Spring 2021 Governance Caucus - First Nations Health Council Reclaiming Our Connections - The Next Ten Years - First ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

First Nations Health Council
Spring 2021
Governance Caucus
Reclaiming Our Connections - The Next Ten Years
fnhc.ca1
As we prepare for the next full Gathering Wisdom in 2022, FNHC
engagement intends to hear directly from our Chiefs and leaders about
their most pressing concerns and ideas on themes of health legislation,
addressing racism and regionalization.
At Gathering Wisdom 2022, the First Nations Health Council will put forward
a resolution for endorsement by Chiefs to set forth a redefined governance
structure for the Council. We need your input, wisdom and guidance to renew
our advocacy priorities to meet this moment and realize our vision of health and
wellness transformation for our communities, families and people. Remember
that the original 2011 resolution set the stage for creation of the FNHA — a first
in Canada and one of only a few in the world.
Transformation is about self-determination. It’s about the multi-million-dollar
annual Funding Agreement for programs and services. It’s about providing
equitable access to services for First Nations people. It’s about a health
care experience free of racism. It’s about addressing — and changing — the
underlying determinants of health through a new 10-year strategy. At its heart,
our purpose is to strengthen our made-in-BC health governance structure to
better mobilize our Canada and BC partners and entrench Indigenous self-
determination in health within law.
The journey described in our “Reclaiming our Wellness — The Next Ten Years”
Governance Guidebook details the steps within the Engagement and Approval
Pathway to develop regional and provincial social determinant strategies
grounded in our #1 directive — Community-Driven, Nation-Based.
2
About this Workbook:
This workbook has been developed to support engagement at the
Spring 2021 Virtual Governance Caucuses.
Over the next 18 months, the First Nations Health Council (FNHC) will engage BC First Nations
Leaders on a series of timely issues. This engagement will be summarized and presented back
to participants in order to build consensus on the ongoing role of the FNHC, its mandate and
advocacy agenda.
As part of this process, the FNHC will be facilitating a dialogue between First Nations leaders, the
Province of BC and the Government of Canada on:
⚫ The Province of British Columbia’s Action Plan on the Implementation of the BC Declaration on the
Rights of Indigenous People; and
⚫ Federal Distinctions-Based Health Legislation.
The FNHC is committed to upholding the 7 Directives, including Directive #1: Community-Driven,
Nation-Based, by ensuring that BC First Nations leaders and caregivers are meaningfully included
in these important provincial and federal processes.
Complete the Workbook online via ENGAGE.FNHC.CA
3
Tell Us About Yourself
Personal Info:
Name_________________________________________________________________________________________________________________________
Community__________________________________________________________________________________________________________________
Do you identify with a Nation? ___________________________________________________________________________________________
Region/Sub-Region__________________________________________________________________________________________________________
Position_______________________________________________________________________________________________________________________
Were you in a leadership Role in 2013?__________________________________________________________________________________
In your community, would you be considered to be an:
o Elder
o Matriarch
o FNHC rep
o Hereditary Chief
o Knowledge Holder
o Other
o None of the above
4 First Nations Health Council | Reclaiming Our Connections: The Next Ten Years
Section One
Introduction:
The purpose of this Workbook document is to engage Chiefs, leaders, and caregivers attending the spring
2021 Virtual Regional Governance Caucus sessions on the ongoing role, mandate and advocacy agenda of
the First Nations Health Council. Workbooks are an integral tool of the Engagement and Approvals Pathway.
They are used to provide background on key governance topics and as a tool to engage leaders.
This work was launched at Gathering Wisdom for a Shared Journey X in January 2020, though delayed due to
the onset of the COVID-19 pandemic. The FNHC is restarting this process by asking leaders to provide their
wisdom, thoughts and perspective on the direction of the FNHC’s work.
The Spring 2021 Virtual Regional Governance Caucus session is part of an updated Engagement and
Approvals Pathway process. The FNHC will engage leadership throughout the next 18 months on the
following priority areas:
⚫ Spring 2021: DRIPA and Health Legislation
⚫ Fall 2021: Racism in Health Care
⚫ Spring 2022: Regionalization and Emergency Management
⚫ Fall 2022: Regional Partnership Accords and Tables
The FNHC will prepare a workbook for each round of Regional Caucus events to outline the topics of
engagement. The FNHC will also engage leaders on key governance principles and areas for future advocacy
with partners. This includes creating space the Spring 2021 Caucus for Chiefs and leaders and federal/
provincial governments to have direct facilitated engagement on:
⚫ British Columbia’s Action Plan on the Implementation of the BC Declaration on the Rights of
Indigenous People (DRIPA); and
⚫ Federal Distinctions Based Health Legislation.
Each Region’s specific feedback to this Workbook, along with their regional caucus discussions will be
summarized and reported back at each next caucus through Fall 2022. Chiefs and leaders will have the
opportunity to review the summary and provide additional feedback to ensure all views are reflected.
