Structured Imaging Approach for Viral Encephalitis - BINASSS
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
S t r u c t u re d I m a g i n g
A p p ro a c h f o r Vi r a l
Encephalitis
Norlisah Mohd Ramli, MBBS, FRCRa,*, Yun Jung Bae, MD, PhDb
KEYWORDS
Magnetic resonance imaging (MRI) Neuroimaging Viral encephalitis
Acute encephalitis syndromes (AES) Infectious encephalitis
KEY POINTS
Understanding the typical MR imaging (MRI) patterns caused by archetype viral pathogens is
important, despite considerable overlap, diagnostic uncertainty, and unknown etiologies among
patients with acute encephalitis syndrome.
Acute encephalitis caused by herpes simplex virus type 1 typically affects the temporal lobe.
In patients with bi-thalamic involvement, Japanese encephalitis and influenza-associated enceph-
alitis should be considered.
Enterovirus and rabies virus infections can involve the brainstem.
Varicella-zoster virus infection can cause vasculopathy. Dengue virus can be present with various
MRI patterns.
INTRODUCTION patients.3 Table 1 shows the wide variety of viruses
known to cause human disease, including herpes
Acute encephalitis syndrome (AES) is defined as simplex virus (HSV, 11%–22% of cases in some
acute inflammatory processes affecting the brain, studies), varicella-zoster virus (VZV, 4%–14%), en-
resulting in neurologic manifestations, such as fe- teroviruses (1%–4%), arboviruses (arthropod-
ver, seizures, psychiatric/behavioral/speech disor- borne pathogens spread by mosquitos, ticks, and
ders, disturbances of consciousness/memory, other vectors, usually with geographic and sea-
focal neurologic deficit, involuntary movement, sonal variability in incidence) such as Japanese en-
and ataxia; the cause can be both infective cephalitis virus (JEV), dengue virus (DENV), and
and noninfective (such as immune-mediated en- Zika viruses. Outbreak viruses, such as Hendra,
cephalitis).1 In many population studies, up to Nipah, Middle East respiratory syndrome, severe
50% of AES cases have an unknown etiology. acute respiratory syndrome coronavirus 1, and se-
There are ongoing global efforts to identify new vere acute respiratory syndrome coronavirus 2 are
and emerging infectious agents and new forms of uncommon but cause disproportionate public
immune-mediated encephalitis.2 The estimated health damage, while cytomegalovirus is an essen-
incidence of presumed cases of infectious enceph- tial consideration for immunocompromised pa-
alitis is approximately 1.5 to 7 cases per 100,000 tients.4 Readers are encouraged to refer to
people per year, with a higher incidence among articles 4 and 5 for neuroimaging features of Coro-
the elderly, pediatric, and immunocompromised navirus disease.
neuroimaging.theclinics.com
a
Department of Biomedical Imaging, Faculty of Medicine, University of Malaya, Jln Profesor Diraja Ungku
Aziz, 50603 Kuala Lumpur, Malaysia; b Department of Radiology, Seoul National University Bundang Hospital,
Seoul National University College of Medicine, 82, Gumi-ro 173 Beon-gil, Bundang-gu, Seongnam-si,
Gyeonggi-do 13620, Republic of Korea
* Corresponding author. Department of Biomedical Imaging, University of Malaya Medical Centre, 12B South
Tower, Kuala Lumpur 50603, Malaysia.
E-mail address: norlisahramli@gmail.com
Neuroimag Clin N Am 33 (2023) 43–56
https://doi.org/10.1016/j.nic.2022.07.002
1052-5149/23/ÓDescargado
2022 Elsevier Inc. AllMedica
para Biblioteca rightsHospital
reserved.
México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.44 Ramli & Bae
Abbreviations Table 1
ADEM acute disseminated Viruses that can cause encephalitis
encephalomyelitis
AES acute encephalitis syndrome DNA viruses
CE chronic viral encephalitis ssDNA viruses Anelloviridae
CNS central nervous system Parvoviridae
CSF cerebrospinal fluid Parvovirus
DENV dengue virus Parvovirus B19
DWI diffusion-weighted imaging
Partially Hepadnaviridae
FLAIR fluid-attenuated inversion
ssDNA viruses
recovery
GRE gradient-echo recalled dsDNA viruses Adenoviridae
HHS human herpesvirus Adenovirus
HSE HSV encephalitis Adenovirus serotypes
HSV herpes simplex virus 7, 12, 32
JE Japanese encephalitis virus Herpesviridae
JEV Japanese encephalitis virus Human herpes virus
PCR polymerase chain reaction Herpes simplex virus
PML progressive multifocal (HSV)*
leukoencephalopathy Varicella-zoster virus
VZV varicella-zoster virus (VZV)*
Epstein-Barr virus
(EBV)*
Cytomegalovirus
However, chronic viral encephalitis (CE) is rare. (CMV)*
Chronicity can be defined as a period of 4 weeks, Human herpesvirus 6
but no consensus has been reached on the defini- (HHV-6)*
tion. Clinically, CE can present similarly to AES, Human herpesvirus 7
but the course can be protracted, and neurologic (HHV-7)*
syndromes can be unspecific5; viruses respon- Papillomaviridae
sible for CE include John Cunningham virus and Polyomaviridae
Polyomavirus
measles viruses.
