Robot-assisted revisional bariatric surgery - Digestive ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Review Article
Page 1 of 11
Robot-assisted revisional bariatric surgery
Cristina J. Ponce1^, Alfredo D. Guerron1, Ranjan Sudan2
1
Division of Metabolic and Weight Loss Surgery, Department of Surgery, Duke University Health System, Durham, NC, USA; 2Surgical Education
and Activities Lab, Department of Surgery, Duke University Health System, Durham, NC, USA
Contributions: (I) Conception and design: All authors; (II) Administrative support: All authors; (III) Provision of study materials or patients: None;
(IV) Collection and assembly of data: None; (V) Data analysis and interpretation: None; (VI) Manuscript writing: All authors; (VII) Final approval of
manuscript: All authors.
Correspondence to: Ranjan Sudan, MD, FACS, FASMBS. Professor of Surgery & Psychiatry, Vice Chair of Education, Director of Surgical Education
and Activities Lab, Department of Surgery, Duke University Health System, 407 Crutchfield St., Durham, NC 27704, USA.
Email: ranjan.sudan@duke.edu.
Abstract: As more bariatric procedures are performed every year in the United States, the number of
revisions has increased concomitantly. Most commonly indicated due to weight regain or insufficient weight
loss, these operations are usually more challenging and tend to be associated with higher morbidity rates than
primary surgery. Although technically demanding, revisional surgery offers additional weight management
and improvement of obesity-related comorbidities. Enhanced visualization, improved range of motion
and ergonomics, multi quadrant access, and motion scaling are all features that make robotic platforms
potentially promising for complex operations such as revisional bariatric surgery. A robotic approach also
reduces mechanical strain from thick abdominal walls and allows for easier hand-sewn anastomoses when
the field of vision is limited. Benefits need to be contrasted by the known limitations of longer operative
times (OTs), including docking, lack of haptic feedback, equipment costs, and the training needed to acquire
expertise. So far, most studies do not show significant differences in outcomes between robot-assisted and
laparoscopic approaches. Further advancement in the field and widespread use could likely bring costs down
and improve patient outcomes when chosen judiciously. Overall, robot-assisted revisional bariatric surgery
appears to be a safe and feasible alternative to laparoscopic revisional bariatric surgery (LRBS) for complex
patients.
Keywords: Robotic; robot-assisted; revisional; conversion; bariatric surgery; weight-loss surgery
Received: 20 January 2021; Accepted: 30 March 2021; Published: 30 June 2021.
doi: 10.21037/dmr-21-6
View this article at: http://dx.doi.org/10.21037/dmr-21-6
Introduction as the laparoscopic adjustable gastric banding (LAGB), are
not frequently performed nowadays (5,6). Along with the
Weight loss surgery is considered one of the best options
increasing numbers of bariatric procedures comes a larger
for long-term management of obesity and its associated pool of potential candidates for revisional surgery, making
comorbidities (1-3). Bariatric surgical volume has increased it the fastest-growing field in bariatric surgery (7). Revision
exponentially in the past years and has reached over surgery went up from 6% of all estimated bariatric surgeries
252,000 cases annually in 2018 (4). The most commonly in 2011 to 15.4% in 2018 (4).
performed bariatric procedure is sleeve gastrectomy (SG), The most common causes for revisional bariatric surgery
with 61.4% of all bariatric interventions. Other procedures, include inadequate weight loss, significant weight regain,
^ ORCID: 0000-0001-9019-1856.