This collective engagement work will help inform and lead to a decision at the Gathering Wisdom for a
Shared Journey XII forum in Fall 2022, where Chiefs and Political leaders will review a draft consensus paper
and vote on a resolution to update the mandate of the FNHC.
This process will also inform ongoing work with partners on a Ten-Year Strategy on the Social
Determinants of Health.
Complete the Workbook online via ENGAGE.FNHC.CA 5Why Do This Work Now?
The topics of focus at each Regional Caucus
session have far-reaching impact on how health
Regarding health legislation, the FNHA
services are delivered to First Nations communities
and communities faced barriers in
in BC. To support this process, the FNHC will be
providing a coordinated response to
engaging Chiefs and leaders on its role in this
emergencies as the COVID-19 pandemic,
important work, as well as its overall structure to
wildfires and flooding. These barriers
inform the work on the Social Determinants of
included limited information-sharing,
Health and support a Community-driven, Nation-
challenges integrating into the provincial
based approach to health and wellness.
response, and receiving adequate funding
The development and implementation of UNDRIP to support community needs. Many of
legislation and federal distinctions-based health these challenges stem from the fact that
legislation provide opportunities to advance BC the FNHA did not have the legislated
First Nations’ interests across important areas of authority to operate in these areas.
health and wellness. There is risk in not carefully
Additionally, there are sections within
weighing options and advancing what is in the best
the Tripartite Framework Agreement on
interests of all BC First Nations in terms of First
First Nations Health (2011) which outline
Nations health service governance, oversight
the potential need for legislation as
and delivery.
the FNHA matures in its role within the
The implementation of DRIPA has far-reaching health system.
implications relating to BC First Nations health.
Finally, the In Plain Sight Report (2020) notes
Through DRIPA, there may be opportunities to:
that the development of indigenous health
⚫ To align laws related to BC First Nations legislation could serve to mitigate some of
health with UNDRIP. the challenges faced by the partners of the
made-in-BC Health Governance Structure
⚫ Further develop and strengthen Community-
in achieving cultural safety within the BC
driven, Nation-based relationships between
health system.
First Nations and BC.
⚫ Continue the conversation to improve health
and the Social Determinants of Health.
6 First Nations Health Council | Reclaiming Our Connections: The Next Ten YearsEngagement Pathway:
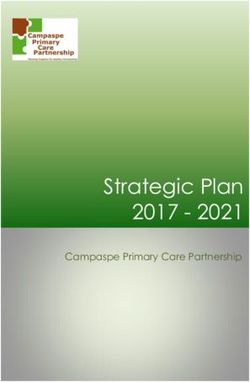
Through Resolution 2011-01, First Nations Figure 1
called upon the FNHC to design and describe
Reciprocal
a process for key decisions consistent Accountability
with the 7 Directives and the principle of A process of collecting
wisdom, advice, feedback and
Based on the
Reciprocal Accountability as adopted by First guidance from First Nations
in BC on a health and
Engagement, developing
options, questions, and
wellness matter.
Nations in the Consensus Paper. A process of
models and providing
those back to First
approval for the Nations in BC for further
Consensus reached engagement.
The FNHC is guided by the Engagement and among First Nations
in BC.
Approvals Pathway (Figure 1), which outlines
a process of engagement and dialogue
when making significant, province-wide
decisions regarding roles, responsibilities,
and mandates.
The Engagement and Approval Pathway
provides a process by which the FNHC and Based on the discussion
document, providing a
FNHA gather input and build consensus on A process of of dialogue and
amendment as required, to
description of the
common area(s) of
amend the Engagement
key decisions. It is a critical component of the Summary to build and
capture consensus among
agreement among BC
First Nations as it relates
to that health and
First Nations in BC.
ongoing success of the First Nations Health wellness matter.
Governance Structure. 7 Directives
The process is used for high level strategic decisions that concern
general direction, long-term goals, philosophies and values. They are
of significant importance and reach far into the future.
The dialogue on the ongoing role and function of the FNHC will be informed through discussion and
consideration of emerging priorities, including DRIPA and Health legislation, addressing systemic racism in
health, regionalization and emergency management and regional partnership accords and tables.
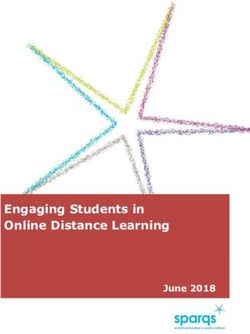
Complete the Workbook online via ENGAGE.FNHC.CA 7The engagement plan (see Figure 2 below) for this work includes the following steps:
1. Engagement:
a. Chiefs and leaders will have the opportunity to contribute to this process in a variety of ways, including:
⚫ Regional Caucus sessions;
⚫ Sub-regional sessions;
⚫ Working groups;
⚫ Nation Assemblies; and
⚫ Province-wide webinars.
