The ALPHA Project: Establishing consensus and prioritisation of global community recommendations to address major challenges in lupus diagnosis ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Epidemiology and outcomes
Lupus Sci Med: first published as 10.1136/lupus-2020-000433 on 9 February 2021. Downloaded from http://lupus.bmj.com/ on December 28, 2021 by guest. Protected by copyright.
The ALPHA Project: Establishing
consensus and prioritisation of global
community recommendations to address
major challenges in lupus diagnosis,
care, treatment and research
Karin Tse ,1 Sanjyot Sangodkar,2 Lauren Bloch,2 Kathleen Arntsen,3
Sang-Cheol Bae,4 Ian N Bruce,5,6 Erin Connolly-Strong,7 Karen H Costenbader,8
Bradley Dickerson,9 Thomas Dörner ,10 Sydney Evans,11 Kenneth Kalunian,12
Amy H Kao,13 Susan Manzi,14 Eric F Morand,15 Sandra C Raymond ,1
Brad H Rovin,16 Laura Eve Schanberg,17 Joan M Von Feldt,18 Victoria P Werth,19,20
Angel Williams Derricott,21 David Zook,2 Timothy Franson,22 Kenneth Getz,23
Yaritza Peña,23 Leslie M Hanrahan,1 On behalf of the ALPHA Project Global
Advisory Committee
To cite: Tse K, Sangodkar S, ABSTRACT
Bloch L, et al. The ALPHA The Addressing Lupus Pillars for Health Advancement
Key messages
Project: Establishing consensus (ALPHA) Project is a global consensus effort to
and prioritisation of global What is already known about this subject?
identify, prioritise and address top barriers in lupus
community recommendations ►► Lupus is a complex, heterogeneous autoimmune
impacting diagnosis, care, treatment and research.
to address major challenges disease in which outcomes vary widely across the
in lupus diagnosis, care, To conduct this process, the ALPHA Project convened
globe, with lengthy time to diagnosis, limited treat-
treatment and research. a multistakeholder Global Advisory Committee (GAC)
of lupus experts and collected input from global ment options and recognised health disparities.
Lupus Science & Medicine
►► The Addressing Lupus Pillars for Health Advancement
2021;8:e000433. doi:10.1136/ audiences, including patients. In phase I, the ALPHA
Project used expert interviews and a global survey of (ALPHA) Project is a multiphase, global consensus
lupus-2020-000433
lupus experts to identify and categorise barriers into effort that has thoughtfully engaged global lupus
three overarching pillars: drug development, clinical experts, including clinicians, researchers, industry
►► Additional material is
care and access to care. In phase II, reported here, the representatives, advocacy organisations and peo-
published online only. To view,
GAC developed recommended actionable solutions to ple with lupus to identify and prioritise key barriers
please visit the journal online
address these previously identified barriers through an spanning drug development, clinical care and access
(http://dx.doi.org/10.1136/
lupus-2020-000433). in-person stakeholder meeting, followed by a two-round to care.
scoring process. Recommendations were assessed What does this study add?
for feasibility, impact and timeline for implementation ►► The ALPHA Global Advisory Committee convened to
Received 10 August 2020 (FIT), where potential FIT component values were develop strategies and recommendations to address
Revised 28 January 2021 between 1 and 3 and total scores were between 3 and
Accepted 29 January 2021 prior outlined barriers, including simplifying and
9. Higher scores represented higher achievability based standardising outcome measures, including steroid
on the composite of the three criteria. Simplifying and sparing; defining the lupus spectrum; increasing
standardising outcomes measures, including steroid understanding of social determinants of health and
sparing as an outcome (drug development) and defining contributors to health disparities; and assessing and
the lupus spectrum (clinical care) ranked as the highest identifying gaps of current biomarker development
two priority solutions during the GAC meeting and
and data sharing activities.
received high FIT scores (7.67 and 7.44, respectively).
© Author(s) (or their Leveraging social media (access to care) received the
employer(s)) 2021. Re-use highest FIT score across all pillars (7.86). Cross-cutting
permitted under CC BY-NC. No INTRODUCTION
themes of many solutions include leveraging digital
commercial re-use. See rights Background
technology and applying specific considerations for
and permissions. Published by
special populations, including paediatrics. Implementing Systemic Lupus Erythematos (SLE, or lupus)
BMJ. is a complex, heterogeneous autoimmune
the recommendations to address key barriers to
For numbered affiliations see disease with enormous multisystem impact.
drug development, clinical care and access to care is
end of article.
essential to improving the quality of life of adults and Despite considerable variability in outcomes,
Correspondence to children with lupus. Multistakeholder collaboration and people with lupus have an overall increased
Karin Tse; karinstse@gmail.com guidance across existing efforts globally is warranted. risk of death. While lupus impacts people of all
Tse K, et al. Lupus Science & Medicine 2021;8:e000433. doi:10.1136/lupus-2020-000433 1Lupus Science & Medicine
Lupus Sci Med: first published as 10.1136/lupus-2020-000433 on 9 February 2021. Downloaded from http://lupus.bmj.com/ on December 28, 2021 by guest. Protected by copyright.
source of concern for patients and healthcare providers.
