SCIENCEDIRECT - KURTZ PSYCHOLOGY
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CBPRA-00814; No of Pages 14: 4C
Available online at www.sciencedirect.com
ScienceDirect
Cognitive and Behavioral Practice xx (2020) xxx-xxx
www.elsevier.com/locate/cabp
1
Contains Video
Expanding Treatment Options for Children With Selective Mutism: Rationale,
Principles, and Procedures for an Intensive Group Behavioral Treatment
Nicole E. Lorenzo, Danielle Cornacchio, Tommy Chou, Florida International University
Steven M.S. Kurtz, Kurtz Psychology Consulting
Jami M. Furr and Jonathan S. Comer, Florida International University
Children with selective mutism (SM) experience significant challenges in a variety of social situations, leading to difficulties with
academics, peers, and family functioning. Despite the extensive evidence base for cognitive-behavioral interventions for youth anxiety,
the literature has seen relatively limited advancement in specialized treatment methods for SM. In addition, geographic disparities in
SM treatment expertise and the roughly 6-month duration of some of the supported SM treatment protocols can further restrict the
accessibility and acceptability of quality SM care. Intensive group behavioral treatment (IGBT) for SM was developed to expand the
portfolio of evidence-based SM treatment options by offering brief, but high-dose, expert SM intervention in a group format for youth ages
3–10 years that can be completed in 1 week. In this article, we outline IGBT for SM program, which has already received initial support
in a waitlist-controlled trial. Our presentation is organized around the five main components of the treatment model: (1) individual
“lead-in” sessions, (2) camp (i.e., all-day group sessions for children held in a simulated classroom setting, with an emphasis on
graduated exposures and structured reinforcement), (3) parent training, (4) school outreach, and (5) booster treatment, as needed. We
conclude with a discussion of clinical considerations and future directions for further IGBT refinement and evaluation.
S ELECTIVE mutism (SM) is a particularly interfering
anxiety disorder characterized by a persistent failure
to produce speech in settings in which verbalization is
most children with SM go undiagnosed until at least age 5
when they begin school (Muris & Ollendick, 2015).
Despite relatively low prevalence rates, SM presents with
expected, despite fluent speech in other settings (American a wide range of complex challenges in early childhood.
Psychiatric Association, 2013). To diagnose SM, a child’s School can be extremely challenging for children with SM,
failure to produce speech must extend beyond the first as they fail to communicate effectively with teachers, staff,
month of school, given that inhibition in new situations can and/or peers, and they commonly fail to demonstrate their
result in initially restricted speech even among nonanxious full intellectual and social competencies. Family and social
youth. Research suggests that SM is a relatively rare anxiety dysfunction are quite common, as well (Bergman et al.,
disorder with a broad constellation of negative effects 2002a, 2002b; Viana et al., 2009). Research demonstrates
(Viana et al., 2009). Prevalence rates have been document- particularly high rates of comorbidity of SM with other
ed between 0.2 and 1.9% (Bergman, Piacentini, & anxiety diagnoses, especially social anxiety disorder and
McCracken, 2002a, 2002b; Elizur & Perednik, 2003; Kopp separation anxiety disorder (Kristensen, 2000)—which in
& Gillberg, 1997; Muris & Ollendick, 2015), with estimates turn are associated with additional difficulties across
seeming to rise in recent years with improved identification, multiple domains—including peer relationships (Cohen
awareness, and assessment methods. Onset typically occurs & Kendall, 2014; Verduin & Kendall, 2008), family
in early childhood, between 2 and 5 years of age functioning (Swan & Kendall, 2016; Thompson-Hollands
(Cunningham et al., 2006; Kristensen, 2000). However, et al., 2014), sleep hygiene (Weiner et al., 2015), academic
performance (Mychailyszyn et al., 2010), and later sub-
stance misuse (Duperrouzel et al., 2018; Wu et al., 2010).
Further, a growing body of evidence identifies a roughly
1
Video patients/clients are portrayed by actors. 20% subset of youth with SM who also exhibit significant
oppositional behaviors (Kristensen, 2001; Steinhausen &
Keywords: selective mutism; intensive group; anxiety; treatment;
feasibility Juzi, 1996).
Although a substantial body of literature now documents
1077-7229/13/© 2020 Association for Behavioral and Cognitive the effectiveness of cognitive-behavioral interventions for
Therapies. Published by Elsevier Ltd. All rights reserved. youth anxiety (Comer et al., 2019; Higa-McMillan et al.,
Please cite this article as: Lorenzo et al., Expanding Treatment Options for Children With Selective Mutism: Rationale, Principles, and
Procedures for an Intensive Group Behav..., Cognitive and Behavioral Practice (2020), https://doi.org/10.1016/j.cbpra.2020.06.0022 Lorenzo et al.
2016; Silverman et al., 2008), scientific advances in the Given (a) geographic disparities in SM expertise, (b)
treatment of SM have been quite limited. Only a very small observed limitations in the quality of broad dissemination
handful of controlled trials have examined SM intervention and implementation of treatments for relatively rare
options, with cognitive-behavioral treatment (CBT) formats conditions and for treatments involving more complex
garnering the most empirical support to date (Catchpole and intensive strategies (Comer & Barlow, 2014), (c)
et al., 2019; Cohan et al., 2006; Kovac & Furr, 2019; Muris & limited dissemination-to-date of the scant literature on
Ollendick, 2015). In the first randomized controlled trial SM treatment, (d) limited prior SM experience that can
(RCT) of CBT for youth SM, Bergman and colleagues be brought to bear in treatment by typical providers, even
(2013) evaluated a 6-month-long, weekly individual treat- if they are working from a supported SM treatment
ment program involving affected children, parents, and protocol, and (e) the heterogeneous nature of SM across
their teachers, relative to a waitlist control condition. Their affected youth (Sharp et al., 2007), many youth with SM
integrated behavior therapy for SM incorporated systematic may particularly benefit from services delivered by
and gradual exposure to speaking situations, combined providers in SM specialty settings characterized by a
with behavioral techniques such as stimulus fading, high volume of SM patients. This is consistent with strong
shaping, systematic desensitization, and contingency man- evidence in medicine that surgical effectiveness is
agement. Bergman and colleagues (2013) found high rates positively associated with surgeon patient volume
of diagnostic remission (67%) and treatment response (Pasquali et al., 2012)—the more patients a provider
(75%), demonstrating the efficacy of the CBT model for sees with a particular condition, the more familiar they
youth with SM. A second RCT (Oerbeck et al., 2014) are with the range of variability associated with such
corroborated the efficacy of the CBT model in their version presentations of that condition, and the more readily
of a 6-month weekly protocol involving children, parents, they are able to navigate positive outcomes among similar
and teachers, with treatment occurring specifically in school new cases. Indeed, malignant tumors are not removed by
and home settings. For the majority of treated youth, positive primary care physicians, they are removed by specialists—
outcomes were maintained a year after treatment ended surgical oncologists who have completed relevant edu-
(Oerbeck et al., 2015). Principles from Parent-Child cation and advanced surgical competency training, and
Interaction Therapy (PCIT) have also been applied success- who see a high volume of patients with cancer (see Comer
fully in treatments for children with SM (Cotter et al., 2018). & Barlow, 2014).
