
1994 when a pediatric neurology consortium was established Ontario, Canada N6A 5A5
Downloaded from https://www.cambridge.org/core. IP address: 46.4.80.155, on 09 AugSuppl. 4 - S27subject to the Cambridge Core terms of use, available at
2021 at 10:38:50,
https://www.cambridge.org/core/terms. https://doi.org/10.1017/S0317167100034946THE CANADIAN JOURNAL OF NEUROLOGICAL SCIENCES
adverse effects, efficacy of treatment over time, quality of life and The end result is a Windows based program using Microsoft
any combination of these. Anyone who wishes access to data in Access 2.0, the best platform available at the time, with ability
CEDAR must submit a proposal in writing to the executive com- to run on individual personal computers as well as networks.
mittee of the CLAE who will determine if the request is reason- CEDAR runs best on a Pentium computer with at least 16
able and if there are costs involved. Since the information megabytes of RAM and an SVGA monitor. It is not yet avail-
regarding patients in the national database is anonymous, any able for Macintosh users. There are 13 data screens (Figures 1
research requiring further patient contact can be done through and 2 are examples) as well as pregnancy and surgery screens.
individual participating centres with the patient's consent. Subse- The content and structure resemble what would be found in a
quent to the development of CEDAR, a Canadian Epilepsy Con- patient's chart, including history, physical, diagnosis, investiga-
sortium (CEC) was formed with a mandate of focusing on, tions, treatment, quality of life and follow-up. The International
encouraging and coordinating multicentre research trials in Classification of Seizures3 and the International Classifications
epilepsy in Canada. The CEC/CEDAR initiatives are complimen- of Epilepsies4 are used to document seizures and syndromes;
tary to one another and provide a powerful resource for industry details regarding seizure frequency and type as well as dose and
and government funded epilepsy research in this country. side effects of antiepileptic drugs are updated at each return visit
More than two years of work by many people including of the patient. CEDAR version 2.0, based on feedback from
numerous clinicians and two software programmers was users who entered the first 5000 patients, incorporates automatic
required before CEDAR version 1.0 was available for distribu- data analysis for individual clinics. It also has graphing capabili-
tion to Canadian epilepsy centres in February, 1997. During ty for data collected over time such as individual response to
development, as pediatric and adult neurologist across the coun- antiepileptic drugs and the ability to generate a summary letter
try submitted suggestions for content, it became apparent that for the referring physician. It will also print a Patient Summary
CEDAR could not only be used as a research tool, but as a prac- page of commonly required information (Figure 3). Examples of
tical office resource for following and analyzing patient data in the type of data available from CEDAR are seen in Tables 1 and
individual clinics. Much effort was directed at making CEDAR 2. Figure 4 shows a sample graph.
as users friendly as possible by incorporating mouse-driven In order to make CEDAR as user-friendly as possible, we
menus and pick lists throughout. elected to leave out specific data fields which were of interest to
File Edit Cedar Cedar fleports Help \=1§M
lAdemo, Joanne
Choose J
Patient pj ; lliJ,',i4ll„l„| ; fff fiSBg^fl Last Opened: f g g g | j Age: E l EHM
Open
Canadian Canadian
Epilepsy League
Database Against
and Epilepsy
Registry
Version 2.0
Figure 1: Patients are selected from the main screen of CEDAR and the desired information file is opened, (fictitious patient)
Downloaded from https://www.cambridge.org/core. IP address: 46.4.80.155, on 09 Aug 2021 at 10:38:50, subject to the Cambridge Core terms of use, available at
https://www.cambridge.org/core/terms. https://doi.org/10.1017/S0317167100034946
Suppl. 4 - S28LE JOURNAL CANADIEN DES SCIENCES NEUROLOGIQUES
Ademo. Joanne Chart No: 11-22-33
Syndrome: Tempoial lobe epilepsy
Etiology Group Afebrile Statu* Epilepticu*
O Idiopathic (Genetic) O Cryptogenic (Cause Unknown) &.*• [ f y m ^ o j S ^ A ^ i S n L i Type: | Complex Partial | ll
Cause >- - " - • • ' » ' •> f, -
Age at First Seizure: 23 Years | ! | Duration: 3 (Hours)
Seizures Occur in Clusters? |*7
imfanaagifflM^aimismMftSM *
CNS Infection • CJ Disease
CNS Infection • Herpes Encephalitis Age at First Episode: | 25 Years 11\
Seizures exclusively Diurnal? V Nocturnal? V CNS Infection • Other Encephalitis
Longest Sz-free period since onset: | 8||Months CNS Infection -Viral Meningitis
Age at start of Seizure-free period: | | |Years
1*1 Cortical Dysplasia
Genetic Syndrome
Precipitant*
Hydrocephalus [Fatigue I Sleep Deprivation
Injuries due to Epilepsy None | S|
Sleep
Injuries: Metabolic Alcohol
Neurocutaneous Syndrome Poor Compliance
Neurodegenerative Fever / Infection
Prenatal Damage Photic
Febrile Seizures
Perinatal Damage
Exercise / Hyperventilation
Occurred? f Age at First: | ||Months l~fj Trauma
Tumor - Benign Astrocytoma Menstrual
Recurrence?! - Age Recurred: [ "[[Months | j j | Reflex
Tumor - Ganglioglioma Startle
Atypical Characteristics Tiimnr • HflmArlnmA izi Other
Other: One for the record books
.Id.
