Secondary AML and MDS - ALAN - July 6, 2021 Moshe Mittelman Tel Aviv, Israel - Acute Leukemia Advocates ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Secondary AML and MDS
ALAN – July 6, 2021
Moshe Mittelman
Tel Aviv, Israel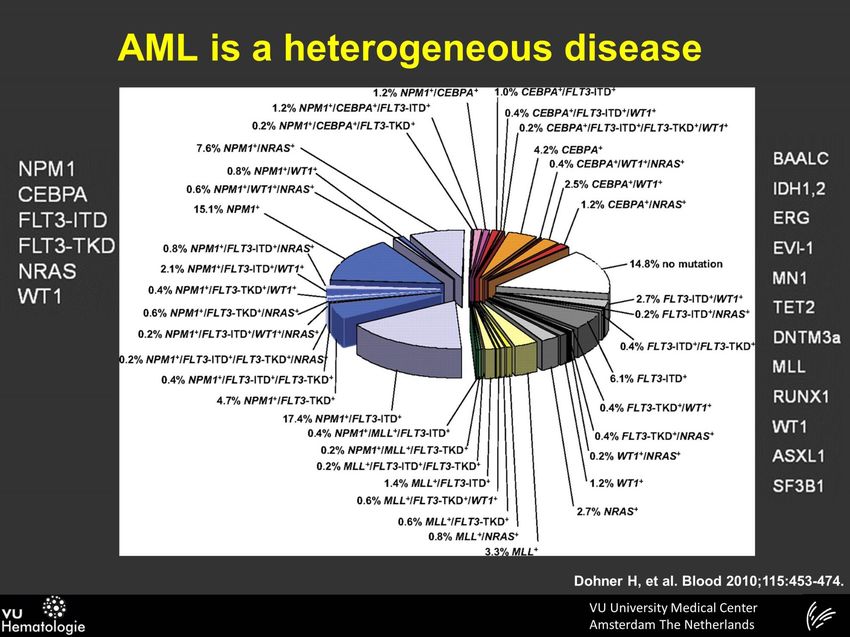
MM: Disclosures
Research funding:
Amgen; Celgene; Johnson & Johnson; Roche;
Novartis; Gilead; Takeda
Speakers’ bureau:
Johnson & Johnson; Novartis
Advisory boards:
Pfizer; Amgen; Roche; Novartis; Takeda; Silence
What are we talking about ?
Secondary (acute myeloid) leukemia
A collective term used to describe
a group of patients with acute myeloid leukemia (AML)
or myelodysplastic syndrome (MDS) with a history of
exposure:
environmental, occupational, chemo, radiation, …
Following hematologic disease (MDS)
We will describe the spectrum starting with MDS and
progressing to acute (myeloid) leukemia (AML)
3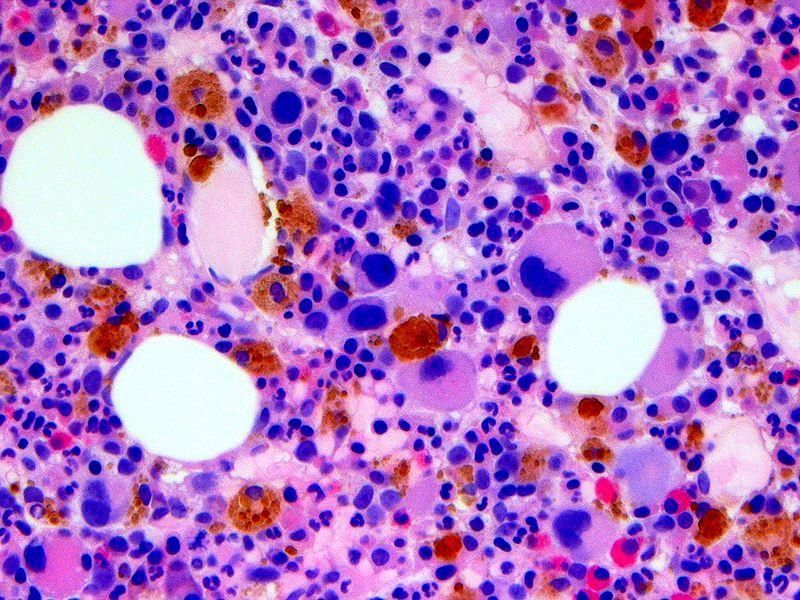
1986: My trip began… Heme-Onc Fellowship – GW – NIH (USA) 1986-1989
Sec AML / MDS: 60 sec (I)
Bone marrow disease
Wear & Tear problem
Slowly progressive
Wide spectrum
Phases:
(“Pre-MDS”)
MDS
Intermediate MDS-AML
Acute leukemia (AML)
5
MDS and AML: 60 sec (II)
• Myelodysplastic syndromes evolve into acute leukemia
• Age-related clonal hematopoietic stem cell disease(s)
• Ineffective hematopoiesis:
• Abnormal differentiation, maturation, impaired apoptosis
• Genetic (Immune) basis + environmental exposure
• Involvement of the immune system
• Median age: 74 years
• Incidence increases with age (40–50/100 000 in > 70yr)
• Anemia (90%); Pancytopenia (50%)
• AML Transformation (20%-60%)
Mittelman M Isr J Med Sci 1990;26:468; Malcovati L, Blood 2013;122:2943;
Tefferi A, NEJM 2009;361:1872; Ades L Lancet 2014;383:2239;
Garcia-Manero G, AJH 2020;95:1399; Cazzola NEJM 2020;383:1358
Sh.Y. (20th Century)
• 1983
• 67 yo, lady, painter (dyes exposure)
• weakness, macrocytic anemia
• BM: mild dysplasia, 3% blasts, 5q-
• 1986
• Blood (RBC) transfusions
• 1989
• Pancytopenia, BM: 10% blasts
• Low -dose Ara C:
• One cycle - no reaction; intolerance
• 1990
• Leukemic transformation
• Course: chemo (7 + 3), died
LS (21st Century) 2001: 82yo lady, hair stylist, asymp. anemia – FU 2004: Mild weakness; BM: MDS, 3% Bl, 5q-, FU 2005: Hb decline – transfusions- EPO- response ! 2007: Transfusions, Len, response for 26m 2009: Pancytopenia; BM: 10% blasts, Aza – CR 2011: Pancytopenia, bleeding, PLT 15k, eltrombopag Excellent PLT rise – survived brain bleeding ! 2013: AML – azacitidine – Complete remission 2017: Deterioration, relapse, sepsis, died (98yr)