JC virus (JCV)*
There are three broad mechanisms by which vi- Poxviridae
ruses cause central nervous system (CNS) dis-
RNA viruses
ease: infection limited to the meninges (also
called “aseptic meningitis”; this mild, self-limiting +ssRNA viruses Astroviridae
Coronavirida
disease has a good prognosis); brain invasion
Flaviridae
resulting in encephalitis; and immune-mediated
Flavivirus
processes [such as acute disseminated encepha- West Nile virus
lomyelitis (ADEM)].4 Correct and timely diagnosis Japanese encephalitis
of infectious encephalitis (Box 1) and identifying virus*
the causative pathogen are necessary for patient Tick-borne encephalitis
management, especially since patients with AES virus
often undergo prolonged hospitalization and can Dengue virus types 1-
have poor outcomes resulting in disability or 4*
death.6 However, the clinical diagnosis can be Hepacivirus
Hepatitis C virus*
challenging for the following reasons: (a) cerebro-
Hepeviridae
spinal fluid (CSF) examination can show normal
Picornaviridae
glucose and normal protein and may not conform Enterovirus*
to the typical pattern of increased protein with Poliovirus types 1-3
predominantly lymphocytic pleocytosis,7 (b) Coxsackievirus A and B
confirmatory polymerase chain reaction (PCR) is Enterovirus 70, 71*
time-consuming, expensive, and scarce8,9; and Retroviridae
(c) a negative test result does not rule out the diag- Lentivirus
nosis. Furthermore, it is difficult to differentiate Human immunodefi-
viral from immune-mediated encephalitis on imag- ciency virus 1-2*
Deltaretrovirus
ing alone. The antibodies responsible for autoim-
mune encephalitis are broadly categorized into (continued on next page)
neuronal surface antibodies, such as NMDAR,
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.Structured Imaging Approach for Viral Encephalitis 45
Table 1 Box 1
(continued ) Diagnostic criteria for presumed infectious or
autoimmune encephalitis
DNA viruses
Major criterion (required):
Human T-lymphotropic
virus 1-2* Altered mental status (ie, decreased or
Togaviridae altered level of consciousness, lethargy, or
Alphavirus personality change) lasting 24 hours with
Rubellavirus no identifiable alternative cause
-ssRNA viruses Arenaviridae Minor criteria (two required for possible en-
Arenavirus cephalitis, more than three required for prob-
Bornaviridae able or confirmeda encephalitis):
Orthomyxoviridae*
Influenzavirus A Fever 38 C within 72 hours before or after
Influenza A virus presentation
Influenzavirus B New onset of focal neurologic findings
Influenza B virus
Paramyxoviridae CSF WBC count 5 mm3
b
Henipavirus Abnormality of brain parenchyma on neuro-
Hendra virus imaging suggestive of encephalitis that is
Morbillivirus either new from prior studies or appears
Measle virus* acute in onset.
Rubulavirus Abnormality on electroencephalography
Mumps virus* consistent with encephalitis and not attribut-
Respirovirus able to another cause
Human parainfluenza
virus Abbreviations: CSF, cerebrospinal fluid; WBC, white
Pneumoviridae blood cell.aConfirmed encephalitis requires patho-
Rhabdoviridae logic examinations or laboratory tests that can
strongly suggest autoimmune encephalitis.bMR imag-
dsRNA viruses Picobirnaviridae ing is the modality of choice for the evaluation of the
Reoviridae encephalitis.
Coltivirus Adapted from Venkatesan A, Tunkel AR, Bloch KC,
Seadornavirus Lauring AS, Sejvar J, Bitnun A, Stahl JP, Mailles A, Dre-
Rotavirus bot M, Rupprecht CE, Yoder J, Cope JR, Wilson MR,
Rotavirus* Whitley RJ, Sullivan J, Granerod J, Jones C, Eastwood
K, Ward KN, Durrheim DN, Solbrig MV, Guo-Dong L,
Abbreviations: +ssRNA, positive-sense single-stranded Glaser CA; International Encephalitis Consortium.
RNA; dsDNA, double-stranded DNA; dsRNA, double- Case definitions, diagnostic algorithms, and priorities
stranded RNA; ssDNA, single-stranded DNA; -ssRNA, nega- in encephalitis: consensus statement of the interna-
tive-sense single-stranded RNA; tional encephalitis consortium. Clin Infect Dis. 2013
Common viruses are highlighted with * Oct;57(8):1114-28.
CASPR2, LGI-1, and GABA, versus intracellular
antibodies, such as Hu (ANNA 1), Ri (ANNA2), (ie, AES) or chronic (ie, CE). The next step involves
CRMP5, Amphiphysin, MA2, and GAD 65. Some the assessment of MR imaging abnormalities
patients with autoimmune or paraneoplastic limbic based on the anatomic location. It forms a frame-
encephalitis may show unilateral or bilateral work to understand viruses that preferentially
increased T2/fluid-attenuated inversion recovery show MR imaging changes in the temporal lobes,
(FLAIR) signal in the medial temporal lobes, thalami, brainstem, splenium of the corpus cal-
mimicking HSV-1 encephalitis.10 losum, and other viruses that may be more vari-
able in appearance, such as VZV and DENV.
STRUCTURED APPROACH TO IMAGE Although different pathogens may share similar
ANALYSIS imaging features (eg, HSV-1 and HHV-6), and a
single virus can cause a variety of MR imaging ab-
MR imaging has demonstrated its value in assess- normalities (for instance, DENV), we believe this
ing viral encephalitis.11 This article proposes a approach may have value if we accept its inherent
structured diagnostic approach using MR limitations in overlap and over-simplification, and
imaging-based neuroanatomical localization and bear in mind that neuroimaging alone cannot
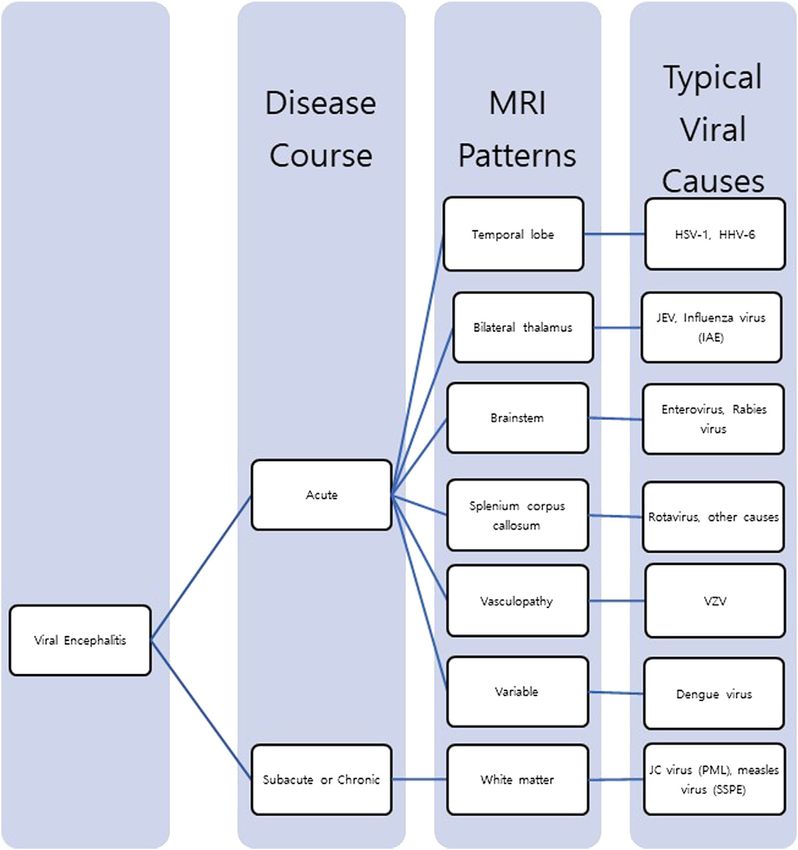
pattern recognition (Fig. 1). First, the course of definitively identify the pathogen but needs
the disease should be determined: if it is acute corroborative clinical and laboratory evidence.