© Digestive Medicine Research. All rights reserved. Dig Med Res 2021;4:35 | http://dx.doi.org/10.21037/dmr-21-6
Page 2 of 11 Digestive Medicine Research, 2021
and development or return of previously resolved or well- may need revision for improving outcomes. These vary
controlled obesity-related comorbidities such as type depending on the primary surgery (10,12). The most
2 diabetes (8). These indications account for 52.2% of commonly performed weight loss procedure, SG, has
revisional operations (9), while other reasons for revisional been associated with the development of gastroesophageal
or conversional bariatric surgery vary and are related to the reflux disease (GERD), sleeve stricture or dilation, and
persistence of comorbid conditions (10). In 2018, Angrisani anastomotic leaks (8). Complications related to RYGB
et al. published a global survey from the International include gastro gastric fistula, gastric pouch stricture or
Federation for the Surgery of Obesity and Metabolic dilation, gastro-jejunal (G-J) stricture or dilation, marginal
Disorders (IFSO), gathering data from 58 national ulcers, severe malnutrition, vitamin deficiency, refractory
societies (6). They reported that the most revised index hypoglycemia or hypocalcemia, and even excessive weight
procedures were LAGB, with a failure/revision rate of 40– loss (8,21,22). It is also important to consider that weight
50%; SG, 25–36%; and Roux-en-Y gastric bypass (RYGB), loss surgery failure could not only be due to technical or
with a failure rate of 20% in morbidly obese patients and anatomical issues but also patient-related factors (23). These
up to 35% in the super-obese population (6). As far as include psychological and behavioral aspects that should be
the most commonly performed revisional procedures, it considered as part of the initial evaluation of a patient who
is worth noting the single-stage conversion from LAGB is regaining weight and need to be managed promptly with
to RYGB, SG to biliopancreatic derivation with duodenal a multidisciplinary team to ensure success (6,21,23).
switch (BPD-DS), and SG to single anastomosis duodeno- Although some of these complications can be addressed
ileal bypass with sleeve gastrectomy (SADI-S) (11). endoscopically (24,25), this chapter will focus on the
These procedures have been traditionally performed surgical management of bariatric surgery failure.
laparoscopically (12-14) since it became the standard
for minimally invasive bariatric surgery after being first Challenges of revisional surgery
described by Wittgrove et al. for RYGB in 1994 (15).
Robot-assisted bariatric surgery has gained popularity, Reoperative bariatric surgery appears to be more technically
and its numbers are increasing as more surgeons overcome challenging than the primary procedure and has been
the learning curve (16-18), and the current trend pointing associated with higher rates of 30-day adverse events (13),
towards it becoming more widespread in bariatric surgery leaks, and ICU stays (26). Chaar et al. (27) described a
(18,19). significant increase in the incidence of complications
The use of robot-assisted surgery has been promoted requiring 30-day reintervention, readmission, reoperation,
for revisional weight loss surgery in the past few years. ICU admission, and continued presence of surgical drain
Proponents of this technique postulate it to be the minimal following revisional RYGB and SG when compared to
access approach that resembles open surgery the most as a primary operations.
result of improved visualization, enhanced manipulation of Morbidity and mortality are usually higher in revisional
tissue by the wrist-like movement adapted to almost all the surgery than after the primary procedure (28,29). Although
instruments, and less dependence on the surgical assistants patients may have lost a considerable amount of weight by
the time they undergo revisional procedures, the presence of
for exposure and manipulation of the camera (18,20).
severe adhesions, obliterated surgical planes, and alteration
This chapter describes the current role of robot-
of anatomy following the index surgery could hinder the
assisted surgery in the revisional bariatric surgery field, its
surgeon’s ability to access the abdominal cavity safely. The
indications with their respective outcomes, technical tips,
surgeon might benefit from a careful examination of the
and potential pitfalls.
operative notes from the previous procedure to develop a
thorough understanding of the anatomic changes brought
Revision surgery about by the previous procedure (28,30). This kind of
understanding of the previous surgery could sometimes
Causes
be unavailable, so surgeons may have to rely on imaging
Although the main indication for revisional surgery seems techniques, endoscopy, or both, pre- and intra-operatively (30).
to be weight regain or inadequate weight loss following the Díaz et al. propose esophagogastroduodenoscopy (EGD) as
index procedure (9), several other chronic complications the best way to evaluate postoperative anatomy in bariatric
© Digestive Medicine Research. All rights reserved. Dig Med Res 2021;4:35 | http://dx.doi.org/10.21037/dmr-21-6Digestive Medicine Research, 2021 Page 3 of 11
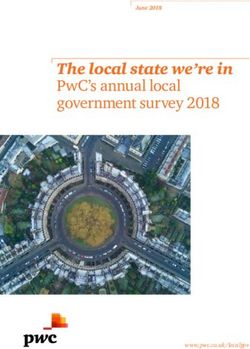
A B
Liver retractor
Robo port
Assist port
12–15 mm
optional/marked
Camera
Stapler
12 mm
12 mm8 mm
Figure 1 Usual trocar placement for robotic platform-assisted bariatric surgery. (A) Scheme; (B) surgeon’s view.
patients (31). Lee Bion et al. recommend performing a for SG strictures has been performed with acceptable
morphological evaluation before the revision procedure, results (37-39), further studies are guaranteed in order to
including at least a CT scan with gastric volumetry and an recommend this approach.
