THE 2021 LIBBY HARRICKS MEMORIAL ORATION
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
THE 2021 LIBBY HARRICKS
MEMORIAL ORATION
Clinical Professor Harvey Coates AO,
DM, MS, FRCS(C) FRACS
Indigenous Ear and Hearing Health
---Tackling the silent epidemic
Introduction
Thank you to Deafness Forum and to Audiology Australia for the
honour of being invited to give the Libby Harricks Memorial Oration
on a subject that I’m passionate about. Firstly, I should like to
acknowledge the Whadjuk Noongar land upon which we meet and the
elders, past, present and emerging.
The exceptional Libby Harricks, who, in spite of progressive hearing
loss, accomplished so much in her advocacy for deaf and hearing
impaired people, brings to mind Nelson Mandela’s statement.
“ What counts in life is not the mere fact that we have lived. It is what
difference we have made to the lives of others that will determine the
significance of the life we lead.”
1
In this Oration I will discuss the problem of Indigenous ear disease
around the world, why it is a silent epidemic, the causes and effects of
middle ear disease, its treatment, and culminating in how we can, in
the 2020’s, close the gap in ear and hearing health.
My distinguished friend and colleague, Professor Andrew Smith who
gave this address two years ago emphasised, from his years leading
the ear health strategies at the World Health Organisation, the critical
role that Public Health initiatives have in detecting, preventing and
treating those causes of deafness and hearing loss.
In the WHO-UNICEF-Lancet Commission on ‘A future for the world’s
children’, chaired by former New Zealand Prime Minister Helen Clark
and published in 2020, the multiple threats of climate change,
ecological degradation, migrating populations, conflict, pervasive
inequalities and predatory commercial practices to health and the
future of all children were outlined.(1) They noted childhood is the
ideal time to intervene as, though it’s a time of vulnerability, it’s also
a time of opportunity. Intervening in childhood has lifelong,
intergenerational benefits. Consider that brain plasticity and
neurogenesis are at their peak, at the critical time for cognitive and
psychosocial skill development. And so it is that in the last decade,
recognition of hearing loss has finally been acknowledged, with
hearing loss increasing from 11th leading cause of years living with
disability (YLD) in 2010 to the 4th leading cause in 2015, ahead of
headline grabbing conditions like diabetes and dementia.(2)
2
Apart from the lancet articles, the World Health Assembly (WHA)
ratified a 2017 “Resolution and action plan for prevention of deafness
and hearing loss’, and a 2019 WHO and the International
Telecommunication Union developed standards for noise exposure
from devices to protect the young and adolescents from noise induced
hearing loss. In Australia Minister Ken Wyatt unveiled a seven year
‘Roadmap for ear and hearing health.’
Half a billion people have disabling hearing loss-7% of the world’s
population, while 1.34 billion have a mild-moderate hearing loss.
32 million children have this all too often overlooked ‘invisible
disability’, especially those in low and middle income nations.
Indigenous populations in particular carry much of the burden,
especially in Asia, the South Pacific and uniquely.
In first world countries such as USA, Canada and Australia. It is the
Indigenous child with hearing loss that we address today.
3
GLOBAL INDIGENOUS EAR HEALTH
Indigenous peoples, also known in some regions as First peoples, First
Nations, Aboriginal peoples or Native peoples are ethnic groups who
are the original or earliest known inhabitants of an area, in contrast to
groups that have settled, occupied or colonised the area more
recently. Indigenous societies inhabit every climate zone and
continent except Antarctica. For the purposes of this talk, Aboriginal
relates to Aboriginal and Torres Strait Islander peoples, the main focus
of my research into chronic middle ear diseases.
As illustrated in Figure 1, the world map of Indigenous peoples
displays the multitude of communities, with an estimated total
population of 350 million people.
Those countries and First Nation peoples where the prevalence,
microbiology and aetiological or causative data of ear health and
hearing loss in their Indigenous population has been well documented
are the Australian Aboriginal, the New Zealand Maori, North American
and Greenland Inuits and Native Americans. In addition to first world
countries with high prevalence of chronic ear disease ( particularly
chronic suppurative otitis media -CSOM or ‘runny‘ ear ) in their
Indigenous population, Tanzania, India, Guam and the Solomon
Islands have prevalence rates of greater than 4%.