Key messages In paediatric patients, drug metabolism differences,
How might this impact clinical practice? puberty and linear growth, and ongoing brain develop-
►► Large-
scale, coordinated efforts to develop and implement rec- ment are important factors that influence therapy devel-
ommendations from the ALPHA Project across global stakeholder opment and drug safety.
groups have the potential to improve outcomes for people with lu-
pus by reducing time to diagnosis, increasing availability of safe and The Addressing Lupus Pillars for Health Advancement (ALPHA)
effective treatment options, and improving access to care. Project
The ALPHA Project is a landmark initiative to identify,
prioritise and implement global strategies to address
ages and races, young age at onset, non-European ancestry the most pressing challenges that limit progress in
and lower socioeconomic status are risk factors for poorer lupus outcomes. ALPHA brings together lupus experts
outcomes. Minority racial/ethnic groups, including people from around the globe—including patients—to identify
of African ancestry, Hispanics and Asians have a significantly barriers impacting drug development, clinical care and
higher risk of death due to lupus. Geographical differences, access to care, along with actionable solutions to address
poverty, education levels and insurance status also nega- each barrier. Phase I, during which these barriers were
tively impact lupus mortality.1 2 Not surprisingly, numerous identified, was completed in 2019.9 As described in this
healthcare access issues persist, including access to specialty article, the goals of phase II were to confirm the barriers,
care and institutions skilled in treating lupus.3 4 These reali- identify and reach consensus on actionable solutions to
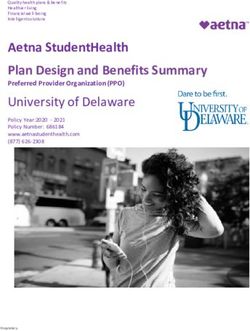
ties contribute to significant unmet needs in care. each barrier, and determine preliminary steps to imple-
In contrast to other autoimmune diseases such as rheu- ment these solutions. Figure 1 summarises the phases of
matoid arthritis and psoriasis, there are few approved medi- the ALPHA Project.
cations for lupus. Persistent challenges to understanding
disease biology, defining clinical trial inclusion criteria and
endpoints, developing instruments to measure changes in ALPHA Project leadership
clinical activity and controlling background medications The ALPHA Project is led by the Lupus Foundation of
have posed as long-standing barriers in lupus drug devel- America (LFA) in collaboration with the Tufts Univer-
opment.5 Many promising therapeutic agents have failed to sity School of Medicine Center for the Study of Drug
demonstrate efficacy over standard of care, and there are Development and a Global Advisory Committee (GAC)
few trials that have focused on or included paediatric popu- of lupus experts. The GAC, composed of the publica-
lations. At the same time, over 30 companies are currently tion authors and listed in online supplemental file 1, is
investing in lupus clinical trials.6 a diverse group of lupus patient advocates, clinicians,
Another pressing consideration in lupus drug devel- academic researchers and biopharmaceutical industry
opment is safety. Current treatments used for lupus, representatives across five countries.
including glucocorticoids and immunosuppressive treat-
ments, are associated with significant toxicity and poor ALPHA Project phase I summary
long-term outcomes.7 8 Many patients with lupus are As described in Manzi et al, phase I of the ALPHA Project
treated with combination therapies and take numerous examined barriers to lupus diagnosis, care, treatment
concomitant medications, making drug interactions a and research, and how these barriers impact the quality
Figure 1 ALPHA Project phases.
2 Tse K, et al. Lupus Science & Medicine 2021;8:e000433. doi:10.1136/lupus-2020-000433Epidemiology and outcomes
Lupus Sci Med: first published as 10.1136/lupus-2020-000433 on 9 February 2021. Downloaded from http://lupus.bmj.com/ on December 28, 2021 by guest. Protected by copyright.
Table 1 Top three barriers in each pillar identified in phase I
Drug development Clinical care Access to care
Lack of biomarkers to predict Lack of diagnostic, predictive and Less effective management of lupus due to
response to drug in clinical trials prognostic biomarkers for lupus social determinants of health in predominantly
lower socioeconomic status areas
Lack of user-friendly, sensitive and Lack of treatment adherence Lack of patient access to clinical lupus experts
accurate outcome measures
Suboptimal clinical trial design and Limited awareness and understanding Lack of access to medications either due to
outcome measures for patients across of lupus among non-expert medical lack of coverage or added cost to patients
age groups professionals
of life of people with lupus. The GAC, consisting of 13 Defining success states
thought leaders in phase I, identified a preliminary list The three pillars and associated barriers identified in
of barriers through a mixed- methods approach that phase I provided a framework to generate actionable solu-
included structured interviews and a global survey. Repre- tions in phase II. To begin this process, GAC members
sentatives from the Tufts University School of Medicine completed a questionnaire (included in online supple-
Center for the Study of Drug Development interviewed 4 mental file 2) to provide brief and specific descriptions
GAC members and 13 additional non-GAC lupus experts of a high-level ‘future success state’ to be achieved for
comprising clinicians, clinical investigators, patient advo- each pillar by addressing the related barriers. The GAC
cates, government representatives and people with lupus members’ responses were then consolidated into the
to further characterise the barriers initially outlined by descriptions of success states included in table 2.