Epidemiology
Age:
8th decade
Median – 74 yr
Registries:
25 new patients /100,000/yr
Etiology (Causes)
Unknown
Leukemogenic:
Radiation
Chemotherapy
Alkylating agents
Chemical: benzene, organic
Drugs: chemo, NSAIDs, Chloramphenicol
Viral (?)
Genetic
Multifactorial
Diseases: PNH, AADistribution by Age and Gender (A. Carmi)
Age at diagnosis
female
Patients
male
AgeWhen to suspect? • Older patient (70+) • Macrocytic anemia • Leukopenia, thrombocytopenia • Other causes of anemia – excluded • Vitamin B12 deficiency, Folic acid, hemolysis • Hypothyroidism, liver disease, viral • In younger people: • After chemotherapy • Secondary MDS
Recurrent Karyotypes in MDS (n=3856)
Schanz J et al - ASH 2009 abstract #2772MDS: Genetic- Recurrently Mutated Genes
(Malcovati L, Blood 2013; 122:2943; ELN 2014)
Gene Frequency (%) References
SF3B1 25-30% Yoshida, Nature 2011; Malcovati Blood 2011
TET2 20-25% Delhommeau, NEJM 2009
RUNX1 10-20% Chen CY, BJH 2007; Dicker, Leukemia 2010
ASXL1 10-15% Bejar NEJM 2011; Thol F JCO 2011
SRSF2 10-15% Yoshida, Nature 2011; Thol F , Blood 2012
TP53 5-10% Bejar NEJM 2011; Padua RA, Leukemia 1998
U2AF1 5-10% Yoshida, Nature 2011; Graubert NatGen 2011
NRAS/KRAS 5-10% Dicker, Leukemia 2010; Paguett Blood 1993
DNMT3A 5% Walter M, Leukemia 2011; Thol F Haematologica
ZRSR2 5% Yoshida K, Nature 2011; Thol F, Blood 2012
EZH2 5% Nikoloski G, Nat Gen 2010; Emst T, Nat Gen 2010
IDH1, IDH2 2-3% Bejar R, NEJM 2011; Kosmider O, Leukemia 2010
ETV6 2% Bejar R, NEJM 2011;
CBL 1-2% Bejar R, NEJM 2011;
NPM1 1-2% Bejar R, NEJM 2011; Dicker F, Leukemia 2010
JAK2 1-2% Bejar R, NEJM 2011; Steensma DP, Blood 2005
SETBP1 1-2% Piazza R, Nat Gen 2013;Age Related Clonal Hematopoiesis
Whole exome sequencing; peripheral blood; 17,182 persons
Looked for somatic mutations in 160 “hematologic” genes
Results;
Rare mutations in < 40 yr
70-79 yr: 9.5% with clonal mutations
80-89 yr: 11.7%
90-108 yr: 18.4%
Common mutations: DNMT3A, TET2, ASXL1
Somatic mutation was associated with increased risk of
Hematologic cancer (HR 11.1)
All -cause mortality (HR 1.4)
Coronary dis. (HR 2.0); Ischemic stroke (HR 2.6)
Jaiswal S et al. N Engl J Med 2014; 371: 2488Evolution: From ICUS to AML
Steensma D et al., Blood, April 30, 2015