( Table 1)
4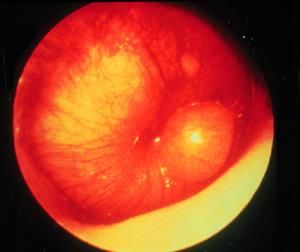
This Photo by Unknown Author is licensed under CC BY-SA
Figure 1. Ethnic Global Groups by the end of the 20th Century
The WHO informs us that 60% of the world’s hearing loss is
preventable especially permanent or sensori-neural hearing loss due
to noise exposure, ototoxic drugs, toxic chemicals and vaccine
preventable diseases as well as poor nutrition and trauma. The
remaining principal preventable cause of conductive hearing loss is
middle ear infection or otitis media (OM) and its sequelae.
5TABLE 1. CSOM PREVALENCE (WHO)
Prevalence of CSOM Nation/Population Group
Highest (>4%)—urgent attention Tanzania, India, Solomon
needed for massive public health Islands, Guam, Greenland,
problem ATSI people
High (2-4%)-avoidable burden of Nigeria, Angola, Korea, China
disease must be addressed Thailand, Malaysia, Vietnam
Philippines, Micronesia, Inuit.
Low (1-2%) Brazil, Kenya
Lowest (>1%) Gambia, Saudi Arabia, Israel,
UK, Denmark, Australia, USA
Source: WHO: Chronic Suppurative otitis media: Burden of illness
and management options.
6Not unexpectedly, the causation and risk factors for otitis media are
very similar in the Indigenous populations of the world particularly as
the most severe form of OM, chronic suppurative otitis media (CSOM)
is a disease of poverty. Where there is overcrowding, poor nutrition
and hygiene, exposure to cigarette or other smoke, lack of running
water and lack of ready access to medical care, OM is prevalent in all
its forms in up to 90% of young children. In Indigenous children OM
appears earlier, more frequently and more severely than in non-
Indigenous children. Almost a third of Aboriginal, Greenlandic and
Native American children suffer from chronic suppurative otitis media
(CSOM), yet the WHO states that a CSOM prevalence of greater than
4% is a serious public health problem requiring urgent attention.
OM-related complications cause 21,000 deaths globally every year.(3)
Otitis media-presentation and complications
Acute otitis media (AOM) is essentially an abscess in the middle ear
(Figure 2) which may perforate causing discharge from the middle ear
into the ear canal. If the discharge continues for six weeks, then, by
definition, we have CSOM (Figure 3). If, however, the eardrum or
tympanic membrane does not perforate and the acute infection
settles, we may be left with a non-sterile effusion or glue ear (otitis
media with effusion-OME) (Figure 4). Chronic OME or some chronic
perforations may lead to cholesteatoma (Figure 5) - skin invading the
middle ear, mastoid bone or even the brain, a condition seen in over
10% of children with longstanding ear disease (4).
7This Photo by Unknown Author is
Figure 2. Figure 3.
Acute Otitis Media (AOM) Chronic Suppurative Otitis Media
(CSOM)
Figure 5. OME
Figure 4. Figure 5.
Otitis Media with Effusion. Attic polyp with cholesteatoma.
( OME)
8Other complications of OM and its sequelae include mastoiditis, facial
nerve palsy, vestibulitis, meningitis and brain abscess.
These signs are overt, but it is the silent development of hearing loss
in the absence of obvious signs or symptoms that may be difficult to
notice. In the child under three, this may present as delayed speech
and language development due to the blockage of auditory signals to
the processing areas in the brain. This, in turn leads to problems
learning new tasks relating to hearing and subsequent learning
problems at school. ”If you can’t hear, you can’t learn” is the mantra
we emphasise over and again in our remote visits
But it is the Aboriginal child with longstanding OME and CSOM that
suffers the most from the effects of their middle ear disease. The facts
are confronting—the average Aboriginal child has OME for 32 months
in their first five years of life compared with three months for non-
Indigenous children. Almost all remote Aboriginal babies have OME by
age 12 weeks and at least one attack of OM by twelve months. (5) The
associated hearing loss affecting a third of Aboriginal children
throughout childhood leads to inattention, non-attendance at school,
social isolation, early school leaving, lack of vocation, interaction with
drugs, alcohol and the judiciary. 93% of adult male Aboriginal
prisoners in Darwin gaol have a longstanding hearing loss. (6)
CAUSATION OF OTITIS MEDIA
9So, what is causing this mini-epidemic of OM and its sequelae in
Indigenous populations?