EGD (32). Decreased vascularization as a consequence of Our approach consists of thorough anatomy delineation
the primary procedure needs to be considered as well (5). using contrast-enhanced studies and endoscopy. Direct
Possible tissue avascularity could negatively impact the communication with the surgeon who performed the index
healing process of the anastomoses in the revision. Robotic operation is highly desired. A multidisciplinary approach
platforms offer the additional advantage of allowing for with early and aggressive involvement of the nutrition and
near-infrared fluorescence with indocyanine green (ICG) psychology departments is paramount.
intra-operatively. The ongoing discussion for the various Preoperative preparation follows standard antibiotic and
uses for ICG has suggested it could be helpful to assess venous thromboembolism (VTE) prophylaxis. Appropriate
tissue perfusion (33,34). At our center, we favor using padding to protect pressure areas and nerves is critical, as
ICG fluorescence to check for leaks after finalizing the the cases are lengthy.
anastomoses. We prefer to perform laparoscopy to assess the anatomy
However, most studies analyzing perioperative prior to placement of robot ports. Four ports are utilized
outcomes in revisional bariatric surgery agree that this for the robotic arms and camera, with an additional assistant
should not preclude patients from getting a revision port, which needs to be available for additional retraction
since the procedures are becoming safer with time and or suctioning (Figure 1). Hand-sewing methods are our
experience (35). In the hands of skilled surgeons, the risk preferred method of anastomoses in almost all cases (Figure 2).
of complications becomes justifiable when compared to
the potential benefits (8). Although challenging, Sudan
Robot-assisted bariatric surgery
et al. reported that revisional bariatric surgery was deemed
safe, and its higher morbidity was acceptable from a Cadiere et al. reported the first robotic bariatric procedure
clinical perspective when considering weight loss achieved, in 1999, a successful, purely robot-assisted, adjustable
comorbidity resolution, and overall long-term benefits (36). gastric banding (40). In 2000, after the Food and Drug
In our center, we favor a robot-assisted approach for Administration (FDA) cleared the Da Vinci Surgical System
bariatric revisional surgeries. Operations such as conversion (Intuitive Surgical, Sunnyvale, CA, USA) for use in general
from sleeve to RYGB secondary to refractory GERD are surgical procedures, both robot-assisted BPD-DS (RABPD-
common, as are band removals with conversion to RYGB, DS) and RYGB (RARYGB) were successfully performed
SG, or biliopancreatic diversion with duodenal switch by Sudan et al. and Horgan et al. respectively (17,41). Since
(BPD-DS). Additional conversions for weight regain from then, the applications for robotics in bariatric surgery
sleeve to BPD-DS are excellent cases to utilize robot- have evolved. From initial hybrid approaches (42-44)
assisted technology. that combined traditional laparoscopy with a robotic
Although controversial, robot-assisted stricturoplasty approach for specific tasks such as hand-sewn G-J or
© Digestive Medicine Research. All rights reserved. Dig Med Res 2021;4:35 | http://dx.doi.org/10.21037/dmr-21-6Page 4 of 11 Digestive Medicine Research, 2021
A B
C D
Figure 2 Robot-assisted revisional RYGB with hand-sewn anastomosis technique. (A) Gastric pouch formation; (B) G-J anastomosis; (C) J-J
anastomosis; (D) mesenteric gap closure. RYGB, Roux-en-Y gastric bypass; G-J, gastro-jejunal; J-J, jejuno-jejunal.
duodeno-ileal (D-I) anastomoses during RYGB or BPD- similarity in post-op complication profiles suggests the
DS, to fully robotic primary weight loss procedures with higher morbidity traditionally associated with laparoscopic
similar benefits as the laparoscopic approach (45). The main revisional bariatric surgery (LRBS) could be decreased to
limitations of robotic surgery have usually been the higher the level of primary procedures with the robotic platform’s
costs and longer operative times (OTs) with no significant help.
