Selection in the social network - Effects of chronic diseases
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
C H R O M I C D I S E A S E S
Selection in the social network
Effects of chronic diseases
MARJA A.R. T1JHUIS, HENK D. FLAP, MARLEEN FOETS, PETER P. GROENEWEGEN *
Background: This article deals with the consequences of disease for someone's personal social network. It is
hypothesized that the duration of a socially severe disease will affect the social network in such a way that the
proportions of women, kin, long-standing relationships and people living nearby are higher for people suffering from
a disease longer. Contacts with colleagues will decline. Methods: These hypotheses were tested on the data of a
representative sample of the Dutch, gathered by means of a health interview (N=10,110). The presence and duration
of diseases were measured by a checklist of 23 chronic diseases. The social severity of a disease was determined
by its visibility, threat to others and functional disablement The network characteristics in this study were church
membership, membership of voluntary organizations, number of dose friends, number of supportgivers, proportions
of kin, women, colleagues, long-standing relationships and people living nearby. Gender, education, life-cyde stage
and work status were taken into account in all analyses. Results: Logistic and linear regression analyses showed that
the duration of a disease, whatever the degree of social severity, does not affect the network strongly. People
suffering longer from socially severe chronic diseases reported fewer friends and supportgivers. People suffering
longer from moderately severe chronic diseases reported fewer supportgivers for health-related support. The results
on socially mild chronic diseases were not in line with the expectations: people who are ill longer reported more
friends and fewer women In their network. Conclusion: We conclude that in a general population the duration of
diseases hardly has any effect on social network characteristics.
Key words: chronic diseases, selection, social network
T,he relationship between social networks and health is
often seen as a one-way-direction: social networks affect
sional helpers as networkmembers.6 Exchange theory also
predicts a change in network size, but the mechanism here
health.1 However, (chronic) disease also influences the is the balance of give and take in relationships. The
social network.2"6 In general, it is hypothesized that the exchange partner who is more dependent will attempt to
social network deteriorates with the duration of a disease. rebalance the relationship. An increase in the size of the
The theory on this subject is not clear about the mechan- social network will reduce per capita demands on each
ism responsible in the empirical association between net- helper and lessen the degree of imbalance within a parti-
work and illness.4 The convoy model expects an increased cular relationship.4 Janssen" argued on the basis of ex-
use but stability in size of the 'inner' circle.' Support in change theory that the number of networkmembers of the
cases of illness is derived almost totally from family mem- patient decreases depending on the degree to which the
bers in the 'inner' circle,4 and family relationships are health deviation is disabling. We propose yet a refinement
relatively stable over time. On the other hand, Litwak8 of these arguments with the help of a theory of social
theorized that networks will increase in size in response capital, which may explain why some of the theoretical
to a greater need for support: when the need for assistance perspectives mentioned are not supported by research
due to diminishing health exceeds the resources of the results. This theory refines the argument of Janssen
social network, additional (e.g. professional) helpers will through the specification of effects on several types of
be recruited. Usually though, the social network of people relationship characteristics.
suffering from a chronic disease is limited to informal The theory of social capital assumes that people have
contacts only, because respondents hardly report profes- access to the resources of the people they know. These
resources are called social or 'second order' resources,
* M A R . Tijhub1. H.D. Flap1. M. Foeti1, PS>. Groenewegen3-' meaning that networkmembers control the social re-
1 While conducting this research; NIVEL, Utrecht, the Netherlands currently
RIVM, CCM, Birthovtn, The Netherlands
sources the person has access to. 12 In order to achieve
2 ICS/Department of Sociology, University of Utrecht The Netherlands certain goals (such as health) people use their personal
3 NIVEL, Utrecht The Netherlands (e.g. economic, cultural and physical resources) and social
4 Department of Sociology, Department of Human Geography, University
resources. People who have more resources, including
of Utrecht The Netherlands
Correspondence: Marja Tijhuls. RIVM, CCM, P.O. Box 1, 3720 BA Bilthoven, social ones, are better able to achieve their goals.13 People
The Netherlands, tel. +31 30 2743438. fax +31 30 2744407 obtain social capital by investing in others: by entering inEffects of diseases on soaal networks
new relationships or expanding or preserving old rela- more life threatening, are progressing rapidly, produce
tionships. People invest in relationships to guarantee symptoms which are more visible and scare people off
future access or to repay investments in the past.11 The (cancer or AIDS). These three factors (functional dis-
idea of social capital implies that social resources play a ability, visibility and threatening nature of the disease)
more or less similar role in social life as economic, cultural are called the 'social' severity of a chronic disease.