The risk factors for OM are varied, but the essential underlying issue
for development of OM, especially CSOM, is poverty. Risk factors
include early nasopharyngeal bacterial colonisation, overcrowding,
lack of breast feeding, poor nutrition and hygiene, passive smoking,
lack of clean running water and lack of access to medical care. (7)
Good housing is critical. Urbanisation worldwide has led to slums,
where 40% of the world’s children live in overcrowded, unsafe,
unhealthy and socially excluding dwellings.
Factors for development of otitis media fall into two major categories,
host-related factors and environmental factors.
Host-Related factors
A major cause of early development of middle ear disease in
Indigenous babies and infants is the failure of their immature immune
systems to elicit a strong response to an overwhelming
nasopharyngeal colonisation by bacterial organisms.
Three principal bacteria, together with respiratory viruses are present
in both the nasopharynx and middle ear, resulting in recurrent acute
OM, CSOM as well as OME at an early age, often before 6 months.(8,9)
This causes hearing loss at those critical months for language
acquisition from shortly after birth to eighteen months of age. This can
lead to loss of central auditory neural plasticity and subsequent delay
in speech and language acquisition. (10) The same applies to
persistent conductive hearing loss in babies and infants with OME.
10Twin and genomic studies have isolated genes which increase the risk
of recurrent OM such as FBOX 11 discovered at TKI. (11).
Environmental factors
Overcrowding is seen in many Indigenous households, with
substandard housing or inadequate numbers of bedrooms. The
average number of persons per Indigenous household is almost five,
compared to half that rate in non-Indigenous households, and in some
remote regions up to nineteen people may share a home. (12). This
overcrowding places children at risk for recurrent upper respiratory
tract infections with middle ear and lower respiratory tract infections
as complications. This is known as the ‘day care effect’. (13).
Passive cigarette smoking, or exposure to other environmental smoke
has been shown in the Kalgoorlie Otitis Media study to significantly
increase the risk of RAOM and chronic OME. (14)
Breastfeeding has a protective effect related to the immunological
properties of breast milk. (15). Poor nutrition leads to a multiplicity of
health disorders including type 2 diabetes mellitus which can impact
on the child’s resistance to infection. Lack of access to clean running
water, and lack of access to medical care are other concomitant
external factors.
In addition to these social determinants of health affecting the
development of otitis media, historical and cultural determinants play
a role as well.
IMPACT OF OM ON CHILDREN’S
DEVELOPMENT
11Otitis media by virtue of its longevity in Indigenous children has an
impact that affects their language and speech development, with
secondary effects on school learning, socialisation, general
development and later, vocational outcomes and interaction with the
judiciary.
The areas of cognitive development most likely to be affected by
hearing loss associated with OM and its sequelae are auditory
processing skills, attention, behaviour, speech and language. (16) The
specific auditory processing skills affecting these children include
difficulty with sound localisation, difficulty discriminating speech
sounds in noisy backgrounds.
Behavioural and attentional difficulties have been noted and speech
perception in Indigenous children with OM showed a reduced ability
in those children with English as a second language. (17). A study of
Aboriginal children with OM showed that, compared with their peers
without OM, they had significantly poorer phonological awareness,
spelling and reading skills. (18) (19)
Williams (16) has noted those myriad of factors that impact on the
ability of an Indigenous child with OM to acquire speech and language.
The factors that are associated with high risk are in Table 2.
• Early onset of OM under 12 months of age
12• More than one episode of OM before 12 months of age
• Long periods of infections
• Poor or no access to medical management
• Compromised environment (passive smoking, overcrowding etc.)