differences in the outcomes (46,47). Conversely, Beckmann
et al. (48) proved robotic primary RYGB (n=114) to have a
Technical advantages
shorter OT and a lower complication rate than laparoscopic
primary RYGB (n=108). Lainas et al. (49) also reported a Early experience with robotic systems seems to outline that
shorter OT with a robot-assisted vs. laparoscopic approach the robot’s role is not to replace the surgeon but to help them
for RYGB with similar post-op complications, length of perform complicated tasks more accurately and repetitive
stay (LOS), and weight loss outcomes. Meanwhile, Acevedo tasks more precisely than standard laparoscopy (54).
et al. (47) found a robotic approach was associated with Robot-assisted surgery provides the surgeon with tools
lower morbidity and mortality in primary RYGB, unlike in such as improved visualization through stereoscopic 3D
SG, where it was considered not cost-effective. A systematic vision (54,55). There is increased precision by stabilizing
review with meta-analysis published by Economopoulos and downscaling the amplitude of the surgeon’s motions
et al. (50) analyzing robotic vs. laparoscopic RYGB pointed by a factor of five or three to one (56) and eliminating or
towards comparable clinical outcomes. It underlined the filtering physiological tremor (18). Manipulation of tissue is
need for higher-quality studies in the future. also enhanced by the increased range of motion provided by
Robot-assisted surgery has proved to be safe, feasible, the wrist-like quality of the novel instruments resembling an
and effective for bariatric operations (51,52), but the open technique (56). Robot-assisted surgery also overcomes
challenge to determine its value remains. One area to look torque on thick abdominal walls, a characteristic limitation
at for a higher robotic platform value is the revisional field of the standard laparoscopic approach (55). Torque on
in weight loss surgery. Iranmanesh et al. (53) found overall laparoscopic instruments leads to imprecise technical
comparable outcomes between 806 patients undergoing movements and surgeon fatigue.
primary robotically assisted laparoscopic (RAL) RYGB Bariatric surgery may require intervention in various
and 266 revisional RAL RYGB. They reported that this quadrants of the abdomen, so hybrid techniques using a
© Digestive Medicine Research. All rights reserved. Dig Med Res 2021;4:35 | http://dx.doi.org/10.21037/dmr-21-6Digestive Medicine Research, 2021 Page 5 of 11
combination of laparoscopy and robot have been developed. the laparoscopic procedure was at 2% or more. However,
However, these have been mitigated by the advances of the if the leak rate fell under 2% for laparoscopy, the robotic
new Da Vinci Xi System by Intuitive Surgical (Sunnyvale, procedures were not as effective. Sensitivity analysis
CA, USA). Sudan et al. reported a successful conversion performed in this study also showed that an increase in
from laparoscopic adjustable gastric band to totally robotic the monthly robotic caseload also helped lower the overall
BPD-DS, using a single dock, multi quadrant strategy (57). cost per procedure, making it cheaper than laparoscopic
This new approach seems helpful for the process of RYGB. The significance threshold was ten monthly cases
measuring limbs after demonstration of easy access for if the leak rate was 2% or seven cases if the leak rate was
splenic flexure mobilization with concomitant pelvic surgery above 2%. The savings found by Hagen et al. were related
by Protyniak et al. (58). to the prevention of leaks with hand-sewn anastomoses in
Benefits from a robotic surgical approach may extend robotic surgery compared to stapled anastomoses during
even to the surgeon. Laparoscopic surgery has been laparoscopy. Leaks usually generated higher costs, and
associated with ergonomic issues due to prolonged preventing the complications altogether made the net cost
operation time in unnatural and sometimes awkward difference more favorable. Hagen et al. concluded that the
postures (18,56,59). This has led to more surgeons suffering robotic approach could be better suited for very complex
from excessive fatigue and career-shortening occupational procedures where the laparoscopic skills are at their limit,
musculoskeletal injuries (55,60,61). The robotic platform such as revision bariatric procedures. It is also essential to
offers a more neutral position with comfortable seating, consider that costs may peak during the initial part of the
avoids forced movements, and decreases the strain on the learning curve (63). Combining relative inexperience with
surgeon’s shoulders, neck, and back muscles by relying more expensive technology may cause the costs to increase
on the robotic arms to overcome torque forces (16,18). until operating room (OR) time can be lowered to an
This ergonomic approach, improved posture, and reduced acceptable point. This is also true when starting a full-on
operator fatigue could help the surgeon prolong their career new robotic program. Initial costs of the robotic equipment
and perform hand-sewn anastomoses and difficult dissection will seem steep at first but will pay off later on when the
with fewer challenges and more freedom of movement (55). increase in surgical volume and better allocation of material
resources can amortize the total cost.
