Strain-Guided Management of Potentially Cardiotoxic Cancer Therapy - American Society of Echocardiography
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

JOURNAL OF THE AMERICAN COLLEGE OF CARDIOLOGY VOL. 77, NO. 4, 2021
ª 2021 BY THE AMERICAN COLLEGE OF CARDIOLOGY FOUNDATION
PUBLISHED BY ELSEVIER
Strain-Guided Management of Potentially
Cardiotoxic Cancer Therapy
Paaladinesh Thavendiranathan, MD, SM,a,* Tomoko Negishi, MD,b,c,* Emily Somerset, MS,d
Kazuaki Negishi, MD, PHD,b,c Martin Penicka, MD, PHD,e Julie Lemieux, MD, MSC,f Svend Aakhus, MD, PHD,g
Sakiko Miyazaki, MD,h Mitra Shirazi, MD,i Maurizio Galderisi, MD, PHD,j,y Thomas H. Marwick, MBBS, PHD, MPH,b,k
on behalf of the SUCCOUR Investigatorsz
ABSTRACT
BACKGROUND In patients at risk of cancer therapy-related cardiac dysfunction (CTRCD), initiation of cardioprotective
therapy (CPT) is constrained by the low sensitivity of ejection fraction (EF) for minor changes in left ventricular (LV)
function. Global longitudinal strain (GLS) is a robust and sensitive marker of LV dysfunction, but existing observational
data have been insufficient to support a routine GLS-guided strategy for CPT.
OBJECTIVES This study sought to identify whether GLS-guided CPT prevents reduction in LVEF and development of
CTRCD in high-risk patients undergoing potentially cardiotoxic chemotherapy, compared with usual care.
METHODS In this international, multicenter, prospective, randomized controlled trial, 331 anthracycline-treated
patients with another heart failure risk factor were randomly allocated to CPT initiation guided by either $12% relative
reduction in GLS (n ¼ 166) or >10% absolute reduction of LVEF (n ¼ 165). Patients were followed for EF and
development of CTRCD (symptomatic EF reduction of >5% or >10% asymptomatic to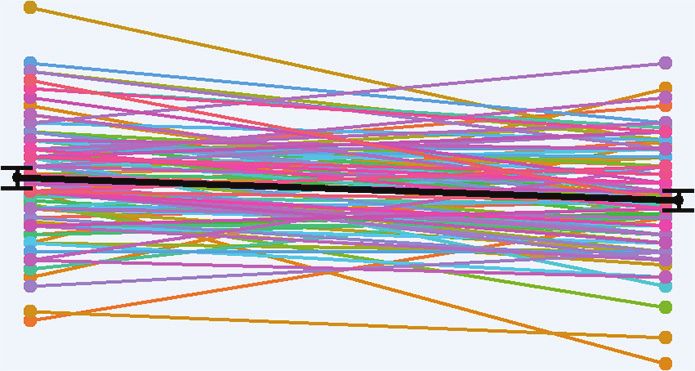
JACC VOL. 77, NO. 4, 2021 Thavendiranathan et al. 393
FEBRUARY 2, 2021:392–401 Strain-Guided Management
C traditional heart failure risk factors: age > 65
hemotherapy-related heart failure is an ABBREVIATIONS
important cause of morbidity and mortality years, type 2 diabetes mellitus, hypertension, AND ACRONYMS
in patients with cancer (1,2). Current preven- or previous cardiac injury (e.g., myocardial
2D = 2-dimensional
tion strategies include the use of fewer cardiotoxic infarction). Exclusion criteria were: 1) base-
3D = 3-dimensional
cancer treatment regimens, cardiovascular risk factor line LVEF of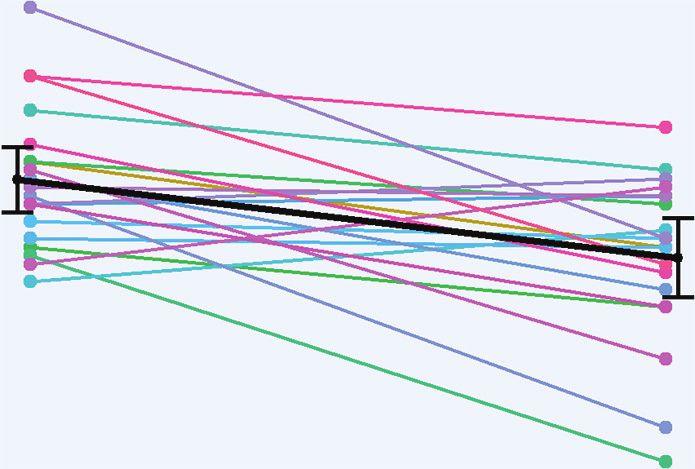
394 Thavendiranathan et al. JACC VOL. 77, NO. 4, 2021
Strain-Guided Management FEBRUARY 2, 2021:392–401
in all patients, and LV volumes and LVEF were appropriate. Primary outcome analyses were per-