2. Discussion Document:
b. A draft discussion document will be created based on the engagement. This discussion document will
be presented back to Chiefs and leaders.
3. Engagement Summary:
c. Based on the Discussion Document, an engagement summary will be prepared providing a description
of the common area(s) of agreement amongst BC First Nations.
4. Building Consensus:
d. Further engagement session will follow the engagement summary. The dialogue will focus on further
amendments to the engagement summary to build and capture consensus.
5. Ratification:
e. A Draft Consensus Paper and resolution will be created from the regional summaries and presented to
Chiefs and leaders at GWXI for review and approval.
8The FNHC Engagement Pathway for 2021-2022
BC
in
s
er
sf
an
Tr
l th
1- r
ea
)
01 e
01
A
(2 ap
H
H
n sP
FN
t
r
rs
pe
t io u
Fi
to
Pa
lu ns
A
IH
s o se
H
s
FN
FN
su
Re on
en
t
d C
to
f
ro
en
ns
a n IV
IH
fe
W
Co
ip
FN
ns
& em
G
ic
2012
es sh
V
ra
of
lt em
W
n g
bl er
T
io ana
G
er
e
in on
ea t
Ta tn
3 nsf
n
t
H ys
,2 O
h
a
i
13
& r
2011
01 a
iz M
ci res lat
ly e
S
s Pa
r
Ju as
al cy
,2 T
0
in g
h nd
er wo
is
Ph
rd al
n n
Ad Leg
lt a
o
ob T
sm s
gi rge
co on
ct e
ea A
O as
Re me
H R IP
Ac egi
Ph
Ra d
R
D
E
e
ur
y
eg
st er
ct
ce ap
lth rat
ru
an s p
ea t
H rS
rn u
of ea
ve ns
Spring
ts n-y
go nse
2022
an e
ed co
in a T
w w
m f
Spring
ne e
er l o
re n
et a
GWXII
d ta
2021
D ov
an dop
al pr
ci ap
Sept 2022
A
Fall
So e
e th
2021
th m
on for
Fall
In
2022
2021 - 2022
Engagement & Approvals
Pathway
A variety of mechanisms for giving feedback will be used, including:
⚫ hard-copy booklets;
⚫ fillable PDFs;
⚫ online through the FNHC’s engagement website; and
⚫ through targeted direct community engagement (depending on COVID-19 guidelines).
Complete the Workbook online via ENGAGE.FNHC.CA 9The 7 Directives:
The 7 Directives are governance principles outlined by Chiefs and leaders through a process of intense
engagement over the course of hundreds of regional and sub-regional meetings. These principles are
fundamental to the health governance structure and guide any discussions that the FNHA, FNHC, and
FNHDA have with communities or partners.
Directive #1: Community-Driven, Nation-Based
⚫ The Community-Driven, Nation-Based principle is overarching and foundational to the entire health
governance arrangement.
⚫ Program, service and policy development must be informed and driven by the grassroots level.
⚫ First Nations community health agreements and programs must be protected and enhanced.
⚫ Autonomy and authority of First Nations will not be compromised.
Directive #2: Increase First Nations Decision-Making and Control
⚫ Increase First Nations influence in health program and service philosophy, design and delivery at the
local, regional, provincial, national and international levels.
⚫ Develop a wellness approach to health including prioritizing health promotion and disease and
injury prevention.
⚫ Implement greater local control over community-level health services.
⚫ Involve First Nations in federal and provincial decision-making about health services for First Nations
at the highest levels.
⚫ Increase community-level flexibility in spending decisions to meet their own needs and priorities.
⚫ Implement the OCAP (ownership, control, access and possession) principle regarding First Nations
health data, including leading First Nations health reporting.
⚫ Recognize the authority of individual BC First Nations in their governance of health services in their
communities and devolve the delivery of programs to local and regional levels as much as possible
and when appropriate and feasible.
10Directive #3: Improve Services
⚫ Protect, incorporate and promote First Nations knowledge, beliefs, values, practices, medicines and
models of health and healing into all health programs and services that serve BC First Nations.
⚫ Improve and revitalize the Non-Insured Benefits program.
⚫ Increase access to primary care, physicians, nurses, dental care and other allied health care by First
Nations communities.
⚫ Through the creation of a First Nations Health Authority and supporting a First Nations
population health approach, First Nations will work collectively to improve all health services
accessed by First Nations.
⚫ Support health and wellness planning and the development of health program and service delivery
models at local and regional levels.
Directive #4: Foster Meaningful Collaboration and Partnership
⚫ Collaborate with other First Nations and non-First Nations organization and governments to address
social and environmental determinants of First Nations health (e.g. poverty, water quality, housing, etc.).
Partnerships are critical to our collective success. First Nations will create opportunities through
working collaboratively with federal, provincial, and regional partners.
⚫ Foster collaboration in research and reporting at all levels.
⚫ Support community engagement hubs.
