Severe Malaria Global Stakeholder Meeting 21-22 October 2019, Abuja, Nigeria - Defeating Malaria Together
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Severe Malaria Global Stakeholder Meeting 21-22 October 2019, Abuja, Nigeria Defeating Malaria Together

Abbreviations ARC Artesunate Rectal Capsules (or RAS = rectal artesunate) CARAMAL Community Access to Rectal Artesunate for Malaria CHAI Clinton Health Access Initiative CHW Community Health Worker CRS Catholic Relief Service GFATM The Global Fund to Fight AIDS TB and Malaria iCCM Integrated Community Case Management Inj AS Intramuscular Artesunate Injection KSPH Kinshasa School of Public Health MMV Medicines for Malaria Venture MSF Médecins Sans Frontières MSH Management Sciences for Health NURTW National Union of Road Transport Workers RBM Roll Back Malaria PMI President’s Malaria Initiative Swiss TPH Swiss Tropical and Public Health Institute WHO World Health Organisation

Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 3
Executive Summary
Background
Medicines for Malaria Venture (MMV) and the Clinton Health Access Initiative (CHAI) convened a Severe
Malaria Global Stakeholder Meeting, under the auspices of the RBM Case Management Working Group
and in collaboration with UNICEF, Swiss Tropical and Public Health Institute (Swiss TPH) and Médecins
Sans Frontières (MSF). The meeting was hosted by the Nigerian Ministry of Health in Abuja, Nigeria and
held on the 21st and 22nd of October, 2019.
This was the first meeting convened on severe malaria case management, building on stakeholder
meetings focused on Injectable artesunate (Inj AS) and artesunate rectal capsules (ARC) in 2011 and
2016, respectively. The meeting assembled countries that have commenced the process of rolling out
rectal artesunate within their systems of severe malaria care.
The meeting brought together delegations representing 19 countries: Angola, Benin, Burkina Faso, CAR,
Congo, DRC, Ethiopia, Ghana, Liberia, Madagascar, Malawi, Mali, Mozambique, Niger, Nigeria, Sierra
Leone, Uganda, Zambia and Zimbabwe, and 15 partner organizations, including RBM, Unitaid, PMI
USAID, Global Fund, UNICEF, MSH, Swiss TPH, Akena, KSPH, CRS, Makarere University, MSF, PSI,
WHO and the Malaria Consortium.
Aims and objectives
The key objective of the meeting was to share experiences from existing efforts to improve the continuum
of severe malaria care from community to referral facility levels, incorporating rectal and injectable
artesunate. The ultimate goal of the meeting was to promote better patient care and reduce mortality
from severe malaria.
Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 4
The meeting sessions
DAY 1 The meeting was introduced with a short review of updated WHO recommendations on pre-referral
interventions and treatment of severe malaria, an overview of the currently available WHO prequalified
severe malaria products (Artesunate Rectal Capsules (ARC) and Injectable Artesunate (Inj AS)), highlighting
that an appropriate ACT is required to complete severe malaria treatment, and an update on ARC and Inj
AS procurement and guideline alignment in endemic countries.
The meeting day was structured according to the following themes, each highlighting a different aspect
of ARC and Inj AS implementation and deployment:
Theme 1: Coordination in funding and implementation
During this session, experiences and perspectives from countries and donors were shared, and
opportunities and ways forward to ensure stronger national leadership, improve coordination and address
health system related challenges were discussed.
Theme 2: Service delivery pre- and post-referral
Country presentations reflected on real-life experiences in the roll out of ARC and Inj AS along a continuum
of care. Challenges included complications in completion of referral, especially in remote settings, stock
management and correct use of artesunate products. Lessons learnt in addressing these problems were
shared, including formal involvement of the private sector.
Theme 3: Referral
Presentations and discussions focussed on the need for communities’ active participation in referral
systems, the importance of community-supported emergency transport systems and the crucial and
potentially life-saving role of community health workers as a first point of care. It was discussed that
countries should move towards compensating community health workers (CHWs) as accountable
workers within the health system, and that up from the first level facility, transport for referral should ideally
be part of the formal health care services.
Theme 4: Logistics and supply chain management
A compilation of currently available data on the stability of ARC were presented by MMV as well as
storage solutions for ARC at community level in Uganda and DRC. The presented preliminary stability
data suggest ARC is stable for at least 18 months at temperatures up to 30°C, and for short periods (up
to 3 months) at 40°C. However, more robust data are required to revise current WHO recommendations
and approved SmPCs which must continue to apply (i.e. “Do not store above 25°C. Avoid excursions
above 30°C”).
DAY 2 On day 2, 8 countries (Angola, Madagascar, Malawi, Mozambique, Nigeria, Uganda, Zambia
and Zimbabwe) participated in workshops and reported on the key themes from day 1: 1)
Coordination, 2) Service delivery pre- and post-referral, 3) Referral, 4) Supply chain, with an additional
topic included on Surveillance.
Meeting Conclusion
The meeting was concluded with an invitation to countries to develop concrete action plans for the next
12 months for the successful implementation of ARC and Inj AS, along the lines of the meeting themes.
Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 5
Introduction
1. World Malaria Report Malaria remains one of the leading causes of illness and death in children under 5 years old. In 2018,
2019. WHO.
2. WHO Guidelines for an estimated 405,000 people died from malaria globally, 61% of whom were children under 5 years old.
the Treatment of Malaria,
3rd edition, 2015. WHO. The heaviest malaria burden is in sub-Saharan African countries, which accounted for an estimated 92%
3. Gomes MF et al.
Pre-referral rectal of malaria cases and 93% of malaria deaths in 2018.1 Severe malaria is linked to delayed treatment of
artesunate to prevent
death and disability
uncomplicated malaria, often due to late treatment seeking or poor quality case management. Mortality
in severe malaria: a
placebo-controlled trial.
from untreated severe malaria (particularly cerebral malaria) approaches 100%. With prompt, effective
Lancet. 2009, Vol. 373, severe malaria treatment and supportive care, this rate falls to 10–20%.2
pp. 577-66.
Patients with severe malaria should first be treated with intravenous or intramuscular artesunate for at
least 24 hours and until they can tolerate oral medication. At this time, the patient should complete
treatment with 3 days of an ACT. If parenteral artesunate is not available, artemether IM should be used
in preference to quinine for treatment of children and adults with severe malaria.
Many patients with severe malaria, however, live in remote settings with poor access to health facilities.
Where Inj AS is not available, ARC is an effective pre-referral intervention recommended for young
children under 6 years of age. ARC rapidly (i.e., within 24 hours) clears 90% or more of the malaria
parasites in children younger than 6 years of age and can reduce the risk of death or permanent
disability by up to 50%.3 Administration of ARC must be followed by immediate referral of the patient to
a higher-level facility where the complete treatment for severe malaria can be provided, which includes
Inj AS and an appropriate ACT.
Despite WHO recommendations since 2006, adoption and use of ARC and Inj AS remained fairly
stagnant over the first 5 to 10 years partly due to limited availability of products and slow uptake by
countries. Developments in recent years, however, are rapidly changing this landscape as quality-
assessed injectable and rectal products have become available. Investments from Unitaid have led
“
to two WHO-prequalified products in both product categories: a WHO prequalified Inj AS product
(30mg, 60 mg, 120 mg) produced by Guilin, available since 2011, is now complemented by the recent
prequalification of an Ipca Inj AS product (60 mg). For ARC, both CIPLA and Strides 100 mg products
received prequalification status in 2018.
Inj AS is now registered in 33 countries, and ARC in 16
countries globally. Many countries have already started
In 2018, an estimated using ARC and others are poised to scale up the use of
ARC and Inj AS over the coming years, with large donors
405,000 people died
including PMI and GFATM pledging their support through
increased funding for the procurement of both WHO
prequalified injectable and rectal products.
from malaria globally,
61% of whom were
children under
5 years old.”Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 6
Stakeholder meeting rationale and purpose
This meeting aimed to serve as a timely platform for countries to share experiences of severe malaria case
management, including sharing of initial experiences from the multi-country Community Access to Rectal
Artesunate for Malaria (CARAMAL) project.4 It provided attending countries with an opportunity to receive
information for implementation plan development, taking into account the next GFATM funding cycle. The
agenda for the meeting was structured around responses to a questionnaire (see annex 2) shared with
invited countries prior to the meeting in order to help prioritize which topics or themes should be included
in the meeting agenda.
This report will provide an overview of the contents and discussions of the meeting, outline trends across
countries and specify any next steps and conclusions.
DAY 1 Day 1 sessions were divided into four themes: (1) Coordination in funding and implementation; (2) Service
delivery pre- and post-referral; (3) Referral; and (4) Rectal artesunate supply chain and stability guidance.
Preliminary experiences from the CARAMAL project and findings from MMV’s rapid assessments5 across
DRC, Liberia and Uganda formed the basis for discussion and reflection in the sessions.
> A complete agenda can be found in annex 1.
Theme 1: Coordination in funding and implementation
Strengthening of severe malaria case management requires coordination with multiple actors, funding
streams, supply lines and implementing agencies. It also requires harmonization of NMCP, child and
community health programs, national supply chain management and pharmacy departments’ policies
and guidelines. In pre-meeting questionnaire responses, many countries identified coordination in funding
and implementation as a priority area of discussion.
The objective of this session was to share experiences and perspectives on coordination in funding and
implementation, including challenges and opportunities.
Three countries (Nigeria, Uganda and DRC) shared their experiences, successes and challenges in the
area of malaria coordination. Each country provided background information on their severe malaria
systems and one example of an effort to combat challenges of coordination. Additionally, a presentation
from PMI gave an overview of funding and coordination from the donor perspective.
Challenges and good practices
Coordination between donors and national programs can be challenging, and there is a need for a better
alignment of priorities, financing cycles and commodity orders. Planning is the government’s responsibility,
but implementation is often led by partners, resulting in a lack of coordination and information flow.