and other resources do.11 Flap11 stated that social capital The cross-sectional nature of our data places limits on the
is more than a simple count of all the people in a network: possibilities of investigating the hypotheses. If the social
access to resources does not imply use. Social capital is the networks of those suffering from chronic diseases were
result of i) the number of people willing to support, ii) the compared with social networks of those not suffering from
resources that can be mobilized in this indirect manner diseases, a difference in network size could be caused by
and iii) the extent to which these people are willing or differences in size between those two groups before disease
committed to support. onset. Then the effects of chronic diseases on social
14
Fischer et al. underscored the influence of all kinds of networks could not be established. We therefore decided
constraints on the emergence and change of social net- to investigate the effects of duration of a disease on social
works. Disease is yet anodier restraint on network forma- networks. When a chronic disease is present for a longer
tion. Chronic disease may be detrimental to people's period of time, the patient usually will develop more
social networks in two ways. First, limitations caused by limitations and become more dependent of others.
diseases will limit die opportunities for new con- The central hypothesis to be tested in this article is that
tacts-'^'^and can also make it difficult for an ill person the duration of a disease will negatively affect personal
16
to invest in his relationships (even with money). Rela- networks of chronically ill people and even more so when
tionships widi people with whom one shares only one the disease is more 'socially' severe. The arguments for this
type of activity, a so-called uniplex relationship, are expected decline, found in the description of the theory
especially vulnerable when one person is no longer able of social capital on this subject and exchange theory
6
to continue this activity. Second, die use of resources according to Janssen are i) either the ill person or the
vested in relationships can become exhausted: the ill networkmember will break off an existing contact because
person requires more investments (social support) from of little investments in the past, which results in less
his supporters than he ever will be able to pay back. feelings of indebtedness on the side of the network-
To develop more specific hypotheses, relationships must member or in a growing imbalance in the relationship or
be distinguished according to the amount of investments ii) the contact is lost since the ill person shared activities
and to the extent of shared activities performed. Rela- with the network-member that he or she is no longer able
tionships of longer duration, such as, for example, those to perform or iii) because people with a chronic disease
usually with kin, will have a longer history of investments have fewer possibilities to make new contacts. These
and will therefore continue when someone develops a specific hypotheses cannot be tested with our data. What
chronic disease. Persons with whom one performs activ- can be tested are the implications of these hypotheses
ities together, as colleagues or co-members of organ- with respect to the composition of the social network. We
izations, are likely to disappear when someone develops a expect that the duration of the disease will affect the
chronic disease because one is no longer able to share in social network in such a way that the proportion of
these activities and there appear to be no alternatives. women, kin, long-standing relationships and people
Since the ill person is in greater need of social support but living nearby will be higher for people suffering from a
is not able to repay the services, only those relationships disease longer. A longer duration of a disease will be
will remain that entail more possibilities to give support accompanied by a decrease in contacts with colleagues.
(such as people living nearby). A relevant group in this These hypotheses were tested on the data of a national
respect is women. In The Netherlands the participation health survey in The Netherlands. The dataset allows us
of women in the labour force is still rather low compared to control for characteristics of the structural circum-
18
to other European countries, most women stay home stances people live under (gender, life-cycle stage, educa-
most of the time and are therefore more available to give tion and work status) that are both related to (chronic)
support. In general, since the patient is not able to repay disease and network characteristics.