measured offline (3DLVQ, EchoPAC, GE Medical Sys- formed on an intention-to-treat basis. Change in
tems, Milwaukee, Wisconsin), with an abnormal LVEF LVEF or GLS from baseline to 1-year follow-up be-
identified as 5% or available echocardiogram was used for analysis. The
asymptomatic drop of >10% in LVEF compared to primary outcome analysis was repeated with adjust-
baseline to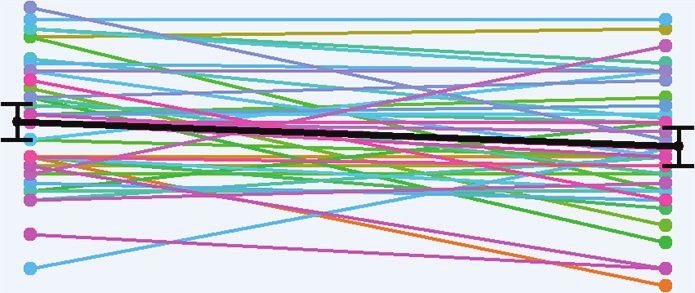
JACC VOL. 77, NO. 4, 2021 Thavendiranathan et al. 395
FEBRUARY 2, 2021:392–401 Strain-Guided Management
F I G U R E 1 CONSORT Flow Diagram
Enrollment Randomized (n = 331)
Allocation
GLS-guided surveillance (n = 166) EF-guided surveillance (n = 165)
• Received allocated intervention (n = 166) • Received allocated intervention (n = 165)
Follow-Up
Dropped-out (n = 12) Dropped-out (n = 12)
Withdrew consent (n = 4) Withdrew consent (n = 5)
Missing data or no images (n = 6) Missing data or no images (n = 5)
Lost to follow-up (n = 1) Lost to follow-up (n = 1)
Died (n = 1) Died (n = 1)
Analysis
Analyzed (n = 154) Analyzed (n = 153)
Of 331 randomized patients (of whom 166 were allocated to GLS-guided surveillance), 307 completed imaging follow-up. CONSORT ¼ Consolidated Standards of
Reporting Trials; EF ¼ ejection fraction; GLS ¼ global longitudinal strain.
therapy with trastuzumab. The median doxorubicin respectively. The trajectories of blood pressure and
equivalent dose was 218 mg/m 2 (interquartile range heart rate over the follow-up period are provided in
[IQR]: 200 to 241 mg/m 2), with no significant differ- Supplemental Figure 1. At the 1-year follow-up visit,
ence between the arms (EF-guided: 210 mg/m 2 [IQR: the LVEF was less in the EF-guided arm compared to
181 to 241 mg/m 2]; GLS-guided: 235 mg/m2 [IQR: 201 the GLS-guided arm (55 7% vs. 57 6%, respec-
to 241 mg/m 2]; p ¼ 0.29). A total of 174 (57%) patients tively; p ¼ 0.050), although a similar proportion had a
received radiation therapy to the chest; in 95 (55%), it new diagnosis of LVEF396 Thavendiranathan et al. JACC VOL. 77, NO. 4, 2021
Strain-Guided Management FEBRUARY 2, 2021:392–401
Figure 2. GLS-CTRCD occurred earlier and more
T A B L E 1 Baseline Characteristics of Patients Included in the Analysis
frequently that LVEF-CTRCD. Also, the trajectory of
EF Guided GLS Guided LVEF and GLS over the follow-up period in both arms
(n ¼ 153) (n ¼ 154) p Value
and the LVEF and GLS response after the respective
Age, yrs 54 (45–63) 53 (44–64) 0.820
diagnosis of CTRCD and initiation of CPT in each arm
Female 144 (94.1) 144 (93.5) >0.99
Race 0.290 based on site-specific measurements are shown in
European 104 (68.0) 97 (63.4) Supplemental Figures 3 and 4, respectively.