Specifically, weekly individual treatment combining behav- Despite geographic disparities in the availability of
ioral techniques and PCIT principles demonstrated signifi- specialty mental health care, recent advances leveraging
cant gains in children’s speaking behaviors up to a year novel intervention formats have begun to meaningfully
posttreatment (Catchpole et al., 2019). PCIT principles extend the reach of expert providers for a range of
including live parent coaching and child directed interaction conditions (Comer et al., 2014). In particular, “intensive”
(CDI) skills (Eyberg & Funderburk, 2011) are used to create treatment formats—which offer high-dose, condensed
a safe and positive environment, as well as support the modifications of interventions that are typically delivered
introduction of unfamiliar individuals. over longer periods of time—have garnered strong
These initial controlled trials of SM treatment provide empirical support for a range of youth anxiety disorders
critical support for the utility of exposure-based CBT (Angelosante et al., 2009; Davis et al., 2009; Gallo et al.,
methods that draw on stimulus fading, shaping, systematic 2014; Ollendick et al., 2009; Öst & Ollendick, 2017;
desensitization, and contingency management. At the Santucci et al., 2009). Importantly, delivering a high
same time, the acceptability of a 6-month treatment dosage of SM treatment in a relatively brief period of time
course that spans two-thirds of a school year may be can allow some affected youth to participate in services
somewhat limited for many, particularly when most youth with specialty providers with extensive relevant experi-
with SM live in regions where access to CBT-SM expertise ence, even if such providers are not in the family’s
may be limited. Comer and Barlow (2014) have discussed immediate vicinity (Wu et al., 2010). Although it would
the poor accessibility of expertise and specialty care for not be possible for a family to participate in 6 months of
low base rate conditions, such as SM, for the majority of weekly face-to-face treatment with a specialty provider
affected individuals. In light of the relatively low base rate located a significant distance away, abbreviated intensive
of childhood SM, providers with SM clinical experience treatment formats offered in specialty practices open up
and expertise tend to cluster in major metropolitan destination treatment options for some families. More-
regions and academic hubs. Even among children over, even among families dwelling in regions character-
dwelling in regions characterized by SM treatment ized by availability of SM specialty providers, the
expertise, investing the time in weekly treatment for half prolonged 6-month duration associated with most of the
of a year may present significant obstacles, and other key small handful of evaluated SM treatments can conflict
barriers to care may remain. with important competing demands on a family’s time.
Please cite this article as: Lorenzo et al., Expanding Treatment Options for Children With Selective Mutism: Rationale, Principles, and
Procedures for an Intensive Group Behav..., Cognitive and Behavioral Practice (2020), https://doi.org/10.1016/j.cbpra.2020.06.002Intensive Group Behavioral Treatment for Selective Mutism 3
Intensive Group Behavioral Treatment (IGBT): Key experience or postdoctoral students acquiring hours for
Components and Procedures licensure. However, the class supervisor can also be a
Given problems for many in the accessibility and licensed clinical psychological if there is only one
acceptability of evidence-based SM treatment provided by classroom. If more than one classroom, the program is
SM specialists, an intensive treatment option for childhood often overseen by a licensed clinical psychologist (herein
SM referred to as Intensive Group Behavioral Treatment called “IGBT director”).
(IGBT), developed by Kurtz (2016), has grown in popularity Staff are typically recruited through email blasts to
(Petersen, 2018; Saint Louis, 2015) and in research support psychology listservs (e.g., Div. 53, 16, ABCT, SMA, ADAA
(Catchpole et al., 2019; Cornacchio et al., 2019). IGBT-SM is child anxiety), as well as local university psychology,
a blend of PCIT, specifically the CDI phase, and CBT. The counseling, speech and language, and social work
benefit of a group-based intensive for children with SM is departments. During the camp week, staff typically
the opportunity to practice exposures with several other schedule patients for the evening hours. During lead-
children. IGBT typically occurs over the course of 1–2 ins, patients are seen on a priority basis. Additionally,
summer weeks, prior to a child’s transition into a new school some students continue to take summer courses or work
year. IGBT programs for SM are typically geared toward other part-time jobs while also volunteering in the IGBT.
children between the ages of 3 and 10, and include five Staff training is typically conducted over 2–3 days,
main components: (a) individual “lead-in” sessions, (b) reviewing and practicing CDI and VDI skills.
analog classroom (i.e., all-day group sessions for children
held in a camp-like setting), (c) parent training, (d) school ASSESSMENT
outreach, and (e) booster treatment as needed (Kovac &
Prior to beginning the camp, children are assessed to
Furr, 2019). Although a recent RCT evaluated the efficacy
determine the fit of the camp. Assessments are often
of IGBT for youth SM and showed very positive support
conducted over the phone (specifically for out-of-town
(Cornacchio et al., 2019), little has been written in the
families). A diagnostic clinical interview (typically the
literature about the principles and procedures that make
ADIS) must be conducted to determine if the child meets
up IGBT for youth SM. To facilitate improved dissemina-
criteria for SM. Families are excluded from participating if
tion of clinical methods for implementing IGBT for youth
the assessment determines that (a) the child has a more
SM, the present paper provides a clinical overview of the
impairing diagnosis than the SM, or (b) if the child is
structure and considerations for the IGBT evaluated in
nonverbal with all caregivers.
