Successful Treatment of Herpes Zoster Ophthalmicus Complicated by Intense Orbital Inflammation Using Laser Irradiation over the Stellate Ganglion ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
doi: 10.2169/internalmedicine.9503-22
Intern Med 62: 623-627, 2023
http://internmed.jp
【 CASE REPORT 】
Successful Treatment of Herpes Zoster Ophthalmicus
Complicated by Intense Orbital Inflammation Using Laser
Irradiation over the Stellate Ganglion
Yoshifumi Ashikawa 1, Fumiko Kusunoki Nakamoto 1, Tatsuya Sato 1, Junko Katsumata 1,
Taro Bannai 1, Tomonari Seki 1, Masako Takeda 2 and Yasushi Shiio 1
Abstract:
A 56-year-old man presented with right-sided headache and ptosis accompanied by a facial skin rash. He
was diagnosed with herpes zoster ophthalmicus (HZO). Despite acyclovir and steroid therapy, the ocular
symptoms worsened. Magnetic resonance imaging (MRI) revealed severe orbital inflammation and abnormal
lesions in the right trigeminal nucleus and tract. The effects of re-administration of intravenous acyclovir and
steroid pulse therapy were limited. Laser irradiation of the stellate ganglion (SGL) and high-dose oral predni-
solone therapy were effective. Our experience suggests the efficacy of early multimodal treatment, including
SGL, in treating ocular symptoms associated with HZO.
Key words: herpes zoster ophthalmicus, ocular symptoms, stellate ganglion laser, stellate ganglion block,
spinal trigeminal nucleus and tract
(Intern Med 62: 623-627, 2023)
(DOI: 10.2169/internalmedicine.9503-22)
and has clinical efficacy similar to that of SGB ther-
Introduction apy (2, 3).
We also reviewed the literature concerning the effects of
Herpes zoster ophthalmicus (HZO) is caused by reactiva- SGB on oculomotor dysfunction in HZO and discussed the
tion of the varicella-zoster virus (VZV) in the trigeminal effects of SGL in the current patient.
ganglia. It accounts for 10-25% of all herpes zoster cases
and causes external ophthalmoplegia in approximately 10% Case Report
of cases (1). It can also cause cranial neuropathies. In order
of frequency, the oculomotor, abducens, and trochlear nerves The patient was a 56-year-old man with chief concerns of
may be affected. Several cranial nerves can be affected si- difficulty opening his right eye and headache on his right
multaneously (1). Treatment of HZO includes acyclovir, oral side. Three weeks before admission, he experienced pain in
steroids, and steroid pulse therapy. Although it has been pre- his right eye and drooping of the right upper eyelid. One
viously reported that stellate ganglion block (SGB) is effec- week later, he consulted with a dermatologist at our hospital
tive in relieving pain in herpes zoster, there is no evidence as a result of erythema, which appeared in the region of the
of its effect on oculomotor dysfunction. skin innervated by the first branches of the right trigeminal
We herein report a patient with severe orbital inflamma- nerve, including the dorsum nasi. He presented with a swol-
tion secondary to HZO, who showed a good clinical re- len eyelid with vesicles and right ocular pain, as well as dif-
sponse to laser irradiation of the stellate ganglion (SGL). ficulty opening his right eye. The patient was thus diagnosed
SGL is performed in the supine position by placing the with herpes zoster in the first branch of the right trigeminal
probe in contact with the skin of the neck and irradiating nerve.
the stellate ganglion region. SGL is less invasive than SGB Acyclovir was administered intravenously at 250 mg/day
1
Department of Neurology, Tokyo Teishin Hospital, Japan and 2 Department of Anesthesiology, Tokyo Teishin Hospital, Japan
Received: February 1, 2022; Accepted: May 23, 2022; Advance Publication by J-STAGE: July 14, 2022
Correspondence to Dr. Fumiko Kusunoki Nakamoto, kusunoki-nhn@umin.ac.jp
623
Intern Med 62: 623-627, 2023 DOI: 10.2169/internalmedicine.9503-22
a
b
Figure 1. Eye movement examination findings. (a) At hospital admission. (b) After intravenous
acyclovir therapy, steroid pulse therapy, and stellate ganglion laser irradiation.