This can result in interventions based on available funding rather than in-country needs. For example, in
Nigeria, funding decisions are often driven by donor policies, with 13 of 36 states still lacking any donor
4. Community access to support.
rectal artesunate for
malaria (CARAMAL) is
a 3-year observational
research study in DRC, National and state level advocacy to ensure that resources are aligned with needs (‘giving Ministries of
Nigeria and Uganda,
funded by Unitaid,
Health a strong voice’) is crucial. In Uganda, there have been severe delays in accessing donor funding
that introduces ARC in
communities through
and poor alignment of donor and government’s financial cycles has affected planning. Inflexible donor
iCCM. CARAMAL aims policies did not allow for reprogramming of funds.
to contribute to reducing
malaria mortality in
children by improving the
community management Procurement of commodities for malaria remains donor-driven and is done according to donor’s funding
of suspected severe
malaria and advance cycles, which can impact stock levels, supply chain plans, and commodity distribution systems. Most
the development of
operational guidance for countries report a lack of funds for procurement of the full array of commodities (in particular non-malarial
the scale-up of ARC. The
evidence generated in the
commodities) needed for the management of severe cases. This gap affects quality of care at all levels
context of the CARAMAL
project will be reviewed
of the health system at all levels, from iCCM to primary, secondary and tertiary facilities. Support for
by WHO in 2021. severe malaria management should, in these countries, be expanded beyond ARC and Inj AS to capture
5. Reports are available on
www.severemalaria.org the entire supply package of consumables required. To lessen donor dependency, in-country advocacySevere Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 7
is needed to increase domestic funding for quality assured malarial and non-malarial commodities
procurement. Irregular donor-driven drug supplies could, for example, be transitioned to a drug revolving
fund model or other mechanisms to increase sustainability in the health system and reliable access to
care. Proper procurement planning of severe malaria commodities is crucial, as only few supplies are
WHO prequalified and lead times may be long.
Decision-making by donors lacks attunement to the reality on the ground. Quality data collection is often
project-based, and does not take continuity and alignment with national systems into consideration. When
quality data exist, these are often not used for decision-making. Regular review meetings with donors are
recommended so that there is early engagement in case of trends, problems and anticipated changes.
In Nigeria, working groups at national level (a Working Group for Severe Malaria which provides strategic
advice and a Malaria Technical Working Group, coordinating all stakeholders) helped to focus attention on
problems and ensure there are information feedback loops to implementers. To ensure working groups
accurately represent the realities on the ground, a strong engagement with health workers is needed and
a culture of data use should be nourished.
There is a need for improved coordination between major malaria donors, the main donors being GFATM
and PMI-USAID. This has been recognized, and recent efforts by PMI have focused on harmonizing
activities and funding categories with GFATM (including financial and supply chain data). In DRC,
coordination with partners in the target areas (eg WHO, GFATM/SANRU) has been poor, and to respond
to this critical gap the partners organized and executed a successful joint field mission which enabled
information sharing and improved planning.
Theme 2: Service delivery pre- and post-referral
The continuum of care for malaria from identification of severe illness signs to care-seeking and then
provision of care is not linear. One child may be taken to see numerous providers across public and
private, formal and informal sectors. This child may or may not receive the complete care s/he requires.
Improving quality of severe malaria care requires engagement of numerous stakeholders (including
caregivers, CHWs, drug shops, and referral facility providers), and ongoing competency retention and
quality improvement measurement at both pre- and post-referral levels of care. Based on pre-meeting
questionnaire (see annex 2) responses, a session on service delivery from community to referral facility
levels was included in the meeting.
“
Session objectives were to provide country specific experiences on quality of care at pre- and post-referral
levels, including challenges and opportunities, and allow countries to assess how these experiences may
be applicable to their own situation.
Challenges and good practices
There is a need for
Regular stock outs of artesunate products, other iCCM
commodities and equipment/ supplies needed to manage
severe malaria at referral level is a highly challenging issue
improved coordination for weak health systems. Poor reporting at facility level
and incomplete data flow to higher levels, often due to
poor digital access, results in inaccurate quantification
between major malaria and suboptimal distribution of medicines. A number of
countries are consistently either overstocked or under-
donors”
stocked with AS products. Complicating factors are a lack
of historical consumption data for ARC and suspected
misuse of Inj AS for uncomplicated malaria. Challenges
also exist in transportation of medicines to remote areas.
In DRC, Uganda and Nigeria, preliminary results from the CARAMAL project found inadequate severe
malaria commodities in secondary and tertiary facilities for the management of severe malaria. In a survey
of CHWs in Uganda, high levels of ARC (45%) and RDT (49%) stock out were observed in the previous 3
months (CARAMAL). In Nigeria, RDT stock-outs had occurred in 54% of communities and 17% of primary
facilities in the last 12 months, while Inj AS was available in only 13% of primary facilities (CARAMAL).Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 8
In DRC, frequent stock-outs of Inj AS, ACT and RDTs occurred; MMVs rapid assessment of found that
ARC had never been available in 40%, and was stocked out in 33% of health facilities. It also found that
Inj AS had never been available in 60%, and was stocked out in 20% of health facilities.6 Ensuring the
continuous availability of medicines and other necessary commodities is crucial to achieve a continuum
of care for severe malaria. Lessons learnt include the utilisation of routine data for stock management
and distribution, and the redistribution of medicines and diagnostics between levels of facilities and from
facility to community level as needed. Support for severe malaria management should preferably be
combined with investments in strengthened reporting and supply management systems.
Poor adherence to guidelines, insufficient training in malaria case management and a lack of availability of
treatment guidelines in facilities is common. This is complicated by a high turnover of human resources
(HR) and a lack of retention of trained HR. Findings from MMV’s rapid assessment found that updated
malaria case management guidelines were available in only 27% of surveyed health facilities in DRC,6 while
in Liberia, 56% of surveyed health facilities had a case management training manual.7 In Uganda, severe
malaria was managed with varying levels of quality in secondary and tertiary facilities and depended on
the level of training and the availability of equipment and supplies.8 Diagnostic capacity at referral level
in Uganda is underused: glycaemia and haemoglobin were most of the times not measured in surveyed
facilities, despite equipment being in place (CARAMAL).