Traditional ICUS MDS by WHO 2008
No clonal CHIP CCUS LR-MDS HR-MDS AML
ICUS
Clonality - + + + + +
Dysplasia - - - + ++ ++
Cytopen. + - + + ++ ++
BM blasts < 5% < 5% < 5% < 5% < 19% > 20%
Risk Very low Very low Low (?) Low/Int High High
Treat Obs/BSC Observat. Obs/BSC/ Obs/BSC/ HMA / SCT Chemo /
GF GF/Imids/I HMA / SCT
ST
-----------Clonal cytopenias-------------
ICUS- Idiopathic cytopenia of undetermined significance; CCUS – Clonal cytopenia of US
Age-related clonal hematopoiesis (ARCH) (Jaiswal S NEJM 2014;371:2488)Clinical Picture
General symptoms:
Weakness
Weight loss
Fever
Bone marrow failure:
Anemia – weakness, fatigue
Cardiovascular complications
Low WBC – infections
Low PLT - bleeding
19AL – Common Features: Clinical
Symptoms/ complications:
Non-specific – generalized (“B”)
Hematologic – related to BM
Anemia; Leukopenia; Leukocytosis; Low PLT
Organ-related complications
Treatment-related complications
Generalized complications
Untreated – rapid lethal course
Treatment: Aggressive; Potential cureAL - Complications Infections: Bacterial; fungal; viral; parasites; mycobacterial Metabolic: Fluid / electrolyte imbalance: Ca; K; Na; Mg Tumor lysis syndrome (TLS) Hyperleukocytosis; DIC Neutropenic enterocolitis Organ involvement: CNS; testicular; Renal; Eyes; any organ…
Impaired Quality of Life Mobility Self care Usual activities Pain / discomfort Anxiety / depression VAS – self rated health pinterest.com
EU: Impaired QoL vs Healthy p < 0.001, p< 0.01, p
Biology & Pathogenesis Environmental factors (leukemogenic) Radiation; Chemical (drugs, benzene); Viral Cytogenetics Genetic (instability); Epigenetics Immune system BM microenvironment (angiogenesis) Cytokines Predisposing disorders (MPN, PNH, AA) Multifactorial (host, external) Intracellular: apoptosis, clonal expansion
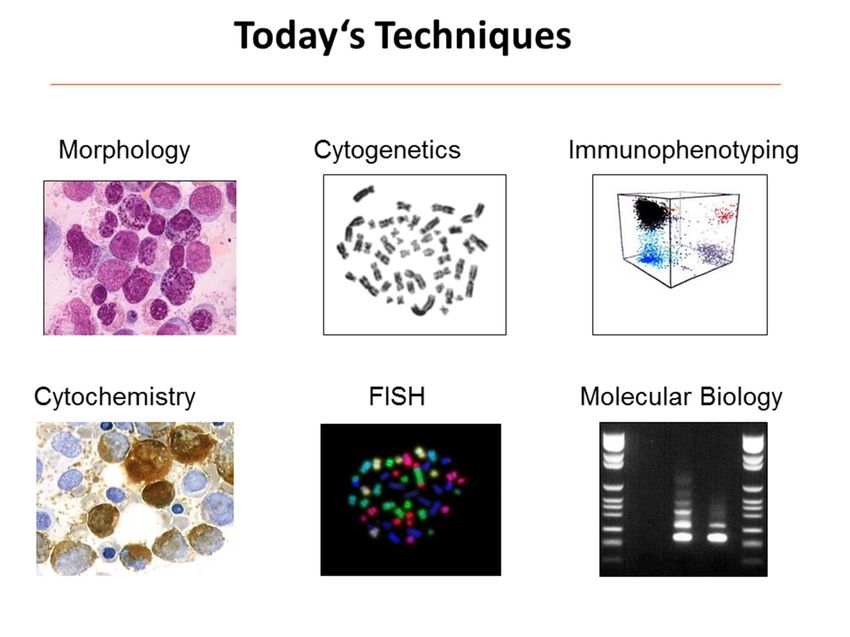
Bone Marrow Examination Biopsy A bone (marrow) sample A solid cylinder of tissue Findings: Structure; Cellularity; Foreign Islands Time frame: (5-10) days (Touch prep can bridge) Aspiration Liquid from the bone marrow Findings: single cell morphology Time frame: hours
MDS/AML Diagnosis: Based on BM
Clinical picture
Age; Normal
anemia; cytopenia
MCV
Exclude other reasons
Bone marrow
Aspirate; Biopsy
Morphology
Dysplasia, MDS
Blast (20-30%) - AML
Additional:
R.sidero; Mono; Fibrosis
Tefferi A, NEJM 2009; 361: 1872; Malcovati L, Blood 2013; 122:2943; ELN 2014;