for 1 week and oral prednisolone at 15 mg/day for 3 days. on days 1 to 3, followed by 250 mg on days 4 and 5) were
During treatment, he developed keratitis and iritis in his administered. Following the initiation of treatment, his
right eye and was started on topical acyclovir ointment. His keratitis and iritis disappeared, and his right visual acuity
skin rash improved, and he was discharged from the hospi- improved. However, there was limited improvement in his
tal. However, his difficulty opening his right eye and his ocular motility, and ptosis and ocular pain persisted. Oral
right ocular pain did not improve after discharge, so he was prednisolone therapy (50 mg/day) was initiated 6 days after
admitted to the Department of Neurology. His medical his- admission, and SGL using SUPER LIZER HA2200™ (To-
tory included gallbladder polyps, and he was not taking any kyo Iken, Tokyo, Japan) and supraorbital nerve block were
regular medication. performed. After the second SGL, the limitations in adduc-
Upon admission, the patient had no fever and was con- tion, elevation, and depression in his right eye significantly
scious and coherent. He had mild erythema on the right improved.
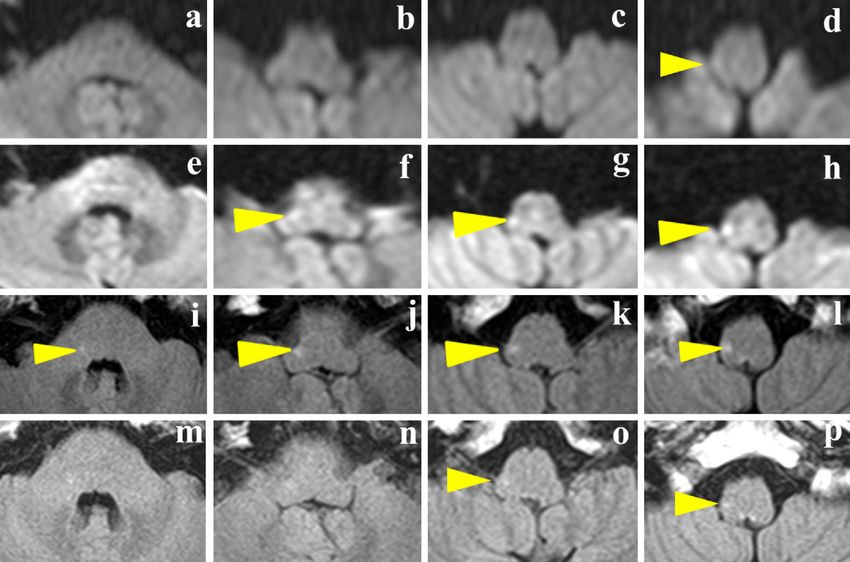
forehead and around the right eye, crusted vesicles on the Ten days after admission, fluid-attenuated inversion recov-
right eyelid, and hyperemia of the right palpebral and bulbar ery (FLAIR) imaging and DWI revealed hyperintense le-
conjunctiva. sions extending from the right side of the lower medulla ob-
His neurological findings included decreased right visual longata to the upper medulla oblongata. These lesions repre-
acuity, inability to open the right eye, and ocular motility sent the anatomical location of the right spinal trigeminal
disorder in all directions, characterized by severe abduction nucleus and tract (STNT) (Fig. 3e-l, arrowhead). There were
deficiency and limitation of adduction, elevation, and de- no new symptoms or worsening of neurological findings,
pression (Fig. 1a). The patient also had hypoesthesia in the and oral prednisolone and SGL were continued. Follow-up
region of the first branch of the right trigeminal nerve. No MRI performed nine days later revealed that the STNT le-
meningeal irritation was observed. A cerebrospinal fluid ex- sions had not improved. After the third SGL, abduction of
amination revealed the following: cell count, 28/μL; pre- the right eye gradually returned. After 49 days of hospitali-
dominance of small lymphocytes; protein level, 44 mg/dL; zation, MRI showed that the swelling of the right external
IgG index, 0.71; negative for VZV IgM antibodies; and ocular muscle had improved, and the abnormal signal in the
positive for VZV IgG antibodies. A visual evoked potential right STNT had become obscured (Fig. 3m-p, arrowhead).