In-service training, mentoring and supervision in health facilities to improve adherence to treatment guidelines
is essential for improving quality of care. Experience shows that gaps created by high staff turnover can be
addressed by creating national repositories of health workers trained in severe malaria management.
Many severe malaria cases are treated at primary level. Case misclassification and poor referral practices
are common. In DRC, severe malaria cases managed at primary level are known to be treated with
quinine or other injectable drugs purchased by the patient. MMV’s rapid assessment found that 75%
of severe malaria patients were treated at the primary level instead of being referred to a higher level.6
Referral rates in DRC may be lower than in other settings due to a number of factors including difficulties
in referral completion (poor roads and limited transportation) and health facility reliance on consultation
fees (primary health facilities can earn as much as 30 USD/case through sales of quinine and blood
transfusion).
Morbidity and mortality in children after treatment for severe malaria is of concern. Under CARAMAL,
enrolled children are assessed at day 28 after treatment. In Nigeria, preliminary results show 5% had
died, 5% were still sick and around 80% were anaemic (Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 9
The role of the private sector in the management of severe malaria is likely to be considerable. There
is a lack of coordination between public and private health sectors and a lack of regulation, reporting
and adherence to guidelines within the private sector. Inj AS sold in the private sector are mostly very
expensive as compared to the public sector.
Pilot studies by CHAI and others demonstrated that investments in the private sector at the community
level can improve malaria case management (at least for uncomplicated malaria); after training, supervision,
linkage of drug shops to affordable high quality commodities and market shaping, the availability of iCCM
commodities increased, prices of RDTs and ACT decreased and private provider knowledge improved.
CHAI also supported the Ministry of Health in Uganda to introduce mTrac mobile weekly reporting to
private health care providers and demonstrated that the private sector is able to consistently report quality
data on febrile diseases.
Proposed good practices are to engage the private sector and involve regulatory bodies to enforce
adherence to the guidelines. Providing training and mentorship in severe malaria case management to the
private sector should improve provider knowledge, and could possibly have a positive impact on quality,
availability and prices. Rolling out a convenient reporting system in the private sector could help generate
consistent quality data.
Theme 3: Referral
The severe malaria continuum requires prompt and accessible transfer of severely ill patients from community
to a higher level facility equipped with wider diagnostic and curative capabilities. Pre-referral ARC is only
effective as a life-saving commodity if followed promptly by this higher level of care. Among others, financial,
geographical, and infrastructural barriers make the rapid transfer of (severely ill) patients challenging.
Objectives of this session on referral were to provide country specific challenges and opportunities around
the referral of children with severe febrile illness, and contextualize experiences to allow countries to
assess how these experiences may be applicable to their own situation.
Challenges and good practices
There may be low community awareness of the danger signs of severe malaria and the treatment options
available at community level. In Uganda, there was an average delay of 2 days before reporting to any
point of care (pharmacy, health facility or CHW), including those within the community itself (CARAMAL).
CHWs are not always engaged as a first point of care. CHWs are meant to be the first point of care
in remote areas and responsible for administering ARC and initiating subsequent immediate referral.
However, they can be insufficient in number and distribution, and inadequately supported, with functions
that are not entirely clear to communities they serve. Since many work on a voluntary basis and are over-
tasked, they cannot be expected to always be readily available.
Caramel findings were that in DRC, caretakers consulted CHW’s in 10 km away for 64% of severe malaria referrals by CHWs.Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 10
To work around these challenges, emergency transport could be organized at community level. Successful
pilots in Nigeria and Zambia involved volunteer drivers, supported by community funds. These volunteer
drivers can also act as agents of change. Communities must actively participate in referral systems and
organize around them, take ownership and be actively involved in developing strategies for emergency
transport. Possible sustainable funding sources for emergency transport systems can include community
based health insurance schemes. It became clear in discussions that referral is a multisectoral issue that
must involve ministries of transport, infrastructure and digital communication. From the first level facility,
transport should ideally be part of the formal health care services.
Costs of care at referral facilities can be high; in DRC, these were prohibitive for a majority of patients.
Long waiting times at referral facilities (due to overburdened staff and poor advance communication of
referrals / triage upon arrival) puts patients at risk and reduces satisfaction with care. In these situations,
setting up a digital communication chain (if sufficient coverage) and a referral protocol can be explored to
help decrease waiting times.
10. WHO bulletin from
December 2019
Bull World Health Organ Health seeking behaviour studies and known poor access to care point to hidden mortality due to
2019;97:810–817| doi:
http://dx.doi. severe malaria in communities. Operational research and death audits are needed to create a better
org/10.2471/
BLT.19.231506 understanding of actual severe malaria burden and mortality.
Emergency transport models
æ
Emergency Transport System in Nigeria
An existing EU-UNICEF partnership with the National Union of Road Transport Workers (NURTW), organizing locally
available transport for maternal and new-born health, was extended to transportation of children referred with danger
signs of severe malaria under CARAMAL. Under this scheme, through NURTW, volunteer drivers in communities
receive various rewards for their services, such as provision of engine oil during Volunteers Appreciation Days, fuel
vouchers, free vehicle servicing vouchers and cash vouchers linked to distances travelled, while in communities,
transport loans with minimal interest are made available. The system proved highly effective in providing access to
transportation, reducing costs of transport for families and improving referral completion for severe malaria.