• Pre-existing cognitive or language deficit
• Disrupted attachment
• Degree of hearing loss
TABLE 2 . FACTORS THAT INCREASE THE RISK OF SUSTAINING LONG-
TERM SPEECH AND LANGUAGE DEFICITS FROM OM. (After Williams
2009)
At school, Indigenous children who have hearing loss and have had
difficulty in picking up the sounds of their own language, may find it
even harder to follow lessons in the second language, English. For
example, high frequency sounds such as s, f, t, th don’t exist in
13Aboriginal languages and will be hardest to hear if there is a hearing
loss. If this hearing loss is compounded by a noisy classroom as well as
a secondary central auditory processing disorder, then the child will
be significantly disadvantaged educationally.
There are subsequent social and emotional issues with long term
hearing loss leading to social isolation, reduced self esteem, mental
health issues, truancy issues, drug and alcohol issues, self harm,
vocational issues and interaction with the judicial system.
PREVENTION OF HEARING LOSS
“An ounce of prevention is better than a pound of cure.”
14Benjamin Franklin.
The WHO categorises prevention in three tiers, primary prevention to
avert an adverse health condition, secondary prevention to detect a
condition early and to treat it promptly and tertiary prevention to
reduce the impact of an established condition and restore function,
where possible.
Significant preventable causes of hearing loss include otitis media,
maternal rubella, other infectious diseases, perinatal problems,
ototoxic medications, consanguinity and loud noise exposure.
The prevention of OM in Indigenous children, apart from vaccination,
and appropriate and early medical intervention, is related principally
to addressing the social determinants of health. Pneumococcal
conjugate vaccination has led to a modest drop in AOM episodes in
Indigenous children. But it is those underlying fundamentals of public
health that are the essential factors requiring attention in order to
effectively prevent OM and its sequelae. Attention to noise protection
such as from rifle fire and snowmobiles in Indigenous children in
Canada is another preventive action, as well as education and
legislation to reduce noise damage from personal musical devices.
Strategies that address the social determinants of ear health include
those in Table 3. Most of these are primary preventions, but early
recognition and treatment of disease is secondary, and ear surgery,
hearing aids, cochlear implants, sign language are tertiary preventive
measures.
15Table 3; PUBLIC HEALTH INTERVENTIONS FOR OTITIS MEDIA
• Avoiding overcrowding - a bed for each child
• Clean water for washing and showering. Swimming pools
• Improved nutrition and healthy eating
• Increasing breastfeeding to at least six months
• Reducing passive smoking from cigarettes and campfires
• Keeping flies away from food and children’s ears, nose & mouths
• Hand and face washing, BBC program (Breathe, Blow, Cough)
• Ensuring all vaccinations up to date, especially pneumococcal
• Early intervention for infections, regular health checks
• Education programs regarding prevention, early diagnosis and
treatment of otitis media
These preventive measures are where those at the coal-face in
Indigenous communities-the primary health care workers, nurses and
general practitioners are the most important to address this
condition, in association with Aboriginal, Indian or Inuit health
services together with Government and non-Government
organisations (NGOs). Secondary to these, audiologists, speech
16pathologists, teachers of the deaf as well as otolaryngologists support
and treat those affected children.
There are internationally, many groups and organisations dedicated
to help manage the global burden of OM, from the WHO, Inuit,
American Indian, and Aboriginal medical services, through to
innovative award winning programs such as Deadly Ears in
Queensland and Earbus Foundation of Western Australia.
Globally, it is well known that persistent, consistent, culturally
appropriate interventions deliver the best outcomes in terms of
disease and hearing outcomes.
EAR AND HEARING CARE IN INDIGENOUS
POPULATIONS
At the global level, stakeholders in the hearing health community at
all levels should join forces to ensure member states have access to
educational material such as the WHO Ear Health Manual, training,
and equipment through existing government, service organisations
17and NGOs, universities and research organisations and Indigenous
health services. Low cost hearing aids, cochlear implants and
telehealth services including tele-audiology should be made available.
At the country level, attention to the call to action by the World Health
Assembly (WHA) in 2017 requires integration of strategies for ear and
hearing care within the framework of their health systems.