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.46 Ramli & Bae
Fig. 1. Diagnostic algorithm using the structured approach to the viral encephalitis. HHV, human herpesvirus;
HSV, herpes simplex virus; JEV, Japanese encephalitis virus; PML, progressive multifocal leukoencephalopathy;
SSPE, subacute sclerosing panencephalitisl VZV, Varicella-Zoster virus.
ACUTE ENCEPHALITIS SYNDROME showing brain abnormalities in 80% to 100% of
Temporal Lobe Location cases.19 T2-and (FLAIR)-high signal intensities
with swelling preferentially affecting unilateral or
Herpes simplex virus type-1
bilateral asymmetric cortical and subcortical areas
The annual incidence of HSV encephalitis (HSE)
of the anterior and medial temporal lobes and
has been estimated to be w2 to 4 individuals/
insular cortex are typical (Fig. 2). HSV infection
million population worldwide.12 More than 90%
can also involve other parts of the limbic system,
of HSE results from HSV type-1 (HSV-1) infection
subfrontal area, and cingulate gyrus; isolated
in adults, while HSV-2 infection usually occurs in
brainstem involvement is rare.19 The lesions can
neonates or immunocompromised patients.13 In
be either unilateral or bilateral and are mostly
addition, about 30% of HSE cases occur from a
asymmetric. It can be combined with hemorrhage,
primary HSV-1 infection, whereas the remaining
which can be well depicted as hypointensity on
cases are attributed to viral reactivation or reinfec-
T2*-gradient-echo recalled (GRE) imaging or
tion.14 The incidence of HSE from HSV-1 infection
susceptibility-weighted imaging. There may be
has a bimodal age peak, with the first in the pedi-
contrast enhancement in the parenchyma or
atric population and the second in adults over
meninges. In the early stage, diffusion-weighted
50 years of age.15,16 CSF examination with PCR
imaging (DWI) can detect diffusion restriction
should be performed for confirmation.17
before the onset of T2-/FLAIR-signal changes,20
MR imaging is sensitive and specific for HSE
and T2-/FLAIR-signal abnormalities seem more
diagnosis even in the early stages of the disease,18
prominent later in the course. In addition, one
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.Structured Imaging Approach for Viral Encephalitis 47
Fig. 2. Herpes simplex virus encephalitis (A) T2-weighted image shows multiple hyperintense lesions in cortical
and subcortical areas of the left temporal lobe and left insular cortex. (B, C) Diffusion-weighted imaging
(DWI) shows high signal intensity of the involving lesions with mixed apparent diffusion coefficient (ADC) values.
study showed that the presence of restricted diffu- HHV-6 encephalitis, like HSE in the early and mid-
sion was associated with poor outcomes at dle stages, can present diffusion restriction in the
discharge, but T2-/FLAIR-abnormalities did not in- affected area.30
fluence functional outcomes.21 In addition, bilat-
eral temporal lobe involvement or more extensive
brain involvement at admission can be associated Bilateral Thalamic Location
with a poor prognosis.22 In immunocompromised Japanese Encephalitis virus
patients, the lesions can be widespread and affect Japanese Encephalitis (JE) is caused by infection
regions other than the temporal lobes. by the JEV, which is endemic in East and South-
east Asia.31 JEV mainly affects children but can
Human herpesvirus type 6 also involve adults and is transmitted through a
Encephalitis caused by HHV-6 is rare but often has zoonotic cycle between mosquitoes, pigs, and
devastating sequelae.23 HHV-6A and HHV-6B are water birds. Humans are accidently infected and
globally dispersed DNA viruses.24 Although HHV-6 are dead-end hosts because of low levels of tran-
infection is generally asymptomatic, its acute sient viremia.32 Although transmission occurs
infection or reactivation in immunocompromised year-round, seasonal epidemics during the rainy
individuals can be associated with encephalitis season occur when the mosquito density is at its
and other diseases, such as Alzheimer’s disease maximum.33 Approximately 35,000 to 50,000 peo-
or cognitive dysfunction,25 several types of can- ple develop JE each year, with an annual mortality
cer, multiple sclerosis, progressive multifocal leu- rate of 10,000 to 15,000. Its incidence and
koencephalopathy (PML), seizure, heart/lung/liver morbidity have substantially decreased due to
diseases, and epilepsy.26 HHV-6 encephalitis can the wide application of the JE vaccine. However,
also be diagnosed using CSF tests.17 outbreaks still occur, with adult infections also
HHV-6 encephalitis typically affects the mesial increasing.34
temporal lobe, thus resembling HSE.26–28 MRI It is common to have bilateral thalamic involve-
may also show T2-/FLAIR-high signal intensities ment35 (Fig. 3). Thus, when patients with AES
in the thalamus, hypothalamus, brainstem, cere- residing in endemic regions present with bilateral
bellum, or basal ganglia.29 In 2010, Noguchi and thalamic lesions, PCR testing should focus on
colleagues26 compared HHV-6 encephalitis and JEV.17 Lesions can also be observed in the sub-
HSE; they found that mesial temporal lobes were stantia nigra, brainstem, cerebellum, cerebral cor-
exclusively affected in HHV-6 encephalitis but, in tex, basal ganglia, and white matter.36 MR imaging
HSE, extratemporal regions could be additionally is sensitive for evaluating the lesions and demon-
involved. They also found that sequential MRI strates higher diagnostic value. Typically, lesions
showed that, in the late period, abnormal signal in- are hypointense on T1-weighted imaging and
tensities resolved in HHV-6 encephalitis but per- hyperintense on T2-weighted imaging and FLAIR
sisted in HSE. Although these subtle differences images. Thalamic lesions may show mixed inten-
may distinguish HHV-6 infection from HSV infec- sity on T1- and T2-weighted imaging in the sub-
tion, there is significant overlap; additionally, acute phase, suggestive of hemorrhagic
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.48 Ramli & Bae
Fig. 3. Japanese encephalitis (A) FLAIR image shows bilateral symmetric high signal lesions in the thalamus. (B, C)
Most of the lesions show high signal on DWI and mixed ADC values.