Community based severe malaria referral system in Zambia
In Zambia, ARC was implemented in 5 districts following a successful pilot which included engagement and education of
communities, training of CHW’s and community grants for emergency transport systems involving bicycle ambulances
with trained riders. 100% of severe malaria cases who received ARC from CHWs were successfully referred, and 72%
travelled to the referral facility using the emergency transport system. The mortality from severe malaria was reduced
by 96% in this pilot.10Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 11
Theme 4: ARC supply chain and stability guidance
Session objectives were to provide country specific findings on ARC distribution and storage, including
challenges and opportunities, and provide an understanding of product characteristics related to ARC
distribution and storage.
ARC ‘melting’
The two WHO prequalified ARC formulations are identical softgel rectal capsules, packed in aluminium
foil (alu/alu) blister packs which fully protect from humidity. These softgel capsules have a consistent
thermostable shape. The soft gelatin shell is filled with a fatty matrix containing the artesunate drug which
is designed to melt and release the drug at body temperature. However, outside the body, the softgel
capsule is not affected and capsules can go through repeated cycles of melting and solidifying which
does not damage either the inert fill or the capsule shell. The capsule can be returned to “solid” and used
simply by cooling it, and can be safely used when the fill is in any physical state, although it is easier to
insert the capsules when the fill is “solid”.
As in communities, CHWs have reported that they discarded melted ARC, they have to be informed that
the product can usually be re-solidified through cooling without reducing the effectiveness of the treatment.
ARC shelf life
The shelf life of the two WHO-prequalified generic ARCs is 24 months when stored at 25°C. The
manufacturers both state that excursions above 30°C should be avoided.
In the WHO Public Assessment Report (WHOPAR), the WHO Prequalification Programme provides
additional important recommendations on the storage of ARC: ‘Artesunate suppositories are generally
less stable above 30°C and in particular at the WHO accelerated storage condition (40°C/75%RH). To
this end, procurers and distributors should take utmost care to avoid excursions above 30°C during
storage and transportation of the product. However, it is understood that this storage requirement may
not always be adhered to when the product is handled by community health workers (CHWs) located
in areas where the ambient temperature is usually above 30°C. Therefore, procurers and distributors
need to ensure that the product is distributed to CHWs located in such areas only as a short-term stock,
generally not exceeding 4-6 months depending on the remaining shelf life of a given batch and severity of
the ambient conditions where the batch is to be distributed.
If unused in the context of the CARAMAL project, ARC is retrieved after this period and disposed of –
a practice that is neither resource-friendly nor sustainable.
Artesunate degrades over time and degradation is greater at higher temperatures. The degradation of
artesunate encapsulated in ARCs is a slow process, as shown by the below ARC stability data, which
were generated by the manufacturers from their registration stability batches (average values from all
batches tested are presented).
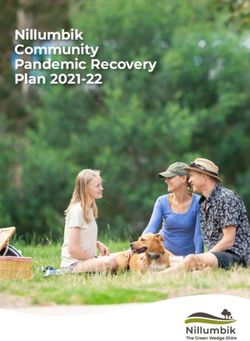
Capsule Stability – Percent Artesunate Data
æ
25°C– Generics and TDR
3m 6m 9m 12m 18m 24m
99% 95%
30°C
3m 6m 9m 12m 18m 24m
Generic 1 99% 92% NT
Generic 2 98% 94% 89%
TDR 96% 91%
40°C– Generics and TDR
3m 6m 9m 12m 18m 24m
99% 89%Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 12
Each capsule must contain 90-105% of the claimed 100 mg artesunate during its shelf life. When stored
at a consistent temperature of 30° for 24 months, the content is approximately 90% for both generic
ARC products. One manufacturer did not test at 24 months (NT) due to borderline OoS value for a non-
specified degradation product at the 18 months timepoint. At community level, temperatures fluctuate
and are not consistently >30°C. The decrease in artesunate content is, therefore, likely to be less than in
the above study. The manufacturers’ stability data suggest that ARC stored in the field between 6 and 24
months is likely to be at a level that does not impact the clinical effectiveness of ARC, taking into account
both variations in patient dosage introduced by the ARC age dosing regimen, and the naturally variable
rectal absorption.
The CARAMAL project monitors temperatures in about 10 ARC storage sites per country for further
analysis.
Storage solutions
æ
Storage and handling of ARC in Uganda during the CARAMAL pilot project
In the context of CARAMAL, in health facilities in Uganda, ARC is kept on the lower shelves, away from the wall directly
facing the sun. Where storerooms are small and the recorded temperatures are above 30°C, ARC is kept in a different
secure and cool location outside the storeroom. ARC is issued in small stocks to CHWs during quarterly review
meetings, for immediate transport back to their communities, avoiding direct body contact. Most CHWs store ARC
in their grass thatched houses which are normally cooler than the outside environment. CHWs are instructed to keep
ARC away from cooking areas, doors and windows. Furthermore, CHWs are instructed to transport ARC stocks from
health facility to the community during early mornings or late afternoons, avoiding the heat of the day.