Arber DA, Blood 2016; 127: 2391; Weinberg OK, Semin Hematol 2019; 56: 15BM in MDS: Several types of immature cells
Acute Leukemia: Blasts in BM & PB
AL Dg:
ELN - EUMDS Countries Austria Reinhard Stauder Czech Republic Jaroslav Cermák France Pierre Fenaux Germany Ulrich Germing Greece Argiris Symeonidis Italy Luca Malcovati Netherlands Saskia Langemeijer Romania Aurelia Tatic Spain Guillermo Sanz Sweden Eva Hellström-Lindberg United Kingdom David Bowen (Co-chair) Denmark (2009) Mette S. Holm Portugal (2010) Antonio Medina Almeida Poland (2010) Krzysztof Mądry Israel (2012) Moshe Mittelman Serbia (2013) Aleksandar Savic Croatia (2013) Njetočka Gredelj Šimec Project Coordination Theo de Witte (Chief Investigator & Chair) Project Management Radboudumc Nijmegen, NL - Corine van Marrewijk Data Management & Statistics University of York, UK - Alex Smith
MDS Diagnosis (2013): Mandatory
Exclude other reasons for cytopenia
Peripheral Blood
Dysplasia (1-3 lines), Blasts
Bone marrow Aspirate:
Dysplasia, Blast % (1-20%), Ring sideroblasts
Bone marrow biopsy:
Cellularity; CD 34+ Cells; Fibrosis
Cytogenetics:
Clonal abnormality ( G- Banding)
(FISH, FCM, Molecular – Recommended)
Malcovati L, Blood 2013; 122:2943; ELN 2014Do all patients need BM for Diagnosis ?
BM exam – gold standard
But…
Invasive; Painful
Possible bleeding
Low PLT
Difficult for elderly
Subjective interpretation
Can we diagnose w/o BME ?A simple modle can dg/exclude MDS
Figure: MDS Predictive Modelling Dg
63
10.9 2.6
48 124
shiny.york.ac.uk/mds
1.3 0.2
122 0.88
Green Brown Red
Oster HS Bl Adv 2021
Figure: The web application; ten variables are entered. For this patient, the
blue line in the red region predicts probable MDS (pMDS).Can We Detect Pre-MDS ?
Early detection
Pre-disease states
Tools:
Genetic
Digital; Big DataPre-MDS: Hb declines before MDS diagnosis
E-data (420 pts), CBC/yr > 3yr prior to MDS diagnosis
Joffe E et al, Hematol Oncol 2020;38:782French-American-British Co-Operative Group, circa 1990
David Galton,
London
Georges Harvey Marie-
Daniel Flandrin, Gralnick, Claude S.
Thérèse John M.
Catovsky, Paris Bethesda Daniel, Paris Bennett, Sultan,
London Rochester Paris
RIP:
Sultan, 1992
Galton, 2006Prognostic Parameters
Included in prognostic models:
% blasts
Cytogenetics
Blood counts
Not included (yet ?)
Genetic mutations
Age
Co-morbidities
Others ??
39MDS: FAB Classification
FAB Type BM Blasts Other Incid. Dyspo.