changes.37 The involvement of the temporal lobe 4. Category 4—post-infectious focal encephalitis
has also been observed in some studies, but all re- 5. Category 5—no abnormal lesions
ported patients also demonstrated abnormalities
of the thalamus and substantia nigra. This may Hence, category 2 IAE may mimic JE on MR im-
help differentiate JE from the HSE.35 On DWI, the aging, causing bilateral thalamic abnormalities. In
lesions may show diffusion restriction in the acute addition, reversible diffusion-restricted splenial le-
phase38 but most often show high apparent diffu- sions have also been reported in the corpus cal-
sion coefficient values.35 In addition, JE in associ- losum (see later).43,44
ation with cerebral venous sinus thrombosis has
been reported with the help of MRI and MR Brainstem Location
venography.39
Enterovirus
Influenza-associated encephalopathy Enteroviruses are classified into four groups (polio-
Influenza-associated encephalopathy (IAE) is most viruses, Coxsackie A viruses, Coxsackie B viruses,
common in children (those under 5 years of age), and echoviruses) and multiple serotypes.45 As
the elderly, and people who are immunocompro- vaccination efforts have almost eradicated polio-
mised or have chronic renal, cardiac, or respiratory virus, Enterovirus-A71 has become the most
diseases. The incidence of IAE from 1999 to 2000 frequent one that causes severe CNS infections
was reported as 6 to 11 cases per 1,000,000 pop- among the non-polioviruses.46,47 Enteroviruses
ulation aged less than 15 years (12–29 per are responsible for large-scale, periodic epidemics
1,000,000 agedStructured Imaging Approach for Viral Encephalitis 49
Fig. 4. Influenza-associated encephalopathy (IAE) manifested as ANEC (acute necrotizing encephalopathy of
childhood) (A, B) T2-weighted and FLAIR images show bilateral symmetric high signal in the thalamus. (C, D)
Focal diffusion-restricted portion is noted in the center of the lesions.
positive ratio was significantly higher than other The MR imaging changes in rabies may be due to
sequences.43 In patients with aseptic meningitis, viral infection per se, host response, or complica-
findings are nonspecific; however, subdural effu- tions such as hypoxia, bleeding, shock, and meta-
sion, meningeal enhancement, and hydrocephalus bolic abnormalities. Rabies encephalitis may show
can be indirect signs.49 T2-hyperintense signal changes in the brainstem,
Acute flaccid paralysis associated with hippocampus, limbic cortex, thalamus, or hypothal-
Enterovirus-D68 can demonstrate diffuse spinal amus regions (Fig. 6). It can also involve the spinal
cord edema, affecting the entire gray matter, cord, and the degree of abnormality may vary
evolving over several days with T2-hyperintensity widely depending on the stage of progression. In
restricted to the anterior horn.44 In addition, the late stages, the lesion may increase due to the
contrast enhancement of the caudal roots and alteration in the blood–brain barrier.36,38 Rabies en-
sometimes of the cranial nerves can be seen. cephalitis typically shows almost exclusive gray
matter involvement in ADEM, which predominantly
involves white matter.
Rabies For the rare survivors, mainly those promptly
Among the bullet-shaped Rhabdoviridae family, treated with immunoglobulin and rabies vaccine,
at least six serotypes in the genus Lyssavirus MR imaging showed progressive brain atrophy, leu-
cause diseases clinically related to rabies, koencephalopathy, persistent T2 hyperintensities in
including rabies virus and multiple bat viruses.50 the basal ganglia, and gliosis. In addition, some
The viruses can be transmitted through the bite have reported blooming artifacts in bilateral basal
of infected bats or other infected mammals, ganglia suggestive of mineralization.39
resulting in fever, agitation, excessive salivation,
and hydrophobia. Rabies has a dismal prognosis
Splenial Location
and limited treatment options once symptoms set
in, with only 12 reported survivors globally.51 Rotavirus
Diagnosis can be made by skin biopsy with PCR Rotavirus is a leading cause of acute gastroenter-
testing.52 itis worldwide, with a high hospitalization rate and
Fig. 5. Enterovirus encephalitis (A–C) T2-weighted images shows typical bilateral hyperintensity in dorsal pons
tegmentum area, midbrain, and medulla (arrows).
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.50 Ramli & Bae
Fig. 6. Rabies encephalitis (A, B) T2-weighted images show typical involvement of bilateral basal ganglia and
midbrain (arrows). (C) On sagittal T2-weighted image, T2-high signal lesions involving medulla and upper cervical
spinal cord are seen. Courtesy of Jitender Saini, MD, NIMHANS, Bengaluru, Karnataka
mortality for children under 5 years of age.53 abnormalities are not specific. They can be caused
Simultaneous CNS involvement has been reported by other infectious agents, including Epstein–Barr
in patients with rotavirus gastroenteritis. The clin- virus, Staphylococcus, Escherichia coli, and
ical findings include encephalopathy, febrile and noninfectious causes such as drug therapy, malig-
afebrile convulsions, hemorrhagic shock, Guil- nancy, metabolic disorders, and trauma.58
lain–Barré syndrome, and Reye syndrome after
primary intestinal infection.54,55 Vasculopathy and Ischemic Infarction in
Brain MR imaging can show hyperintensities in Children
the splenium of the corpus callosum and/or bilat-
Varicella-zoster virus
eral dentate nuclei on T2-weighted imaging or
VZV causes chickenpox (varicella) and shingles
DWI with diffusion restriction (Fig. 7). These le-
(zoster) and was once responsible for over 4
sions are reported to disappear rapidly, the short-
million infections in the United States annually. Af-
est being 12 days and the longest being
ter the resolution of the acute varicella episode,
51 days.56,57 Therefore, especially in pediatric
the virus can remain latent in the dorsal ganglia
AES cases with gastroenteritis, rotavirus encepha-
of the spine and reactivate with declining immu-
litis should be a differential diagnosis when MR im-
nity, causing herpes zoster, often complicated by
aging demonstrates reversible splenial and/or
post-herpetic neuralgia (chronic pain), VZV vascul-
dentate lesions. However, reversible splenial
opathy, meningoencephalitis, meningoradiculitis,
Fig. 7. Rotavirus encephalitis T2-weighted image (A), DWI (B), and ADC map (C) of a neonate show multifocal
white matter involvement with diffusion restriction including corpus callosum splenium and genu. (Courtesy
of S Kumar MD, Bangalore South, India.)