In Uganda, temperatures ranged from 28 to 36°C at the time of project inception. A decision was therefore made to
retrieve ARC from communities every 3 months. This proved logistically complex and led to stock outs at community
level as well as reduced confidence in this pre-referral intervention. Retrieving the commodity is neither a resource-
friendly nor a sustainable option.
Novel storage ideas in a high temperature setting: an example from DRC
In DRC, temperatures during the hot and dry season exceed 30°C at the hottest time of day; storage solutions
deployed were bamboo racks which allow for air flow, and a container sunk in a bucket of water in case of high
temperatures (see picture below).Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 13
Challenges and good practices
Low quality, ineffective ARC formulations are available in some countries and undermine communities’
trust in the effectiveness of ARC. Contrary to prequalified products, these formulations are not stable at
high temperatures and may put lives at risk. Countries should be supported to ban low quality formulations
of AS; strong guidance is needed from WHO and partners on the use of prequalified AS products, and
where and how to procure and use these. WHO has issued an information note on rectal artesunate
for pre-referral “treatment” of severe malaria; the information note is available under the following link:
https://www.who.int/malaria/publications/atoz/rectal-artesunate-severe-malaria/en/.
Retrieving ARC from communities within 6 months is logistically challenging, costly, and risks stock outs
and loss of trust at community level. Robust data and operational research are needed to demonstrate the
stability of ARC under real field conditions, and pragmatic guidance is required for transportation storage
of ARC, particularly at community level. Careful quantification and distribution should be exercised to
avoid overstocking as well as stock outs and ensure uninterrupted availability.
CHWs receiving only small stocks of ARC may run out quickly, but cannot be expected to frequently travel
to health facilities for refills. Temporary stock outs at community level can therefore easily occur. These
stock outs can lead to poor satisfaction with CHW care and may negatively affect care-seeking behaviour.
Moreover, misunderstandings about ‘melting’ of capsules may lead to these being wrongly discarded by
CHW’s. To this end, a guidance document with simplified storage and transportation guidelines for ARC,
including education on ARC stability (‘melting’ is not a problem) should be created.
Concluding remarks
Effective strengthening of severe malaria systems requires not only funding and efforts to introduce
the ARC commodity, but should have a holistic focus on all commodities and components along the
continuum of care. This includes timely and feasible referral and ensuring the presence of higher-level
facilities that can provide the appropriate standard of care. In the meeting, it became apparent that
challenges in these aspects were similar across countries, and that more operational guidance in
“
introducing and scaling up ARC within the cascade of care to manage severely ill children is necessary.
The need for generating further stability data on ARC as well as better guidance on its storage and
transportation were identified as a priority.
The meeting was characterized by a very
high level of engagement and motivation
of both countries and partners. As a next
The need for generating step, countries are encouraged to develop
concrete action plans for the next 12
further stability data on ARC
months for the successful implementation
of ARC and Inj AS, along the lines of the
themes of the meeting: coordination,
as well as better guidance on service delivery pre- and post-referral,
referral, supply chain and surveillance.
its storage and transportation In late 2020 or early 2021, a similar
meeting may be organized with the aim
were identified as a priority.”
to share final CARAMAL study results and
discuss progress made in countries.
www.severemalaria.org
© March 2020 Medicines for Malaria Venture Medicines for Malaria Venture (MMV)
All rights reserved International Centre Cointrin - Route de Pré-Bois 20
Photos: Toby Madden (pp 1, 3 & 10), Damien Schumann (pp 2 & 5) PO Box 1826 - 1215 Geneva 15 - Switzerland
Design: Comstome-Geneva T +41 22 555 03 00 - F +41 22 555 03 69
www.mmv.org | communications@mmv.org
https://www.facebook.com/medicinesformalaria/ https://twitter.com/MedsforMalaria https://www.linkedin.com/company/medicinesformalariaventure Subscribe to our newsletter https://www.mmv.org/subscribeSevere Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 14
Annex 1: Agenda and List of Participants
Agenda
Day 1 – October 21, 2019 – Intercorp Hilton, Level M2, Borno-Rivers Rooms
Chair and co-chair: Olugbenga Mokuolu, NMEP, Chair / Jackson Sillah, WHO AFRO, Co-chair