the GAC. The top barriers identified by interviewees were These definitions of a ‘success state’ were highly consis-
categorised into three pillars: (1) drug development, (2) tent with those collected during the in-depth interviews
clinical care and (3) access to care. performed in phase I. A comparison of the barriers,
Findings from the expert interviews informed the pillars and definitions of success showed alignment
development of an online survey distributed to a diverse, around several key themes: (1) disease heterogeneity,
international stakeholder audience to achieve broad (2) need for improved diagnostic tools, (3) limitations of
consensus on the barriers as well as prioritisation. The current therapies, (4) need for broader physician educa-
study validated known challenges in lupus, identifying tion, (5) lack of treatment or trial protocol adherence
the following top barriers to improving lupus outcomes and (6) rising treatment costs.
(table 1).
Patient survey
ALPHA PROJECT PHASE II To further validate barriers identified by the GAC and to
Goal and activities ensure representation of the patient voice, the ALPHA
The goal of phase II was to develop and prioritise proposed team developed and administered a 23-question global
actionable solutions that directly address barriers iden- online patient and caregiver survey on the top priorities
tified in phase I across lupus drug development, clin- in lupus care and research. The survey questions focused
ical care and access to care. Phase II activities included on three key themes to align with the three lupus pillars:
ensuring alignment of priorities with the patient commu- research participation (aligning with the drug develop-
nity through development, dissemination and analysis of ment pillar), lupus diagnosis (aligning with the clinical
a global online patient survey and further engagement of care pillar), and managing and accessing lupus care
the GAC to develop specific recommendations for next (aligning with the clinical care and access to care pillars).
steps to implement the identified solutions. The survey was administered between 16 November 2019
Table 2 Success states by pillar identified by Global Advisory Committee members in phase II
Drug development Clinical care Access to care
Improved trial design across age groups Biomarkers to support timely and Access to high quality, specialised care
accurate diagnosis regardless of location
Improved outcome measures to be Improved support programmes to Improved access to care for individuals of
uniformly implemented across sponsors encourage treatment adherence lower socioeconomic status
among patients
Improved biomarkers to better define Biomarkers to predict patients’ Improved global access to advanced
heterogeneity and predict response to responses to therapies to support diagnostics and therapies
investigational therapies design of treatment regimens
Tse K, et al. Lupus Science & Medicine 2021;8:e000433. doi:10.1136/lupus-2020-000433 3Lupus Science & Medicine
Lupus Sci Med: first published as 10.1136/lupus-2020-000433 on 9 February 2021. Downloaded from http://lupus.bmj.com/ on December 28, 2021 by guest. Protected by copyright.
and 8 December 2019 and disseminated via email by the Tufts Center for the Study of Drug Development, staff of
LFA and the World Lupus Federation in English, Spanish, the LFA and members of Faegre Drinker Consulting, who
Korean and simplified Chinese. led the phase II strategy and facilitated the meeting.
A total of 3233 people completed the survey and 214 Attendees began the meeting by reviewing and
completed at least 68% of the survey. Partial responses confirming the success states developed based on their
at this cut-off level had complete answers across all three responses to the premeeting questionnaire. The meeting
pillars and were missing only demographic responses, then followed the same set of steps for each of the three
and thus were included in the analysis. Survey respon- pillars:
dents included 3330 individuals with lupus and 117 ►► Review of the patient survey data related to that pillar.
caregivers of children or teenagers under the age of 18 ►► Breakout session group activities (three groups,
years with lupus. Respondents from 83 countries partic- including at least one of the following meeting partic-
ipated in the survey. Respondents represented a broad ipant types per group: clinician–researcher, biophar-
range of lupus manifestations, races/ethnicities, coun- maceutical industry, patient advocate and person with
tries and ages. They self-identified as either White (57%), lupus):
Hispanic/Latino (18%), Black or African–American –– Identify at least one action to achieve each success
(14%), or Asian (10%). Additional information on the state.
survey respondents is included in online supplemental –– Vote on the highest-priority solutions.
file 3. –– Present the breakout group’s proposed highest-
Of the total respondents, most identified as having priority solutions to all meeting participants.
either SLE without nephritis (66%) or SLE with nephritis ►► Vote by all meeting participants on the consolidated
(25%). Fifty- nine per cent of respondents reported set of proposed solutions identified by each breakout
receiving a lupus diagnosis within a year of discussing group, followed by full- group voting on overall
symptoms with their doctor. Approximately 60% of highest-priority solutions.
respondents reported being misdiagnosed before The structured sessions produced consensus lists of
receiving a lupus diagnosis, with depression and anxiety solutions for each of the three pillars as shown in table 3.