criteria
RA < 5% 30% +
RARS < 5% R.Siderob 20% +
RAEB 5-20% 20% ++
CMML 1-20% P.Mono 15% ++
RAEB-t 21-30% Auer rods 15% ++/+++
Bennett JM; BJH 1982MDS Prognostic Classifications
FAB: % blasts (+ morphology)
International Prognostic Scoring System (IPSS)
Prognostic parameters
BM % blasts (+morphology)
Cytogenetics: “good”; “bad”
# Lineages affected
Low-risk (LR); Intermediate -1: Lower risk
Intermediate-2; High-risk; Higher risk
IPSS-R (revised; use #):
Very low; Low; Intermediate; High; Very high
Bennett JM, BJH 1982; Greenberg P, Blood 1997; 2012MDS: Secondary MDS
Following a muatgen for HL, Breast Ca…
chemotherapy / radiotherapy exposure (1-10 yr)
Younger age
Hypocellular BM, fibrosis
Cytogenetics: 90% abnormal (ch 5,7, 3q)
Clinical:
Advanced; Rapid course; Resistant; Leukemic
transformation; Poor prognosis (Management
MDS Treatment – General
Treatment depends on:
Disease status (IPSS/R)
Lower risk MDS
IPSS: Low risk; Intermediate-I
Higher risk MDS
IPSS: Intermediate-II; High risk
Acute leukemia
Patient
Age; co-morbidities; functional
QoL; Pt reported outcomes (PRO)Evaluation of Treatment Response – Not B&W:
Response Criteria
Acute Leukemia: CR (< 5% blasts)
IWG 2000 / 2006:
Complete response (CR)
Marrow CR (mCR); (Partial R)
Cytogenetic response (Cyt R)
Hematologic improvement (HI)
Erythroid (HI-E); Neutrophil; Platelet
IWG 2018: HI-E - Erythroid response
Transfusion burden:
Non (0/16 wk), Low (3-7); High > 8
Response: minor (50% less) or major (TI)
Cheson BD, Blood 2000; Cheson BD 2006; Platzbecker U, Blood 2019MDS EUROPE Guidelines (2019)
Treatment of Anemia
MDS Treatment for Anemia:
RBC Transfusions- Still
~ 80% of MDS patients
have a hemoglobinRBC Transfusions in MDS/AML
RBC-Transfusions – mostly used (50%)
Complication: Iron overload
No disease progression !
Hb threshold ?
Often Hb< 7 g/dl; but Individualize
Hb target ? No target
Transfusion frequency ? As needed (for the pt and doctor)
Consider: Symptomatic benefit vs toxicity
Heptinstall K, Leuk Res 2007; 31 (Sup 1): 107; deSwart L, BJH 2015; Platzbecker U, Blood 2018; Nov 7;
Bowen D, Mittelman M, ELN-EUMDS Guidelines (2019; on line); deSwart L, Haematologica 2020rHuEPO in MDS: Initial (Mittelman M et al. Blood 1992)
Patient Age / FAB sEPO Hb (g/dL) Hb (g/dL)
Gender mU/mL Week 0 Week 8
1. ZS 82 M RARS 300 8.0 8.2
2. GA 79 M RARS - 7.8 8.0
3. DG 79 F RARS 550 7.9 8.0
4. JL 75 F RARS 480 8.1 7.7
5. BB 74 F RARS 660 8.3 8.0
6. DA 78 F RARS 600 8.1 8.0
7. SB 73 F RA 75 8.0 11.0
8. GK 68 F RARS - 8.2 8.3
9. SY 65 M RARS - 7.8 8.1
10. SM 59 F RA 471 8.9 9.4
11. AF 80 M RA 500 7.3 6.9
12. MBB 68 F CMML 400 8.0 7.8
13. IS 82 F RA 96 7.4 11.9Erythropoietin (ESA) in 2021
First line (w/o RBC Transfusions)
Effective
Hb rise
Fewer RBC transfused
Improved QoL
Safe
Cazzola M, BJH 2003;122:386; Hellstrom E, BJH 1997:99;344;
Gafter-Gvili A, Acta Oncol 2013;52:18; Mittelman M, Acta Haematol 1993;
Mittelman M, Med Clin N Amer 1994;8:993–1009EPO Non-Erythroid (immunologic) Effects
Anti-neoplastic (myeloma)
Mittelman M, PNAS 2001; Mittelman M, EJH 1994;
Mittelman M, Acta Haem 1994
Improved immune (T-Cell) functions
Deshet-Unger N, Leuk Res 2017; Sagiv S, BJH 2006
Decreased glucose level
Dseshet-Unger N 2018;
Oster H Acta Haem 2020
Bone loss serum IL6
Hiram-Bab S, FASEB J 2015 16
serum concentration (pg/ml)
Decreased IL-6
14
12
10
Prutchi Sagiv S, BJH 2006 8
6
4
2
0
healthy MM MM + EpoThalidomide is back
55Lenalidomide Del (5q): MDS-004 RRBC TI 56%; Cyto response 50%; 10mg Poor response in TP53 mutation AE: cytopenia, rash, GI, thrombosis No Leukemic transformation Non-del (5q): MDS-005 239 pts; 27% (vs 3.5%) List AF, NEJM 2005; 2006; Lian XY. Plos One 2016;11:e0165948; Alemeida A, Leuk Lymph 2018; Saft L; Haematologica 2014; 99: 1041; Fenaux P, Blood 2011; 118: 3765; Santini V, J Clin Oncol 2016; 34: 2988
Anemia: When ESA fail
Luspatercept (ACE-536) - approved
Activin analog; Sc / 3wk
40% ORR (MEDALIST trial); COMMANDS ongoing
Platzbecker U, Lancet Oncol. 2017; Fenaux NEJM 2020
Oral Aza: 38% response
Quazar (MDS-003) trial (Phase 3)
Garcia Manero G, JCO 2021
Roxodustat:
Oral HIF inhibitor; 38% response; trial ongoing
Henry DH; ASH 2019; ASH 2020; Paper sub.