test revealed a prolonged latency of P100. Magnetic reso- The diplopia in his right gaze disappeared (Fig. 1b), and the
nance imaging (MRI) showed severe inflammation through- patient was discharged after 56 days of hospitalization.
out the orbit with involvement of the extraocular muscles The clinical course of the patient is shown in Fig. 4. Out-
and retrobulbar soft tissues as well as abnormal contrast en- patient follow-up was performed regularly, and the oral
hancement (Fig. 2a-f) and a high signal intensity on the prednisolone dose was gradually decreased. Three months
right side of the lower medulla oblongata on diffusion- after discharge, his diplopia persisted only in the left gaze.
weighted imaging (DWI) (Fig. 3a-d, arrowhead). Follow-up MRI performed one year later revealed that the
Intravenous acyclovir (1,500 mg/day for 14 days) and a STNT lesion had disappeared.
5-day course of methylprednisolone pulse therapy (1,000 mg
624Intern Med 62: 623-627, 2023 DOI: 10.2169/internalmedicine.9503-22
STIR T2WI Contrast-enhanced T1WI
a b c
On admission
d e f
On admission
g h
Just before
discharge
Figure 2. Orbital MRI. (a-c, g) Axial MRI. (d-f, h) Coronal MRI. (a-f) MRI on admission showing
enlargement of the right external ocular muscles and irregular enhancement effects on the right in-
ternal and external orbital ocular muscles, perioptical nerve, and part of the intrafoveal lipid tissue.
(g, h) MRI just before discharge revealed that the swelling of the right external ocular muscle had
improved, and the abnormal signal in the right trigeminal nerve tract nucleus had become obscured.
MRI: magnetic resonance imaging, STIR: short T1 inversion recovery imaging, T2WI: T2-weighted
imaging, T1WI: T1-weighted imaging
DWI on
admission
DWI taken
10 days after
hospitalization
FLAIR taken
10 days after
hospitalization
FLAIR at
discharge
Figure 3. Axial brainstem MRI. (a-d) DWI on admission. (e-l) DWI and FLAIR images obtained 10
days after admission. (m-p) FLAIR images obtained at discharge. DWI: diffusion-weighted imaging,
FLAIR: fluid-attenuated inversion recovery, STNT: spinal trigeminal nucleus and tract
reported that SGB can improve facial pain following herpes
Discussion zoster infection (4). However, to our knowledge, there have
been only three reports of improved oculomotor dysfunction
The therapeutic course of the patient suggests that SGL is after treatment of herpes zoster by SGB (5-7). We summa-
effective not only for pain management due to herpes zoster rized the findings of the five cases in which SGB was effec-
but also for external ophthalmoplegia. Several papers have tive for treating eye movement disorders caused by herpes
625Intern Med 62: 623-627, 2023 DOI: 10.2169/internalmedicine.9503-22
Hospitalization
Right headache
Right eye opening
difficulty & oculomotor
impairment
Right facial rash
Right keratitis &
iritis
-21 -14 0 6 14 18 26 33 Day 56
ACV intravenous 1500mg
250mg
infusion
IVMP
Steroid treatment PSL 15 mg PSL 50mg
Stellate ganglion irradiation
Figure 4. Clinical course. ACV: aciclovir, IVMP: intravenous methylprednisolone pulse, PSL:
prednisolone
Table. Summary of Cases Treated with SGB/SGL for Oculomotor Disorder Due to Herpes Zoster.