the most common misdiagnoses (reported by 20% and
19%, respectively). Feasibility, impact and timeline for implementation (FIT)
The top reported challenges experienced by people scoring of solutions
with lupus were managing medication side effects (43%) Following the in-person meeting, GAC members were
and lack of treatment options to relieve symptoms (30%), asked to assess the priority solutions within each pillar
indicating the priority for new safe and effective treat- by rating each item for its feasibility, impact and timeline
ments. Additionally, difficulty affording care or treatment for implementation (FIT) using a detailed scoring guide
due to high out-of-pocket costs was also listed as a top (online supplemental file 4). This scoring process draws
concern by 27% of respondents. on project management tools such as the Project Manage-
Only a relatively small portion of respondents (23%) ment Institute’s Matrix for the Evaluation of Strategic
had participated in research, including clinical trials, and Alternatives, which facilitates group decision-making by
most of these individuals learnt of research opportunities assessing different factors that contribute to a solution’s
through their doctors (49%). Those who reported not achievability. Individual FIT components had potential
participating in research cited not being asked by their values between 1 and 3, and each solution could receive
doctor (41%) as the top reason for not participating. a total composite score between 3 and 9. Higher scores
Eighty-eight per cent of respondents indicated that, at the represent an overall higher achievability based on the
time of the survey, they currently saw a rheumatologist for composite of the three FIT components.
lupus, and less than half of respondents (44%) reported The LFA programmed the FIT scoring question-
disease management by a primary care physician. A lack naire through Qualtrics survey software and asked GAC
of education and awareness about clinical trials, including members to participate in two scoring rounds. Drawing
addressing concerns about benefits and risks of partici- from the Delphi method and to better drive consensus,
pation, was reported as barriers by 33% of respondents. the LFA shared the anonymised scores from the first
Access and eligibility were also noted as important factors round with GAC members prior to asking them to
to be considered in trial design. Insights from the global complete the second round of scoring. The total scores
patient survey supported themes identified from lupus from round 1 and round 2 of the FIT scoring exercises
experts around top barriers. are presented in table 4.
Four solutions, at least one for each pillar, received FIT
GAC meeting scores notably higher than the others after the second
The GAC held an in-person meeting on 15–16 January round (all scoring greater than 7.00):
2020 in Washington, DC, to identify actionable solutions 1. Access to care: leverage social media (7.78).
to achieve the success states outlined for drug develop- 2. Drug development: simplify and standardise clinical
ment, clinical care and access to care. Meeting attendees trial outcome measures, including steroid-sparing as
included 18 GAC members, representatives from the an outcome (7.67).
4 Tse K, et al. Lupus Science & Medicine 2021;8:e000433. doi:10.1136/lupus-2020-000433Epidemiology and outcomes
Lupus Sci Med: first published as 10.1136/lupus-2020-000433 on 9 February 2021. Downloaded from http://lupus.bmj.com/ on December 28, 2021 by guest. Protected by copyright.
Table 3 Ranked solutions per pillar identified by Global Advisory Committee
Drug development Clinical care Access to care
1. Simplify and standardise clinical trial 1. Define the lupus spectrum. 1. Build the case for World Health
outcome measures, including steroid- 2. Perform longitudinal studies Organisation (WHO) prioritisation of
sparing as an outcome. of prognostic and diagnostic lupus.
2. Develop data sharing approaches biomarkers. 2. Develop standardised and specialised,
related to biomarkers, clinical data and 3. Drive clinical and lab-based expert-driven care pathways.
lab samples. measures for individualised 3. Drive telehealth advances and
3. Propel quality of life-driven studies (eg, treatments. reimbursement, and build on current
fatigue). 4. Identify and support development of infrastructures.
4. Increase participant representativeness treatment adherence strategies that 4. Explore broader partnering.
in clinical trials (e.g., minority, work for lupus and communicate 5. Leverage social media.
paediatric and cutaneous lupus them to patients and providers. 6. Develop evidence base for
erythematosus). interventions, including standardised
endpoints/outcomes.
7. Provide payor education and establish
alignment.
3. Clinical care: define the lupus spectrum (7.44). clinical trial designs, and a lack of validated biomarkers
4. Clinical care: identify and support the development of mean many outcome measures may have limitations
adherence strategies for patients with lupus and com- for regulatory decision-making. For example, the diver-
municate them to patients, caregivers and providers sity of lupus manifestations means that two individuals
(7.22). with active disease may have non-overlapping manifes-
The GAC members showed a clear consensus on the tations, possibly not adequately captured by available
solutions for the clinical care and drug development activity scores. Addressing such variation using a single
pillars both by voting during the GAC meeting and the outcome measure therefore presents a significant chal-
FIT scoring. They ranked ‘defining the lupus spectrum’ lenge. Simplifying and standardising outcome measures
(clinical care) and ‘simplifying and standardising clinical could minimise confusion about which measures to use,
trial outcomes measures, including steroid-sparing as an allow comparisons between trials, and provide a diverse
outcome’ (drug development) as the highest- priority set of measures to evaluate the success of interventions
solutions during the meeting and FIT scoring. However, for the various types of lupus and across adults and chil-
prioritisation of solutions within the access to care pillar dren with this condition. Additionally, steroid- sparing,
differed from the in-person meeting and FIT scoring. which is often used as a secondary endpoint in clinical
‘Building a case for World Health Organization (WHO) trials, has been shown in large cohort studies to be a clin-
prioritisation’ was ranked the highest priority during the ically meaningful outcome important in all age groups to
GAC meeting, but that solution received the lowest FIT prevent long-term organ damage.