Imetelstat: Telomerase inh.; 42% ORR; iMerge ongoing
Steensma D, ASH 2018, Fenaux P, EHA 2019; Platzbecker U; EHA 2020PLT Transfusions Indication – in active bleeding PLT transfusion – per local guidelines Consider “thrombostatics” Tranexamic acid Anti-fibrinolytic: Hexakapron Malouf R Cochrane Database Syst Rev 2018 May 14; Vijenthira 2019 Bowen D, Mittelman M, ELN-EUMDS Guidelines 2019 (on line); Carraway 2020
Romiplostim (weekly injection)
Phase I/II
n=44; Response 46%
Kantarjian H et al. J Clin Oncol 2010;28:437
Phase II:
n=250; Stopped – AML ?
Giagounidis A et al. Cancer 2014;120:1838
Longer FU (5yr) – safe
Similar AML rate
Kantarjian H et al. Lancet Haematol. 2018; 5(3):e117
Commentary:
Long FU but short exposure
Mittelman M, Lancet Haematol. 2018 Mar;5(3):e100Eltrombopag (Tablet)
In LR-MDS:
Effective – 47%
Oliva E, Lancet Haematol 2017
In HR-MDS:
Single agent – ASPIRE Part I: 4/17
Mittelman M et al. Blood 2012;120:abst 3822
ASPIRE II: Fewer events (54% vs 69%)
Mittelman M, Lancet Haematol. 2018 Jan;5(1):e34
Combo: SUPPORT (Elt + Aza)
Early terminated Dickinson M et al. Blood 2016;128 2018
Development stopped !Fewer Clinically Relevant Thrombocytopenic Events in
Eltrombopag Patients
Eltrombopag Placebo Odds ratio
P valuea
(N=98) (N=47) [95% CI]
Mean CRTE (Weeks 5‒12) 54% 69% 0.202
0.0315
[95% CI] [43-64] [57-80] [0.047-0.867]
CRTE Analysis Over Time; Generalized Linear Mixed Model
100
90
78 78
80 74
CRTE, % [95% CI]
67 69 69 69 67 69 68
70 66
60
60
59 59 59 57 59
50 56 54 54 54
53
40 48 48
30
20
Placebo
10
Eltrombopag
0
1 2 3 4 5 6 7 8 9 10 11 12
Weeks
Mittelman M et al, Lancet Haematol 2018 62TPO RA – Still Embargo ? “Negative” trials ROM; SUPPORT “Positive” Others (both agents; LR-MDS) Long-term FU – safe Real-life (GFM/ Elt) – Safe ! Meta-analysis (n=2): No excess mortality ! Conclusion ? Personal: Time to lift the embargo Fenaux 2017; Dodilet 2017; Oliva 2018; Kantarjian 2018; Mittelman 2018; 2019; Meng 2020; Comont 2021; Mittelman BJH 2021
Immunosuppressive Treatment –
Still Alive
A large int cohort, 15 centers,
207 pts
The common: ATG + pred (43%)
ORR 48.8%
11% CR; 30% RBC-TI
Median OS 47.4 m
Longer for pts with TI
TI associated with hypocellular BM (< 20%)
Horse ATG + CSA most effective
Did not predict: Age, HLA-DR 15
Mittelman M Acta Haematol 2015; 134: 135; Stahl M, Blood Adv 2018; 2: 1765RBC Transfusions Result in Iron Overload
RBC 2u/month
24u/yr 100u/4yr
200–250 mg
100 u - 20 g iron !!! iron
Sanz GF et al., Blood 74:395-408, 1989Iron Overload
Organ damage ? Yes
Iron chelation - Effective:
Retrospective (Hoeks M; Haematologica. 2020;105(3):640)
TELESTO (Angelucci E, Ann Intern Med. 2020;172:513)
Prospective; DFX vs Placebo; 221 pts;
36% reduced events (1440d vs 1091d)
No survival advantage
Guidelines:
Use iron chelation, when:
> 25 RBC u; Ferritin>1000
Mittelman M; IMAJ 2008;10: 374Overview of iron chelators
Deferoxamine
Property Deferiprone (DFP) Deferasirox
(DFO)
Usual dose 25–60 mg/kg/day 75 mg/kg/day 20–30 mg/kg/day
Route s.c., i.v. p.o. p.o.