El Chaar et al. used data from the Metabolic and
Challenges of robotic surgery
Bariatric Surgery Accreditation and Quality Improvement
Costs Program (MBSAQIP) database between 2017 and 2018
Adair et al. described a cohort of 753 robotic SG (RSG) to compare the costs of RSG vs. LSG, including OR
matched to 1,506 laparoscopic SG (LSG) patients from time, LOS, and supplies, on patients undergoing the same
data extracted from the National Inpatient Sample (NIS) preoperative workup and postoperative protocol (64). The
database between 2011 and 2013 (62). Although they found analysis showed no statistically significant overall cost
no statistically significant differences in postoperative differences between 39 RSG and 59 LSG patients. Median
complications or in-hospital mortality, the LOS and total cost for RSG was $5,308.99 vs. $4,918.88 for LSG (P>0.05).
hospital charge (THC) were significantly higher in the However, the median cost associated with OR time was
robotic cohort when compared to laparoscopic operation in significantly higher in the RSG cohort, $1,341 vs. $1,112
multivariable analysis adjusted for type of hospital, region, (PPage 6 of 11 Digestive Medicine Research, 2021
correlated with increased experience acquired with each described the learning curve for RABPD-DS as 50 cases (70).
case (64). Buchs et al. identified two distinct phases of the
Although several articles have been published related learning process for RARYGB (72). The first 14 surgeries
to the generally higher costs of robotic surgery (18,65), it represent the initial learning curve phase, while the last 50
is important to remember that its applications continue to surgeries suggest a “mastery” phase where both potential
broaden. Also, the updates in the robotic platforms (58,66) complications and OT are reduced significantly (72).
and their payment structure could reduce the financial Robot simulators have also been proposed as a viable
investment associated with purchasing and maintaining technology to becoming proficient in technical skills
the system. This has been a barrier to adopting robotic before starting live cases (18). Instituting curricula such
platforms, especially in developing countries (67). In as the Fundamentals of Robotic Surgery program early
the future, as the applications and advantages of robotic in residency training will also reduce the learning curve.
surgery become more established, the increased volume, Learning both robotic and laparoscopic techniques
reduced learning curve, judicious use of equipment, and at the same time might prove useful to develop skills
reduced complications will make robotic platforms more simultaneously and in a way that may complement each
economical. In addition, robotic surgery could reduce other. Sanchez et al. reported significantly shorter OR
ergonomic injuries on the surgeon and provide an indirect times for RSG when the surgeon learned both techniques
cost-benefit. simultaneously (44). It is crucial to remember that the
Currently, scarce data is available regarding specific costs learning curve is not exclusive to the surgeon (3). Full
in robotic revisional bariatric surgery (RRBS). As surgical robotic teams need to be trained (nurses, assistants,
volume increases, more studies are needed to obtain residents, anesthesiologists). The whole team learns with
accurate and current data that allow for better-informed the surgeon and develops protocols about patient safety, OR
recommendations regarding the value of this technology. set-up, and instruments required (55). This team effort may
be reflected in reduced OR times with experience, better
Learning curve patient outcomes, less supply waste, and lower costs (55,74).
A learning curve can be quickly defined as an improvement This supports the idea of a standardized training program
in performance over time (68). It may also be measured that will allow the whole team to achieve dexterity and
as the time and ability to complete a task until failure is become more proficient, with subsequent cost-effectiveness
reduced to an acceptable point or altogether eliminated as the surgical volume increases (18).