African 1 (0.7) 1 (0.7) We repeated the primary analysis using a per-
East Asian 31 (20.3) 43 (28.1) protocol approach, excluding 9 patients who either
South Asian 11 (7.2) 5 (3.3) had a significant reduction in LVEF meeting CTRCD
Other 6 (3.9) 7 (4.6)
criteria or a significant reduction in GLS in the GLS
Diabetes 25 (16.3) 14 (9.1) 0.061
arm before the 1-year follow-up but were not treated
Hypertension 46 (30.1) 43 (27.9) 0.710
Dyslipidemia 37 (24.2) 27 (17.5) 0.162
with CPT (either because of patient refusal to receive
Smoking* 44 (28.8) 46 (29.9) 0.900 CPT or missed recognition of a significant change at
Prior cardiovascular disease 14 (9.2) 16 (10.4) 0.850 the site). The proportion of patients meeting CTRCD
Beta-blocker 7 (4.6) 8 (5.2) >0.99 criteria at 1 year remained similar (14.1% in the EF-
ACE inhibitor or ARB 22 (14.4) 21 (13.6) 0.870 guided arm vs. 6.0% in the GLS-guided arm;
Statin 27 (17.6) 15 (9.7) 0.048
p ¼ 0.033), and the difference in the change in LVEF
Systolic blood pressure, mm Hg 122 (113–135) 125 (116–136) 0.550
was not significant (change of 0.27%; 95% CI: –1.35 to
Diastolic blood pressure, mm Hg 75 (70–80) 77 (70–80) 0.410
1.89; p ¼ 0.74).
Heart rate, beats/min 77 (70–85) 74 (66–85) 0.260
Cancer history
CARDIOTOXICITY TREATMENT. During follow-up,
Breast cancer 138 (90.2) 140 (90.9) 0.850
based on site EF or GLS measurements, 20 patients
Breast cancer characteristics
were treated for CTRCD in the EF-guided arm and 44
HER2þ 118 (85.5) 126 (90.0) 0.280
ER þ
79 (58.5) 81 (60.0) 0.900
patients in the GLS-guided arm. In the GLS-guided
PRþ 64 (47.8) 67 (49.6) 0.810 arm, 37 patients had an isolated reduction in GLS
Left sided 69 (50.7) 76 (54.3) 0.820 by $12%, and 7 patients met the GLS and LVEF CTRCD
Bilateral 6 (4.4) 5 (3.6) 0.820 criteria at the same time. The maximal doses of car-
Lymphoma 12 (7.8) 11 (7.1) 0.830 diac medications used to treat CTRCD in each arm are
Acute myelogenous leukemia 3 (2.0) 3 (1.9) >0.99
summarized in Table 3. There were no statistically
Echocardiographic parameters
significant differences in the maximal doses of ACE
Echocardiography pre-trastuzumab† 118 (77.1) 126 (81.8) 0.33
inhibitors/ARBs or beta-blocker achieved between the
Core laboratory measurement, %
3D LVEF 58 6 59 6 0.100 2 arms. The most common reasons for not achieving
GLS –20.4 2.5 –20.9 2.3 0.076 maximal doses include CTRCD being identified only
Site measurement, % at the final visit or inability to further up-titrate
3D LVEF 61 4 61 5 0.520 medications because of hypotension or bradycardia.