Cornacchio et al. (2019). We organize our discussion
around Individual “lead-in” Sessions, Camp (i.e., all-day
group sessions for children held in a simulated classroom LEAD-IN SESSIONS
setting), Parent Training, School Outreach, and Booster
Treatment as Needed. Structure
To facilitate stimulus fading, individualization, child
preparedness for the group component, parental support
IGBT STAFF
of skills to be learned, and overall program effectiveness,
The IGBT-SM program requires a 1:1 child-to-staff prior to participation in camp, families complete “lead-in”
ratio, an “IGBT lead teacher,” and at least one class sessions. These sessions are held at the clinic and entail a
supervisor. If there are multiple classes, an additional parent focused Teach session (described below) followed
supervisor to oversee the various classes is recommended. by “fade-in” sessions. These sessions are typically held
The children are always paired with a staff member during the week immediately prior to camp, and the goal
(herein called “primary counselor”). In many IGBTs, of these sessions is for the child to speak to at least two
these primary counselors are trained undergraduate program staff consistently without their caregiver present,
students or graduate students looking to gain clinical prior to starting the group component of camp. Failure to
experience working with anxious youth. In addition to meet this criterion may indicate that the child may not be
primary counselors matched with each child, a more ready for a group intensive format and may benefit first
specialized “IGBT lead teacher” directs the overall from other treatment options (e.g., medication, individ-
classroom and maintains the class schedule. Typically, ual intensive behavioral treatment). For children who do
the IGBT lead teacher is an undergraduate or graduate not meet the requirement of speaking to two program
student with prior experience working with children with staff, a modified 1:1 intensive is typically offered to
SM. Additionally, at least one “class supervisor” is assigned families. Families vary in the amount of Teach sessions
per classroom to assist with challenging situations or times and “fade-in” sessions needed, with most families requir-
in which multiple staff are needed. These class supervisors ing one 45-minute Teach session and, on average, 4 hours
are typically advanced graduate students with prior SM of fade-in sessions (typically scheduled in 2-hour blocks
Please cite this article as: Lorenzo et al., Expanding Treatment Options for Children With Selective Mutism: Rationale, Principles, and
Procedures for an Intensive Group Behav..., Cognitive and Behavioral Practice (2020), https://doi.org/10.1016/j.cbpra.2020.06.0024 Lorenzo et al.
either on the same day or different days). We describe the blocks?”). Open-ended questions (e.g., “What do you
each of these two types of lead-in sessions, in turn, below. want to play with next?”) are also encouraged but may be
slightly more challenging for children with SM than
Teach Session forced-choice questions. Yes/no questions (e.g., “Do you
The Teach session is typically a 45-minute session that want to play with the trains?”) are strongly discouraged, as
orients parents to the skills and structure of the fade-in children are significantly more likely to answer such
sessions. It can be held in office, or for out of town families questions with a nonverbal response (e.g., head nod,
traveling for IGBT it can be held via videoconferencing. pointing, gesturing) rather than a verbal response.
Specifically, parents are provided with psychoeducation Parents are taught to give their child an ample opportu-
about the nature of SM, as well as brief overviews of Child nity to respond (at least 5 seconds) to any given question.
Directed Interaction (CDI) skills, Verbal Directed Inter- Questions can be repeated up to three times (with at least
action (VDI) skills, and how to use a contingent rewards to 5 seconds of response opportunity in between) until the
reinforce successive approximations toward increased child responds. If the child fails to respond after the third
verbalizations (i.e., “brave talking”). These skills are then prompt then parents are taught to modify the prompt to
role-played to assist parents in learning how to use the make it less challenging for the child (e.g., convert an
skills with their child. open-ended question to a forced-choice question, or vice
CDI skills are adapted directly from PCIT (Eyberg & versa). If the child still does not provide a verbal response,
Funderburk, 2011) and are used to reinforce children for the child is taken to a separate space to practice. If the
verbal behavior with positive attention as well as to child still struggles to respond, then the child is returned
increase child comfort with new individuals. Whereas to the last situation in which he or she was successful in
the CDI skills were originally developed to reinforce answering a question. If necessary, the question can be
appropriate and compliant behavior in children showing revisited at a later time point, but ultimately the question
serious conduct problems (see Elkins, Mian, Comer, & should never be left unanswered. Parents also learn to use
Pincus, 2016), in IGBT parents are taught to focus social additional prompting, as necessary, to ensure verbal
reinforcement strategies toward child vocalizations, verbal responses. For example, if the child provides a nonverbal
responsiveness, and prosocial behavior. CDI skills are to response to a question (e.g., head nod), the parent learns
be employed during interactions in which the parent is to to how to prompt for a verbal response (e.g., “I see you
follow the child’s lead. Video 1 provides an example of nodding your head. Please use your words to answer” or
effective CDI skills. “I see you nodding your head, but I don’t know what
Specifically, during such child-led interactions, parents you’re trying to tell me”). Video 2 provides an example of
learn to use Praise, Reflection, Imitation, Description, and effective VDI skills.
Enthusiasm (i.e., PRIDE skills) to reinforce positive, brave, In the Teach session, parents are also introduced to a
and verbal behavior. For example, parents are encour- customized reinforcement system to be used in the fade-
aged to praise their child for wanted behavior (e.g., “great in sessions (described below), as well as throughout the
job playing with me,” “thanks for using your words”), camp and beyond. This reinforcement system entails a
describe their child’s behavior that they want to see more reward chart presented on a portable dry erase board that
of (e.g., “you’re playing with the Legos now,” “you’re using incorporates the child’s interests (e.g., Paw Patrol, My
your words), and reflect any instances of child speech Little Pony) in the background. For every verbalization
(e.g., child says, “I like blue,” then the adult says, “you said and/or positive social interaction the child earns a check.
you like the color blue”). Additionally, as in traditional The child can earn up to 12 checks on their reward chart.
PCIT for conduct problems (Eyberg & Funderburk, Once they complete the reward chart they earn a gold
2011), parents also learn to ignore minor misbehavior coin that can be used to redeem prizes; stickers or other
and to avoid commands, critical statements, and questions small reinforcers (e.g., jellybeans) may be given instead of
during CDI. checks if the child is unmotivated by the check system.