Time Theme Session Speakers Time needed
7:45 – 8:00 Registration
8:00-8:15 Welcome and opening remarks Bala Audu, National 15 minutes
Coordinator, NMEP
Nigeria
8:15-8:30 Objectives of the meeting Jackson Sillah, WHO 15 minutes
AFRO
Co-chair
8:30-9:00 Setting the scene Current guidelines for the treat- Peter Olumese, WHO 10 minutes
ment of severe malaria Geneva
Severe malaria products Hans Rietveld, MMV 10 minutes
Roll out and uptake of Rectal Arte- Theodoor Visser, CHAI 10 minutes
sunate and Injectable Artesunate
9:00-9:05 Introduction of themes: Eliza Walwyn-Jones, 5 minutes
1. Coordination in funding and CHAI
implementation
2. Service delivery pre- and
post-referral
3. Referral
4. Logistics & supply chain mana-
gement
9:05-10:35 Theme 1: Coordina- Nigeria: Nnenna Ogbulafor, 15 minutes
tion in funding and NMEP
implementation
Moderator: Valenti- Uganda: Denis Rubahika, NMCP 15 minutes
na Buj
DRC: Rie Takesue - UNICEF/ 15 minutes
DRC
Remarks by severe malaria donors Jordan Burns, 15 minutes
PMI
Discussion with presenters and 30 minutes
audience
10:35-11:00 Coffee break 25 minutes
11:00-12:45 Theme 2: Introduction to session Christian Lengeler 10 minutes
Service
delivery pre- and Preliminary learnings on pre- and DRC: 30 minutes
post-referral post-referral care in CARAMAL Antoinette Kitoto Tshefu
Moderator: Chris- countries Uganda:
tian Phyllis Awor
Lengeler Nigeria:
Ocheche Yusuf
MMV rapid assessments Hans Rietveld, MMV 15 minutes
of severe malaria case
management:
Uganda, DRC, Liberia
…Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 15
Day 1. Continued
Understanding the role of and Alex Ogwal, CHAI 15 minutes
involving private sector providers Uganda
Continuum of care for severe Martin de Smet, MSF 10 minutes
malaria from community to
hospital
Discussion with presenters and 25 minutes
audience
12:45-1:45 Lunch
1:45-3:00 Theme 3: Learnings from CARAMAL on DRC: Antoinette Kitoto 30 minutes
Referral seeking, reaching and receiving Tshefu (10 mins/country)
Moderator: care Uganda:
Martin de Smet Phyllis Awor
Nigeria:
Ocheche Yusuf
Accessible & affordable transport Halima Abdu, Bauchi 10 minutes
from community to referral facility: Field Office, UNICEF
Emergency Transport System (ETS)
in Nigeria
Results and learnings from a Stephen Bwalya, 10 minutes
community-based severe malaria Zambia NMCP
pilot project in rural Zambia
Discussion with presenters 25 minutes
and audience
3:00-3:30 Coffee break 30 minutes
3:30-4:45 Theme 4: Rectal Artesunate supply chain Valentina Buj pre- 15 mins
Logistics and supply management: quantification, senting on behalf of
chain management transport and storage Uganda UNICEF
Moderator:
Hans Rietveld Rectal Artesunate supply chain Andrew Slade, MMV 20 minutes
and stability guidance
Novel storage ideas in a high Alain Mugoto, DRC 10 minutes
temperature setting: An example PNLP
from DRC
Discussion with presenters 30 minutes
and audience
4:45-5:10 Summary of day 1 with key Margriet den Boer, 25 minutes
takeaways Rapporteur
5:10-5:15 Day 2 logistics Eliza Walwyn-Jones 5 minutes
5:15-5:30 Closing Chair 15 minutes
…Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 16
Day 2 – October 22, 2019 – Intercorp Hilton Hotel, Level M2, Borno-Rivers Rooms
Time Theme Session Speakers Time needed
8:30-8:50 Day 1 Recap Rapporteur 20 minutes
8:50-9:00 Introduction to break out sessions Eliza Walwyn-Jones, 10 minutes
and reporting template CHAI
9:00-10:30 Country breakout sessions: 90 minutes
Rotations through 3 / 5 thematic
stations (30 minutes each)
10:30-11:00 Coffee break 30 minutes
11:00-12:30 Breakout sessions, continued: 90 minutes
Rotations through 5 / 5 thematic
stations (30 minutes each)
12:30- 2:00 Lunch 90 minutes
2:00-4:00 Country presentations to group 2 hours
on action plan broken down by
thematic areas
4:00-4:30 Break 30 minutes
4:30-4:50 Summary of day 2 with key Rapporteur 20 minutes
takeaways
4:50-5:00 Closing Chair 10 minutes
List of Participants
Halima Abdu Nigeria UNICEF
Adebimpe Adebiyi Nigeria Child Health Division
Isaac Adejo Nigeria MSH
Bosede Adeniran Nigeria Child Health Division
Issa Amadou Niger NMCP
Maureen Amutuhaire Uganda NMCP
Joselyn Atuhairwe Nigeria CHAI
Bala Mohamed Audu Nigeria NMCP
Phyllis Awor Uganda Makerere University
Patrick Bahizi Bizoza DRC WHO
Joel Naa Balbaare Ghana Global Fund
Philippe Batienon Senegal RBM
Sanjana Bhardwaj Nigeria UNICEF
Valentina Buj Switzerland UNICEF
Jordan Burns USA PMI
Stephen Bwalya Zambia NMCP
Mugoto Byamungu DRC MOH
Yakubu Cherima Nigeria Malaria Consortium
…Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 17
List of Participants. Continued
Welby Chimwani Kenya NMCP
Martin De Smet Belgium MSF
Clifford Dedza Malawi NMCP
Margriet den Boer UK rapporteur
Patience Dhliwayo Zimbabwe NMCP
Mércia Dimene Mozambique NMCP
Amadou Doucoure Senegal PNLP
Stephan Duparc Switzerland MMV
Perpetua Egonmwan Nigeria NMEP
Keith Esch USA PMI