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.Structured Imaging Approach for Viral Encephalitis 51
Fig. 8. Varicella-zoster virus (VZV) related vasculopathy (A–C) Axial DWI and coronal FLAIR image demonstrate
multifocal acute infarctions with restricted diffusion in left globus pallidus, left occipital cortex and frontal white
matter. (D) MR angiography (MRA) shows several short stenosis at left M1 and A1 segments (arrows).
cerebellitis, myelopathy, and ocular disease.59,60 VZV meningitis may also present as normal
In addition to CSF analysis, other pathogen tests, brain images, or very rarely, it can cause rhomben-
including virology tests, antibody detection, and cephalomyelitis involving the pons and spinal
molecular biology tests, may help confirm VZV cord, with T2-/FLAIR-high signal and variable
encephalitis.61 contrast enhancement.64 The involved cranial
In children, VZV vasculopathy accounts for 31% nerves (trigeminal, facial, and/or vestibuloco-
of all arterial ischemic strokes; moreover, stroke chlear) can be enhanced.65
was preceded by chickenpox in 44% of children
with transient cerebral arteriopathy.61 Ischemic le-
sions involving gray–white matter junctions and Variable Imaging Pattern
deep gray matter of the thalamus could also be Dengue virus
seen60 (Fig. 8). Angiography revealed abnormal- The Aedes mosquito transmits multiple serotypes
ities in 70% of subjects, with large and small ar- of DENV, which is prevalent in 128 countries, with
teries involved in 50%, with small arteries only in 2.5 billion individuals at risk each year.66 Three neu-
37% and large arteries only in 13%.60 Other com- ropathogenic mechanisms are associated with
plications of VZV vasculopathy include cerebral DENV infection: (1) invasion of the CNS and periph-
aneurysm, subarachnoid and intracerebral hemor- eral nervous system leading to meningitis, enceph-
rhage, ectasia, and dissection.61 The DWI image alitis, myelitis, and paresis; (2) metabolic and
can detect ischemic lesions associated with VZV vascular disorders leading to encephalopathy,
vasculopathy, and the GRE image can detect vasculitis, and bleeding in the CNS; and (3)
hemorrhagic lesions.62 Also, DWI can be better immune-mediated dengue syndromes, including
than conventional MR imaging for spinal cord ADEM, neuromyelitis optica, neuritis, myelitis, en-
involvement to detect spinal cord ischemia and cephalopathy, and Guillain–Barré syndrome.67
infarction.63 Therefore, MR imaging can play a sig- The diagnostic criteria for dengue encephalitis
nificant role in diagnosing neurologic manifesta- include fever, AES symptoms, and the detection
tions of VZV, and DWI and GRE sequences of anti-dengue IgM antibodies or genomic materials
should be included. in the serum or CSF.68
Fig. 9. Dengue encephalitis (A, B) T2-weighted and FLAIR images show multifocal lesions in bilateral basal
ganglia (arrows) and cerebral white matter. Hypointense hemorrhage on coronal T2*-gradient recalled echo im-
age (C) and diffuse leptomeningeal enhancement on coronal contrast-enhanced T1-weighted image are noted
(D).
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.52 Ramli & Bae
Fig. 10. Classic progressive multifocal leukoencephalopathy (PML) and PML-IRIS (A, B) Classic PML shows focal T2-
and FLAIR-hyperintense lesion without mass effect or contrast enhancement located in the subcortical white mat-
ter. Unlike classic PML, (C–E) PML-IRIS shows multifocal T2-and FLAIR-hyperintense lesions in bilateral cerebral
subcortical white matter with contrast enhancement.
Neuroimaging in dengue encephalitis shows Readers are encouraged to refer to article 9 for neu-
variable features, with normal findings in most roimaging features of HIV.
cases. Multifocal confluent and ill-defined
increased T2-weighted signal abnormalities are
reported in the cerebral white matter, hippocam- Progressive Multifocal Leukoencephalopathy
pus, basal ganglia, and thalamus, with or without Caused by John Cunningham Virus
cortical involvement.66,69 There can be hemor-
rhage, edema, patchy focal diffusion restriction, MR imaging is the modality of choice for the diag-
and meningeal enhancement (Fig. 9).70 nosis of PML. Typical PML lesions frequently
Most post-dengue ADEM cases are similar to involve subcortical hemispheric white matter (Fig
ADEM from other etiologies, with white- and gray 10), but they can also affect cerebellar white mat-
matter abnormalities on T2-weighted and FLAIR ter or gray matter structures, such as basal ganglia
images. These demyelinating lesions may be or thalamus. The lesions can be multifocal,
disseminated to multiple sites, including the peri- showing T1-low, T2-and FLAIR-high signal inten-
ventricular area, corona radiata, internal capsule, sities. Classic PML does not usually show any
and cerebral peduncles, possibly showing hemor- mass effect or contrast enhancement. However,
rhagic foci.69,71 inflammatory PML or progressive multifocal leu-
koencephalopathy immune reconstitution inflam-
SUBACUTE OR CHRONIC COURSE matory syndrome (PML-IRIS) lesions (see Fig 10)
can show substantial contrast enhancement due
Viruses can rarely present with a subacute or to inflammation and blood–brain barrier disruption.
chronic course, particularly human immunodefi- It can also accompany edema, swelling, or mass
ciency virus (HIV) and associated complications. effects.72
Fig. 11. Subacute sclerosing panencephalitis (SSPE) (A, B) Multifocal T2-and FLAIR-high signal lesions are demon-
strated in bilateral periventricular and subcortical white matter.
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.Structured Imaging Approach for Viral Encephalitis 53
Table 2
Summary of MR imaging patterns in typical acute viral encephalitis
Preferential Anatomic
Involvement Viral Pathogens Radiological Features Clinical Features
Temporal lobe Herpes simplex Typically insula and HSV-1 infection in adults,
virus type-1 limbic system, frontal HSV-2 in children
lobe. More widespread
in HSV-2
Human herpes Typically exclusive mesial Immunocompromised
virus type-6 temporal lobe patients
Bilateral thalami Japanese May show hemorrhage Especially children in
encephalitis endemic area
virus
Influenza virus Acute necrotizing Antecedent respiratory
encephalopathy infection especially in
children
Brainstem Enterovirus Medulla, pons, midbrain, Associated with
callosal splenium, and hand–foot–mouth
ventral spinal cord disease or outbreaks
in children
Rabies virus Brainstem, hippocampus, History of rabid animal
limbic system, bite
hypothalamic and spinal
cord (predominant in
gray matter)
Splenium of corpus Rotavirus Typically reversible on DWI Associated with acute
callosum gastroenteritis in
children
Subacute Sclerosing Panencephalitis Caused cortex, corpus callosum, and deep structures
by the Measles Virus can be involved in the more advanced stages.