In the Teach session, parents also learn VDI skills to Parents are taught that the reinforcers will be given less
directly prompt and reinforce child speech in ways that frequently over time for increasingly challenging verbal
optimize the likelihood of eliciting verbal responses. tasks/situations.
Parents learn to apply these VDI skills in situations in
which their child is hesitant to respond (e.g., when a Fade-in Procedures
stranger or adult confederate is in the room). Specifically, The second component of IGBT lead-in sessions
after using CDI skills to help ease the child into the promotes child verbalization with the camp staff via
situation, parents are encouraged to ask forced-choice stimulus fading. This procedure begins with the child
questions, in which the answer is given as a choice within interacting solely with an individual with whom they are
the question (e.g., “Do you want to play with the trains or comfortable speaking (typically the parent) in a room by
Please cite this article as: Lorenzo et al., Expanding Treatment Options for Children With Selective Mutism: Rationale, Principles, and
Procedures for an Intensive Group Behav..., Cognitive and Behavioral Practice (2020), https://doi.org/10.1016/j.cbpra.2020.06.002Intensive Group Behavioral Treatment for Selective Mutism 5
themselves. The set-up works best when the parent-child using the fading process (Cornacchio et al., 2019). Other
dyad is situated in a room with a one-way mirror, behind methods, including gradual shaping of sounds to speech,
which the IGBT staff can monitor the interactions. For iPad games eliciting speech, videos and self-modeling, can
settings in which an observation room with a one-way be used to prepare the child to meet the criteria to enter
mirror is not available, a live observation system can be set camp.
up by placing a computer or tablet with a webcam in the
room with the parent-child dyad and using videoconfer- CAMP
encing to allow the IGBT staff to monitor from a separate
Overview
room. During these interactions similar to standard PCIT,
The core of IGBT is a multi-day course of all-day group
the parent receives real-time guidance and prompting
sessions for children held in a simulated classroom
from the IGBT staff through a bug-in-the-ear device that
setting, referred to as “camp.” In the IGBT model tested
allows the IGBT staff to speak to the parent without the
by Cornacchio and colleagues (2019), the camp consisted
child hearing. There is a range of technological options
of a 5-day Monday through Friday program held from
that can afford bug-in-the-ear parent guidance, including
9:00 A.M. to 5:00 P.M. during a summer week. Typically,
a walkie-talkie system with an earpiece, a phone with an
there are between 6 and 12 children in an IGBT
ear bud, or a Bluetooth earpiece system.
classroom, grouped by age (e.g., children aged 3–5,
While the parent is alone in the room with the child,
children aged 5–7, children aged 8–10). With sufficient
the IGBT staff coaches the primary caretaker via the bug-
staffing and patient volume, IGBT programs can simulta-
in-the-ear through the skills (i.e., CDI, VDI, reinforce-
neously run multiple classrooms at the same time. Given
ment chart) until the child is relatively comfortable and
that programs are often run in the summer, many IGBT
speaking consistently to the caretaker (i.e., completes at
programs have been run out of schools where classrooms
least one reward chart). A new individual (e.g., child’s
can be rented. Alternatively, conference room space can
primary counselor during fade-in sessions) gradually
be used as a modified classroom.
moves closer and closer to the child, while the child
Each child is paired daily with a “primary counselor”
continues to interact with their parent. The new
(i.e., 1:1 staffing model) who is responsible for assisting
individual (e.g., child’s primary counselor during fade-in
the child throughout each task and scheduled activity
sessions) is typically a M.S.- or Ph.D.-level practicum
while using CDI and VDI skills, and the child’s reward
student, extern, or undergraduate research assistant who
chart, to reinforce adaptive and speech behaviors. To
has been trained on fading procedures and CDI and VDI
promote speech generalization, the child’s primary
skills. Using fading procedures (Furr et al., 2019), the new
counselor rotates throughout the week as the child is
individual only moves closer to the child when the child is
deemed ready for this transition. The camp is structured
consistently verbalizing to their parent. The new individ-
much like a school or camp week. In general, the
ual might start by opening the door slightly and sitting in
schedule and domains targeted are similar each day,
the hallway looking the other way while the parent uses
though the specific activities and level of difficulty of
the CDI and VDI skills and uses the reinforcement chart.
activities changes. The difficulty of daily activities is
After the child eventually resumes consistent speech with
titrated upward throughout the week in order to promote
the parent, the new individual might open the door
gradual and systematic exposure to increasingly challeng-
further, but still not be directing their gaze at the child.
ing and more generalizable situations. For example,
This process continues as the new individual gradually
although a period of time devoted to “warm-up” is
enters the room, and moves slightly closer to the parent-
allotted each day, the amount of time is reduced (i.e.,
child dyad.
30 minutes on days 1 and 2; 15 minutes on days 3–5).
Eventually, the new individual would move close
Therefore, many activities overlap in content or context,
enough that they can hear and interact with the child.
but as the week progresses, counselors challenge children
When the child is consistently verbalizing in front of the
to demonstrate increasing steps toward independence
new individual, the new individual may begin to use CDI
and spontaneity in their verbal and/or social behaviors.
skills (e.g., praise for speaking) and then VDI skills (e.g.,
ask the child a forced-choice question), while utilizing Scheduled Activities
shaping (Furr et al., 2019) and positive reinforcement While the schedule for each day is unique, each activity
strategies to encourage the child to speak directly to him is designed to target and/or simulate an array of
or her (see Video 3 for an example of a fade-in). Once the experiences that children typically encounter in their
child is consistently verbalizing to the new individual, the daily lives. For example, throughout the day there are a
parent gradually exits the situation at a roughly similar number of tasks that target ordering (e.g., selecting
pace (i.e., fade-out). The majority of children meet the snacks, ordering lunch, treasure chest), speaking with
criteria of speaking to two camp staff after fade-in sessions adult figures (e.g., asking for help from camp counselors,
Please cite this article as: Lorenzo et al., Expanding Treatment Options for Children With Selective Mutism: Rationale, Principles, and
Procedures for an Intensive Group Behav..., Cognitive and Behavioral Practice (2020), https://doi.org/10.1016/j.cbpra.2020.06.0026 Lorenzo et al.
