Role and Responsibility of Nurses in Central Line - Insertion and Maintenance - Insertion ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
International Journal of Research and Review
DOI: https://doi.org/10.52403/ijrr.20210935
Vol.8; Issue: 9; September 2021
Website: www.ijrrjournal.com
Short Communication E-ISSN: 2349-9788; P-ISSN: 2454-2237
Role and Responsibility of Nurses in Central Line -
Insertion and Maintenance
R. Surendra Naik1, Avadhesh Kumar Yadav2, Rajendra Kumar Sahu3,
Ram Niwas Sharma4
1
Nursing Officer-A (MHM) (Officer In-Charge Surgical ICU), Mahamana Pandit Madan Mohan Malviya
Cancer Centre Varanasi Uttar Pradesh 221005.
2
Nursing Officer-B, Officer In Charge (Pediatric and Laser Surgery), Mahamana Pandit Madan Mohan Malviya
Cancer Centre Varanasi Uttar Pradesh 221005, (A Unit of Tata Memorial Centre Mumbai, Department of
Atomic Energy)
3
Nursing Officer-A, M.Sc. (MHN), Mahamana Pandit Madan Mohan Malviya Cancer Centre Varanasi
Uttar Pradesh 221005.
4
Nursing Officer-B, Officer In Charge, Mahamana Pandit Madan Mohan Malviya Cancer Centre Varanasi
Uttar Pradesh 221005, (A Unit of Tata Memorial Centre Mumbai, Department of Atomic Energy)
Corresponding Author: Rajendra Kumar Sahu
ABSTRACT which can obstruct the airway, Tracheal injury,
Air emboli during venous puncture or removal
Introduction -A central venous catheter (CVC) of the catheter, Pulmonary embolism, Local
is thin, a flexible tube (catheter) that is placed cellulitis, Catheter infection, Cardiac
into a large vein above the Heart. It may be tamponade, Intravascular loss of guidewire,
inserted through A vein in the Neck, (internal Hamo thorax, Phrenic nerve injury, Brachial
jugular) chest (subclavian vein. Axillary vein) plexus injury, Cerebral infarct from carotid
groin (femoral vein), or through veins in the artery cannulation, Bladder perforation, Bowel
arms known as a PICC, or peripherally inserted perforation, Sterile Thrombophlebitis.
central catheters. Post-procedural complications: Catheter-
Site- Internal jugular vein, subclavian vein, related bloodstream infections – bacterial or
axillary vein, femoral veins, the best approach fungal, Central vein stenosis, Thrombosis,
or access point for Central line insertion. Delayed bleeding with multiple attempts in a
Indications - The indications for central venous coagulopathic patient Clinical
access are broad and are often situational. Significance - Ensure that sterile products are
Inability to obtain venous access in emergent not contaminated and that there is no evidence
situations, chemotherapy administration, of damage to the packaging. Follow sterile
medications administration (Vasopressors. procedures at all times. Central line infections
inotropic administration Total Parental nutrition can be a serious and life-threatening illness.
administration, Hemodynamic monitoring are Always ensure that the catheter is appropriately
common indications for CVC insertion. placed through one or several methods:
Contraindication- Local cellulitis, Low platelet radiographic evidence, measurement of CVP, or
count, Local infections, Thrombocytopenia, by analyzing a venous blood gas. Never use
Congenital anomalies, Trauma are common excessive force during any part of this
contraindications of CVC insertion. procedure. It will lead to damage to local
Complications - Numerous potential structures.
complications can occur during the procedural Nursing Responsibility - After a CVC
placement of a central venous catheter, but also placement, nurses are responsible for
as a result of the indwelling equipment. maintaining, monitoring, and utilizing central
Arrhythmias, Arterial puncture, Pulmonary venous catheters. The assigned nurse must
puncture with or without resultant check complications such as infections,
pneumothorax, Bleeding – hematoma formation, hematoma, thrombosis of the catheter, and signs