GLS –20.4 2.6 –20.7 2.4 0.270 Other than the patients who refused treatment with
cardiac medications, all other patients received at
Values are median (interquartile range), n (%), or mean SD. Clinical, cancer, cancer therapy, and cardiovascular
risk factors and cardiac imaging parameters are compared between the EF-guided and GLS-guided arms. least 1 of an ACE inhibitor/ARB or a beta-blocker.
*Smoking indicates prior or current smoking. †Refers to the proportion of patients who had baseline echocar-
diography performed after anthracycline but before trastuzumab; the remaining patients received baseline None of the patients had serious adverse events
imaging before any chemotherapy (i.e., before anthracyclines). related to the initiation of cardiac medications.
3D ¼ 3-dimensional; ACE ¼ angiotensin-converting enzyme, ARB ¼ angiotensin receptor blocker; EF ¼ ejection
fraction; ERþ ¼ estrogen receptor positive; GLS ¼ global longitudinal strain; HER2þ ¼ human epidermal growth In post hoc analysis, we examined the differences
factor receptor 2 positive; LVEF ¼ left ventricular ejection fraction; PRþ ¼ progesterone receptor positive. in core laboratory LVEF measurement between
baseline and the final visit in the patients who
developed CTRCD and received CPT in each arm and
measurements, during treatment, 20 patients (13.1%) those who did not develop CTRCD (Figure 2). In the
met LVEF-CTRCD criteria in the EF-guided arm, EF-guided arm (n ¼ 20), the reduction in LVEF was
whereas only 7 patients (4.5%) met criteria in the 9.1% (95% CI: 14.2% to 4.0%), whereas in the GLS arm
GLS-guided arm (p ¼ 0.013; RRR: 65%; 95% CI: 20% to (n ¼ 44), it was significantly lower at 2.9% (95% CI:
85%). All LVEF-CTRCD events in the GLS-guided arm 5.1% to 0.6%), with a difference of 6.2% (95% CI:
occurred simultaneously, with a $12% reduction in 11.8% to 0.7%; p ¼ 0.03). There was no significant
site measured GLS. The timing of CTRCD in each arm difference between the arms in the change in LVEF in
based on site 3D LVEF or GLS measurements and the those who did not develop CTRCD. Similarly, among
respective definitions are provided in Supplemental the patients who met the respective CTRCD criteria in
Downloaded for Anonymous User (n/a) at SARASOTA MEMORIAL HEALTH CARE SYSTEM from ClinicalKey.com by Elsevier on
September 21, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.JACC VOL. 77, NO. 4, 2021 Thavendiranathan et al. 397
FEBRUARY 2, 2021:392–401 Strain-Guided Management
T A B L E 2 Changes in LVEF and GLS Between Baseline and the 1-Year Follow-Up
EF Guided GLS Guided
LV Function, LV Function, Difference,
n % (95% CI) p Value* n % (95% CI) p Value* % (95% CI) p Value†
Core laboratory 3D EF, %
Baseline 153 58 (57 to 59) 154 59 (58 to 60) –1.2 (–2.6 to 0.2) 0.10
1 year 153 55 (54 to 56) 154 57 (56 to 58) –1.5 (–3.0 to 0.0) 0.05
1 year – baseline 153 –3.0 (–1.8 to –4.2)398 Thavendiranathan et al. JACC VOL. 77, NO. 4, 2021
Strain-Guided Management FEBRUARY 2, 2021:392–401
GLS-DRIVEN CARDIOPROTECTION. An important hin-
T A B L E 4 Reasons for Interruption or Discontinuation of Cancer Therapy
drance to routine clinical use of GLS for surveillance
Interruption Discontinuation has been the lack of robust data to suggest that a GLS-
EF Guided GLS Guided EF Guided GLS Guided based approach to surveillance and initiation of CPT
(n ¼ 8) (n ¼ 5) (n ¼ 5) (n ¼ 9)
reduces future CTRCD. Two prior studies have
Adverse events/serious adverse effects 1 0 1 2
explored a GLS-guided strategy to institute car-
Left ventricular dysfunction 1 3 1 2
Chemotherapy side effect 3 1 1 4
dioprotective medications. In a cohort of 159 women
Other reasons 3 1 2 1 with breast cancer treated with anthracyclines, tras-
tuzumab, or anthracyclines followed by trastuzumab,
There was no difference in the reasons for chemotherapy interruption between the 2 groups, p ¼ 0.44 or for patients who had a $11% reduction in GLS were fol-
chemotherapy discontinuation, p ¼ 0.91.