⚫ Enable relationship-building between First Nations and the regional health authorities and the
First Nations Health Authority with the goal of aligning health care with First Nations priorities and
community health plans where applicable.
Directive #5: Develop Human and Economic Capacity
⚫ Develop current and future health professionals at all levels through a variety of education and
training methods and opportunities.
⚫ Result in opportunities to leverage additional funding and investment and services from federal and
provincial sources for First Nations in BC.
⚫ Result in economic opportunities to generate additional resources for First Nations health programs.
Complete the Workbook online via ENGAGE.FNHC.CA 11Directive #6: Be Without Prejudice to First Nations Interests
⚫ Not impact on Aboriginal Title and Rights or the treaty rights of First Nations, and be without
prejudice to any self-government agreements or court proceedings.
⚫ Not impact on the fiduciary duty of the Crown.
⚫ Not impact on existing federal funding agreement with individual First Nations, unless First Nations
want the agreements to change.
Directive #7: Function at a High Operational Standard
⚫ Be accountable, including through clear, regular and transparent reporting.
⚫ Make best and prudent use of available resources.
⚫ Implement appropriate competencies for key roles and responsibilities at all levels.
⚫ Operate with clear governance documents, policies, and procedures, including for conflict of interest
and dispute resolution.
12Section Two: DRIPA
Background:
The United Nations Declaration on the Rights of Indigenous Peoples (UNDRIP) is an international set of
standards to protect the rights of Indigenous peoples. It describes specific rights across all areas of life
— like health, education and cultural identity. The Truth and Reconciliation Commission called for the UN
Declaration to be used as a framework for moving toward true and lasting reconciliation.
In November 2019, Bill 41, the Declaration on the Rights of Indigenous Peoples Act (DRIPA) was passed in BC.
The Act sets out a framework to implement UNDRIP and requires the BC Government, in consultation and
cooperation with Indigenous peoples, to:
⚫ Align BC’s laws with the UN Declaration;
⚫ Develop an action plan to meet the objectives of the UN Declaration; and
⚫ Table an annual report on progress to align BC’s laws and on the action plan.
In June 2020, the provincial government released the first annual report on progress for implementing the
Act for the period of November 28, 2019 (when DRIPA was enacted) to March 31, 2020 (fiscal year end). In
these first four months of initial actions under the Act, the provincial government held early discussions
with First Nations, negotiating partners, modern treaty nations and the First Nations Leadership Council to
identify areas for legislative development or amendment and priorities for the action plan.
Following the provincial election in October 2020, the NDP government
signaled that advancing the implementation of DRIPA as a priority.
The NDP party platform and the party’s foundational principles lay out commitments to furthering the rights
of Indigenous peoples, and all provincial ministerial mandate letters outline that ministers are expected to
focus on progressing these commitments.
The Ministry of Indigenous Relations and Reconciliation (MIRR) is tasked with the development of the action
plan required under DRIPA. As part of this work, MIRR has established an engagement process to support
a cross-government effort to engage Indigenous partners on the development of the action plan, including
with Chiefs and caregivers through the Spring 2021 Governance Caucus sessions.
As part of this process, the BC Ministry of Health and the Ministry of Mental Health and Addictions plans
to engage First Nations on sector specific priorities and actions and explore opportunities for further
engagement with First Nations through the virtual Regional Caucuses.
Complete the Workbook online via ENGAGE.FNHC.CA 13Additionally, the federal government has begun work on its own
legislation related to the implementation of UNDRIP principles federally.
On December 3, 2020, the Honourable David Lametti, Minister of Justice and Attorney General of Canada,
and the Honourable Carolyn Bennett, Minister of Crown-Indigenous Relations, announced the introduction
and first reading of Bill C-15, United Nations Declaration on the Rights of Indigenous Peoples Act. Similar to
the BC DRIPA, once passed by Parliament, this legislation would require the Government of Canada, in
consultation and cooperation with Indigenous peoples, to:
⚫ Take all measures necessary to ensure that the laws of Canada are consistent with UNDRIP;
⚫ Prepare and implement an action plan to achieve the purposes of UNDRIP; and
⚫ Table an annual report on progress to align the laws of Canada and on the action plan.
The second reading and debate of the bill in the House was on February 17, 2021; the bill has not yet
been passed.
DRIPA and Nation-Rebuilding:
Outcomes from FNHC’s engagement on the Social Determinants of Health (2016-present) show that Chiefs
and leaders noted broad, system-wide challenges which affected the ability of communities and Nations to
make progress on health-related initiatives. These include:
⚫ Insufficient and inflexible funding tied to government priorities rather than community need;
⚫ Burdensome reporting requirements, which take time, energy, and resources away from supporting
the community;
⚫ Limited authority in decision-making, with programs and services being determined by Ottawa and
Victoria; and
⚫ Limited support for culture and language.