International Journal of Research and Review (ijrrjournal.com) 252
Vol.8; Issue: 9; September 2021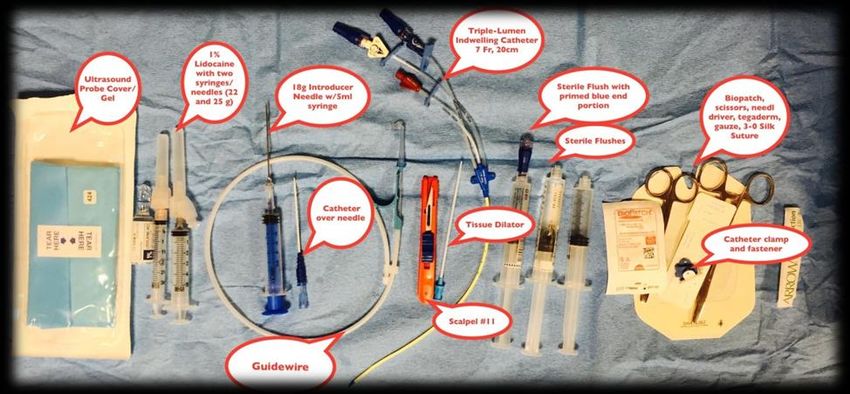
R. Surendra Naik et.al. Role and responsibility of nurses in central line – insertion and maintenance.
of pneumothorax and bleeding. Nurses are also Internal jugular vein, subclavian
responsible for ensuring that the site is vein, axillary vein, femoral veins, the best
maintained in a clean and sterile fashion. Daily approach or access point varies always
inspection of the access site and device patency depend up on patient condition and clinical
should be performed during nursing rounds. In needs IJV or EJV this vein lie both sides of
particular, nursing officers must disinfect
neck this vein carry deoxygenated blood
injection ports, catheter hubs, and needleless
connectors with institutionally approved from head, face, and neck towards the heart
antiseptics. Intravenous administration sets both veins unite to subclavian vein, the
should be changed regularly per hospital policy. Internal Jugular approach allows for
The site should be checked for bleeding, ultrasound Guidance approach While
hematoma formation, and signs of cellulitis, following this approach insertion related
which include erythema, purulent drainage, complication reduced ,disadvantages
and/or warmth. Dressings should be changed if includes in this approach is arterial
visibly soiled. This must be performed with puncture, infection rates is higher than
proper sterile technique. subclavian approach the internal jugular site
more preferable for temporary dialysis
Keywords - CVC, Central Line, Central venous
purpose and this site not a first choice in
catheter
post tracheostomies or post vascular
surgical patients adjacent anatomy includes
INTRODUCTION
A central venous catheter (CVC) is carotid artery ,phrenic and vagus nerves
thin, a flexible tube (catheter) that is placed pulmonary apex, thoracic duct The External
into a large vein above the Heart. It may be Jugular veins are located outside of the
inserted through a vein in the Neck, SCM, This veins are easily visible from the
(internal jugular) chest (subclavian vein. surface making it easy to locate ,uses of
Axillary vein) groin (femoral vein), or External Jugular Veins is considered
through veins in the arms known as a PICC, advanced skill the veins close to proximal
or peripherally inserted central catheters It’s carotid artery, the adjacent anatomy
also called central venous line or central line includes carotid artery, phrenic artery,
some catheters have 2 are 3 tubes (double pulmonary apex thoracic duct the Sub
are triple lumen catheters. clavian veins are lies below the clavicle
A central venous catheter is an which is located above the 1st Rib An
invasive catheter that is peripherally extension of the large axillary vein ,it begins
inserted into the (veins large and small at outer border of the first Rib passage over
veins) mostly preferable in the internal the Rib extend to inner border of clavicle,
jugular and subclavian or femoral veins, the for subclavian vein adjacent anatomy
term central line first described in 1929 after includes Right Lymphatic duct,
that venous access following rapidly costoclavicular ligament, first Rib Axillary
increased as like an important device that veins is a continuation of brachial veins
mainly used in cardiac surgeries for central cephalic veins continuous to becomes
venous pressure monitoring and pulmonary subclavian veins at Lateral border of first
artery pressure monitoring, Glenn pressure Rib, Adjacent anatomy includes Cephalic
monitoring purposes useful central line vein, subclavian vein, First Rib ,clavicle
mostly for hemodynamic monitoring for femoral vein is the main vein in the leg and
critically ill patients in critical care units accompanies to the femoral artery in the
Renal Replacement purpose for emergency femoral sheath, it stretches from the
resuscitation using in critical care units. adductor canal to the internal jugular
ligament at which point it becomes the
Anatomy and physiology: Central venous external iliac veins the femoral nerve which