SGB Number of SGB/SGL Other treatments
Age/ Steroid therapy Total number
References or before improvement of in combination
sex before SGB/SGL of SGB/SGL
SGL oculomotor disorders with SGB/SGL
(5) 81/F SGB PSL 3 Pain control 15
72/F SGB PSL+IVMP 3 Pain control 13
(6) 61/M SGB No 8 PSL+pain control 16
73/F SGB No Not mentioned Pain control 12
(7) 52/M SGB PSL 7 Pain control 16
The present patient 56/M SGL PSL+IVMP 2 PSL+pain control 5
SGB: stellate ganglion block, SGL: stellate ganglion laser irradiation, PSL: prednisolone, IVMP: intravenous methylprednisolone
zoster (Table). In these reports, there was no improvement ity disorder five to six weeks after the onset. Based on the
with steroid pulse or oral prednisolone therapies; however, clinical course of the patient and previous reports, we pro-
after SGB was performed three to eight times, improvements pose that SGL itself was effective in improving ocular
in oculomotor disturbance were observed. After further symptoms.
SGB, diplopia disappeared. Several patients in previous re- Previous papers have suggested that the therapeutic
ports showed improvements in oculomotor disorders during mechanisms involved in SGB and SGL are related to in-
SGB, using only pain control medications without steroid creased cerebral blood flow, which improves tissue ische-
therapy (5-7). mia (9, 10). SGB has been reported to increase the blood
How SGL contributed to the improvement of ocular flow of the optic nerve head and the peripapillary retina (9),
symptoms in our patient is unclear. Movement disorders due and SGL has been reported to increase the blood flow to the
to herpes zoster can occasionally improve spontaneously. ophthalmic and central retinal arteries (10). SGL is less in-
However, this patient showed intense orbital inflammation, vasive than SGB and has been reported to have clinical effi-
and if the treatment had not been initiated, he would have cacy similar to that of SGB (2, 3).
had severe visual sequelae. There is also a possibility that Several mechanisms underlying the oculomotor disorders
only steroid therapy was effective. However, the patient in this patient have been proposed. The oculomotor nerve
showed significant improvement after starting SGL. In a re- may first have been damaged by VZV, which is known to
port of 18 cases of unilateral rather than bilateral ophthal- incubate in the trigeminal ganglion via the cavernous sinus,
moplegia with ocular motor deficits in all 4 directions due superior orbital fissure, and orbital apex. The trochlear and
to herpes zoster, ophthalmoplegia took an average of 4.4 abducens nerves may have been affected by the invasion of
months to disappear. Several patients had residual ophthal- the VZV or the spread of inflammation. Inflammation and
moplegia despite antiviral drugs, or steroids, or a combina- swelling of extraocular muscles and retrobulbar soft tissues
tion therapy with antiviral drugs and steroids (8). In our can also cause oculomotor disorders. The effect of SGL on
case, SGL was started four weeks after the onset, and the oculomotor disorders suggests ischemia caused by occlusive
patient showed significant improvement in his ocular motil- vasculitis.
626Intern Med 62: 623-627, 2023 DOI: 10.2169/internalmedicine.9503-22
In the present patient, abnormal signals were observed cidence of postherpetic neuralgia. Pain Phys 15: 467-474, 2012.
along the STNT. It was previously reported that 9 of 16 pa- 5. Hase K, Meguro K, Fujimoto T. Stellate ganglion-block improved
abducense nerve palsy associated with facial herpes zoster. Nihon
tients with herpes zoster in the trigeminal and cervical nerve
Pain Clin Gakkaishi (J Jpn Soc Pain Clin) 6: 105-109, 1999 (in
regions had abnormal signals in the brainstem or cervical Japanese, Abstract in English).
spinal cord on MRI (11). However, there have been only 6. Tomita N, Katsumata N, Kurihara M, et al. Two cases of stellate
five case reports in which the entire STNT has been deline- ganglion block for oculomotor nerve palsy associated with herpes
ated. In these patients with herpes zoster, the STNT showed zoster in the first branch of the trigeminal nerve. Nihon Pain Clin
Gakkaishi (J Jpn Soc Pain Clin) 22: 564-565, 2015 (in Japanese).
a high signal on T2-weighted images, and in several pa-
7. Hara A, Yashima N. Abducens nerve palsy caused by herpes
tients, the STNT also showed a high signal intensity on zoster. Nihon Pain Clin Gakkaishi (J Jpn Soc Pain Clin) 25: 86-
FLAIR or DWI (12-16). In the present patient, DWI at the 90, 2018 (in Japanese, Abstract in English).