There is need for collection of high quality population-based data,
human resource development, early identification and management
Services, noise control and improving access to hearing technologies
and communication.(20).
The services to Indigenous patients should be culturally appropriate
and safe.(21) There is a disparity between supply of services such as
health clinics, equipment and staff training and the demand which
refers to the patient’s ability to access services with cultural
appropriateness. rapport with health professionals and awareness of
services.
At the regional and community level, early and appropriate
antibiotic treatment for acute otitis media and topical drops
and local treatment for CSOM, with timely referral to surgeons
for grommet, and middle ear surgery accompanied by
audiologic and habilitation is essential. As hearing health
professionals are scarce in low and middle income countries,
capacity building and education are a high priority. Task
18sharing may be an approach to ameliorate this skills shortage.
Research and innovation may allow, as in India, trained
technicians performing myringoplasty procedures, or the new
tissue engineered techniques with reduced operating
time.(22,23)
In Australia the 2020 otitis media guidelines and the new app
improve access to the most up to date evidence on best
practice in otitis media and hearing loss prevention and
management for ATSI children.
DIFFERENT MODELS OF EAR AND HEARING CARE
COMMUNITY BASED EAR HEALTH CLINICS
Whether by fly in-fly out ear health teams, such as in the Queensland
Deadly Ears Program, or mobile units with sound treated buses,
(Earbus Foundation of WA, Variety Club ear buses in New Zealand),
the essentials of these programs is to provide diagnostic and
therapeutic ear health in the local community, especially in rural and
19remote communities. This is often closely allied to local community
health organisations such as Aboriginal Medical Services providing on
the ground support and their own ear health teams as well. Aboriginal
Health Workers, Community, school and child health nurses are the
linchpin providing ongoing care between ear health team visits.
Community liaison and education workers are important members of
the team, as are health promotion officers.
Initiatives such as the MRFF project chaired by Professor Catherine
McMahon are exploring innovative methods to co-produce,
implement and evaluate a community-based model of ear and hearing
care for Aboriginal children with strengthened partnerships between
health and early years through to primary education.
Eventually, the aim is for each community to have dedicated
Aboriginal Ear Health Workers (or Ear, Eye and Dental AHWs as
suggested by Minister Ken Wyatt) and Aboriginal community liaison
workers with ear nurse specialists, audiologists and general
practitioners providing secondary support and ENT surgeons and
other groups such as Hearing Australia providing tertiary services.
TELEHEALTH OUTREACH
The exponential growth in telehealth, especially during the Covid era
has significantly enhanced the capabilities of remote consultations,
either as ‘live’ or as ‘store and send’ consultations. Complex
audiological procedures such as brain stem evoked audiometry or
mapping of cochlear implants can be supervised by telemedicine, as
can surgical procedures. (24) The stand-out tele-health centres in ear
health are in Alaska and Ontario, with validation of significant benefits
both clinically with wait times and financially with cost savings. In
20Australia, some tele-otology and tele-audiology programs have been
in service for over ten years, but there is a significant need for more
such initiatives. (25) (Figures 7,)
This Photo by Unknown Author is licensed under CC BY-ND
Figure 7. Telehealth
SURGICAL BUSES
Globally, fully equipped surgical buses have been used to perform
various specialised surgical procedures in urban, rural and remote
locations. Between 50-70% of all procedures performed today are day
surgical procedures, ideally suited, with appropriate patient
screening, for surgical buses. Examples include those in the Solomon
Islands, India, and Bali as well as New Zealand. Otologic surgery lends
21itself to day surgery and the cost and patient satisfaction of having
their surgery in their local region rather than often hundreds of
kilometres away is undeniable. Hopefully, the next generation of
surgeons will continue to advocate for surgical buses, ideal in
Australia’s vast outback. (Figure 8)
This Photo by Unknown Author is licensed under CC BY-SA
Figure 8. Mobile operating bus
INDIGENOUS EAR HOSPITALS
In Anchorage, Alaska, the Alaska Native Medical Centre has a
173 bed hospital offering comprehensive medical services
including otolaryngology to Alaska Native and American Indian
people living in Alaska. The 9 staff otolaryngologists provide
medical and surgical management as well as perform
telemedicine consultations to remote communities in Alaska,
with significant cost savings from live on line consultations
22compared with transferring patients to Anchorage. The
Community Health Aides in each village liaise with the patients
to ensure this is effective.