line mainly following three sites less outside the femoral sheath
International Journal of Research and Review (ijrrjournal.com) 253
Vol.8; Issue: 9; September 2021
R. Surendra Naik et.al. Role and responsibility of nurses in central line – insertion and maintenance.
Indications Resuscitation of intravascularly depleted
The indications for central venous patients
access are broad and are often situational
(1). In no particular order, they include: Contraindication
Inability to obtain venous access in Local cellulitis
emergent situations. Low platelet count
For critically ill patients (ICU patients Local infections
with septic shock. Cardiac surgery Avoid intracranial pressure raised when
patients mostly required in pediatric femoral approach required
patients) Patient Non-compliance
For chemotherapy administration Thrombocytopenia
medications administration Congenital anomalies
(Vasopressors. inotropic administration Trauma
Total Parenteral nutrition administration Typically, patients who have an
Hemodynamic monitoring, including international normalized ratio (INR) of
central venous pressures. Glenn greater than 3.0 patients who have low
pressures platelets count less than 150000 this patient
For venous interventions, including may have an increases Risk of bleeding It
inferior vena cava filter placement, and may be warned sign to transfuse platelets or
cardiac surgery patients may need fresh frozen plasma the central line is
For a long time, pain management contraindicated in coagulopathy’s patients,
For hypertonic fluid administration
For Emergency Renal Replacement
Therapy
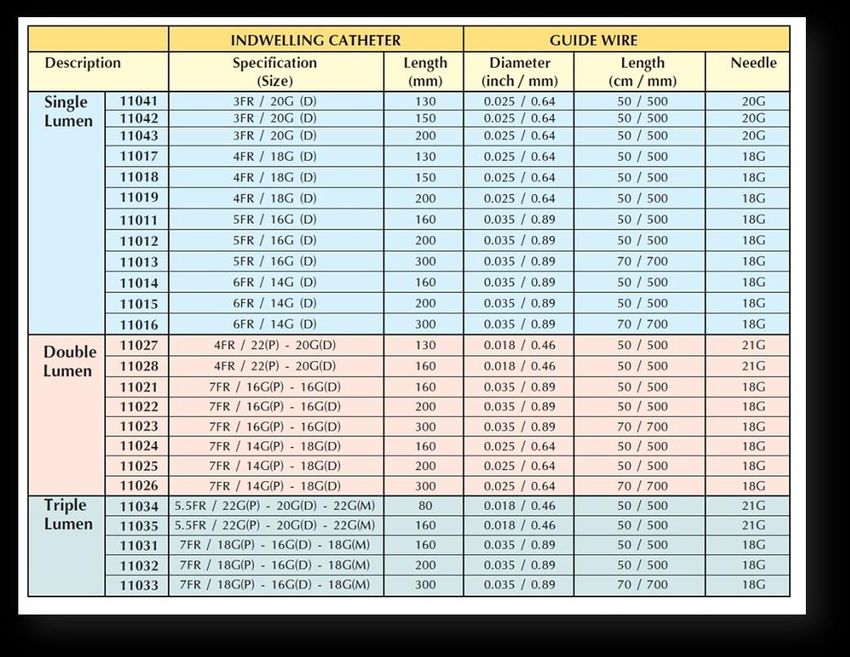
Sizes of Central line:
International Journal of Research and Review (ijrrjournal.com) 254
Vol.8; Issue: 9; September 2021
R. Surendra Naik et.al. Role and responsibility of nurses in central line – insertion and maintenance.
Equipment Sterile products:
There are various types of Personal protective equipment:
manufactures central line catheters kits is including gloves, gown
available in different types of catheters ICU pack (small towel. Big towel.
basically required equipment are following Whole towel drape)
that ultrasound machine with linear probe Gown pack (sterile gown with rapper)
.camera cover, jelly, and personal protective Surgical gloves are an appropriate size.
equipment’s (cap mask gown gloves shoo Gauze (4x4)
cover ) ICU pack which may include drapes Chlorohexidine, bactoprep
(small towel big towel whole towel drape) Sterile ultrasound probe covers with
gown pack sterile surgical gloves suture sterile ultrasound gel
material 10 cc syringe local(lignocaine2%) Camera cover
sterile needle 100 ml normal saline gauze Biopath
pieces and Gamze pad central line Tigard "Lure locks" or catheter caps for each
rum proper biomedical waste management. lumen
Central venous catheter kit, which
generally includes:
Central venous catheter (triple-lumen,
dual-lumen, or large bore single-lumen)
18-gauge introducer needle, with a
syringe
#11 blade Scalpel
Guidewire
Venodilator
Suture material (generally 3-0 silk
suture with a straight needle or a needle
driver)