Abbreviations as in Table 1. lowed up for 6 additional months with initiation of a
beta-blocker at the discretion of the treating clini-
heart failure (4). This may provide a window of op- cians (11). Those who received a beta-blocker had an
portunity for early intervention (e.g., closer surveil- improvement in GLS and LVEF at follow-up, whereas
lance, CPT) to prevent future LVEF-CTRCD or heart those who were not treated had further decline in
failure. GLS is also well suited for routine monitoring both measures. More recently, in 116 women with
of myocardial function during cancer therapy because HER2 þ breast cancer receiving anthracyclines fol-
of its excellent interobserver, intraobserver, and test- lowed by trastuzumab, followed with echocardiogra-
retest variability and multicenter reproducibility phy every 3 months (12), patients who developed
compared to LVEF methods (9,10). GLS-CTRCD (GLS drop of >15%) or LVEF-CTRCD
F I G U R E 2 Baseline and Final Visit LVEF Measured by the Core Laboratory
GLS-Guided EF-Guided
80 Δ LVEF 2.9% (95% CI 0.6%, 5.1%) Δ LVEF 9.1% (95% CI 4.0%, 14.2%)
75
70
65
Received CPT
60
55
50
45
40
35
Core-Lab 3D-LVEF (%)
30
25
80 Δ LVEF 2.7% (95% CI 1.5%, 3.8%) Δ LVEF 2.1% (95% CI 1.0%, 3.2%)
75
70
Did Not Receive CPT
65
60
55
50
45
40
35
30
25
Baseline Final Visit Baseline Final Visit
Baseline and final visit core laboratory LVEF in the 2 arms divided based on those who were treated with CPT and those who were not. Among those who
received CPT (top), there was a larger reduction in LVEF between baseline and the final follow-up in the EF-guided arm, suggesting that a GLS-guided
strategy does prevent decrement in LVEF. Among those who did not receive CPT (bottom), the change in LVEF was similar between the 2 arms when
patients did not develop CTRCD. The black dots at baseline and the final visit represent the mean, and the bars represent 95% confidence intervals.
CPT ¼ cardioprotective therapy; LVEF ¼ left ventricular ejection fraction; other abbreviations as in Figure 1.
Downloaded for Anonymous User (n/a) at SARASOTA MEMORIAL HEALTH CARE SYSTEM from ClinicalKey.com by Elsevier on
September 21, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.JACC VOL. 77, NO. 4, 2021 Thavendiranathan et al. 399
FEBRUARY 2, 2021:392–401 Strain-Guided Management
C ENTR AL I LL U STRA T I O N Various Surveillance Strategies, Initiation of Cardioprotective
Therapy, and the Subsequent Response at the 1-Year Follow-Up
Baseline Echo surveillance 1-year
echocardiography during therapy follow-up
Potentially cardiotoxic chemotherapy
Abnormal
ejection fraction
Cardio-protection
65%
response Abnormal left
ventricular ejection
fraction response
39%
Abnormal 35%
Cancer
patient global longitudinal
strain response
61% Normal LVEF
response
Normal 66%
response
Thavendiranathan, P. et al. J Am Coll Cardiol. 2021;77(4):392–401.