score. At the same time, the GAC members gave ‘lever-
aging social media’ the highest FIT score within the access Next steps
to care pillar and among all three pillars, but ranked it as GAC members will publish an update on the current
a low priority during the GAC meeting. lupus outcome measures and issue a declarative
consensus statement on steroid- sparing, emphasising
DISCUSSION AND NEXT STEPS that steroid tapering in practice should be the goal and
After completing two rounds of FIT scoring, the GAC should be used as a secondary endpoint in clinical trials
members and the patient representatives convened virtu- to help achieve that goal. By crystallising current thinking
ally on 20 May 2020 and 17 June 2020 to provide input and expanding the evidence base on outcome measures,
on the next steps to implement the top-priority solutions. including steroid-sparing, GAC members provide an
opportunity for the US Food and Drug Administration
Drug development and other regulatory organisations to enhance the drug
The GAC members and patient representatives ranked development process by modifying currently accepted
‘simplifying and standardising clinical trial outcome outcome measures.
measures, including steroid-sparing as an outcome’ as the
highest-priority solution for the drug development pillar Clinical care
during the GAC meeting and the FIT scoring process. The GAC members and patient representatives ranked
During the in-person meeting, participants agreed that defining the lupus spectrum as their highest priority for
current trial outcome measures have many limitations. the clinical care pillar during the GAC meeting and the
The heterogeneity of lupus, the wide age spectrum of FIT scoring. In phase I, the GAC began to explore concep-
affected individuals, including children, suboptimal tualising lupus as a spectrum, or umbrella, of related
Tse K, et al. Lupus Science & Medicine 2021;8:e000433. doi:10.1136/lupus-2020-000433 5Lupus Science & Medicine
Lupus Sci Med: first published as 10.1136/lupus-2020-000433 on 9 February 2021. Downloaded from http://lupus.bmj.com/ on December 28, 2021 by guest. Protected by copyright.
science also characterises lupus as a systemic spectrum
Table 4 Total FIT scores
disorder, rather than as multiple single-organ diseases.13
Total However, misuse of the current classification criteria as
Consensus item Round 1 Round 2 diagnostic criteria has become a norm in routine prac-
Drug development tice. Therefore, development of broader diagnostic
Simplify and standardise clinical 7.28 7.67 criteria better suited for clinical use across the full ‘lupus
trial outcome measures, including spectrum’ is warranted.
steroid-sparing as an outcome.
Increase participant 6.67 6.56 Next steps
representativeness in clinical trials GAC members will lead the development of a consensus
(e.g., minority, paediatric and effort to define lupus that builds on current research
cutaneous lupus erythematosus). definitions and includes closely related IMIDs and,
Propel quality of life-driven 6.39 6.56 for example, cutaneous variants. After establishing a
studies (e.g., fatigue). consensus definition, GAC members will work with other
Develop data sharing approaches 6.00 6.06 stakeholders in the global lupus community to dissemi-
related to biomarkers, clinical nate the definition through publication and broader
data and lab samples. discussion.
Clinical care
Access to care
Define the lupus spectrum. 6.94 7.44
Although GAC members and the patient representa-
Identify and support development 7.17 7.22 tives ranked leveraging social media as a lower priority
of adherence strategies that work during the in-person meeting, they gave it the highest FIT
for lupus and communicate them
score within the access to care pillar and overall. Many
to patients and providers.
people with lupus already use social media such as Face-
Drive clinical and lab-based 6.06 5.89 book, Twitter, online communities, blogs, Instagram and
measures for individualised
YouTube to access information and support for managing
treatments.
their disease.14 Social media tools are fast, widely used,
Perform longitudinal studies 6.17 5.50 accessible and low-cost options that can be optimised for
of prognostic and diagnostic
broad outreach. By leveraging social media tools, lupus
biomarkers.
providers, advocacy organisations, researchers and other
Access to care stakeholders can increase interaction with the lupus
Leverage social media. 7.94 7.78 patient community to enable opportunities for individ-
Explore broader partnering. 6.71 6.89 uals to access research opportunities, educational and
Provide payor education and 6.35 6.44 self-management resources, and social support.
establish alignment. During the in- person meeting, meeting participants
Develop standardised and 6.28 6.44
ranked ‘identifying and supporting the development
specialised, expert-driven care of successful treatment adherence strategies for people
pathways. with lupus and communicating them to patients and
Develop evidence base 6.36 6.00
providers’ as a low priority, but this solution received the
for interventions, including second highest FIT score within the access to care pillar.
standardised endpoints/ Treating lupus is a lifelong process that requires ongoing
outcomes. planning and communication. It is important to apply
Drive telehealth advances and 6.22 6.00 the findings from existing literature about support strat-
reimbursement, and build on egies, treatment adherence and non-adherence in lupus
current infrastructures. to everyday practice. This is especially important among
Build the case for World Health 5.52 5.11 populations with more limited access to care and who are
Organization (WHO) prioritisation. more likely to be non-adherent.