Normal saline for locking purpose
2% lidocaine, small gauge needle (25 or
Non-sterile products: 27 gauge), syringe
Cap surgeon Ultrasound machine with a high-
Mask with face shield frequency linear transducer
Biomedical waste bins (red yellow. Camera cover
Block) for safe disposal of waste Jell for probe
management
Sharp container
International Journal of Research and Review (ijrrjournal.com) 255
Vol.8; Issue: 9; September 2021
R. Surendra Naik et.al. Role and responsibility of nurses in central line – insertion and maintenance.
ICU INTENSIVIST: Apply sterile drapes over the patient
CVC insertion should be performed with the exposure of site only. Open the
by a proceduralist skilled in the technique CVC kit in a sterile manner.
and a nurse to assist. Before insertion assesses the site and
checks the landmark and identify the vein
and mark if Necessary.
Instruct the patient to turn his or her
head slightly away from the insertion site.
Apply local 2% Lignocaine. Place
the sterile probe over the ultrasound
equipment and locate the vessel.
Technique
Place the patient in the
Trendelenburg position and apply bolster.
Clean the area with chlorhexidine 2%.
Use Seldinger technique to puncture
the skin and advanced the needle while
maintaining slight negative pressure with a
syringe until the free flow of blood is
returned. Instruct the patient to hold his
breath.
Preparation Insert the guidewire into the needle
First explain the need for central line then remove the needle.
insertion and assess The patient and family Insert the dilator in the vessel with
understanding. the help of a guidewire. Dilate the vessel
Explain to family members about with the help of a dilator and observe the
central line procedure, benefits, and bleeding pattern. Hold the guidewire and
complications and obtain informed consent. gently remove the dilator.
Examine the patient's past medical Insert the central venous catheter
history example past surgeries related to the with the help of a guidewire. Check the
chest neck are femoral region. backflow of each lumen and flush with
Determine the patient medical normal saline all lumen. “Lure locks” may
history related to pneumothorax or be attached to the end of each port and clean
emphysema. with 2% chlorhexidine solution.
Assess the intended site (IJV. EJV. Fix the central venous catheter by
Subclavian. Axillary. femoral). placing sutures, a bio-patch should be
Perform the procedure for this need placed between the catheter hub and the
to arrange all equipment needed for skin, and a sterile occlusive dressing should
insertion of CVC line. be placed over the catheter/skin entry site.
Prepare ultrasound machines with Sterile drapes and soiled non-sharp
the linear probe with jelly and arrange all products should be disposed of as per
personnel protective equipment (cap mask hospital policy. All sharps should be placed
glove sterile gown face shield). in sharps bins. The patient should be placed
Place the waterproof pad beneath the back into a position of comfort, and the
site to be accessed and make sure that Physician should verify that the line is
patient is in Trendelenburg position. appropriately placed within a central vein.
Prepare the skin with an antiseptic Confirmation of catheter in situ
solution (2%chlorohexidine). Perform hand should be done by X-ray.
hygiene and apply sterile gown and gloves.
International Journal of Research and Review (ijrrjournal.com) 256
Vol.8; Issue: 9; September 2021
R. Surendra Naik et.al. Role and responsibility of nurses in central line – insertion and maintenance.
Document procedure details with efficacious, and potentially life-saving.
date and time in patients' records, maintain However, certain clinical pearls should be at
asepsis as per infection control committee the forefront of the proceduralist’s mind
guidelines. A Central line-related when performing this procedure.
bloodstream infection (CLABSI) chart Whenever possible, take the time to
should be maintained. fully prepare for the procedure, and
assure that all necessary personnel and
Complications equipment are in the room and readily
Numerous potential complications available. Lack of preparation will
can occur during the procedural placement compound any potential complications
of a central venous catheter, but also as a that may be encountered.
result of the indwelling equipment. Ensure that sterile products are not
contaminated and that there is no
Procedural complications: evidence of damage to the packaging.
Arrhythmias – typically ventricular or Follow sterile procedures at all times.
bundle branch blocks due to guidewire Central line infections can be a serious
irritation of the atria or ventricle and life-threatening illness.
Arterial puncture When using the IJ or SC site for
Pulmonary puncture with or without access, be sure to obtain a stat portable
resultant pneumothorax chest x-ray immediately after line
Bleeding – hematoma formation, which placement to ensure there is no
can obstruct the airway pneumothorax and that the line
Tracheal injury terminates in the superior vena cava.