asking for clues for a scavenger hunt), interacting with verbally, as well as carrying out the responsibilities
peers (e.g., games, sports, lunch), and group participation associated with his or her job, as needed. For some
(e.g., “show and tell,” morning meeting, classroom children, making decisions is a particular challenge (and
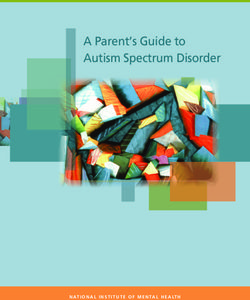
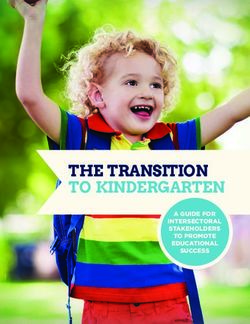
introductions). Figure 1 displays a sample schedule of therefore, an appropriate intervention target). For these
an IGBT camp. children, counselors may initially facilitate job selection by
Each day begins with a warm-up period (i.e., Centers), offering fewer options or assisting in selection. However,
during which children are engaged in free play. During the goal of this activity is ultimately for children to make
this time the child interacts with their primary counselor decisions on their own.
and the counselor focuses on using CDI skills and slowly Below is an example of a counselor assisting a child
introduces VDI skills. The goal of this time is to support with participating in job selection in which the child
children in becoming comfortable and feeling successful successfully responds to the IGBT lead teacher:
in the classroom environment without an expectation of
speech. The amount of time dedicated toward warm up IGBT LEAD TEACHER: It is time to pick jobs for today. Raise
decreases throughout the week. During activities through- your hand to tell me what job you want to do today.
out the rest of the day, counselors engage in CDI and VDI COUNSELOR [to their assigned child in the group]: We
skills, as well as implement the reward chart, scaffolding need to pick a job for today. You can pick to be a snack helper,
the level of difficulty based on the child’s speech progress line leader, or lunch helper. Which job do you want to pick today?
and difficulty of the situation. CHILD: Snack helper.
Each day, the first structured activity is the morning COUNSELOR: Great! You get a check for answering that
meeting. A different counselor leads the morning question. Raise your hand to tell Ms. Jami (IGBT LEAD
meeting each day to provide children with novel social TEACHER) that you want to be snack helper and you will get
interaction opportunities. Throughout the morning two more checks.
meeting, all the children are prompted to answer IGBT LEAD TEACHER [to child with hand raised]: I see
questions, share information, and participate in activities you raising your hand. What job do you want to pick today?
in front of the group, much like what most morning CHILD: Snack helper.
meetings entail in early child classroom settings. Morning IGBT LEAD TEACHER: Great job telling me you want to be
meeting typically begins with an introductory prompt for snack helper! Here’s a coin for answering in front of the group.
children to participate nonverbally, quickly followed by a COUNSELOR [to child]: Great job being brave saying you
prompt to share information verbally with the group (e.g., want to be snack helper. You get two checks.
name, game/activity played that morning, number of
coins earned so far). Each counselor works with his or her If the child fails to respond in the group, the role of the
assigned camper for the day to identify appropriate goals counselor is to scaffold the question to assist the child in
for participation. For example, one child may immedi- successfully using speech to respond to the prompt. Below
ately raise his or her hand and volunteer an answer to the is an example of a counselor assisting a child with
IGBT lead teacher in an audible voice without support participating in job selection in which the child has
from his or her counselor, whereas another child may difficulty responding to the IGBT lead teacher:
only whisper a response to his or her counselor at the back
of the room. The morning meeting also includes a review IGBT LEAD TEACHER: It is time to pick jobs for today. Raise
of the daily calendar (e.g., date, weather) and schedule. your hand to tell me what job you want to do today.
During this portion of the morning meeting, children are COUNSELOR [to child amongst the group]: We need to
prompted to answer questions, as well as volunteer to pick a job for today. You can pick to be a snack helper, line
come up to the front of the group to fill in the appropriate leader, or lunch helper. Which job do you want to pick today?
information on various boards. Therefore, this activity CHILD: Snack helper.
facilitates both speaking and nonverbal participation in a COUNSELOR: Great! You get a check for answering that
group setting. question. Raise your hand to tell Ms. Jami (IGBT LEAD
Each day, children either select or are assigned jobs. TEACHER) that you want to be snack helper and you will get
These jobs also mimic the roles children typically receive two more checks.
in classroom settings, such as “line leader” or “snack IGBT LEAD TEACHER [to child with hand raised]: I see
helper.” Throughout the day, counselors prompt children you raising your hand. What job do you want to pick today?
to remind them of their jobs. For example, at snack time, [IGBT lead teacher waits 5-10 seconds for a response and
the IGBT lead teacher may call out, “Who wants to be child does not respond. IGBT lead teacher asks the
snack helper today?” and wait for a child to raise his or her child’s counselor for the child’s job selection. With that
hand. The primary counselor paired with that child response the IGBT lead teacher reframes the question to
supports the child in volunteering this information a forced choice question.]
Please cite this article as: Lorenzo et al., Expanding Treatment Options for Children With Selective Mutism: Rationale, Principles, and
Procedures for an Intensive Group Behav..., Cognitive and Behavioral Practice (2020), https://doi.org/10.1016/j.cbpra.2020.06.002Intensive Group Behavioral Treatment for Selective Mutism 7
Figure 1. Sample IGBT Camp Schedule
Please cite this article as: Lorenzo et al., Expanding Treatment Options for Children With Selective Mutism: Rationale, Principles, and
Procedures for an Intensive Group Behav..., Cognitive and Behavioral Practice (2020), https://doi.org/10.1016/j.cbpra.2020.06.0028 Lorenzo et al.