these services, repayment may be accomplished by prior
investments or by services rendered by third parties. In METHODS
dense personal networks, A may get repaid for something Data was gathered as part of the national survey 'Morbid-
A did for B by C, because B did something for C once. ity and Interventions in General Practice',19 by means of
The remaining personal network will then have a dense a health interview. Respondents were selected through
structure, because people in the network have to be the administration of 161 general practitioners (a ran-
connected to make this type of repayment possible. dom, stratified, non-proportional sample, stratified in
Different diseases will not impair social networks in the terms of region, degree of urbanization and distance from
same way. The restrictions in functioning people have to a hospital). Since nearly all inhabitants of The Nether-
cope with because of illness can be more or less severe for lands are registered with a general practice and since the
people's social life.-' In addition, the type of illness mat- sample is quite similar to the Dutch population,20 our
ters: some diseases cause more anxiety because they are sample is representative. The total sample includedEUROPEAN JOURNAL OF PUBLIC HEALTH VOL. 8 1998 NO. 4
17,047 respondents, with a response rate of 77%. Only scores for the number of supportgivers for all support
the findings for respondents aged 18 years and over categories (range 0-6 and mean 3.9), health-related sup-
(N=10,110) are presented. port (range 0-2 and mean 0.6) and for support not related
For all analyses, respondents who reported a specific to health (range 0-4 and mean 2.0). Since the content of
chronic disease were selected. The presence of a chronic specific relationships was not investigated, these numbers
disease was measured by a checklist developed by Van den may be labelled indicators of social integration.
Bos 21 included in the health interview. For each of 23 The third type of indicator concerns the structure of the
diseases the respondent filled in whether he or she had social network. The measures available were related to the
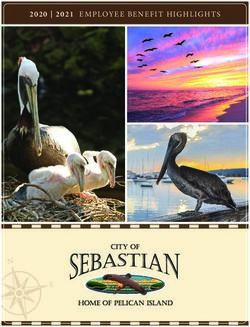
this disease and, if so, since when. 22 The prevalence support-giving network: proportion of kin, women, col-
figures for chronic diseases range from 1 to 15%(wble 1). leagues, long-standing relationships and people living
Most people in the population experience one or more nearby. 23 The mean percentage of women in the network
chronic diseases (55%). Fifty percent of all people that do is 60%, of kin 44%, of long-standing relationships 6 1 %
experience chronic diseases experience more than one. and 55% of the supportgivers lived nearby. The mean
These chronic diseases are categorized into three groups percentage of colleagues is rather low compared to the
according to their social severity (visibility of the disease percentages given above: 4%.
for others, threat to others and functional disablement of The analyses are controlled for gender, education, life-
the disease which may cause a need for help from others). cycle stage and work status of the respondents. Life-cycle
The categorization is presented in table 2. As no publica- stage was indicated by the combination of three personal
tions on the social severity of diseases were found, we characteristics: age (in three groups of 18-30 years, 31-55
categorized the diseases ourselves. The value of this cat- years and 55 years and over), having a partner and having
egorization will be discussed. children. The combination of these three characteristics
Network characteristics can be distinguished as three produces 12 groups; for each age group four combinations
types: 23 social integration, the content of social rela- of having children and partner status are possible. The
tionships (e.g. social support) and social network struc- most common life-cycle stage were people at the age of
ture. The indicators of social integration in our survey are 30-55 years with a partner and children (37%); the least
church membership and church attendance, membership present were people at the age of 18-30 years without a
of voluntary organizations, number of close friends and partner but with children (1%). Work status is broadly
number of people providing
support. Church member- Table 1 Chronic diseases, prevalence (percentage) and duration (N-10,110)
ship and attendance were Prevalence Duration in years
combined to measure active % Mean SD
membership. Of all respond-
Arteriosclerosis 0.7 6.9 6.2
ents selected (N=5,571), 15.2 12.5 11.1
Backache (slipped disc and sciatica)
32% reported being active in
Chronic bronchitis/emphysema or asthma 7.7 21.1 17.7