In order to address these issues, the FNHC outlined a bold vision for change at Gathering Wisdom for a
Shared Journey X in the governance Guidebook “Reclaiming our Connections — The Next Ten Years.” This
Guidebook outlined where we communities and Nations want to be in ten years:
⚫ Actively rebuilding and strengthening their Nations.
⚫ Receiving sufficient, flexible funding for health and wellness services.
⚫ Redesigning and strengthening services to reflect the vision, values and laws of their Nation.
⚫ Full and equal partners in decisions about their health and wellness.
⚫ Receiving equal access to services as compared to other residents of BC.
14UNDRIP has several articles which support this work.
UNDRIP Summary
Articles 3-4 ⚫ Indigenous peoples have the right to self-determination. By virtue of that right they
freely determine their political status and freely pursue their economic, social and
cultural development.
⚫ Indigenous peoples, in exercising their right to self-determination, have the right to
autonomy or self-government in matters relating to their internal and local affairs, as well
as ways and means for financing their autonomous functions.
Article 5 ⚫ Right to maintain and strengthen distinct political, legal, economic, social and cultural
institutions, while retaining the right to participate fully, if they so choose, in the political,
economic, social and cultural life of the State.
Article 9 ⚫ Indigenous peoples and individuals have the right to belong to an indigenous community
or nation, in accordance with the traditions and customs of the community or nation
concerned. No discrimination of any kind may arise from the exercise of such a right.
Article 11-13 ⚫ Indigenous peoples have the right to practice and revitalize their cultural traditions and
customs. This includes the right to maintain, protect and develop the past, present and
future manifestations of their cultures, such as archaeological and historical sites, artefacts,
de-signs, ceremonies, technologies and visual and performing arts and literature.
⚫ States shall provide redress through effective mechanisms, which may include restitution,
developed in conjunction with indigenous peoples, with respect to their cultural,
intellectual, religious and spiritual property taken without their free, prior and informed
consent or in violation of their laws, traditions and customs.
Article 21 ⚫ Indigenous peoples have the right, without discrimination, to the improvement of their
economic and social conditions, including, inter alia, in the areas of education, employment,
vocational training and retraining, housing, sanitation, health and social security.
⚫ States shall take effective measures and, where appropriate, special measures to ensure
continuing improvement of their economic and social conditions. Particular attention
shall be paid to the rights and special needs of indigenous elders, women, youth, children
and persons with disabilities
Article 24: ⚫ Indigenous peoples have the right to their traditional medicines and to maintain their
health practices, including the conservation of their vital medicinal plants, animals and
minerals. Indigenous individuals also have the right to access, without any discrimination,
to all social and health services.
⚫ Indigenous individuals have an equal right to the enjoyment of the highest attainable
standard of physical and mental health. States shall take the necessary steps with a view
to achieving progressively the full realization of this right.
Complete the Workbook online via ENGAGE.FNHC.CA 15Language and Culture as a Basis for Nation-Rebuilding:
Culture is recognized as one of the social determinants of health; in particular, First Nations’ unique
languages and cultures are central to nationhood. Identity and belonging are key to human wellbeing.
Through the Tripartite Partnership to Improve Mental Health and Wellness Services and Achieve Progress on the
Determinants of Health and Wellness (2018), groups of communities have begun working together on the
basis of shared history, language and culture to plan, design and deliver mental health services in BC that
support the unique needs of their citizens.
Alongside these services, groups of communities have worked towards developing governance structures
which are truly Community-driven and Nation-based. The implementation of DRIPA can support the
recognition and embedding of these structures within the funding and service delivery models of Canada
and BC. As Canada has consolidated the services it delivers to Indigenous people through the creation
of Indigenous Services Canada (ISC), there is an opportunity to align funding and decision-making with
community health and wellness plans to enable direct investment in community priorities.
First Nations in BC are asked to consider whether shared language groups are an appropriate basis to
continue the discussion on Nation-rebuilding and DRIPA legislation (see Appendix A for Language Map).
Indigenous Language Groups:
Nłeʔkepmxcín Sk̲wx̱wú7mesh sníchim Tsi l hqot’ in
Sgüüx̣s Nsyilxcən Oowekyala / ’Uik̓alaShe
shashishalhem
Danezāgé’ Dakelh (ᑕᗸᒡ)
Southern Tutchone
Éy7á7juuthem Kwak̓wala
Sm̓algya̱x
diitiidʔaatx̣ Dene K’e
Ktunaxa
Gitsenimx̱ Anishnaubemowin
Secwepemctsín
St̓át̓imcets SENĆOŦEN / Malchosen /
Lekwungen / Semiahmoo / Łingít
Dane-Zaa (ᑕᓀ ᖚ) T ’Sou-ke
Nuučaan̓uɫ
Hul’q’umi’num’ / Halq’eméylem Witsuw it’en / Nedut’en
/ hən̓q̓əmin̓əm̓ ᓀᐦᐃᔭᐍᐏᐣ (Nēhiyawēwin)
X̄enaksialak̓ala / X̄a’islak̓ala
Háiɫzaqvḷa Nuxalk
Tāłtān
Ni s g̱ a’a Tse’khene
X̱aad Kil / X̱aaydaa Kil
Nlaka’pamux
SENĆOŦEN
16Potential Role for the FNHC on DRIPA:
FNHC members each have a responsibility to work as 1-of-1, as advocates for their respective family/
sub-region; as 3-of-3, as regional advocates to address and elevate regional interests and concerns;
and as 15-of-15, to provide political advocacy in health transformation. The following table outlines the
potential role of FNHC members, at the three levels, with respect to development and implementation
of the DRIPA Action Plan.