These lesions may show contrast enhancement
Subacute sclerosing panencephalitis (SSPE) is a
and high signal intensities on DWI.79 In the
rare, progressive, chronic inflammatory encephali-
chronic phase, the lesions may disappear, new
tis secondary to a measles virus infection that
lesions can occur, and progressive brain atrophy
causes widespread demyelination in children and
can develop.
adolescents.73 In the developed world, the preva-
lence of SSPE has steadily declined since the
introduction of the measles virus vaccine in the SUMMARY
1960s. The incidence of SSPE is inversely related Clinical diagnosis of the cause of viral encephalitis
to the rate of measles vaccination.74 Overall, 4 to can be difficult. Nonetheless, an accurate and
11 cases of SSPE are expected for every timely diagnosis is essential to guide management
100,000 cases of measles, with a higher incidence and appropriate treatment. In this article, a diag-
among children aged less than 5 years (18/ nostic algorithm based on MR imaging features
100,000, compared with 1.1/100,000 after 5 years is proposed to systematically aid the differential
of age).75 The highest incidence of SSPE relative to diagnosis of viral encephalitis. The typical MR im-
measles is reported in the Middle East, where the aging patterns should not be overlooked (Table 2).
rate is 360/100,000 in individuals infected before The proposed MR imaging findings must be
1 year of age. The incidence varies dramatically interpreted in the correct clinical context, and
depending on the measles infection’s age and thus, making a diagnosis solely based on the MR
vaccination status.76 imaging findings has limitations. Nonetheless, us-
MR imaging findings mainly depend on the dis- ing this simple systemic approach based on the vi-
ease duration.77 MR imaging findings can be sual assessment of structural imaging can help
normal in the early stages. As the disease pro- both radiologists and clinicians evaluate MR imag-
gresses, periventricular and subcortical T2-high ing to support the correct diagnosis. We believe
signal lesions are seen78 (Fig. 11). The cerebral that future validation of the diagnostic algorithm
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.54 Ramli & Bae
is necessitated. Future studies using advanced and Neurological Complications in Japan and the
techniques, such as automated classifier algo- Rest of the World. Int J Mol Sci 2019;20(20):5201.
rithms may play a complementary role in clinical 9. Kumar R. Understanding and managing acute en-
practice. cephalitis. F1000Res 2020;9.
10. Dalmau J, Graus F, Villarejo A, et al. Clinical analysis
CLINICS CARE POINTS of anti-Ma2-associated encephalitis. Brain 2004;
127(Pt 8):1831–44.
11. Jayaraman K, Rangasami R, Chandrasekharan A.
Magnetic Resonance Imaging Findings in Viral En-
Viruses can cause central nervous system dis- cephalitis: A Pictorial Essay. J Neurosci Rural Pract
ease via three broad mechanisms: aseptic 2018;9(4):556–60.
meningitis, encephalitis, and immune- 12. Granerod J, Ambrose HE, Davies NW, et al. Causes
mediated processes; adopting a structured of encephalitis and differences in their clinical pre-
but simplified diagnostic approach based on sentations in England: a multicentre, population-
typical MR imaging patterns can assist in sug- based prospective study. Lancet Infect Dis 2010;
gesting a viral pathogen, even though there
10(12):835–44.
is considerable overlap.
13. Aurelius E, Johansson B, Sköldenberg B, et al. En-
By aggregating imaging, clinical and labora- cephalitis in immunocompetent patients due to her-
tory evidence, radiologists can contribute to pes simplex virus type 1 or 2 as determined by
multidisciplinary teams caring for patients,
type-specific polymerase chain reaction and anti-
leading to the appropriate treatment and
body assays of cerebrospinal fluid. J Med Virol
better outcomes.
1993;39(3):179–86.
14. Piret J, Boivin G. Immunomodulatory Strategies in
Herpes Simplex Virus Encephalitis. Clin Microbiol
DISCLOSURE Rev 2020;33(2).
15. Kolski H, Ford-Jones EL, Richardson S, et al. Etiol-
The authors have nothing to disclose.
ogy of acute childhood encephalitis at The Hospital
for Sick Children, Toronto, 1994-1995. Clin Infect Dis
1998;26(2):398–409.
REFERENCES
16. Glaser CA, Honarmand S, Anderson LJ, et al.
1. Kar A, Dhanaraj M, Dedeepiya D, et al. Acute Beyond viruses: clinical profiles and etiologies asso-
encephalitis syndrome following scrub typhus ciated with encephalitis. Clin Infect Dis 2006;43(12):
infection. Indian J Crit Care Med 2014;18(7): 1565–77.
453–5. 17. Venkatesan A, Tunkel AR, Bloch KC, et al. Case def-
2. Granerod J, Tam CC, Crowcroft NS, et al. Challenge initions, diagnostic algorithms, and priorities in en-
of the unknown. A systematic review of acute en- cephalitis: consensus statement of the international
cephalitis in non-outbreak situations. Neurology encephalitis consortium. Clin Infect Dis 2013;57(8):
2010;75(10):924–32. 1114–28.
3. Boucher A, Herrmann JL, Morand P, et al. Epidemi- 18. Domingues RB, Fink MC, Tsanaclis AM, et al. Diag-
ology of infectious encephalitis causes in 2016. Med nosis of herpes simplex encephalitis by magnetic
Mal Infect 2017;47(3):221–35. resonance imaging and polymerase chain reaction
4. Bookstaver PB, Mohorn PL, Shah A, et al. Manage- assay of cerebrospinal fluid. J Neurol Sci 1998;
ment of Viral Central Nervous System Infections: A 157(2):148–53.
Primer for Clinicians. J Cent Nerv Syst Dis 2017;9. 19. Stahl JP, Mailles A. Herpes simplex virus enceph-
1179573517703342. alitis update. Curr Opin Infect Dis 2019;32(3):
5. Bechter K. Encephalitis, Mild Encephalitis, Neuro- 239–43.
progression, or Encephalopathy-Not Merely a Ques- 20. Renard D, Nerrant E, Lechiche C. DWI and FLAIR
tion of Terminology. Front Psychiatry 2019;9:782. imaging in herpes simplex encephalitis: a compara-
6. Goel S, Chakravarti A, Mantan M, et al. Diagnostic tive and topographical analysis. J Neurol 2015;
Approach to Viral Acute Encephalitis Syndrome 262(9):2101–5.