ADJUNCTIVE SERVICES
Services such as Hearing Australia, a government sponsored
agency provides innovative diagnostic services including
PLUM and HAP-EE, hearing aid fitting and classroom
amplification systems. Speech pathologists, teachers of the
deaf and other para-medicals are important members of the
team habilitating children with hearing loss. The interface of
medicine and education is often overlooked and teachers,
Aboriginal education workers together with other community
staff are critical in the school aged child’s ear and hearing
health.
CLOSING THE GAP IN INDIGENOUS EAR & HEARING HEALTH
So, how do we address this silent epidemic? We start with community-
based organisations educating parents and carers and treating the
children at the earliest stages of infection, with frequent opportunistic
hearing screening by health workers and nurses, utilising telemedicine
for the difficult cases, and expedited treatment
23Including surgery. We should advocate, develop and ensure pathways
into addressing professional inequality on vocational training for
Indigenous people.
In order to close the gap in ear and hearing health equity in Indigenous
communities generally, we need to consider the seven steps
suggested by respected public health advocate Professor Ian Ring
recently.
These are relatable to all First Nations globally -
1. Setting of achievable and fully budgeted targets
2. Needs based funding- Funding based on the burden of disease,
which is three times greater in ATSI populations than in non-
ATSI populations
3. Focus on services--From resourcing and policy issues at the
national level though to staffing, training and resourcing at the
regional level
4. Training - Development of a national training plan to ensure all
involved in the field are trained in culturally appropriate service
delivery, with capacity building for Indigenous staff a linchpin
5. Management - Development of a formal, integrated, multi-
layered management system, underpinned with information
and evaluation systems
6. Continuous quality improvement - The need for proper systems
to measure, monitor and evaluate the quality of services.
Output assessment is good, outcomes assessment essential
247. Learning from national and international experience -
Adaptation of successful programs using systematic application
of current knowledge to the local regional services
IN CONCLUSION
Sixty percent of Indigenous hearing loss and ear disease is
preventable. The major problem of chronic middle ear disease is
preventable in the majority of cases by diligent application of early
diagnosis, timely treatment, appropriate ,supportive habilitation with
accompanying translational research and attention to the underlying
social determinants of health.
Hearing loss cannot and must not continue to be a silent epidemic.
REFERENCES
1. Clark H et al, A future for the world’s children? A WHO-
UNICEF- Lancet Commission. Lancet, 395; 2020:605-614.
252. Wilson BS, Tucci DL, Merson MH, O’Donoghue GM. Global
hearing health care: new findings and perspectives.
Lancet.390;2017:2503-2515.
3. Murray CH, Lopez AD. Global Burden of Disease. Geneva,
World Health Organisation, 1996; 433-468.
4. MacKendrick A. Ear surgery in Australian Aboriginal
children-is it indicated and when is the best time? Aust J
Otolaryngol 1999;3:240-242.
5. Lehmann D, Weeks S, Jacoby P, Elsbury D, Finucane J,
Stokes A, Monck R & Coates H. Absent otoacoustic emissions
predict otitis media in young Aboriginal children; a birth cohort
study in Aboriginal and non-Aboriginal children in an arid zone
of Western Australia. BMC Pediatr 2008;8:32.
6. Vanderpoll T & Howard D. Massive prevalence of hearing
loss among Aboriginal inmates in the Northern Territory.
Indigenous Law Bulletin, 2012-search.informit.com.au.
7. Kong K & Coates HL, Natural history, definitions, risk
factors and burden of otitis media. Med J Aust, 2009, 191, S39-
43.
8. Leach AJ, Boswell JB, Asche V, Nienhuys TG, Mathews JD.
Bacterial colonisation of the nasopharynx predicts very early
onset and persistence of otitis media in Australian Aboriginal
infants. Pediatr Inf Disease Journ. 1994. 13 (11): 983-989.