IGBT LEAD TEACHER [to child]: Do you want to be snack them to engage in verbalizing. If after this type of
helper or line leader? scaffolding the child still fails to respond, the counselor
CHILD: Snack helper. can choose to continue to scaffold by removing the child
IGBT LEAD TEACHER: Great job telling me you want to be and practicing further away from the group, or outside
snack helper! Here’s a coin for answering in front of the group. the room. Additionally, the counselor can engage in a
COUNSELOR [to child]: Great job being brave saying you different form of scaffolding by changing their own
want to be snack helper, you get two more checks. position using shaping strategies. For example, the
counselor can have the child stay in the circle and the
If the child still failed to respond to the question with a counselor can move towards the center (towards the
forced choice question, then the counselor would IGBT lead teacher) until the counselor is next to the
continue to scaffold the process to help make it easier IGBT lead teacher, while continuing to answer the
for the child to verbally respond to the question in the question. Once the counselor is right next to the IGBT
group. Below is the continuation of the sample script if lead teacher, the IGBT lead teacher can ask the question.
the child would not have responded to the forced choice Below is a sample script of such an interaction, after the
question: child failed to respond to the IGBT lead teacher and the
child had already practiced with the counselor:
IGBT LEAD TEACHER [to child]: Do you want to be snack
helper or line leader? [IGBT lead teacher waits 5 seconds for a [Child is positioned along the circle, counselor is directly
response and child does not respond. IGBT lead teacher in front of the child in the middle of the circle at close
asks the same question again to give the child a second distance.]
opportunity to answer. If child still fails to respond, the COUNSELOR: I have an idea! When you can tell Ms. Jami
IGBT lead teacher asks the child’s counselor to practice (IGBT lead teacher) you will get one coin! Let’s practice what
with the child until they are ready to respond. In this you told me before. Do you want to be snack helper or line leader?
situation the counselor would practice and repeat the CHILD: Snack helper.
question with the child until they felt comfortable to COUNSELOR: Snack helper. Great job telling me! One check.
answer to the IGBT lead teacher. The goal is to keep the [Counselor moves slightly further away from the child,
child in the same room to practice, but there is flexibility toward the center of the circle and the IGBT lead
to take the child to a separate place in- or outside of the teacher.]
room to practice.] COUNSELOR: Do you want to be snack helper or line leader?
COUNSELOR: I know that was a little hard. Let’s practice what CHILD: Snack helper.
you told me before. Do you want to be snack helper or line leader? COUNSELOR: Snack helper. Great job telling me! One check.
CHILD: Snack helper. [Counselor moves slightly further away from the child,
COUNSELOR: Snack helper. Great job telling me! You get one toward the center of the circle and the IGBT lead
check on your chart. Do you want to practice one more time or are teacher. This process repeats until the counselor is
you ready to tell Ms. Jami (IGBT lead teacher)? directly next to the IGBT lead teacher.]
CHILD: Practice. COUNSELOR [directly next to IGBT lead teacher]: Do
COUNSELOR: Practice. Thanks for telling me. You get one you want to be snack helper or line leader?
check. Do you want to be snack helper or line leader? CHILD: Snack helper.
CHILD: Snack helper. COUNSELOR: Snack helper. Great job telling me! One check.
COUNSELOR: Snack helper. I love how you said that nice and Now tell Ms. Jami (IGBT lead teacher).
loud. Raise your hand to tell Ms. Jami you want to be snack helper. IGBT LEAD TEACHER: Do you want to be snack helper or
IGBT LEAD TEACHER [to child with hand raised]: I see line leader?
you raising your hand. Do you want to be snack helper or line CHILD: Snack helper.
leader? IGBT LEAD TEACHER: Snack helper! Thanks so much for
CHILD: Snack helper. telling me! Now I know you want to be snack helper! You get two
IGBT LEAD TEACHER: Snack helper. Great job telling me you coins for being so brave!
want to be snack helper! Here’s two coins for answering in front of COUNSELOR: Great job telling Ms. Jami (IGBT lead
the group. teacher) that you wanted to be snack helper! Here is your coin.
COUNSELOR [to child]: Great job being brave saying you Lunch and recess are times for children to continue
want to be snack helper, you get three checks. practicing their brave talking and social skills, while also
receiving a break from structured exposures. During this
For some children, especially on the first day of camp, time, rather than having each child paired with his or her
the group setting is often the most difficult situation for counselor, a less dense ratio of approximately one
Please cite this article as: Lorenzo et al., Expanding Treatment Options for Children With Selective Mutism: Rationale, Principles, and
Procedures for an Intensive Group Behav..., Cognitive and Behavioral Practice (2020), https://doi.org/10.1016/j.cbpra.2020.06.002Intensive Group Behavioral Treatment for Selective Mutism 9
counselor per four children is utilized. IGBT lead when they are ready. If they fail to complete the task
teachers and the child’s counselors decide if any of the without assistance from their counselor, then the coun-
children may benefit from continued one-on-one time selor can assist with similar scaffolding procedures
with their primary counselor. This allows counselors to previously described. However, the goal is for the child
continue to facilitate peer interactions, while also to successfully verbally respond with progressively less
removing some of the intensity and pressure for children assistance from their counselor throughout the week.
to speak consistently. Additionally, while children are Once children receive their prize (Monday through
invited to participate in occasionally structured activities Thursday) they are transitioned in to “childcare” from
during recess (e.g., freeze tag), counselors are also 3:00 P.M. to 5:00 P.M., while parents participate in parent
encouraged to give children agency in choosing how training. During childcare, children are allowed free time
they would like to spend their time. Typically, this to play with any games or engage in any activities they
incorporates clinical judgment and balance between choose. All childcare counselors are trained in CDI skills,
placing demands on a child to participate in a group and many of them are the same staff members who served
activity and allowing a child to isolate themselves. Ideally, as counselors earlier in the day. During childcare,
during this time, all children are within close proximity to counselors use only CDI skills and do not prompt children
one another, but specific demands related to participa- to engage or speak, in order to allow children time to
tion, socialization, and verbalization are reduced. relax after a long day. Typically, children engage with one
In addition to a primary focus in IGBT on behavioral another during childcare and have opportunities for
reinforcement strategies, IGBT also integrates emotion further brave talking practice.