a church. More than half of
Chronic gastrointestinal disorders 4.4 12.4 12.1
the respondents selected
Chronic skin diseases/eaema 6.0 14.1 13.4
(53%) reported being a
Diabetes 23 9.7 11.6
member of voluntary organ-
Diseases of the nervous system (Parkinson's disease,
izations. The mean number multiple sclerosis and epilepsy) 1.4 15.2 13.5
of close friends was 6.6. Gallbladder and liver disease (including bilestones) 1.3 11.8 12.5
The second type of indic- Haemorrhoids 9.3 12.4 12.6
ators concerns support. To Hay fever 4.7 14.7 13.2
assess the amount and kinds Heart complaints or cardiac failure 6.4 93 11.4
of social support people ex- Hereditary handicaps 0.5 42.0 213
perience the exchange Hypertension 9.5 9.8 10.1
method was used. Re- Kidney disease (including kidney stones) 1.7 14.4 12.8
spondents were requested to Menstruation, menopause complaints" 3.2 10.2 10.0
name a maximum of three Migraine/chronic headache 10.6 15.6 14.2
people outside the house- Neoplasm/cancer (including leukaemia) 1.1 5.8 6.4
hold in response to six name- Prostatism/prostatis 1.2 4.9 63
generating questions, each Rheumatism/arthritis/arthrosis 3.7 11.5 11.4
referring to the provision of Serious consequences of accident 2.8 13.7 14.0
a specific type of social sup- Thyroid gland diseases 13 13.0 12.6
port. These questions can be Ulcus cruris 03 13.9 14.5
distinguished as two types: Varices 8.7 17.9 14.1
health-related support and
support not related to su For women only
b; For men only
health. 23 The questions were SI> Snndanl deviation
combined to compute sum-Effects of diseases on social networks defined as having a job or odier activities outside the tion. Arteriosclerosis, chronic bronchitis, diabetes, kidney household that could provide for social contacts. Half of diseases, neoplasm and ulcus cruris were not related to the respondents (48%) were integrated in the work force personal network characteristics. Lack of power, stem- (formally as well as informally). Our sample consisted of ming from die low prevalence of particular diseases, may fewer males than in the total sample (44 versus 54%) and have been a reason for some of diese results (for instance the educational level in the selection of respondents was on arteriosclerosis and ulcus cruris), but certainly not for somewhat lower than in the total sample (Pearsons % = all. For most odier diseases only one network charac- 255.2, df=4,p
EUROPEAN JOURNAL OF PUBLIC HEALTH VOL. 8 1998 NO. 4
no statistically significant relationships at all with church decline in social contacts through ageing. 28 - 29 For people
membership, membership of voluntary organizations and no longer active in the workforce, less severe effects are
having colleagues in the social network. also expected, because leaving the workforce is generally
The results for linear regression analyses are presented in related to a decline in social contacts. 30 One could argue
table 4. The number of friends, supporters and people who that the disease had caused leaving the workforce and that
gave health-related support was related to a shorter dura- controlling for work status would be unnecessary. How-
tion of severe chronic diseases, as expected. A higher ever, earlier results22 showed that half of the respondents
proportion of women, kin and long-standing relationships suffering from a chronic disease are still active in the
was related to a longer duration of severe chronic diseases, workforce. We do not know when the other half of these
as expected, but these coefficients are not statistically respondents left the workforce; this may have been before
significant. The results for people with moderate or mild or after the onset of the disease. Gender and education
chronic diseases are on the whole not in line with the also appeared to be major determinants of social network
expectations. characteristics. 23 ' 31 Women report to have more friends
and more people diey can rely on for support than men
DISCUSSION do. People with a lower education also report to have
The theory of social capital led us to expect that chronic more friends but name fewer people they rely on for
illness would have a deteriorative effect on personal net- support than higher educated people.
works. We expected chronic diseases to differ in their We must conclude in general, that the duration of disease
effects, depending on their social severity. It was hypo- does not have much effect on the personal network. Only
thesized that the duration of diseases would be related to for social moderate and severe chronic diseases are some
less involvement in church and other informal organ- relationships found that are in line with the expectations.