Ongoing Role - FNHC
Individually ⚫ Act as a facilitator, connect communities within their respective sub-region or
Nation Assemblies to discuss working together through the First Nations Health
Governance engagement structure.
Regionally ⚫ Support communities and Nations to maintain and strengthen distinct political,
legal, economic, social and cultural institutions.
⚫ Advocate on behalf of communities and Nations, when requested, to support the
improvement of their economic and social conditions in areas related to the Social
Determinants of Health with regional partners.
Provincially ⚫ Utilize the FNHC’s Social Determinants of Health Deputy Ministers Tables to advocate
for a streamlined approach to funding, investing directly into Community-Driven,
Nation-Based plans, such as a health and wellness transfer payment.
⚫ Support self-identified collectives of First Nations communities to be recognized
as Nations by the federal and provincial governments.
⚫ Advocate for the federal and provincial governments to engage directly with
the Nations on how best to implement DRIPA and support the overall self-
determination of First Nations people.
⚫ Engage with First Nations leaders on whether the structure of the FNHC needs to
change to support a community-driven, Nation-based approach to this work.
Complete the Workbook online via ENGAGE.FNHC.CA 17Engagement Questions:
1. As a legislative framework DRIPA can help to generate meaningful change at a systems level
(see page 14 and 15 for health-related articles of UNDRIP). In addition, we identified issues from
FNHC’s engagement on Social Determinants of Health (2016-present). These include:
⚫ Insufficient and inflexible funding tied to government priorities rather than community need;
⚫ Burdensome reporting requirements, which take time, energy and resources away from supporting
the community;
⚫ Limited authority in decision-making, with programs and services being determined by Ottawa and
Victoria; and
⚫ Limited support for culture and language.
Given this opportunity to address issues through DRIPA:
a) Which issues should we address first?
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
b) Are there any important issues you think are missing from this list?
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
182. The potential role of FNHC members, at the three levels, with respect to the development and
implementation of the DRIPA Action Plan is presented on page 17.
Given the issues you indicated and prioritized in question #1:
a) Do you think the proposed roles outlined in the chart on page 17 will be effective in addressing
these issues? Why or why not?
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
b) Is there anything you would add or change for any of the proposed roles?
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
Complete the Workbook online via ENGAGE.FNHC.CA 193. At Gathering Wisdom for a Shared Journey X in the governance Guidebook “Reclaiming our
Connections — The Next Ten Years” the FNHC outlined a bold vision for change. This Guidebook
outlined where communities and Nations want to be in ten years.
The implementation of DRIPA provides an opportunity for achieving this vision (outlined below).
⚫ Actively rebuilding and strengthening their Nations.
⚫ Receiving sufficient, flexible funding for health and wellness services.
⚫ Redesigning and strengthening services to reflect the vision, values and laws of their Nation.
⚫ Full and equal partners in decisions about their health and wellness.
⚫ Receiving equal access to services as compared to other residents of BC.
a) Do you think that the FNHC can effectively achieve the implementation of DRIPA and this
vision above? Why or why not?
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
b) If no, does the structure of the FNHC need to evolve in order to do so?
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
204. The implementation of DRIPA provides an opportunity for First Nations in BC to transform
funding and delivery service models for community health and wellness to be truly Community-
driven and Nation-based.
a) Would working together on the basis of shared language groups best support this
transformation, instead of the current regional framework (see page 16 for details on language
and culture as a basis for Nation-rebuilding)? Why or why not?
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
b) D
o you have any other thoughts or ideas for how a community-driven and Nation-based
system can be achieved?
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
Complete the Workbook online via ENGAGE.FNHC.CA 215. Do you have any other thoughts on how the implementation of DRIPA can support Community-
Driven, Nation-based decision making?
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
_______________________________________________________________________________________________________________________
22Section Three: Distinctions-based Health Legislation
Introduction:
Currently, there is no specific statute setting out the federal government’s responsibilities related to the
provision of funding or services for First Nations health, nor are there any statutes describing First Nations
authorities related to health governance. The Indian Act, Canada Health Act, Department of Health Act and the
Department of Indian Affairs and Northern Development Act are silent on these matters. The Constitution Act,
1867 sets out that overall responsibility for the delivery of health services rests with the provinces.