8–12 h, 5 days/week 3 times daily once daily
Half-life 20–30 min 3–4 h 8–16 h
Excretion Urinary, faecal Urinary Faecal
Approved Treatment of chronic Thalassaemia major Treatment of chronic iron
indications iron overload due to overload due to frequent
transfusion-dependent blood transfusions
anaemias
Deferoxamine Prescribing Information.
Deferasirox Summary of Product Characteristics.
Deferiprone Summary of Product Characteristics.Treatment
HR-MDS / AML Treatment: Principles
Strategic decision:
Treat the disease ?
Or supportive treatment ?
If anti-MDS/AML:
Quite aggressive
Chemotherapy
Epigenetic (biologic) treatment
Investigational
Frame:
Protocols
Skilled team
Facilities (intensive care)
70Azacitidine (Vidaza) – 1st line
(Aza 001 Trial): Response 50%; 2yr
100
Azacitidine (n=179)
80 CCR (n=179)
60 24.5 months 18 pts & Int-1
Patients surviving (%)
40 15.0 months
20
p=0.0001
0
0 5 10 15 20 25 30 35 40
Time from randomisation (months)
Fenaux P, et al. Lancet Oncol 2009;10:223–32HR MDS/AML: How can we do better ?
HMA still, but:
Better formulations: oral? Derivative ?
Guadecitabine; Oral Aza
Add-on: HMA (Aza) combinations
Identify responding subgroups
Minimize toxicity: infections; low PLT; supportive
Other known: Lenalidomide
Chemotherapy
Stem cell transplant
Novel agents / strategiesHMA: Identifying Responders –Personalized
Females respond better to DAC
DeZern AE, Leuk & Lymph 2017; 58: 1325
TP53 mutation predicts response to DAC:
Welch JS, NEJM 2016; 375: 2023; Chang CK, BJH 2017; 176: 600
TP53 activator: APR (Sallman D JCO 2021; Cluzeau JCO 2021)
TET2 loss/mutation identified responders
Bejar R, Blood 2014; 124:2705; Santini V, Curr Opin Hem 2015; 22: 155
NPM1 mut + DNMT3A WT: DAC Favorable outcomes
Wu L, Br J Haematol. 2020 Apr 8. doi: 10.1111/bjh.16628Infections on Aza
Israel MDS Working Group:
Retrospective, 184 pts on Aza
16.5% infect, 75% admission; 20% fatal !
Merkel D; Am J Hematol 2013; 88:130
Infections more common
In 7d > 5d cycle; In PLT < 20k
Ofran Y; Clin Lymphoma Myeloma Leuk 2015; March
Fungal infections
Kim GYG; Am J Hematol. 2020 Apr
Prophylaxis ?
GFM: failed ? (Sebert M; MDS 2015)
Ongoing Israel trialSUPPORT (phase 3) – Aim: Minimize Aza Toxicity
Eltrombopag Placebo
(+ Azacitidine) (+ Azacitidine)
Death, n (%) 57 (32%) 51 (29%)
Disease 16% 12%
Sepsis 10% 7%
AML , n (%)
By investigators 27 (15%) 16 (9%)
Central lab 21 (12%) 10 (6%)
The study was early terminated
Dickinson M Blood 2018; 132:2629Aza+ Combination: Vi-Len-01
Azacitidine (Vidaza) & Lenalidomide
Recruited – 27 pts (evaluable – 25)
Overall response rate (ORR): 18/25 (72%)
CR / mCR: 9 pts (36%)
Hematologic improvement (HI): 9 pts
Ery 6; PLT 4; Neut 5
Probable OS 12m
Mittelman M et al; ASH 2013; Ann Hematol. 2016; 95:1811Novel (I): Venetoclax (+HMA): The Winner ?
Anti BCL-2, oral, tolerable
Multicenter, phase 1b:145 pts, unfit AML,
CR/Cri 73%; OS 17.5m
DiNardo CD, Lancet Oncol 2018; 19: 216; Blood 2019; 133: 7
V+HMA: ORR 59%
Ball BJ, Blood Adv. 2020 Jul 14;4(13):2866
RCT Phase 3 (AML): 14.7m (V+Aza) vs 9.6m
DiNardo CD, NEJM 2020 Aug 13;383:617
V+ HMA – standard (?), but low ORR !
Azizi A, Leuk Lymphoma. 2020 Jun 16:1-8 .