Air emboli during venous puncture or If one has a failed attempt at the IJ site
removal of the catheter and needs to seek access at another site,
Pulmonary embolism the ipsilateral subclavian is preferred,
Local cellulitis given the risk of bilateral
Catheter infection pneumothoraxes with an attempt at the
Cardiac tamponade contralateral internal jugular vein. One
Intravascular loss of guide wire may anticipate this possibility by
Hemothorax cleaning and prepping both the IJ and
Phrenic nerve injury SC site on the side of the procedure.
Brachial plexus injury If unsure of the placement of a
Cerebral infarct from carotid artery guidewire within the vein, and limited
cannulation views on ultrasound, manometry is a
Bladder perforation useful tool to establish that the
Bowel perforation guidewire is within the venous system.
Sterile Thrombophlebitis However, in shock states, where arterial
pressure is low, this may be falsely
Post-procedural complications: reassuring.
Catheter-related bloodstream infections Subclavian access does appear to have
– bacterial or fungal fewer infections but potentially higher
Central vein stenosis procedural complications, especially if
Thrombosis performed by a clinician with limited
Delayed bleeding with multiple attempts experience.
in a coagulopathic patient The internal jugular, subclavian, and
femoral veins have higher success rates
Clinical Significance and fewer complications when access is
When performed properly, the performed with ultrasound.
insertion of a central venous catheter is safe,
International Journal of Research and Review (ijrrjournal.com) 257
Vol.8; Issue: 9; September 2021R. Surendra Naik et.al. Role and responsibility of nurses in central line – insertion and maintenance.
The clinician must maintain hold of the complication rates increase when lines
guidewire at all times while it is inside are left in too long.
the patient. The wire can be lost inside
the patient and may migrate into the Daily care of Patient with Central Line
right ventricle or inferior vena cava, Daily inspection of the access site and
leading to additional invasive device patency should be performed
procedures to recover the wire. during nursing rounds.
Always ensure that the catheter is In particular, nursing officers must
appropriately placed through one or disinfect injection ports, catheter hubs,
several methods: radiographic and needleless connectors with
evidence, measurement of CVP, or by institutionally approved antiseptics.
analyzing a venous blood gas. Intravenous administration sets should
Never use excessive force during any be changed regularly per hospital policy.
part of this procedure. It will lead to The site should be checked for bleeding,
damage to local structures. hematoma formation, and signs of
cellulitis, which include
Nursing Responsibility erythema, purulent drainage, and/or
After procedure warmth.
After a CVC placement, nurses are Dressings should be changed if visibly
responsible for maintaining, monitoring, soiled. This must be performed with
and utilizing central venous catheters. proper sterile technique.
The assigned nurse must check Importantly, any manipulation of the
complications such as infections, catheter site should be done using a
hematoma, thrombosis of the catheter, sterile procedure. A bouffant cap, mask,
and signs of pneumothorax and and sterile gloves must be worn to
bleeding. minimize infection.
Nurses are also responsible for ensuring The site should be cleaned with
that the site is maintained in a clean and approved antiseptics, allowed to dry,
sterile fashion. and a sterile occlusive dressing must be
Beyond the immediate complications of replaced.
the procedure itself, the nursing officer At interprofessional team rounds, there
must be immediately aware of any should be a daily discussion about
ongoing issues and delayed whether or not the central venous
complications. catheter is still indicated. If deemed
Their role in the interprofessional team unnecessary for further management, the
is of monumental importance in central venous catheter should be
maintaining the central venous catheter removed expeditiously.
and recognizing potential complications.
Clear communication between all team Safety Guidelines while central line care
members is essential to appropriate 1. Wash hands before doing any central
patient care. line care and wear gloves.
The clinician should inform the nurse as 2. Always keep a clean and dry dressing
soon as the proper placement of the over the central line.
CVC is confirmed, and nursing should 3. Follow the instructions for cleaning the
wait for this confirmation before using cap and using the sterile equipment.
the line to administer medications. Both 4. Always keep sharp objects away from
the nurse and the clinician should be the central line.
aware of and keep track of when the line 5. If the central line is hard to flush do not
was placed. CVC's are temporary, and try to flush inform the intensivist.
International Journal of Research and Review (ijrrjournal.com) 258
Vol.8; Issue: 9; September 2021R. Surendra Naik et.al. Role and responsibility of nurses in central line – insertion and maintenance.