Regarding Indigenous health, the federal government uses policy and contractual domains to guide service
delivery and governance. First Nations have consistently challenged the lack of certainty regarding First Nations
health, noting that the federal government has a fiduciary responsibility to provide and fund health services. This
responsibility is grounded in the inherent rights of First Nations peoples to health, embedded in the constitution,
described in historic and modern treaties, and confirmed in various international legal documents.
The lack of a legislative base for First Nations health has led to uncertainty and gaps in health service delivery
by First Nations communities and organizations. The lack of clear authority, roles and responsibilities has
created jurisdictional debates on which government is responsible for health services, prompting the need for
supports and infrastructure to help facilitate the resolution of jurisdictional confusion, e.g., Jordan’s Principle.
This uncertainty also raises questions about the e continuity and sustainability of programs, services and
funding for First Nations health — not only in BC but across Canada.
Following the 2019 federal election, the minority Liberal government made a commitment to advance
Indigenous health through the development of distinctions-based Indigenous health legislation, as outlined
in the December 2019 Speech from the Throne and Minister of Indigenous Services’ Mandate letter.
On January 28, 2021 the Minister of Indigenous Services, Marc Miller,
announced that the federal government would begin engagement on
the development of Indigenous health legislation.
Through this engagement, the federal government is seeking to establish overarching principles; support the
transformation of health service delivery through collaboration with Indigenous organizations; and advance
Canada’s commitment to reconciliation. The engagement will happen in two stages, firstly through broad
engagement including with First Nations, provinces and subject matter experts; followed by co-development of
legislative options.
The federally-led engagement will be broad-based and seek to define the scope and parameters of
distinctions-based Indigenous health legislation, working with First Nations, Inuit and Metis Nation
partners, as well as the provinces and territories.
Complete the Workbook online via ENGAGE.FNHC.CA 23This process includes reaching an agreement on mutual areas of interest and practical objectives,
and supporting discussions on:
⚫ Closing the gaps that arise from the patchwork of federal/provincial/ territorial/Indigenous
policies and legislation relevant to Indigenous health services; and,
⚫ How federal legislation could complement provincial/territorial legislation.
Basis for a BC-Specific Approach to Health Legislation:
With the made-in-BC Health Governance Structure, BC is in a unique position to inform the federal
approach to health legislation. The FNHA, FNHC and FNHDA are unique organizations within the
Canadian health system, and discussions regarding federal health legislation must take this into
account. Since the BC Health Governance Structure was created, the development of health legislation
has been noted in multiple documents, including the Tripartite Agreement on First Nations Health (2011),
the Consensus Paper 2012, the “Building Blocks of Transformation” workbook (2013), and the “In Plain
Sight” Report (2020) (see Appendix B).
Chiefs and leaders must consider how federal health legislation can support and bolster the First Nations
Health Governance Structure in BC, including determining the scope of the FNHA.
Considerations regarding Health Legislation:
The enactment of federal Indigenous health legislation raises a number of considerations in the BC context.
Preliminary considerations include:
Establishing a clear The need to establish a mandate from leadership, through National and/or
mandate: Regional processes.
Establishing Some Chiefs have raised concerns that the direction to co-develop the proposed
clear scope and legislation only appears in the mandate letter of the Minister of Indigenous
responsibility: Services and is not referenced in the Minister of Health’s mandate letter; the
integration, role and accountabilities of the provinces in the legislation remains to
be determined.
Relationship with Treaty and non-treaty Nations have a different relationship with the Crown. It is
Treaty Nations: important that Indigenous Services Canada (ISC) articulate how legislation will
interact with historic and modern treaty Nations in addition to non-treaty Nations.
In addition, legislation will need to not impact existing Treaty or Aboriginal rights.
24Obligations to ISC will need to clarify how health legislation will encompass its differing
different Indigenous responsibilities to First Nations, Metis, and Inuit peoples.
groups:
Alignment with Federal legislation will need to consider the BC Tripartite Framework Agreement
BC Tripartite on First Nation Health Governance including the Tripartite Partners’ shared goal
Agreements: of improving the health and wellbeing of First Nations individuals, families and
communities in BC as envisioned in the Tripartite First Nations Health Plan (2007).
Co-Development Should Indigenous health legislation move forward, engagement to inform the co-
processes and development processes will be significant and fast-paced. The federal government
principles: will need to consider how its processes work with BC First Nations and align with
established bilateral mechanisms. First Nations in BC may wish to establish their
own co-development processes and principles to inform federal legislation, rather
than working through national bodies such as the AFN. As such, BC First Nations
political leadership bodies, including the First Nations Health Council (FNHC), will
need to consider how they envision political engagement in the development of
federal health legislation. This includes processes to engage political leadership
(e.g., Chiefs and Council) throughout the process; potentially using established
engagement mechanisms (regional tables and assemblies).