Abnormal left ventricular ejection fraction was defined as400 Thavendiranathan et al. JACC VOL. 77, NO. 4, 2021
Strain-Guided Management FEBRUARY 2, 2021:392–401
HER2 þ breast cancer, in which cancer therapy is prognostic for a subsequent reduction in LVEF or
seldom interrupted unless the LVEF drops to below CTRCD (4,14–16). Given that sites were not blinded to
50%. Finally, in the patients who received only the study arm membership of the patients, there may
anthracycline, we still performed cardiac surveillance be bias in the local measurements of LVEF. However,
every 3 months to ensure the consistency of surveil- our primary outcome measures were based on blinded
lance for the entire cohort and based on prior data core laboratory measurements. We used 3D LVEF as
suggesting that CTRCD occurs within 3 to 6 months of our primary outcome measure, but whenever this
completion of anthracycline therapy (3). Cancer ther- measure was not possible because of image quality, we
apy would have already been completed by the time used 2D LVEF consistently at baseline and follow-up.
CTRCD was detected in this subgroup of patients. Although it would have been ideal to use 3D LVEF in
all patients, our approach is more consistent with
CLINICAL IMPLICATIONS. Our data support the
clinical care. Although there were multiple definitions
routine use of a GLS-guided strategy for cardiomy-
of CTRCD, we chose the Cardiac Review and Evaluation
opathy surveillance in anthracycline-treated patients
Committee criteria for our study (17). This reflects the
at increased risk of CTRCD (based on pre-existing
design of the SUCCOUR study before the publication of
conditions or adjunctive therapy) followed by care-
the American Society of Echocardiography or Euro-
ful initiation and titration of CPT to minimize the risk
pean Society of Echocardiography definitions of
of subsequent LVEF-CTRCD. This may be best
CTRCD. Furthermore, several studies have demon-
accomplished through cardio-oncology programs
strated the long-term prognostic significance of pa-
when available (13). The fact that a GLS-guided
tients developing Cardiac Review and Evaluation
strategy was effective in an international multi-
Committee–defined CTRCD (18,19). Given the fact
center setting is reassuring for the clinical translation
that our study was started before the approval of newer
of our findings. However, the adoption of GLS-guided
HER2-targeted therapies in early-stage breast cancer,
surveillance in routine practice does require the
we are unable to determine the impact of these specific
commitment of echocardiography laboratories and
therapies on the development of CTRCD. Finally, in
training of analyzing/reporting clinicians. All sites
women with HER2 þ breast cancer, there is a shift to-
participating in the SUCCOUR study first engaged in a
ward a greater use of non–anthracycline-based thera-
standardization process that we have previously
pies. Given our focus on anthracycline-treated patients,
described (10). Such standardization processes need
our findings are not generalizable to those who
to be performed and repeated periodically by indi-
are treated with non–anthracycline-based regimens.
vidual laboratories to ensure the accuracy and
reproducibility of GLS measurements. Finally, expe- CONCLUSIONS
rience is important in the precision of strain mea-
surements (10), and hence, sites adopting a GLS- The 12-month LVEF response for all patients
based approach should promote minimal annual receiving anthracycline-based cancer therapy at
volumes to maintain competency. elevated risk for CTRCD was not altered by a GLS-
based surveillance. However, GLS-guided CPT
STUDY STRENGTHS AND LIMITATIONS. To our knowl-
significantly reduced a meaningful fall of LVEF to the
edge, our study is the first randomized controlled
abnormal range. This paradox likely reflects the pro-
study to examine 2 separate approaches to cardiac
portion of patients that met the threshold for
surveillance followed by initiation of CPT in patients
receiving CPT—when patients receiving CPT were
receiving anthracycline-based cancer therapy to pre-
compared, those in the GLS-guided arm had a
vent LVEF-CTRCD. A major strength of our study is the
significantly lower reduction in LVEF at 1-year follow-
fact that decisions to initiate CPT were made by 28
up. These results support the use of GLS in surveil-
participating centers based on their local measure-
lance for CTRCD, but indicate that further work is
ments of both GLS and LVEF. This provides an
needed to better understand the threshold for CPT.