recognition skills, cognitive restructuring, and coping
strategies into the treatment program. These strategies
PARENT TRAINING
are incorporated in the form of structured group Bravery
Lessons held near the end of each day. The content of the In addition to participating in an initial individual Teach
Bravery Lesson varies each day (including review of session at the outset of IGBT and live coaching during lead-
previously covered topics throughout the week), but ins, parents participate throughout IGBT camp in daily
typically incorporates activities that teach relaxation group parent-training sessions, Monday through Thursday
strategies, coping thoughts, mindfulness exercises, iden- from 3:00 P.M. to 5:00 P.M. (during childcare). During this
tifying and sharing feelings, as well as problem-solving time, a lead clinician (usually the IGBT director or a class
anxiety provoking situations (e.g., asking to go to the supervisor) reinforces the skills that have been introduced
bathroom at school, approaching or responding to in treatment and teaches strategies for implementing them
unfamiliar peers). The Bravery Lessons are tailored to through didactics and role-plays. During these daily group
classrooms (broken up by age and developmental levels), parent-training sessions, parents are more thoroughly
such that the content and activities are similar across introduced to CDI and VDI skills, and are provided a
classrooms but are adapted so that they are age and more in-depth psychoeducation on fear, anxiety, and the
developmentally appropriate. A Brave Muscles activity is cycle of reinforcement. Parents are also taught strategies for
also included daily to reinforce the skills by helping avoiding “contamination” that can interfere with child
children identify how they were “brave” to help them progress in new settings. In the context of SM, contamination
recognize their growth and their successes. refers to a negative reinforcement process in which
Throughout each day of IGBT camp, children earn repeated exposure in a given setting to acceptance and/
coins for their brave behavior by completing their reward or accommodation of nonverbal responses (e.g., teachers
chart. At the end of each day, children count the coins accepting nonverbal responses from a child, or a child
they have earned with the assistance of their counselor, being allowed to whisper responses to one special friend in
and cash them in for a prize from the treasure chest (or a classroom who speaks aloud for him or her) ingrains a
prize store). All prizes in the prize store are valued the child’s lack of speech in that setting. When a given new
same. During this activity, children are given the setting gets “contaminated,” it becomes increasingly
opportunity to independently approach and select the challenging for the child to provide verbal responses in
prize they have earned for the day, without support from that specific setting, relative to an “uncontaminated”
their counselors. They are asked by the counselor at the setting. Further, parents are provided with tips and
prize store to name the prize they have selected and share resources for communicating their child’s difficulties and
verbally how many coins they earned throughout the day. treatment strategies to their child’s school and teachers.
The counselor leading the activity scaffolds the question Each day during the latter hour of parent training, parents
type (i.e., open-ended to forced-choice) as necessary. If are coached by a clinician (usually a class supervisor or
the child is unable to respond, they go with their IGBT lead teacher) as they practice the skills they are
counselor to practice and return to collect their prize learning and lead their child through exposures (e.g.,
Please cite this article as: Lorenzo et al., Expanding Treatment Options for Children With Selective Mutism: Rationale, Principles, and
Procedures for an Intensive Group Behav..., Cognitive and Behavioral Practice (2020), https://doi.org/10.1016/j.cbpra.2020.06.00210 Lorenzo et al.
ordering a snack from a snack shop, asking a peer a SNACK CLERK: What kind of chips?
question in a group, asking for help at the school office). [Child does not respond. Parent practices similar
Children are pulled temporarily from childcare to sequence and child still does not respond. The clinician
participate in these exposures while their parents are live then jumps in to coach the parent on scaffolding the
coached. Parents rotate throughout the week so that each skills.]
parent has the opportunity to practice at least once with CLINICIAN (to parent): It looks like that one might be a little
their child. The IGBT lead teachers arrange for small more difficult. Go ahead and practice where she answered
groups of 2–3 children with their parents to practice the originally. Then practice in front of the snack clerk and then
exposures. Given the size of the groups, the rest of the have the snack clerk ask the question again.
parents are offered an opportunity to have questions
answered by the lead clinician about SM, and also offers Once the child and family complete the sequence, the
the group time to share their experiences and/or offer clinician then coaches the other parents in the group.
support to other families. The parents are coached on Typically, the parents are coached through 3–4 scenarios
how to practice the tasks prior to attempting them. Based that include situations with adults, peers, and groups.
on the child’s progress throughout the day, and/or their Parents of other children in the IGBT who are not being
ability to practice with the parents, the clinician will select coached often rotate through being the snack clerk to
a child to attempt the exposure while the other 1–2 give them the opportunity to observe other parent-child
children practice. This allows for the clinician to dyads and live coaching from the clinician.
individually coach the parent if their child has difficulty
with the exposure. Below is a sample script of a clinician SCHOOL OUTREACH
coaching a parent through ordering a snack with their Upon completion of the program, families receive a
child: report documenting their child’s initial diagnoses, infor-
mation about the behavioral conceptualization of SM and
about IGBT, and specific recommendations about how to
CLINICIAN: Parents, we are going to practice ordering a snack
manage the child’s anxiety and promote child verbaliza-
with your kids. They have already practiced with their counselors
tion in the school setting. Furthermore, two 2-hour
during the day. The options for snacks are chips, fruit, or cookies.
teacher trainings are offered by a lead clinician prior to
The chip options are Doritos, Cheetos, and Lays. The fruit is an
the beginning of the upcoming school year. Any teachers
apple or banana. The cookies are chocolate chip or peanut butter.
or other school staff members involved in the child’s care
Practice with your child by asking them what kind of snack they
are invited to attend one of the two offered training times.
want. Once they select the type of snack, ask them which option
They may attend in-person at the clinic or via live webcast
specifically. I will be here to assist you before we go ahead and
or videoconferencing session. Additionally, the trainings
order the snack.
are recorded for teachers unable to attend. Similar to the
[The clinician should be able to listen in on all the
IGBT parent-training sessions, the IGBT teacher trainings
practice and assist if any of them need help. Once the
introduce the CDI and VDI skills and reinforcement
group is ready or the clinician knows one child is ready,
system, such as a daily report card or behavioral chart as
they can head to the order counter.]
mentioned above, that can help promote child speech
CLINICIAN (to family they believe is ready): Looks like
and participation. These trainings include didactics and
your child is ready. Go ahead and help them order. (To other
psychoeducation as well as role plays with the other
families): Keep practicing and I will let you know when it is
teachers and clinicians. School-home communication is
your child’s turn.
pertinent in order to implement a reinforcement system
SNACK CLERK (to child): What would you like to get?
similar to the camp reward chart. Teachers are also given
[Child does not respond.]
handouts and recommended readings that review the
CLINICIAN (to parent): Let the snack clerk know to give you
skills covered throughout the trainings. Handouts include
a minute. Then practice the question again in front of the snack
a brief overview of SM, treatment guidelines, CDI rules,
clerk. If they can answer, then have the snack clerk ask again.
how to ask questions, and sample CDI and VDI sequences
PARENT: Remember what we practiced. What snack would you
(treatment guidelines, how to ask questions, and VDI
like?
sequences sample included in Supplemental Material).