Alignment with Both Canada and BC have committed to implementing the UN Declaration on the
UNDRIP: Rights of Indigenous Peoples (UNDRIP). UNDRIP contains significant provisions related
to health, the social determinants of health, governance, and self-determination.
Expanded Scope of Since the transfer of services from the First Nations-Inuit Health Branch (FNIHB)
FNHA compared to of Health Canada in 2013, FNHA has expanded the scope of its operations as
FHNIB: compared to FNHIB, including in areas such as:
⚫ increased advocacy for First Nations people within the broader provincial
health system;
⚫ increased policy function informed by on the ground operational
experience; and
⚫ modifications to the health benefit program.
Complete the Workbook online via ENGAGE.FNHC.CA 25Expanded Scope of In particular, FNHA has been attempting to clarify roles in emergency management
FNHA for Emergency at various levels (operational and strategic; regional, provincial, and federal). In that
Management: time, the majority of emergency response has been related to other emergencies
such as environmental spills and natural disaster events, however, the COVID-19
global pandemic, and the Mental Health and Wellness / opioid crisis have presented
FNHA and its partners with unique and complex challenges and opportunities.
In emergencies the FNHA is operating at the request of Nations, who ask for trusted
FNHA support, advisory services and partnership. There continues to be confusion
over FNHA’s role in the provincial and federal emergency management processes as
FNHA is not legislated nor formally recognized as part of the emergency response or
Incident Command Structure. While the FNHA is not seeking regulatory enforcement
authority, having some recognition in legislation would clarify the FNHA’s role when
responding to community requests in public health emergencies.
Legislation that recognizes the FNHA as a legislated body created though the
authorities of BC First Nations communities would enable the FNHA to respond
to emergencies (environmental, public health, mental health, and pandemic) on
behalf of communities, if directed to do so by communities.
Respecting the The Consensus papers outline the 7 Directives and compel the FNHA and FNHC
7 Directives: to operate in a way that is Community-driven, Nation-based (Directive #1), while
not prejudicing first Nations rights and title or jurisdiction (Directive #6).
FNHA and Tripartite A number of evaluations, including the FNHA Evaluation and Tripartite
Framework Framework Agreement Evaluation, have collected extensive feedback from BC
Agreement First Nations on the work done thus far. These evaluations include important
Evaluations: lessons for the FNHA and the FNHC in meeting the needs of First Nations —
and can inform the scope of the FNHA within legislation. The FNHC plans to
hire an independent consultant to conduct an evaluation of its activities since
transfer. The scope of this evaluation will be determined by a Chiefs Working
Group, consisting of one leader from each region. These evaluations will
include important lessons for this work.
Evolution of funding During engagement on the Social Determinants of Health (2016-Present),
structures: First Nations leaders and caregivers have noted that funding and accountability
structures need to reflect community priorities. To address this issue, the FNHC
proposed in the “Reclaiming our Connections — The Next Ten Years” Governance
Guidebook that Canada and BC work with First Nations to streamline funding
delivered for health and wellness services into a single block funding agreement,
called a “health and wellness transfer payment.” Consideration should be given to
how Indigenous health legislation could ensure that funding mechanisms reflect
community priorities.
26Potential Role for the FNHC on Health Legislation:
FNHC members each have a responsibility to work as 1-of-1, as political advocates for their respective family/
sub-region; as 3-of-3, as regional advocates to address and elevate regional interests and concerns; and as 15-
of-15, to provide political advocacy in health transformation. The following table outlines the potential role of
FNHC members, at the three levels, with respect to the implementation of Federal Health legislation.
FNHC Ongoing Role
Individual ⚫ Work with leaders within their respective sub-regions and/or Nation Assemblies to
identify priorities, elevating issues to the regional and provincial level as needed,
through the First Nations Health Governance engagement structure.
Regionally ⚫ Work with First Nations in their respective regions to support the development
of community-driven, Nation-based governance structures, for the purposes of
capacity-building.
Provincially ⚫ Support the FNHA through political advocacy with Canada and BC in negotiating a
BC-specific approach to federal health legislation.
⚫ Support Nations with capacity-building in order for them to express their inherent
rights related to health and the social determinants of health.
⚫ Embedding a community-driven, Nation-based, and regionally-coordinated approach
to health services within legislation.
Complete the Workbook online via ENGAGE.FNHC.CA 27Engagement Questions:
1. The federal government announced it would begin engagement on the development of
Indigenous health legislation. The process will involve engagement and co-development of
legislation (see pages 24-26 for details). Given this opportunity, Chiefs and leaders must consider
how federal health legislation can support and bolster the First Nations Health Governance
Structure in BC.
With the support of federal health legislation, what aspects of health and wellness would your
Nation benefit from having greater control over?
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
______________________________________________________________________________________________________________________
28 First Nations Health Council | Reclaiming Our Connections: The Next Ten YearsYou can also read