assessment of the real-life efficacy of a GLS- versus EF-
guided strategy to the initiation of cardioprotective ACKNOWLEDGMENTS The authors are indebted to
therapy and enhances the broader application of our the time and commitment of the trial participants. The
study findings. Our study was a randomized approach authors would like to acknowledge the sonographers
to a screening strategy as opposed to a treatment and coordinators at all sites for coordinating recruit-
strategy. Therefore, whether patients in the GLS arm ment, image collection and transfer, and follow-up.
who received CPT would have eventually developed The authors mourn the passing of Prof. Galderisi on
LVEF-CTRCD without treatment is unclear. However, March 27, 2020, and dedicate this report to his
existing data do suggest that GLS reduction is memory.
Downloaded for Anonymous User (n/a) at SARASOTA MEMORIAL HEALTH CARE SYSTEM from ClinicalKey.com by Elsevier on
September 21, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.JACC VOL. 77, NO. 4, 2021 Thavendiranathan et al. 401
FEBRUARY 2, 2021:392–401 Strain-Guided Management
AUTHOR DISCLOSURES PERSPECTIVES
This study was supported in part by a project grant (1119955) from
the National Health and Medical Research Council, Canberra, COMPETENCY IN PATIENT CARE AND PROCEDURAL
Australia, and an unrestricted grant from General Electric Healthcare,
SKILLS: Echocardiographic measurement of GLS can identify
Horten, Norway. At the Centre Hospitalier Universitaire (CHU) de
Québec site, the study was funded by the Fondation du CHU de
myocardial dysfunction early during anthracycline chemo-
Québec. Dr. Thavendiranathan is supported by the Canadian In- therapy and predict subsequent clinical cardiac dysfunction.
stitutes of Health Research New Investigator Award (147814), the In a randomized trial, a strategy of GLS-guided
Ontario Early Research Award, and a Canada Research Chair in
surveillance followed by angiotensin inhibitor and
Cardio-oncology. Dr. Negishi is supported by a Fellowship (award
reference no. 101868) from the National Heart Foundation of
beta-blocker therapy reduced the incidence of later
Australia. The authors have reported that they have no relationships cardiotoxicity.
relevant to the contents of this paper to disclose.
TRANSLATIONAL OUTLOOK: Further studies are needed to
ADDRESS FOR CORRESPONDENCE: Dr. Thomas H.
determine whether a GLS-guided approach to cardioprotective
Marwick, Baker Heart and Diabetes Institute, 75
therapy reduces the long-term risk of heart failure and improves
Commercial Road, Melbourne, Victoria 3004,
clinical outcomes.
Australia. E-mail: Tom.Marwick@bakeridi.edu.au.
Twitter: @BakerResearchAu, @dineshpmcc1.
REFERENCES
1. Abdel-Qadir H, Austin PC, Lee DS, et al. relevance and response to pharmacologic therapy. 16. Narayan HK, Finkelman B, French B, et al.
A population-based study of cardiovascular mor- J Am Coll Cardiol 2010;55:213–20. Detailed echocardiographic phenotyping in breast
tality following early-stage breast cancer. JAMA cancer patients: associations with ejection fraction
9. Lambert J, Lamacie M, Thampinathan B, et al.
Cardiol 2017;2:88–93. decline, recovery, and heart failure symptoms over
Variability in echocardiography and MRI for
3 years of follow-up. Circulation 2017;135:
2. Armenian SH, Xu L, Ky B, et al. Cardiovascular detection of cancer therapy cardiotoxicity. Heart
1397–412.
disease among survivors of adult-onset cancer: a 2020;106:817–23.
community-based retrospective cohort study. 17. Seidman A, Hudis C, Pierri MK, et al. Cardiac
10. Negishi T, Negishi K, Thavendiranathan P,
J Clin Oncol 2016;34:1122–30. dysfunction in the trastuzumab clinical trials
et al. Effect of experience and training on the
experience. J Clin Oncol 2002;20:1215–21.