Focal? r Duration > 30 Minutes? \~
Head Trauma
Clusters? p* Abnormal Exam? [""
Occurred? | 7 Type: Closed 111 Description:
Family History - Siblings? ["" Others? V Severity: Mild [concussion) 11\ Amnesia? |~" Duration: [ |f
13
Age at Injury: f~" Years
Seizure Types and Seizure
History
J Lost Consciousness? ,|T .;-
Epilepsy Syndromes Time until 1st Seizure: D uration: f 11M inutes | i J
Comments
13
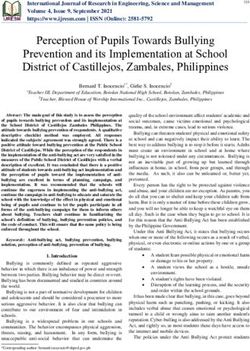
Figure 2: Opening the Seizurefilefrom the Main screen brings up the Seizure History screen. The International Classifications of Seizures and Syn-
dromes is entered from this screen and additional typewritten comments can be entered under "Seizure History Comments ".
only selected clinicians or marginally to the whole group. record. In this regard, it should be kept in mind that databases
Although CEDAR does not document every piece of informa- such as CEDAR are not static but are evolving processes
tion that might be available on a patient, there are numerous which require changes in content and structure over time.
fields where additional comments can be typed into the patient Thus, it is important to design a program from the outset
which is flexible and can incorporate such changes. CEDAR
Table 1: Summary Reports. allows us to do that and the plan for version 3.0 is to update to
Visual Basic or Access 97 as a platform which will provide
Patients listed by: -AED even greater flexibility and ease of use, particularly in the net-
-Seizure type work environment.
-Epilepsy syndrome CEDAR is now used by 20 centres across the country (Table
3) but is available through the CLAE for any physician who fre-
-Surgery type quently sees patients with epilepsy. Individual neurologists vary
-Name
-ID number Table 2: Seizure Classification Summary.
Seizure classification Seizure Type* Number of Patients (n = 7559) Percent of Total
Epilepsy syndrome Simple partial 1158 .15%
AED use Complex partial 2472 33%
Abnormal test results Partial evolving to GTC 1839 24%
Physician directory Generalized 3629 48%
Inactive
Inactive patient
patient list
list *Patients can have more than one seizure type.
Suppl. 4 - S29
Downloaded from https://www.cambridge.org/core. IP address: 46.4.80.155, on 09 Aug 2021 at 10:38:50, subject to the Cambridge Core terms of use, available at
https://www.cambridge.org/core/terms. https://doi.org/10.1017/S0317167100034946THE CANADIAN JOURNAL OF NEUROLOGICAL SCIENCES
Summary of Patient's Epilepsy
Summary Ademo, Joanne 34; Years j
Chart: 11-22-33
ft;
Age at First Seizure: j_23J Years Status Epilepticus: Complex Partial
AED From Dose Now Previously Used AEDs
Carbamazepme j19-Sep-97j>| 1200]; i
Clonazepam
Clobazam ||19-Sep-97jJ 10]; Gabapentin
Lamotrigine :J19-Sep-97|] 300' Methylphenobarbital
. . . .-•-,. Nitrazepam
O Idiopathic C r y p t o g e n i c ^ ^Symptomatic ' Drug Allergies |
Seizure Classifications ?*-•
£
__1.4|,|Simple Partial • - 11 with psychic symptoms ir
.' Desc: deiavu
f$
:
2.5] |Complex Partial • . ' ' •" j |SPS with psychic symptoms evolving to CPS
^l
Desc: I^OA with automatisms
_ 3 J | jPartial evolving to GTG!)|SPS evolving to CPS evolving to GTC
H
:
^
fWir I !!-
SyndrornefsJ
1.2.1 Temporal lobe epilepsy
>,•:*
,m
Etiology
:.«ifc Surgery |±.