time of admission showed a hyperintense lesion in the right 8. Sanjay S, Chan EW, Gopal L, et al. Complete unilateral ophthal-
lower medulla oblongata, possibly involving the STNT. Ten moplegia in herpes zoster ophthalmicus. J Neuroophthalmol 29:
325-337, 2009.
days later, the lesion had extended to the superior medulla
9. Yu HG, Chung H, Yoon TG, et al. Stellate ganglion block in-
oblongata. The first branch of the trigeminal nerve termi- creases blood flow into the optic nerve head and the peripapillary
nates in the caudal part of the spinal trigeminal nucleus, and retina in human. Auton Neurosci 109: 53-57, 2003.
it is speculated that the abnormal lesion spread from the 10. Mii S, Kim C, Matsui H, et al. Increases in central retinal artery
caudal part of the STNT in a cephalad direction during the blood flow in humans following carotid artery and stellate gan-
glion irradiation with 0.6 to 1.6 microm irradiation. J Nippon Med
clinical course.
Sch 74: 23-29, 2007.
In summary, we encountered a patient with severe orbital 11. Haanpää M, Dastidar P, Weinberg A, et al. CSF and MRI findings
inflammation secondary to herpes zoster ophthalmicus with in patients with acute herpes zoster. Neurology 51: 1405-1411,
high-intensity signals in the STNT on DWI and FLAIR 1998.
MRI who demonstrated a good clinical response to SGL. 12. Nagane Y, Utsugisawa K, Yonezawa H, Tohgi H. A case with
trigeminal herpes zoster manifesting a long lesion of the spinal
Early multimodal treatment with SGL may be required in
trigeminal nucleus and tract on MR T2-weighted image. Rinsho
patients with HZO with severe orbital inflammation. Shinkeigaku 41: 56-59, 2001 (in Japanese).
13. Douglas JE, Buch VP, Mamourian AC. Varicella zoster-induced
The authors state that they have no Conflict of Interest (COI). magnetic resonance imaging abnormalities of the trigeminal nu-
cleus. J Neurol Sci 359: 57-58, 2015.
14. Hung CW, Wang SJ, Chen SP, et al. Trigeminal herpes zoster and
References Ramsay Hunt syndrome with a lesion in the spinal trigeminal nu-
cleus and tract. J Neurol 257: 1045-1046, 2010.
1. Marsh RJ, Cooper M. Ophthalmic herpes zoster. Eye (Lond) 7: 15. Nogueira RG, Seeley WW. Ramsay Hunt syndrome associated
350-370, 1993. with spinal trigeminal nucleus and tract involvement on MRI.
2. Liao CD, Tsauo JY, Liou TH, et al. Efficacy of noninvasive stel- Neurology 61: 1306-1307, 2003.
late ganglion blockade performed using physical agent modalities 16. Himeno T, Takeshima S, Kubo S, et al. Trigeminal herpes zoster
in patients with sympathetic hyperactivity-associated disorders: a presenting with high-intensity signals for the spinal trigeminal nu-
systematic review and meta-analysis. PLOS ONE 11: e0167476, cleus and tract on diffusion-weighted image: a case report of
2016. stroke mimic. Brain Nerve 70: 161-164, 2018 (in Japanese).
3. Liao CD, Tsauo JY, Chen HC, Liou TH. Efficacy of stellate gan-
glion blockade applied with light irradiation: a systemic review The Internal Medicine is an Open Access journal distributed under the Creative
and meta-analysis. Am J Phys Med Rehabil 96: e97-e110, 2017. Commons Attribution-NonCommercial-NoDerivatives 4.0 International License. To
4. Makharita MY, Amr YM, El-Bayoumy Y. Effect of early stellate view the details of this license, please visit (https://creativecommons.org/licenses/
ganglion blockade for facial pain from acute herpes zoster and in- by-nc-nd/4.0/).
Ⓒ 2023 The Japanese Society of Internal Medicine
Intern Med 62: 623-627, 2023
627You can also read

















