izations and to fewer friends, fewer supportgivers and For social severe chronic diseases negative relationships
colleagues left in the network. Other studies showed that between the number of friends, the number of supporters
a relationship may break up not only because the sup- (in general and with regard to health-related matters) and
porter is no longer willing to support (because he no the duration of these diseases are found. For moderate
longer feels indebted and sees no future repayments for chronic diseases the number of supportgivers with regard
his services from the ill person), 15 but also because the ill to health-related matters is related negatively to the dura-
person does not want to be a burden any longer. The tion of these diseases. Other results for moderate chronic
duration of diseases will be related to the structure of the diseases are not statistically significant. The statistically
personal networks in such a way that the proportion of significant results reported on mild chronic diseases are
women, kin, long-standing and nearby living rela- not all in line with the expectations. The number of
tionships will be higher for people suffering from a disease friends is positively related to duration and the proportion
longer. In the analyses we controlled for gender, life-cycle of women is negatively related to duration for these
stage, education and work status because these factors are diseases.
both related to (chronic) disease and to network charac- Our results do not present strong evidence for selection
teristics. For instance, the consequences of a chronic effects triggered by disinvestment in each other after the
disease for the social network are probably less severe for onset of a chronic disease. One might object, however,
older people, because they are already confronted with a that a cross-sectional design such as we use is not optimal.
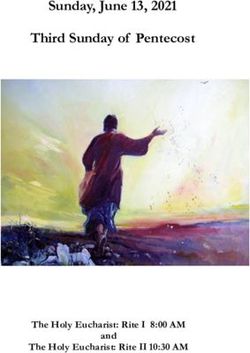
Table 3 Results of logistic regression analyses to determine associations between network characteristics and the duration of a chronic
disease, controlled for gender, educaoon, life-cycle stage and work status
Model A 1 Model Bb Model C°
Dependent variable N Log-likelihood X2 change X change X2 change B
Active church membership
Duration of Severe diseases 1,012 1,27935 13.78 50.67 0.01 -0.01
Moderate diseases 2,633 3326.86 62.39 93.56 0.07 0.01
Mild diseases 1,226 1,516.33 24.62 85.95 0.16 -0.01
Membership of voluntary organizations
Duration of Severe diseases 1,012 1,401.02 42.12 12.68 0.18 -0.01
Moderate diseases 2,633 3,638.21 123.51 62.49 0.41 -O.01
Mild diseases 1,226 1,692.98 45.94 38.44 0.45 0.01
Colleagues in the social network
Duration of Severe diseases 935 555.74 29.53 82.63 1.59 -0.01
Moderate diseases 2396 1366.51 80.78 136.08 0.02 0.01
Mild diseases 1,134 708.76 47.80 46.58 0.98 -0.01
a: Model including gender and education
b: Model also including life-cycle stage and woric status
a Model abo including duration of diseases
None of the B coefficients is statistically significantEffects of diseases on social networks
A longitudinal study of people not chronically ill at Another method used several times, is a longitudinal
baseline is preferred. Some of them would develop one or study in which personal networks of patients are com-
more chronic diseases. Such a researchproject would be pared at several points in time. The results may be biased
rather costly and time-consuming. However, we believe in this type of study when time intervals are chosen such
other methods would be biased. For instance, when per- that network changes remain undetected.32 De Witte's5
sonal networks of chronically ill and a matched healthy multiwave study on patients suffering from spinal cord
group are compared, there is a chance of mixing the effects injury, ankylosing spondylitis and rheumatoid arthritis is
of networks on diseases with the effects of diseases on an example. He reported a smaller network, fewer friends
networks. An example of this method is the longitudinal and other non-kin relationships for patients two years
study of Janssen.6 She compared the personal networks of after admission to a rehabilitation centre than at ad-
a healthy group with those of patients suffering from mission. Between discharge and three months later the
ankylosing spondylitis or Crohn's disease on three occa- personal networks first shrink, then grow a bit and finally
sions. The patients reported fewer informal networkmem- end at a lower level than at admission.
bers and less emotional support received than the healthy The two studies5'6 partly used the same measurement of
group. The size of the network shrinks when the disease personal networks. They both invited the respondents to
is present for a longer period. name the people with whom they had good personal ties.