(AES) in Paediatric Age Group: A Study from New 21. Singh TD, Fugate JE, Hocker S, et al. Predictors of
Delhi. J Clin Diagn Res 2017;11(9):Dc25–dc29. outcome in HSV encephalitis. J Neurol 2016;
7. Chaudhuri A, Kennedy PG. Diagnosis and treatment 263(2):277–89.
of viral encephalitis. Postgrad Med J 2002;78(924): 22. Sili U, Kaya A, Mert A. Herpes simplex virus en-
575–83. cephalitis: clinical manifestations, diagnosis and
8. Gonzalez G, Carr MJ, Kobayashi M, et al. Entero- outcome in 106 adult patients. J Clin Virol 2014;
virus-Associated Hand-Foot and Mouth Disease 60(2):112–8.
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.Structured Imaging Approach for Viral Encephalitis 55
23. Fida M, Hamdi AM, Bryson A, et al. Long-term Out- 39. Rao A, Pimpalwar Y, Mukherjee A, et al. Serial brain
comes of Patients With Human Herpesvirus 6 En- MRI findings in a rare survivor of rabies encephalitis.
cephalitis. Open Forum Infect Dis 2019;6(7):ofz269. Indian J Radiol Imaging 2017;27(3):286–9.
24. Santpere G, Telford M, Andrés-Benito P, et al. The 40. Sugaya N. Influenza-associated encephalopathy in
Presence of Human Herpesvirus 6 in the Brain in Japan. Semin Pediatr Infect Dis 2002;13(2):79–84.
Health and Disease. Biomolecules 2020;10(11): 41. Fujimoto S, Kobayashi M, Uemura O, et al. PCR on
1520. cerebrospinal fluid to show influenza-associated
25. Eimer WA, Vijaya Kumar DK, Navalpur acute encephalopathy or encephalitis. Lancet
Shanmugam NK, et al. Alzheimer’s Disease-Associ- 1998;352(9131):873–5.
ated b-Amyloid Is Rapidly Seeded by Herpesviridae 42. Chen YC, Lo CP, Chang TP. Novel influenza A
to Protect against Brain Infection. Neuron 2018; (H1N1)-associated encephalopathy/encephalitis
99(1):56–63.e3. with severe neurological sequelae and unique im-
26. Noguchi T, Yoshiura T, Hiwatashi A, et al. CT and MRI age features–a case report. J Neurol Sci 2010;
findings of human herpesvirus 6-associated en- 298(1–2):110–3.
cephalopathy: comparison with findings of herpes 43. Lian ZY, Huang B, He SR, et al. Diffusion-weighted
simplex virus encephalitis. AJR Am J Roentgenol imaging in the diagnosis of enterovirus 71 encepha-
2010;194(3):754–60. litis. Acta Radiol 2012;53(2):208–13.
27. Handley G, Hasbun R, Okhuysen P. Human herpes- 44. Maloney JA, Mirsky DM, Messacar K, et al. MRI find-
virus 6 and central nervous system disease in ings in children with acute flaccid paralysis and cra-
oncology patients: A retrospective case series and nial nerve dysfunction occurring during the 2014
literature review. J Clin Virol 2021;136:104740. enterovirus D68 outbreak. AJNR Am J Neuroradiol
28. Noguchi T, Mihara F, Yoshiura T, et al. MR imaging of 2015;36(2):245–50.
human herpesvirus-6 encephalopathy after hemato- 45. Hixon AM, Frost J, Rudy MJ, et al. Understanding
poietic stem cell transplantation in adults. AJNR Am Enterovirus D68-Induced Neurologic Disease: A
J Neuroradiol 2006;27(10):2191–5. Basic Science Review. Viruses 2019;11(9):821.
29. Yassin A, Al-Mistarehi AH, El-Salem K, et al. Clinical, 46. World Health Organization. Regional Office for the
radiological, and electroencephalographic features Western, P., A guide to clinical management and
of HHV-6 encephalitis following hematopoietic stem public health response for hand, foot and mouth dis-
cell transplantation. Ann Med Surg (Lond) 2020;60: ease (HFMD). Manila: WHO Regional Office for the
81–6. Western Pacific; 2011.
30. Liu D, Wang X, Wang Y, et al. Detection of EBV and 47. Casas-Alba D, de Sevilla MF, Valero-Rello A, et al.
HHV6 in the Brain Tissue of Patients with Rasmus- Outbreak of brainstem encephalitis associated with
sen’s Encephalitis. Virol Sin 2018;33(5):402–9. enterovirus-A71 in Catalonia, Spain (2016): a clinical
31. Meng Q, Zou Y-L, Bu H, et al. Imaging and cytolog- observational study in a children’s reference centre
ical analysis of 92 patients with Japanese encepha- in Catalonia. Clin Microbiol Infect 2017;23(11):
litis. Neuroimmunology and Neuroinflammation 874–81.
2014;1(-1):29–34. 48. Jones E, Pillay TD, Liu F, et al. Outcomes following
32. Misra UK, Kalita J. Overview: Japanese encephali- severe hand foot and mouth disease: A systematic
tis. Prog Neurobiol 2010;91(2):108–20. review and meta-analysis. Eur J paediatric Neurol
33. Umenai T, Krzysko R, Bektimirov TA, et al. Japanese 2018;22(5):763–73.
encephalitis: current worldwide status. Bull World 49. Li J, Chen F, Liu T, et al. MRI findings of neurological
Health Organ 1985;63(4):625–31. complications in hand-foot-mouth disease by
34. Zheng Y, Li M, Wang H, et al. Japanese encephalitis enterovirus 71 infection. Int J Neurosci 2012;
and Japanese encephalitis virus in mainland China. 122(7):338–44.