Temporal Lobectomy - Left
CNS Infection - Bacterial Meningitis
Mesial Temporal Sclerosis -fi r
Tumor - DNT (dysembryoplastic neuroe _
' * " ' ' • < % ' "
One for the record books " frirrt SuTmmary RepoflKl
Figure 3: A summary of an individual patient's data is useful for quick reference such as when speaking to a patient on the telephone.
in their use of CEDAR, some documenting basic clinical infor- entry can take 30-45 minutes and is often done by a nurse or
mation only on their patients, while others rely on it as they other clinical assistant but follow-up information can be entered
would the patient's chart. Clinic nurses have found CEDAR to in two or three minutes. Patient data, stripped of identifying
be particularly useful in their follow-up of patients. Initial data information, is downloaded periodically to the national database
Table 3: Centres Contributing to CEDAR. Table 3: (continued).
Dr. R.S. McLachlan London Dr. E. Starreveld Edmonton
Dr. J. Dooley Halifax Dr. B. Sinclair Edmonton
Dr. M. Jones Vancouver Dr. S. Levin London
Dr. R. Desbiens Quebec City Dr. M. Sadler Halifax
Drs. N. Pillay/J. Maher Winnipeg Dr. J.D. Buckley St. John's
Dr. G. Ronen Hamilton Dr. M.A. Lee Calgary
Dr. K. Farrell Vancouver Dr. H.Z. Darwish Calgary
Dr. A. Guberman Ottawa Dr. F. Dubeau Montreal
Dr. J.M. Saint-Hilaire Montreal Dr. A. Ogunyemi St. John's
Dr. J. Schneiderman Toronto Dr. N. Lowry Saskatoon
Downloaded from https://www.cambridge.org/core. IP address: 46.4.80.155, on 09 AugSuppl.
2021 at 10:38:50,
4 - S30subject to the Cambridge Core terms of use, available at
https://www.cambridge.org/core/terms. https://doi.org/10.1017/S0317167100034946LE JOURNAL CANADIEN DES SCIENCES NEUROLOGIQUES
file £dit £edat Cedar Qepoits j^elp
\ •'•^C-AV^'""'4*^ifefc*>:'i>i •
8z, Frequencies for Complex Partial - eRS^jtopsycrji^symptajris^^ symptoms Complex
Partial - SPS
10 t t -t—» «
- Vt with psychic
•• . » — * - N
| 8 symptoms
— V ^ 3 evolvi
i a 4
V) 2 • Simple Partial -
with psychic
I; • "---ui ^ d 3' d\ & •«' >' o'' J to" is'," tf' *!*' »9»'ei> ;"5" c$u!*t" •>»'.*' t ) - i »>>'* •ef-ivitv,St***^*'. tc*';-.'S~* ..V.'\ ?.v ;x.-..k-.. .;'. ±1
i^^-N'V- I I Carbamazepira
3
I Clobazam
! 8f | 3 f & S £ 8 8' S |' i £ I •?' 4 $ $ £ $ &' tS'« I* £ £ §' 3* Sr
±IJ .d
33
Lamatrfgine Dose and Blood Levels DBlood
•300 Levels
.= 22'
•200 i
; a. ^ 100 t Lamotriglne
0
^ B' - | | g
< s r» «
.«, > ,y. ...v^...-„>, ..V> •I
Figure 4: Data from individual patients can be graphed over time based on frequency of different seizure types, drug doses andAED blood levels.
situated in London, Ontario. As of this writing, there were REFERENCES
approximately 8000 patients in the database. Our goal of at least 1. McLachlan RS, Dooley J, Casbourne H. Canadian Epilepsy
10,000 patients will provide a sound basis to begin some studies Database and Registry. Epilepsia 1997; 38 (Suppl. 3): 89.
on treatment, outcome and epidemiology of epilepsy. As the 2. Avanzini G. For the Network Epilepsy Centers Regione Lombar-
dia. Survey of the diagnostic and therapeutic approach to
numbers increase, the power of CEDAR as a research tool will patients followed by the Lombardia Epilepsy Network. Epilepsia
of course grow. With time, it may be possible to incorporate a 1995; 36 (Suppl. 3): 62-63.
disease specific database such as CEDAR with other neurologi- 3. Commission on Classification and Terminology of the International
League Against Epilepsy. Proposal for revised clinical and elec-
cal databases (e.g., headache, stroke, multiple sclerosis) to pro- troencephalographic classification of epileptic seizures. Epilep-
vide a comprehensive and powerful resource for neurology sia 1981; 22: 489-501.
research as well as general neurology office and clinic manage- 4. Commission on Classification and Terminology of the International
League Against Epilepsy. Proposal for revised classification of
ment. epilepsies and epileptic syndromes. Epilepsia 1989; 30: 389-399.
Downloaded from https://www.cambridge.org/core. IP address: 46.4.80.155, on 09 Aug Suppl. 4 - S 3 1subject to the Cambridge Core terms of use, available at
2021 at 10:38:50,
https://www.cambridge.org/core/terms. https://doi.org/10.1017/S0317167100034946You can also read