VERONA Trial: Phase 3, MDS, RCT, ongoing !AML Treatment: Induction (I)
ELN Guidelines (2010):
Standard Approach (“Young”)
7+3
Cytarabine (Ara-C)
100-200mg/m/d X 7 days
Anthracycline
Daunorubicin
60-90 mg/m/d x 3 days, or
Idarubicin 10-12 mg/m/d x 3 days
Dohner H; Blood 2010AML Treatment: Induction (II)
Additional 3rd drug ? Novel
Chemotherapy:
Etoposide; Cladribine; Clofarabine
Antibodies:
Gemtuzumab-Ozogomycin (Mylotarg, Anti-CD33)
Targeted:
Anti-FLT3: Midostaurin
Anti Bcl2: Venetoclax
Anti IDH1,2AML: Post Remission
Conservative:
Chemotherapy
High-dose Ara-C (Cytarabine)
Other chemo regimens
Stem cell transplant (SCT)
Allo-SCT (or auto)
For high-risk
“Young”
Resistant/ relapse (RR)Other Chemo for HR-MDS/AML
Clofarabine: mostly studied (phase 2)
Horikoshi A Chemotherapy 2013;59:152; Becker PS AJH 2015;90:295;
Sellesag D Haematol 2017;102:e50; Buckley SA BJH 2015;170:349;
Rudrapatna VK Leuk Res 2015;39:835; Roberts DA Leuk Res 2015;39:204;
Jabbour E Cancer 2017; 123: 629
Other: Benda+ Ida; Ida+cytarabine+Mylotarg
Lionberger JM Br J Haematol 2014;166:375; de Witte T Ann Hematol
2015;94:1981
Aza similar to 7+3
Othus M, Leukemia 2018; October 12
CPX-351: Liposomal cyatabine / daunoribicin 5:1
Lancet JE, J Clin Oncol 2018; 36: 26Stem Cell Transplantation Basic idea: Replace the sick marrow Problems: HLA typing – rejection GVHD Conditioning – pancytopenia Veno-occlusive disease of the liver Indications: AL/MDS (high-risk) Allow aggressive chemo - ABMT Source: BM; Peripheral; Cord blood
SCT for HR-MDS/AML The only curable !! Questions: Who? High-risk When? Pre-SCT treatment ? If blasts > 10% HMA or Chemo ? Similar RIC or MAC ? Similar Post SCT maintenance / DLI ? For HR of relapse ELN Recommendations - summary Robin M, Leuk Res 2015; Della Porta MG, Leuk 2017; Nazha A, ASH 2018; Symeonidis A BJH 2015; Sohn SK Crit Rev Oncol Hematol 2015; Konuma T, Hematol Oncol 2018; Potter VT, Biol BMT 2016; Damaj G, JCO 2012; Kroger N, JCO 2017; deWitte T, Blood 2017
Novel (Targeted/ Biologic) Agents
Abs: Mylotarg (A-CD33; Gemtuz-Ozogamicin); Anti-CD123
Targeted molecules:
Midostaurin – anti-FLT3; Venetoclax – anti-bcl2
Rigosertib - RAS/MEK inhibitor
Pevonedistat - NEDD8 activ. enzyme inhib. – “ubiquitin”
Glasdegib - Hedgehog inhibitor; PO
Selinexor (Etanexor): Oral nuclear export protein inh.
APR 246 (Eprenetapopt) – TP53 activator
IDH inhibitors: Enasidenib; Ivosidenib
Immunotherapy
Sabatolimab (MBG 453; Anti TIM-3 Ab)
Future: CAR-T; Others
86MDS/AML Treatment 2021: Summary
LR-MDS
RBC transfusions; ESA
Luspatercept; Investigational
PLT transfusions; Thrombomimetics (?)
HR-MDS / AML
Hypomethylating; (HMA + ?)
Chemotherapy
Stem Cell Transplant
Novel / InvestigationalWhy Clinical Trials ? Novel (inaccessible) treatments Close follow up Free treatment Helps people / science All supervised / controlled
Sec AML & MDS - Summary
Spectrum from pre-MDS through AML
Usually elderly people
Better understanding
Early diagnosis
Not a verdict !
More effective treatments
Future looks better !
89Young / Rich / Healthy
90Thx to Collaborators and… TASMC (Ichilov) – Tel Aviv team Hematology team (I. Avivi) Howard Oster Study coordinators: N. Sagy, N.Goldsmidt Israel MDS Working Group European Leukemia Net (ELN) European MDS group Patients
“The drug has no side effects; However, the price will make you dizzy”
From Tel Aviv
You can also read

















