GAC members and the patient representatives ranked
The solutions are listed in order of highest to lowest Round 2 FIT
score within each pillar.
building a case for the WHO prioritisation as the highest-
FIT, feasibility, impact and timeline for implementation. priority solution within the access to care pillar during
the in-person meeting, but this solution had the lowest
overall FIT score. Engaging with the WHO could pave the
disorders across immune-mediated inflammatory disor- way for globally recognised lupus standards, guidance and
ders (IMIDs) (e.g., rheumatoid arthritis, antiphospho- best practices, with substantial and far-reaching effects on
lipid syndrome, Sjögren’s syndrome), as well as ranging access to care. However, the potential logistical difficul-
from cutaneous lupus through systemic disease. Lupus ties of engaging with the WHO may make other solutions
may coexist with and often presents with clinical features to improve access to care more achievable, especially in
similar to other autoimmune diseases.10–12 Emerging the next 1–5 years.
6 Tse K, et al. Lupus Science & Medicine 2021;8:e000433. doi:10.1136/lupus-2020-000433Epidemiology and outcomes
Lupus Sci Med: first published as 10.1136/lupus-2020-000433 on 9 February 2021. Downloaded from http://lupus.bmj.com/ on December 28, 2021 by guest. Protected by copyright.
Next steps increase awareness and involvement with ALPHA efforts
The GAC members agreed that the set of access to care to increase adoption of implementation plans.
solutions needs to be refined prior to defining specific Lupus is a major public health challenge and the
next steps. GAC members will lead an effort to (1) gain ALPHA Project represents the first global initiative to
a better understanding of social determinants of health transform outcomes across the entire continuum of drug
and contributors to health disparities by examining how development, clinical care and access to care by bringing
current tools, such as the LFA registry,15 can help capture scientific leaders and the lupus patient community
the patient experience for regulatory and coverage together. Implementation of each solution will require
purposes, as well as disparities interventions, and (2) substantial resources and a coordinated series of activi-
explore the unique access to care issues faced by paedi- ties across stakeholders. Such a global concerted effort
atric patients. that includes a strong patient voice alongside clinicians,
academics and industry partners will be essential for its
Cross-pillar initiative success.
The GAC also noted that identifying and validating
biomarkers could help to address overlapping barriers to Author affiliations
1
both drug development and clinical care. While recom- Research, Lupus Foundation of America Inc, Washington, District of Columbia, USA
2
Faegre Drinker Consulting, Faegre Drinker Biddle and Reath LLP, Washington, DC,
mendations related to biomarkers received low FIT USA
scores, largely due to the longer timelines for implemen- 3
Lupus and Allied Diseases Association, Inc, Verona, New York, USA
tation, this work would still make an important impact. 4
Rheumatology, Hanyang University Seoul Hospital, Seongdong-gu, Seoul, South
Biomarkers may provide better targets for drug develop- Korea
5
ment efforts and aid clinicians with diagnosis, monitoring NIHR Manchester Biomedical Research Centre, Manchester, UK
6
Musculoskeletal and Dermatological Sciences, The University of Manchester,
disease activity and determining an appropriate care Manchester, UK
regimen for patients. 7
Autoimmune and Rare Disease Division, Mallinckrodt Pharmaceuticals Specialty
Brands, Bedminster, New Jersey, USA
8
Next steps Medicine, Brigham and Women's Hospital, Boston, Massachusetts, USA
9
The GAC will lead an assessment of current biomarker Aurinia Pharmaceuticals Inc, Victoria, British Columbia, Canada
10
Rheumatology and Clinical Immunology, Charite University Hospital Berlin, Berlin,
development and data sharing activities and identify gaps. Germany
This assessment will inform next steps to building stand- 11
Patient Representative, Riverdale, Maryland, USA
ardised global data sharing efforts that link North Amer- 12
Medical Center, University of California San Diego, La Jolla, California, USA
13
ican initiatives with global initiatives, where possible, EMD Serono Research and Development Institute, Billerica, Massachusetts, USA
14
and open the door for international collective research Medicine, Allegheny Health Network, Pittsburgh, Pennsylvania, USA
15
Rheumatology, Monash University, Clayton, Victoria, Australia
collaborations. 16
Internal Medicine/Nephrology, The Ohio State University Wexner Medical Center,
Columbus, Ohio, USA
Cross-cutting themes 17
Pediatrics, Duke University Medical Center, Durham, North Carolina, USA
18
Throughout the in-person meeting discussion, it was clear GlaxoSmithKline USA, Philadelphia, Pennsylvania, USA
19
that leveraging digital technology was an emergent theme Dermatology, University of Pennsylvania, Philadelphia, Pennsylvania, USA
20
Corporal Michael J Crescenz VA Medical Center, Philadelphia, Pennsylvania, USA
in GAC recommendations across the pillars, whether 21
Patient Representative, Richmond, Virginia, USA
for developing data sharing approaches related to 22
Faegre Drinker Consulting, Faegre Drinker Biddle and Reath LLP, Indianapolis,
biomarkers or leveraging telehealth practices to increase Indiana, USA
23
access to care. Additionally, each of these recommenda- Center for the Study of Drug Development, Tufts University School of Medicine,
tions warrants applying specific considerations for special Boston, Massachusetts, USA
populations, including children and teens with lupus,
Twitter Kathleen Arntsen @kathleenarntsen and Ian N Bruce @Lupusdoc
as development and outcomes differ from adult popula-
tions. As lupus affects predominantly diverse people of Acknowledgements The authors thank the Global Advisory Committee members,
the in-person meeting participants, including global collaboration presenter Dr. Tim
colour and of lower socioeconomic status, special consid- Coetzee of the National Multiple Sclerosis Society, and the individuals with lupus
erations for these groups are also needed. and caregivers who participated in the global survey for their leadership in phase II
of the Addressing Lupus Pillars for Health Advancement Project.