Table 4 Results of linear regression analyses to determine associations between network characteristics and the duration of a chronic
disease, controlled for gender, education, life-cycle stage and work status
Model A" Model Bb Model C B(not
Dependent variable N Total R 2
Total R2 Total R2 standardized)
Number of friends
Duration of Severe diseases 913 0.0021 0.0110 0.0160 -0.04*
Moderate diseases 2,308 0.0039 0.0119 0.0134 0.02
Mild diseases 1,095 0.0040 0.0278 0.0327 0.04*
Number of supportgivers
Duration of Severe diseases 1,012 0.0540 0.1064 0.1130 -0.01 **
Moderate diseases 2,633 0.0456 0.0743 0.0744 -0.01
Mild diseases 1,226 0.0670 0.1000 0.1001 0.01
Number of supportgivers for health-related support
Duration of Severe diseases 1,012 0.0553 0.0885 0.1004 -0.01 *•*
Moderate diseases 2,633 0.0616 0.0952 0.0983 -0.01 •*
Mild diseases 1,226 0.0906 0.1370 0.1397 -0.01
Number of supportgivers for support not related to
health
Duration of Severe diseases 1,012 0.0968 0.1488 0.1493 -0.01
Moderate diseases 2,633 0.1080 0.1473 0.1483 -0.01
Mild diseases 1,226 0.1223 0.1590 0.1591 0.01
Proportion of women
Duration of Severe diseases 981 0.2783 0.2884 0.2884 0.01
Moderate diseases 2,493 0.2857 0.2962 0.2972 -0.01
Mild diseases 1,179 0.3081 0.3160 0.3194 -0.01*
Proportion of kin
Duration of Severe diseases 981 0.0606 0.1324 0.1339 0.01
Moderate diseases 2,493 0.0493 0.0928 0.0928 0.01
Mild diseases 1,179 0.0707 0.1280 0.1280 -0.01
Proportion of people living nearby
Duration of Severe diseases 981 0.0211 0.0362 0.0371 -0.01
Moderate diseases 2,493 0.0185 0.0319 0.0320 -0.01
Mild diseases 1,179 0.0234 0.0412 0.0413 0.01
Proportion of long-standing relationships
Duration of Severe diseases 981 0.0680 0.2048 0.2058 0.01
Moderate diseases 2,493 0.0653 0.1904 0.1904 -0.01
Mild diseases 1,179 0.1226 0.2791 0.2804 0.01
a- Model including gender and education
b: Model also including life-cycle stage and wort: status
c. Model also including duration of diseases
Statistical significances * pEUROPEAN JOURNAL OF PUBLIC HEALTH VOL. 8 1998 NO. 4
This method appears better than asking people about supportgivers (and related to this also our measurements
specific transactions (at least in the case of chronically ill of the structure of the social network which concern only
persons), because not being able to perform these trans- the support-giving part) is limited to a maximum of six
actions would bias the network size. A study that did persons. We would have preferred a longer list of name-
measure network size by counting the number of support- generators of supportgivers and their characteristics. One
givers apart from an eventual partner showed that net- can also question the hypotheses, more specifically the
work size increases.^ The respondents, elderly people, nature of the relationship between disease duration and
developed more disabilities and needed and received social network. We assumed this relationship to be linear.
more support at time 2 than at baseline. It seems possible that the effect of the development of a
A remark about all these studies is that they did not chronic disease for the social network is first positive, later
incorporate measures of social integration. The 'outer' on negative and stable in the last stage. Through the
circle (fewer close contacts, as measured by social in- occurrence of a disease people will visit the patient.