Rev Med Virol 2012;22(5):301–22. 50. Hankins DG, Rosekrans JA. Overview, prevention,
35. Helfferich J, Knoester M, Van Leer-Buter CC, et al. and treatment of rabies. Mayo Clin Proc 2004;
Acute flaccid myelitis and enterovirus D68: lessons 79(5):671–6.
from the past and present. Eur J Pediatr 2019; 51. Netravathi M, Udani V, Mani Rs, et al. Unique clinical
178(9):1305–15. and imaging findings in a first ever documented
36. Pleasure SJ, Fischbein NJ. Correlation of clinical PCR positive rabies survival patient: A case report.
and neuroimaging findings in a case of rabies en- J Clin Virol 2015;70:83–8.
cephalitis. Arch Neurol 2000;57(12):1765–9. 52. Mahadevan A, Suja MS, Mani RS, et al. Perspectives
37. Chuang YY, Huang YC. Enteroviral infection in neo- in Diagnosis and Treatment of Rabies Viral Enceph-
nates. J Microbiol Immunol Infect 2019;52(6):851–7. alitis: Insights from Pathogenesis. Neurotherapeu-
38. Kalita J, Bhoi SK, Bastia JK, et al. Paralytic rabies: tics 2016;13(3):477–92.
MRI findings and review of literature. Neurol India 53. Naghavi M, W.H., Lozano R, et al. Global, regional,
2014;62(6):662–4. and national age-sex specific all-cause and cause-
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.56 Ramli & Bae
specific mortality for 240 causes of death, 1990- 66. Li GH, Ning ZJ, Liu YM, et al. Neurological Manifes-
2013: a systematic analysis for the Global Burden tations of Dengue Infection. Front Cell Infect Micro-
of Disease Study 2013. Lancet 2015;385(9963): biol 2017;7:449.
117–71. 67. Almeida Bentes A, Kroon EG, Romanelli RMC.
54. Lynch M, Lee B, Azimi P, et al. Rotavirus and central Neurological manifestations of pediatric arboviral in-
nervous system symptoms: cause or contaminant? fections in the Americas. J Clin Virol 2019;116:
Case reports and review. Clin Infect Dis 2001; 49–57.
33(7):932–8. 68. Soares C, Puccioni-Sohler M. Dengue encephalitis:
55. Abe T, Kobayashi M, Araki K, et al. Infantile convul- Suggestion for case definition. J Neurol Sci 2011;
sions with mild gastroenteritis. Brain Dev 2000;22(5): 306(1):165.
301–6. 69. Wan Sulaiman WA, Inche Mat LN, Hashim HZ, et al.
56. Li C-Y, Li C-HJNA. Probable etiology of mild enceph- Acute disseminated encephalomyelitis in dengue
alopathy with reversible isolated lesions in the viral infection. J Clin Neurosci 2017;43:25–31.
corpus callosum in children: A review of 20 cases 70. Jugpal TS, Dixit R, Garg A, et al. Spectrum of find-
from northern China 2018;23(2):153–8. ings on magnetic resonance imaging of the brain
57. Paketçi C, Edem P, Okur D, et al. Rotavirus enceph- in patients with neurological manifestations of
alopathy with concomitant acute cerebellitis: report dengue fever. Radiol Bras 2017;50(5):285–90.
of a case and review of the literature. Turk J Pediatr
71. Sundaram C, Uppin SG, Dakshinamurthy KV, et al.
2020;62(1):119–24.
Acute disseminated encephalomyelitis following
58. Starkey J, Kobayashi N, Numaguchi Y, et al.
dengue hemorrhagic fever. Neurol India 2010;
Cytotoxic Lesions of the Corpus Callosum That
58(4):599–601.
Show Restricted Diffusion: Mechanisms, Causes,
72. Cortese I, Reich DS, Nath A. Progressive multifocal
and Manifestations. Radiographics 2017;37(2):
leukoencephalopathy and the spectrum of JC vi-
562–76.
rus-related disease. Nat Rev Neurol 2021;17(1):
59. Shaw J, Gershon AA. Varicella Virus Vaccination in
37–51.
the United States. Viral Immunol 2018;31(2):96–103.
73. Cece H, Tokay L, Yildiz S, et al. Epidemiological find-
60. Nagel MA, Gilden D. Neurological complications of
ings and clinical and magnetic resonance presenta-
varicella zoster virus reactivation. Curr Opin Neurol
tions in subacute sclerosing panencephalitis. J Int
2014;27(3):356–60.
Med Res 2011;39(2):594–602.
61. Gilden D, Cohrs RJ, Mahalingam R, et al. Varicella
74. Anlar B, Köse G, Gürer Y, et al. Changing epidemi-
zoster virus vasculopathies: diverse clinical manifes-
ological features of subacute sclerosing panence-
tations, laboratory features, pathogenesis, and treat-
phalitis. Infection 2001;29(4):192–5.
ment. Lancet Neurol 2009;8(8):731–40.
62. Prelack MS, Patterson KR, Berger JR. Varicella zos- 75. Campbell H, Andrews N, Brown KE, et al. Review of
ter virus rhombencephalomyelitis following radiation the effect of measles vaccination on the epidemi-
therapy for oropharyngeal carcinoma. J Clin Neuro- ology of SSPE. Int J Epidemiol 2007;36(6):1334–48.
sci 2016;25:164–6. 76. Zilber N, Kahana E. Environmental risk factors for
63. Orme HT, Smith AG, Nagel MA, et al. VZV spinal subacute sclerosing panencephalitis (SSPE). Acta
cord infarction identified by diffusion-weighted MRI Neurol Scand 1998;98(1):49–54.
(DWI). Neurology 2007;69(4):398–400. 77. Gutierrez J, Issacson RS, Koppel BS. Subacute
64. Becerra JC, Sieber R, Martinetti G, et al. Infection sclerosing panencephalitis: an update. Dev Med
of the central nervous system caused by varicella Child Neurol 2010;52(10):901–7.
zoster virus reactivation: a retrospective case se- 78. Tuncay R, Akman-Demir G, Gökyigit A, et al. MRI in
ries study. Int J Infect Dis 2013;17(7):e529–34. subacute sclerosing panencephalitis. Neuroradi-
65. Inagaki A, Toyoda T, Mutou M, et al. Ramsay Hunt ology 1996;38(7):636–40.
syndrome associated with solitary nucleus, spinal 79. Oguz KK, Celebi A, Anlar B. MR imaging, diffusion-
trigeminal nucleus and tract, and vestibular nucleus weighted imaging and MR spectroscopy findings in
involvement on sequential magnetic resonance im- acute rapidly progressive subacute sclerosing pan-
aging. J Neurovirol 2018;24(6):776–9. encephalitis. Brain Dev 2007;29(5):306–11.
Descargado para Biblioteca Medica Hospital México (bibliomexico@gmail.com) en National Library of Health
and Social Security de ClinicalKey.es por Elsevier en febrero 20, 2023. Para uso personal exclusivamente. No se
permiten otros usos sin autorización. Copyright ©2023. Elsevier Inc. Todos los derechos reservados.You can also read

















