Contributors All authors contributed to the discussions and data interpretation
CONCLUSION contained in this paper and provided input on the manuscript and approved its
The ALPHA Project has convened lupus experts across final version. SS, KT and LB contributed to the initial manuscript drafting and
finalisation. KT contributed to patient and feasibility, impact and timeline (FIT)
stakeholder groups, including people with lupus, to iden- scoring survey drafting and finalisation. KT and YP contributed to patient survey
tify, assess, and prioritise concrete solutions to address data analysis. DZ, LB, SS and TF contributed to overall phase II strategies and
barriers in lupus drug development, clinical care and execution, including the critical review of patient survey, moderation of Global
access to care. To begin the next phase of the ALPHA Advisory Committee (GAC) discussions before, during and after the in-person
GAC meeting, and drafting criteria for FIT scoring. LMH oversaw and approved all
Project, the GAC will appoint a task force to develop an research efforts.
implementation plan for the chosen solutions, including
Funding The Addressing Lupus Pillars for Health Advancement Project
selecting teams to carry out the efforts. The ALPHA team was launched in partnership with founding partner EMD Serono Research &
will continue to engage broad stakeholder audiences to Development Institute, Inc. (a business of Merck KGaA, Darmstadt, Germany)
Tse K, et al. Lupus Science & Medicine 2021;8:e000433. doi:10.1136/lupus-2020-000433 7Lupus Science & Medicine
Lupus Sci Med: first published as 10.1136/lupus-2020-000433 on 9 February 2021. Downloaded from http://lupus.bmj.com/ on December 28, 2021 by guest. Protected by copyright.
and through additional support by GlaxoSmithKline. Aurinia Pharmaceuticals and Open access This is an open access article distributed in accordance with the
Mallinckrodt Pharmaceuticals provided additional sponsorship. Creative Commons Attribution Non Commercial (CC BY-NC 4.0) license, which
permits others to distribute, remix, adapt, build upon this work non-commercially,
Competing interests SCR is an employee of the Lupus Foundation of America
and license their derivative works on different terms, provided the original work is
(LFA). SS, LB, TF and DZ are consultants of Faegre Drinker Consulting, a division of
properly cited, appropriate credit is given, any changes made indicated, and the use
Faegre Drinker Biddle & Reath, a law and consulting firm that represents patient
is non-commercial. See: http://creativecommons.org/licenses/by-nc/4.0/.
advocacy organisations and sponsors developing drugs. INB receives grant/
research support from Genzyme Sanofi, GSK and UCB; is a consultant of Eli Lilly, ORCID iDs
AstraZeneca, UCB, Iltoo and Merck Serono; and affiliated with speakers bureaus Karin Tse http://orcid.org/0000-0003-4992-8590
for UCB and AstraZeneca. EC-S is an employee of Mallinckrodt (former). KHC Thomas Dörner http://orcid.org/0000-0002-6478-7725
receives grant/research support from Merck and is a consultant of AstraZeneca. Sandra C Raymond http://orcid.org/0000-0003-1778-8095
BD is an employee of Aurinia (former). TD receives grant/research support from
Janssen, Novartis, Roche and UCB; is a consultant of Abbvie, Celgene, Eli Lilly,
Roche, Janssen and EMD; and affiliated with speakers bureaus for Eli Lilly, Roche,
Samsung and Janssen. KK receives grant/research support from UCB, Novartis and
Resolve; and is a consultant of AstraZeneca, Viela Bio, Genentech/Roche, Biogen,
Iltoo, GSK, BMS, Janssen, Abbvie, Amgen, Eli Lilly, Kyowa Kirin, Equillium Bio and REFERENCES
Celgene. AHK is an employee of EMD Serono. EFM receives grant/research support 1 Singh RR, Yen EY. Sle mortality remains disproportionately high,
from AstraZeneca, BMS, Eli Lilly, GSK, Janssen and Merck-Serono; is a consultant despite improvements over the last decade. Lupus 2018;27:1577–81.