6. Maintain CLABSIS bundles record date REFERENCES
of insertion and day of the catheter. 1. Beheshti MV. A concise history of central
7. As per CDC guidelines use only sterile venous access. Tech Vasc Interv
to access catheters. Radiol. 2011 Dec;14(4):184-5. [PubMed]
8. Immediately replace dressings that are 2. BOLT W, KNIPPING HW.
[Congratulations to Werner Forssmann on
wet, solid. Or dislodged winning the 1956 Nobel prize for
9. Perform routine dressing changes using medicine]. Med Klin. 1956 Dec 07;51(49):
aseptic technique with clean or sterile 2073-6. [PubMed]
gloves 3. Konner K. History of vascular access for
10. Change gauze dressing at least every hemodialysis. Nephrol Dial Transplant.
two days or semipermeable dressing at 2005 Dec;20(12):2629-35. [PubMed]
least every seven days 4. http”//booksite.elevevier.com/97803233766
11. For patients 18 years of age or older, use 2
chlorhexidine impregnated dressing with 5. Ipe TS, Marques MB. Vascular access for
FDA cleared label that specific a clinical therapeutic plasma exchange. Transfusion.
indication for reducing CLABSIS for 2018 Feb;58 Suppl 1:580-589. [PubMed]
6. American Society of Anesthesiologists Task
short-term non-tunneled catheters unless Force on Central Venous Access. Rupp SM,
the facility demonstrating success at Apfelbaum JL, Blitt C, Caplan RA, Connis
preventing CLABSIS with baseline RT, Domino KB, Fleisher LA, Grant S,
prevention practices. Mark JB, Morray JP, Nickinovich DG,
12. Change administration sets for Tung A. Practice guidelines for central
continuous infusions no more frequently venous access: a report by the American
than every 24 hours. Society of Anesthesiologists Task Force on
13. If blood products or fat emulsions are Central Venous Access. Anesthesiology.
administered change tubing every 24 2012 Mar;116(3):539-73. [PubMed]
hours 7. Suess EM, Pinsky MR. Hemodynamic
14. Perform a daily audit to assess whether Monitoring for the Evaluation and
Treatment of Shock: What Is the Current
each central line is still needed are not
State of the Art? Semin Respir Crit Care
15. Provide a checklist to the clinician to Med. 2015 Dec;36(6):890-8. [PubMed]
ensure adherence to aseptic insertion
practices. AUTHORS’ PROFILE:
16. Use hospital-specific or collaborative-
based performance measures to ensure Mr. R. Surendra Naik
compliance with recommended Nursing officer-A (MHM)
practices. (Officer In-charge Surgical ICU)
Mahamana Pandit Madan Mohan
17. Educate health care workers about Malviya Cancer Centre Varanasi
indications for a central line, proper Uttar Pradesh 221005.
procedures for insertion and
maintenance, and appropriate infection Mr. Avadhesh Kumar Yadav
prevention measures. Nursing officer-B, Officer in
charge (Pediatric and laser
Acknowledgement: None Surgery)
Mahamana Pandit Madan Mohan
Conflict of Interest: None Malviya Cancer Centre Varanasi
Uttar Pradesh 221005, (A unit of
Source of Funding: None Tata Memorial Centre Mumbai,
Department of Atomic Energy)
International Journal of Research and Review (ijrrjournal.com) 259
Vol.8; Issue: 9; September 2021R. Surendra Naik et.al. Role and responsibility of nurses in central line – insertion and maintenance.
Mr. Rajendra Kumar Sahu
Nursing officer-A How to cite this article: R. Surendra Naik,
M.Sc. (MHN) Yadav AK, Sahu RK et.al. Role and
Mahamana Pandit Madan Mohan responsibility of nurses in central line –
Malviya Cancer Centre Varanasi insertion and maintenance. International
Uttar Pradesh 221005. Journal of Research and Review. 2021; 8(9):
252-260. DOI: https://doi.org/10.52403/ijrr.
Mr. Ram Niwas Sharma 20210935
Nursing officer-B, Officer in
charge
Mahamana Pandit Madan Mohan
Malviya Cancer Centre Varanasi
Uttar Pradesh 221005, (A unit of
Tata Memorial Centre Mumbai,
Department of Atomic Energy)
******
International Journal of Research and Review (ijrrjournal.com) 260
Vol.8; Issue: 9; September 2021You can also read

















