CHILD: Chips.
PARENT: Chips. Great! One check. Now tell her for two checks.
PARENT (to snack clerk): Could we ask again please? BOOSTER SESSIONS, AS NEEDED
SNACK CLERK: (nods yes). What would you like to get? Given that families that participate in IGBT often do
CHILD: Chips. not live locally and that some children and families still
PARENT: Great job answering! Two checks. need additional support, we provide the opportunity for
Please cite this article as: Lorenzo et al., Expanding Treatment Options for Children With Selective Mutism: Rationale, Principles, and
Procedures for an Intensive Group Behav..., Cognitive and Behavioral Practice (2020), https://doi.org/10.1016/j.cbpra.2020.06.002Intensive Group Behavioral Treatment for Selective Mutism 11
booster sessions as needed. Depending on a family’s need, between post and follow-up, where about 35% of families
there are three different types of boosters offered: group reported receiving some type of mental health service
booster days, videoconferencing sessions, and in-person following the IGBT (Cornacchio et al., 2019). Further, the
individual sessions. Most children have made substantial teachers of IGBT-treated children in the following school
gains by the end of the camp and benefit most from group year reported significantly improved verbal behavior in
booster sessions every few months. The group booster day the classroom as well as significantly decreased academic
is run similar to a camp day, often offered on a weekend and social impairment in school, relative to teachers of
or school break. Videoconferencing sessions (see Doss et IGBT-treated children in the year prior to treatment.
al., 2017) are typically offered for out-of-town families Moreover, families reported high satisfaction with the
needing additional support. These sessions can vary IGBT program and low perceived barriers to treatment
depending on the child’s specific needs and can include participation; daily attendance was 100% with only two
practice for a particular situation with which the child is families (out of 29 total families) choosing not to
still struggling. For example, a 1-hour videoconferencing participate in treatment (both families were waitlisted
session can include practicing a presentation like “show families choosing not to participate in treatment following
and tell.” Additionally, school consultations with teachers the waitlist period). Taken together, these results provide
or staff, or attending IEP or 504 plan meetings can also be promising initial empirical support for the efficacy of
included as a booster session if needed. Lastly, for IGBT for SM.
children who are still experiencing significant difficulties,
we offer in-person individual sessions, again focusing on Discussion
practicing the skills and exposures specific to the child’s IGBT for SM was developed to expand the portfolio of
needs. treatment options for youth with SM by offering brief, but
high-dose, expert intervention in a group intensive format.
IGBT works directly with affected children in classroom-
EMERGING EMPIRICAL SUPPORT FOR IGBT
based settings, with parent- and teacher-focused components
Recent efforts have begun to establish the empirical working to increase speech in new environments and with
support for IGBT for SM. Several presentations at new individuals. IGBT for SM builds on established cognitive-
professional conferences (e.g., ABCT, SRCD, SMA) have behavioral treatments for youth anxiety (Kendall & Hedtke,
shown pilot trials that have demonstrated the clinical 2006; Suveg et al., 2006), parent training programs for early
significance of the IGBT-SM model, highlighting the child problems (Elkins et al., 2016; Eyberg & Funderburk,
effectiveness of the intervention from the open clinical 2011), and SM-specific weekly outpatient treatment pro-
trials (Barroso et al., 2017; Cornacchio, Furr, et al., 2017). grams (Bergman et al., 2013; Oerbeck et al., 2014). As in
However, to date only one study has examined the efficacy other anxiety-based PCIT adaptations (Comer et al., 2012),
of the IGBT-SM using an RCT. A recently completed IGBT for SM emphasizes the use of positive attending
randomized controlled trial evaluated the feasibility and behaviors, active ignoring, and modeling to reinforce
preliminary efficacy of the IGBT for SM in a sample of preferred child behavior (i.e., verbal social behavior) and
children diagnosed with SM between 5 and 9 years old extinguish patterns of avoidance in anxiety-provoking
(Cornacchio et al., 2019). This study employed a situations. This intensive treatment also draws heavily on
randomized waitlist-controlled design (N = 29), compar- exposure-based strategies to increase child experience with
ing children receiving IGBT immediately to children on a and mastery of verbal behavior in classroom and other
4-week waitlist (waitlisted children participated in subse- social settings, incorporating traditional CBT components
quent IGBT immediately following the 4-week waitlist such as reinforcement systems, prompting, shaping, system-
period). Results demonstrated significant treatment atic desensitization, modeling, and social skills training
response among children receiving IGBT, whereas (see Cornacchio, Sanchez, et al., 2017).
children on the waitlist did not improve. Immediate IGBT for SM is novel in structure and intensity.
posttreatment results found significantly greater improve- Whereas previously supported treatments for children
ments in social anxiety severity, verbal behavior in social with SM typically are implemented as individual sessions,
settings, and global functioning among IGBT-treated once or twice a week (Bergman et al., 2013; Oerbeck et al.,
children relative to waitlist children. Follow-up evalua- 2014), IGBT for SM benefits from access to other affected
tions during the following school year of treated children children via the group setting and allows for more
found that, with time, improvements even broadened frequent interactions during the camp intensive week.
across additional domains—such as reduced SM severity, Additionally, the camp has often been conducted in
increased verbal behavior in the home setting (e.g., with conjunction with other summer treatment programs (if
babysitters, family members) and reduced overall anxiety. other camp-like programs are offered nearby or within
These findings include controlling for service use the same organization) and therefore has allowed for
Please cite this article as: Lorenzo et al., Expanding Treatment Options for Children With Selective Mutism: Rationale, Principles, and
Procedures for an Intensive Group Behav..., Cognitive and Behavioral Practice (2020), https://doi.org/10.1016/j.cbpra.2020.06.002You can also read