tegration) would be affected by the onset of a chronic Because of getting used to the disease, people may lose
disease according to Kahn and Antonucci whereas the interest in the patient and the mechanism of de-
'inner' circle (people close to the person at focus) would terioration starts to operate. In die last stage the patient
not. Yet, in his study on mental health and social selec- has become used to his disease and may start to rebuild
tion, Johnson showed that more distress at baseline is his life again and also his social network. Whether this
related to fewer primary ties (close friends and relatives, stage process actually operates must be investigated for
the 'inner' circle) at time 2. The secondary ties (the 'outer' specific diseases, following the people who suffer from
circle, measured by the number of voluntary groups or these diseases and their social networks from disease onset
organizations one participates in and church attendance) for a longer period of time.
at time 2 were not affected by distress at baseline. Our Since other researchers selected respondents with severe
results also do not make clear that the 'outer' circle chronic diseases and we studied a general population, it
(measured by active church membership and membership is not surprising that we find relatively small effects on
of voluntary organizations) is affected. Our results and the characteristics of the social network. Since our data
those of others showed that the 'inner' circle is (some- comprehend many respondents and measurements with
what) affected by the onset of a chronic disease. regard to chronic diseases and the social network, we
After having described other studies and their weak- think we have made a point. After taking the effects of
nesses, it is time to discuss the limitations of our study. gender, education, life-cycle stage and work status into
Our research population consisted of a representative account, the duration of diseases hardly bears any effect
sample of the Dutch, of whom 55% reported suffering on social network characteristics. The design and vari-
from one or more chronic diseases. This percentage may ables in control should be considered thoroughly by future
seem rather high, but is not surprising since the list also researchers.
includes rather common and mild diseases (backache, hay
fever and migraine/chronic headache). These diseases The work reported here is supported by NWO, grant number 500-
and their duration are self-reported. Van den Bos21 com- 279-202 as part of a larger study on social networks and healrJi. Some
pared self-reported data gathered widi an identical list of of these results were presented in Amsterdam, in 1993, at die
International Conference on Chronic Diseases and Changing Care
diseases with medical records and found good cor-
Patterns in an Ageing Society.
respondence for most diseases in our study. Thus, we have
little reason to doubt these data. One may have doubts on
the categorization of social severity, which was based on
the judgments of one of the authors and discussed and
agreed upon within the group of all authors. This 1 Cohen S, Syme SL, editors. Social support and hearth.
Orlando: Academic Press, 1985.
categorization does not allow for individual variability. 2 Johnson TP. Mental health, social relations, and social
However, since the duration of severe chronic diseases selection: a longitudinal analysis. J Hrth Soc Behav 1991;32:4O8-23.
clearly has other effects on social networks than the 3 Lyons RF. The effects of acquired illness and disability on
friendships. In: Perlman D, Jones W, editors. Advances in
duration of moderate or mild chronic diseases and since personal relationships 3. London: Jessica Kingsley Publishers,
these results are comparable to the results found in the 1991:233-76.
analyses for each particular disease, our distinction makes 4 Stoller EP, Pugliesi KL Size and effectiveness of informal
helping networks: a panel study of older people in the
sense. It would be preferable, of course, to construct a community. J Hrth Soc Behav 1991:32:180-91.
categorization in a more distinguished way. 5 De Wrtte L After the rehabilitation centre: a study into
Co-morbidity was present in half of the respondents re- the course of functioning after discharge from rehabilitation.
Amsterdam/Lisse: Swets & Zeitlinger, 1991.
porting a chronic disease. Only 3 % of the analyses on 6 Janssen M. Personal networks of chronic patients.
co-morbidity in each disease (results not shown) showed Maastricht: Datawyse, 1992.
statistically significant relationships with the network 7 Kahn RL, Antonucci T. Convoys of social support: a life
course approach. In: Kiesler SB, Morgan JN, Oppenheimer VK,
characteristics, although the power for most of these editors. Ageing: social change. New York: Academic Press,
analyses was good. 1981:383-405.
8 Litwak E. Helping the elderly: the complementary roles of
A further comment can be made on the measurements of Informal networks and formal systems. New York/London:
the social network. Our measurement of the number of Guilford Press, 1985.Effects of diseases on social networks
9 Bourdieu P. Le capital social: notes provisoires (The social 21 Van den Bos GAM. Zorgen van en voor chronisch zieken
capital: preliminary notes). Actes de la Recherche en Sciences (Care for the chronically ill). Utrecht Bonn, Schettema &
Sociales 1980;3:2-3. Holkema, 1989.