Sonachi Ezeiru Nigeria CRS
Bosede Ezekwe Nigeria FMOH
Chizoba Fashanu Nigeria CHAI
Dale Halliday Switzerland Unitaid
Theotime Migan Benin NMCP
Uwem Inyang Nigeria PMI USAID
Olusesan Ishola-Gbenla Nigeria Management Sciences for Health
Mina Jaja Nigeria NMEP
Anitta Kamara Sierra Leone NMCP
Madina Konate Coulibaly Mali NMCP
Oumar Kone Mali PNLP
Sosten Lankhulani Malawi NMCP
Christian Lengeler Switzerland Swiss TPH
Christopher Lourenço USA PSI
Mark Maire Nigeria PMI / CDC
Momolou Massaquoi Liberia MOH
Anita Mbadiwe Nigeria CHAI
Elisa Miguel Angola NMCP
Wahjib Mohammed Ghana NMCP
Olugbenga Mokuolu Nigeria NMEP
Inocencia Morais Angola NMCP
Salou Mounkaila Niger NMCP
Eric Mukomena Sompwe DRC PNLP
Filipe Murimirgua Mozambique NMCP
Monique Murindahabi Ruyange Burkina Faso RBM
Ombeni Mwerindeo Switzerland Unitaid
Andriamananjara Mauricette Nambinisoa Madagascar NMCP
Christophe Ndoua CAR PNLP
Linda Nsahtime-Akondeng Nigeria UNICEF
Timothy Obot Nigeria NMEP
Dorothy Ochola-Odongo Nigeria UNICEF
Nnena Ogbulafor Nigeria NMEP
Alex Ogwal Uganda CHAI
Abraham Okita Nigeria CHAI
Placide Welo Okitayemba DRC iCCM Program
Charles Okon Nigeria Akena
Tayo Olaleye Nigeria CHAI
Carine Olinga DRC CHAI
…Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 18 List of Participants. Continued Peter Olumese Switzerland WHO Omokore Oluseyi Nigeria FMOH Femi Owoeye Nigeria BMGF Frederic Pinguedbamba Dianda Burkina Faso NMCP Oliver Pratt Liberia NMCP Abigail Pratt USA BMGF Tiana Ramanatiaray Madagascar NMCP Voahangy Razanakotomalala Madagascar NMCP Remi Peregrino Nigeria CHAI Hans Rietveld Switzerland MMV Denis Rubahika Uganda NMCP John Hafu Sande Malawi NMCP Vincent Sanogo Mali MOH Yacouba Savadogo Burkina Faso NMCP Silvia Schwarte Switzerland WHO Emmanuel Shekarau Nigeria NMEP Jackson Sillah Congo (Republic) WHO / AFRO Andrew Slade Switzerland MMV Laura Steinhardt Nigeria CDCP Rie Takesue DRC UNICEF Tinu Taylor Nigeria FMOH Jose Tchofa Nigeria PMI Soukeynatou Traore Nigeria Management Sciences for Health Andritiana Tsarafihavy Madagascar PMI Access Antoinette Kitoto Tshefu DRC Kinshasa School of Public Health Alhaji S Turay Sierra Leone MOH Joy Ufere Nigeria WHO Essien Ukanna Switzerland Unitaid Theodoor Visser USA CHAI Paul Waibale Liberia Management Sciences for Health Eliza Walwyn-Jones Botswana CHAI S. Olasford Wiah Liberia CHSD Bélia Xirinda Mozambique NMCP Ambachew Yohannes Switzerland Unitaid Ocheche Yusuf Nigeria Akena
Severe Malaria Global Stakeholder Meeting | 21-22 October 2019, Abuja, Nigeria 19
Annex 2: Pre-meeting Questionnaire
Interviewee Name and Function:
Country:
Date of interview:
Personal role in severe malaria case management:
Interview administered by:
Pre-meeting survey for severe malaria case management implementation experience
# Topic Are you inte- Are there If yes provide Comment
Theme
rested hearing experiences in contact details
from colleagues your country of resource
with experiences that would be persons or
in this topic/ relevant to agencies which
aspect? share with other has relevant
1. Low interest countries related experience to
2. Modest to this topic/ share on this
interest aspect? topic
3. High interest
(Note 1, 2 or 3) (Note Yes/No) (Name, Function,
phone or email)
1 How to deal with multiple actors, funding streams, supply
Coordination
lines and implementing agencies
2 How to harmonize NMCP, child health/community health
programs, pharmacy departments, and their policies/
guidelines
3 How to adequately conduct quantification, forecasting, and
Supply Chain Management
ordering of rectal artesunate and/or injectable artesunate
4 How to handle storage, transport, replacement of unused
rectal artesunate, and routine replenishment
5 How to handle transport and storage of rectal artesunate
when exposed to temperatures of 35-40 °C or higher
6 How to build awareness on signs of severe disease among
Behavior &
Communication
parents/caretakers; how to promote appropriate care
seeking behaviors
7 How to overcome reluctance/poor acceptability of rectal
artesunate by parents/caretakers
8 How to ensure accessible & affordable transport from
Referral
community to referral facility following administration
of rectal artesunate
9 How to involve informal and private providers
Service Delivery
(i.e., traditional healers, private sector) in early recognition
of severe febrile illnesses and prompt referral
10 How to ensure knowledge, skills and adherence
to guidance for diagnosis, treatment and referral
by Community Health Workers and/or PHC providers
11 How to monitor appropriate case management practices
with rectal artesunate (i.e., appropriately administration
to correct patients)
12 How to promote and monitor complete post-referral
treatment with injectable artesunate (instead of quinine)
and full course of ACT at referral facility level, including
appropriate case management for special groups
(e.g. pregnant women)You can also read