269. Massa HM, Cripps AW, Lehmann D. Otitis Media :viruses,
bacteria, biofilms and vaccines. Med J Aust 2009; 191 (9) S44-
S49.
10. Yoshinaga-Itano C, Sedey AL, Coulter DK, Mehl AL.
Language of early and later- identified children with hearing
loss. Pediatrics 1998 102 (5), 1161-1171.
11. Rye MS, Wiertsema SP, Scaman ES, Oommen J, Sun W,
Francis RW, Ang W, Pennell CE, Burgner D, Richmond P,
Vijayasekaran S, Coates HL, Brown SD, Blackwell JM, et al,
FBX011, a regulator of the TGFbeta pathway, is associated with
severe otitis media in Western Australian children. Genes
immune.2011 Jul;12(5):352-9.
12. Jervis-Bardy J, Sanchez L, & Carney AS. Otitis Media in
Indigenous Australian children: review of epidemiology and risk
factors. Journ Laryngol otol. 2014 Jan, 128;S1.
13. Wald ER, Dashefsky B, Byers C et al. Frequency and
severity of infections in daycare. J Pediatr.1988, 112:540-546.
14. Jacoby P, Coates H, Arumugaswamy A et al. The effect of
passive smoking on the risk of otitis media in Aboriginal and
non-Aboriginal children in the Kalgoorlie-Boulder region of
Western Australia. Med J Aust 2008; 188:599-603.
15. Breastfeeding and childhood acute otitis media: a
systematic review and meta-analysis. Bowatte G, Tham R, Allen
KJ, Tan DJ, Lau MXZ, Dai X, Lodge CJ.Acta Paediatrica 2015,
104; 85-95
2716. Williams CJ & Jacobs AM. The impact of otitis media on
cognitive and educational outcomes. Med J Aust. 2009
;191(9):S69-S72.
17. Aithal S, Yonovitz A, Aithal V. Perceptual consequences of
conductive hearing loss, speech perception in Indigenous
students learning English as a ‘school’ language. Aust NZ J
Audiol2008; 30: 1-18.
18. Walker N, & Wigglesworth G. The effect of conductive
hearing loss on phonologic awareness, reading and spelling of
urban Aboriginal children. Aust NZ J Audiol 2001;23: 37-51.
19. Zubrick SR, Lawrence DM, Silburn SR, et al. The Western
Australian Aboriginal Child Health Survey; the health of
Aboriginal children and young people. Perth; Telethon Institute
for Child Health Research, 2004.
20. Chadha S, Cieza A, World Health Assembly adopts a
resolution on hearing loss: a defining moment for the global
hearing health community. ENT and Audiology news. 26. 2017.
21. Curtis, E., Jones R, et al. (2019) Why cultural safety rather
than cultural competency is required to receive health equity:
a literature review and recommended definition. Int. journal
for equity in health. 18(1) 174.1082-3.
22. Kanemaru S-I, Umeda HKitani Y, Nakamura T ,Hirano S, Ito
J. Regenerative treatment for tympanic membrane perforation.
Otol Neurotol. 32 (2011), 1218-1223.
2823. Acharya AN, Coates H, Tavora-Vieira D, Rajan GP. A pilot
study investigating basic fibroblastic growth factor for the
repair of chronic tympanic membrane perforations in pediatric
patients. Int J Pediatr Otorhinolaryngol. 79 (2015) 332-335.
24. Golnick C, Elvin Asay, Provost E, Van Liere D, Bosshart C,
Rounds-Riley J et al. Innovative primary care delivery in rural
Alaska: a review of patient encounters seen by community
health aides. International Journal of Circumpolar Health Vol
71, 2012. Issue 1.
25. Swanepoel DW, Myburgh HC, Howe DM, Mahomed F,
Eikelboom RH. Attitude to telemedicine, and willingness to use
it, in audiology patients.Int. Journal of audiology.53 (12),2014;
841-849.
29You can also read

















