10 Coleman JS. Social capital in the creation of human 22 Tijhuis MAR, Flap HD, Foets M, Groenewegen PP.
capital. Am J Sociol 1988;94:s95-120. Kenmerken van sociale relaties en gezondheid (Characteristics of
11 Flap H. Conflict loyalty, and violence. Frankfurt- social relations and hearth). Tijdschr Soc Gezondheidsz
Peter Lang, 1988. 1994;72:341-51.
12 Boxman EAW. Contacten en carriere: een 23 Tijhuis MAR, Flap HD, Foets M, Groenewegen PP.
empirisch-theoretisch onderzoek naar de relatie tussen sociale Netwerken in Nederland: een onderzoek naar persoonlijke
netwerken en arbeidsmarktposlties (Contacts and careers: an netwerken van Nedeiianders (Networks in The Netherlands: a
empirical-theoretical study on the relationship between social study of personal networks of the Dutch). Mens en Maatschappij
networks and labour market positions). Amsterdam: Thesis 1992;67:5-22.
Publishers, 1992. 24 Fischer CS. To dwell among friends: personal networks of
13 Campbell KE, Marsden PV, Hurlbert JS. Social resources in town and city. Chicago: Chicago University Press, 1982.
and socloeconomic status. Soc Networks 1986;8:97-117. 25 Hosmer DW, Lemeshow S. Applied logistic regression.
14 Fischer CS, Jackson RM, Stueve CA, et al. Networks and New York: Wiley, 1989.
places: sodal relations in the urban setting. New York: The Free 26 Weisberg S. Applied linear regression, 2nd ed. New York:
Press. 1977. Wiley, 1985.
15 Rounds KA, Israel BA. Social networks and social support: 27 Joosten J, Van der Horst F, De Witte l_ Chronlsche
living with chronic renal disease [Review]. Patient Educat Counsel patienten en hun sociale contacten (Chronic patients and their
1985,7:227-47. social contacts). Paper for the Dutch-Flemish Days for Sociologists,
16 Fischer CS. The friendship cure all. Psychol Today 1986.
1983; 1:74-8. 28 Shulman N. Ufe-cycle variations in patterns of close
17 Tolsdorf CC Social networks, support, and coping: an relationships. J Marriage Family 1975;37:813-21.
exploratory study. Family Process 1976;4:407-17. 29 Fischer CS, Oliker SJ. A research note on friendship,
18 Hooghiemstra BTJ, Niphuis-Nell M. Sociale atlas van de gender, and the life-cycle. Soc Forces 1983;62:124-33.
vrouw. Deel 2: arbeid, inkomen en fadliterten om werken en de 30 Sprengers M, Tazelaar F. Werkloosheid en sociaal netwerk
zorg voor klnderen te comblneren (Women's sodal atlas. Vol. 2: (Unemployment and social network). In: Spruit IP, Tazelaar F,
employment income and facilities to combine work with caring editors. Leven met werkloosheid (Living with unemployment).
for children). Rijswijk: Sociaal en Cultured Planbureau, 1993. Groningen: Worters-Noordhoff, 1987:39-48.
19 Foets M, Van der Velden J, De Bakker D. Survey design: 31 Marsden PV. Core discussion networks of Americans.
National Study of Morbidity and Interventions in General Research note. Am Soc Rev 1987;52:122-31.
Practice. Utrecht NIVEL, 1992. 32 Schulz R, Tompkins CA. Life events and changes In social
20 Foets M, Van der Velden J. Een Nationale Studle van relationships: examples, mechanisms, and measurement J Soc
Ziekten en Verrichtingen in de Huisartspraktijk. Basisrapport C1in Psychol 1990;9:69-77.
meetlnstrumenten en procedures (National study of morbidity
and interventions in general practice. Basis-report: measurements
Received 19 March 1997, accepted 14 August 1997
and procedures). Utrecht NIVEL, 1990.You can also read