3. Cardinale D, Colombo A, Bacchiani G, et al. Early concordance and precision of strain measure-
detection of anthracycline cardiotoxicity and ments. J Am Coll Cardiol Img 2017;10:518–22. 18. Romond EH, Jeong JH, Rastogi P, et al.
improvement with heart failure therapy. Circula- Seven-year follow-up assessment of cardiac
11. Negishi K, Negishi T, Haluska BA, Hare JL,
tion 2015;131:1981–8. function in NSABP B-31, a randomized trial
Plana JC, Marwick TH. Use of speckle strain to
comparing doxorubicin and cyclophosphamide
4. Oikonomou EK, Kokkinidis DG, Kampaktsis PN, assess left ventricular responses to cardiotoxic
followed by paclitaxel (ACP) with ACP plus
et al. Assessment of prognostic value of left chemotherapy and cardioprotection. Eur Heart J
trastuzumab as adjuvant therapy for patients
ventricular global longitudinal strain for early Cardiovasc Imaging 2014;15:324–31.
with node-positive, human epidermal growth
prediction of chemotherapy-induced cardiotox-
12. Santoro C, Esposito R, Lembo M, et al. Strain- factor receptor 2-positive breast cancer. J Clin
icity: a systematic review and meta-analysis. JAMA
oriented strategy for guiding cardioprotection Oncol 2012;30:3792–9.
Cardiol 2019;4:1007–18.
initiation of breast cancer patients experiencing
19. Yu AF, Flynn JR, Moskowitz CS, et al. Long-
5. Negishi T, Thavendiranathan P, Negishi K, cardiac dysfunction. Eur Heart J Cardiovasc Im-
term cardiopulmonary consequences of
Marwick TH, SUCCOR Investigators. Rationale and aging 2019;20:1345–52.
treatment-induced cardiotoxicity in survivors of
design of the strain surveillance of chemotherapy
13. Demissei BG, Adusumalli S, Hubbard RA, et al. ERBB2-positive breast cancer. JAMA Cardiol
for improving cardiovascular outcomes: the SUC-
Cardiology involvement in patients with breast 2020;5:309–17.
COUR trial. J Am Coll Cardiol Img 2018;11:
cancer treated with trastuzumab. J Am Coll Cardiol
1098–105.
CardioOnc 2020;2:179–89.
6. Swain SM, Whaley FS, Ewer MS. Congestive
14. Negishi K, Negishi T, Hare JL, Haluska BA,
heart failure in patients treated with doxorubicin: KEY WORDS cancer therapy–related
Plana JC, Marwick TH. Independent and incre-
a retrospective analysis of three trials. Cancer cardiac dysfunction, cardioprotective
mental value of deformation indices for prediction
2003;97:2869–79. therapy, global longitudinal strain, heart
of trastuzumab-induced cardiotoxicity. J Am Soc
failure
7. Thavendiranathan P, Abdel-Qadir H, Fischer HD, Echocardiogr 2013;26:493–8.
et al. Risk-imaging mismatch in cardiac imaging
15. Sawaya H, Sebag IA, Plana JC, et al. Assess-
practices for women receiving systemic therapy
ment of echocardiography and biomarkers for
for early-stage breast cancer: a population-based A PP END IX For supplemental tables and
the extended prediction of cardiotoxicity in
cohort study. J Clin Oncol 2018;36:2980–7. figures, as well as a full list of SUCCOUR
patients treated with anthracyclines, taxanes,
investigators, please see the online version of
8. Cardinale D, Colombo A, Lamantia G, et al. and trastuzumab. Circ Cardiovasc Imaging 2012;5:
this paper.
Anthracycline-induced cardiomyopathy: clinical 596–603.
Downloaded for Anonymous User (n/a) at SARASOTA MEMORIAL HEALTH CARE SYSTEM from ClinicalKey.com by Elsevier on
September 21, 2021. For personal use only. No other uses without permission. Copyright ©2021. Elsevier Inc. All rights reserved.You can also read

















