of AbbVie, Amgen, AstraZeneca, Biogen, BMS, Eli Lilly, GSK, Janssen, Neovacs and 2 Carter EE, Barr SG, Clarke AE. The global burden of SLE: prevalence,
Sandoz; and is affiliated with speaker bureaus for AstraZeneca and Novartis. BHR is health disparities and socioeconomic impact. Nat Rev Rheumatol
a consultant for GSK, Aurinia, AstraZeneca, Novartis, Alexion and BMS. LES receives 2016;12:605–20.
grant/research support from Sobi, BMS, CARRA Inc.; is a consultant of Aurinia, UCB 3 Gillis JZ, Yazdany J, Trupin L, et al. Medicaid and access to care
among persons with systemic lupus erythematosus. Arthritis Rheum
(DSMB), Sanofi (DSMB) and Sobi. VPW receives grant/research support from Biogen, 2007;57:601–7.
Celgene, Gilead, Janssen and Viela; and is a consultant of Biogen, Gilead, Janssen, 4 Demas KL, Costenbader KH. Disparities in lupus care and outcomes.
Abbvie, GSK, Resolve, AstraZeneca, Amgen, Eli Lilly, EMD Serono, BMS, Viela and Curr Opin Rheumatol 2009;21:102–9.
Kyowa Kirin. JMVF is a shareholder and employee of GSK (former). KT and LMH are 5 The Lewin Group Inc. Overcoming barriers to drug development
employees of the LFA (former). SE and AWD are LFA patient ambassadors. in lupus, 2009. Available: https://www.lupus.org/s3fs-public/
documents/Overcoming_Barriers_to_Drug_Development_in_Lupus.
Patient and public involvement statement Lupus patient representatives pdf
and advocacy organisation representatives have been included in all steps of 6 Clinicaltrials.Gov, 2019. Available: https://clinicaltrials.gov/ [Accessed
the Addressing Lupus Pillars for Health Advancement Project, including serving 21 Feb 2019].
on the Global Advisory Committee (GAC). Results from a patient survey, which 7 Apostolopoulos D, Morand EF. It hasn't gone away: the problem of
was developed with the GAC and distributed by patient advocacy and support glucocorticoid use in lupus remains. Rheumatology 2017;56:i114–22.
groups to over 3000 people with lupus and caregivers, informed discussion of 8 Tian J, Luo Y, Wu H, et al. Risk of adverse events from different drugs
for SLE: a systematic review and network meta-analysis. Lupus Sci
recommendations during the in-person meeting. Patient representatives were
Med 2018;5:e000253.
involved in the in-person meeting, actively participating in discussion, selection of 9 Manzi S, Raymond S, Tse K, et al. Global consensus building and
top action items, subsequent feasibility, impact and timeline scoring activities and prioritisation of fundamental lupus challenges: the ALPHA project.
GAC calls, and providing critical review of this publication. Lupus Sci Med 2019;6:e000342.
Patient consent for publication Not required. 10 Lockshin MD, Levine AB, Erkan D. Patients with overlap autoimmune
Ethics approval The Advarra Institutional Review Board (IRB) determined the disease differ from those with 'pure' disease. Lupus Sci Med
2015;2:e000084.
Addressing Lupus Pillars for Health Advancement patient survey to be exempt from 11 Lorber M, Gershwin ME, Shoenfeld Y. The coexistence of
IRB oversight. systemic lupus erythematosus with other autoimmune diseases:
Provenance and peer review Not commissioned; externally peer reviewed. the kaleidoscope of autoimmunity. Semin Arthritis Rheum
Data availability statement Data are available upon reasonable request. 1994;24:105–13.
12 Jury EC, D'Cruz D, Morrow WJ. Autoantibodies and overlap
Supplemental material This content has been supplied by the author(s). It has syndromes in autoimmune rheumatic disease. J Clin Pathol
not been vetted by BMJ Publishing Group Limited (BMJ) and may not have been 2001;54:340–7.
peer-reviewed. Any opinions or recommendations discussed are solely those 13 Merrill JT. Connective tissue diseases: is SLE many single-organ
of the author(s) and are not endorsed by BMJ. BMJ disclaims all liability and diseases or an overlapping spectrum? Nat Rev Rheumatol
2015;11:385-6.
responsibility arising from any reliance placed on the content. Where the content
14 Wheeler LM, Pakozdi A, Rajakariar R, et al. 139 Moving with the
includes any translated material, BMJ does not warrant the accuracy and reliability times: social media use amongst lupus patients. Rheumatology
of the translations (including but not limited to local regulations, clinical guidelines, 2018;57.
terminology, drug names and drug dosages), and is not responsible for any error 15 Lupus Foundation of America. Research Accelerated by You (RAY).
and/or omissions arising from translation and adaptation or otherwise. Available: https://www.lupus.org/research/enroll-in-a-lupus-registry
8 Tse K, et al. Lupus Science & Medicine 2021;8:e000433. doi:10.1136/lupus-2020-000433You can also read