(69,70). Every surgical procedure has a multifactorial
learning curve. The initial training period is usually
Outcomes
characterized by continuous repetition of tasks until
proficiency is achieved (69). During this phase of learning, Although robot-assisted primary bariatric surgery has
longer procedure times and higher complication rates not been shown to be superior to laparoscopic surgery
are common, and it is expected that these will diminish (46-50,75), it is possible that robotic surgery can thrive in
with acquired experience (70). Published evidence specialized circumstances. Weight loss surgery in super-
appears to point towards a shorter learning curve for obese patients and revisional bariatric surgery may be
robotic procedures when compared with the laparoscopic particular areas that benefit from a robotic approach
technique. However, it is worth noting that learning curve in technically challenging patients (5,16,20,53,76,77).
measurement is not entirely standardized in surgery and However, it is not easy to get to that stage without first
although some authors refer to OT as a parameter to developing the skills in primary cases (5). Some of the
measure the “learning” process, not every study reports OR higher-impact published literature has been summarized in
time equally; some include docking time while others do Table 1.
not, so care must be taken when interpreting these results. In a retrospective single-center report of revisional
Schauer et al. proposed that the learning curve for bariatric interventions, Beckmann et al. (76) analyzed
laparoscopic RYGB was 100 cases (71). Studies from the US 30 laparoscopic, four open, and 44 robotic procedures
and Europe show a learning curve of 25 to 35 cases in the in terms of 30-day postoperative outcomes. After
robotic RYGB cases (3,44,72). Vilallonga et al. reported a comparing revisional LRYGB with RRYGB, they found
learning curve of 20 cases for RSG cases (73). Sudan et al. that robotic interventions lasted on average 37 minutes
© Digestive Medicine Research. All rights reserved. Dig Med Res 2021;4:35 | http://dx.doi.org/10.21037/dmr-21-6Digestive Medicine Research, 2021 Page 7 of 11
Table 1 High-impact RRBS literature
Study Year Country Design Robotic cases Comparison Conclusions
Bindal 2015 United States RC N=32 RRBS – RRBS safe and effective, no increased
et al. (29) morbidity
Gray et al. 2018 United States RC N=18 RRBS N=66 LRBS RRBS with similar safety profile as LRBS
(78) with significantly shorter LOS
Clapp 2019 United States RC + MBSAQIP N=1,929 RRBS N=35,988 LRBS No significant differences in post-op
et al. (20) complications with increased OT and LOS
Rebecchi 2019 Italy PC N=68 RRBS – Low morbidity rate. Significantly shorter OT
et al. (79) and lower cost in last 10 cases vs. first 30
cases
Acevedo 2020 United States Matched RC + N=1,144 RRBS N=1,144 LRBS Significantly longer OT, LOS, and ICU
et al. (10) MBSAQIP admission for RRBS. In SG subgroup,
increased risk of sepsis and SSI
Nasser 2019 United States RC + MBSAQIP N=1,077 RR-SG, N=15,935 LR-SG, Higher complication rates in SG subgroup
et al. (80) N=1,230 RR-RYGB N=11,212 LR-RYGB and decreased complication rates in RYGB
subgroup
Moon 2020 United States RC N=30 RRBS N=64 LRBS RRBS associated with significantly longer
et al. (65) OT. Potential benefit for RRBS in more
complex operations
Dreifuss 2021 United States RC + MBSAQIP N=76 RRBS – Index procedure might influence the
et al. (81) outcomes, %EWL significantly higher after
LAGB vs. SG
RRBS, robotic revisional bariatric surgery; RC, retrospective cohort; LRBS, laparoscopic revisional bariatric surgery; LOS, length of
stay; PC, prospective cohort; MBSAQIP, Metabolic and Bariatric Surgery Accreditation and Quality Improvement Program database; OT,
operative time; RR-SG, robotic revisional sleeve gastrectomy; RR-RYGB, robotic revisional Roux-en-Y gastric bypass; SG, sleeve
gastrectomy; SSI, surgical site infection; RYGB, Roux-en-Y gastric bypass; %EWL, percentage excess weight loss; LAGB, laparoscopic
adjustable gastric banding.
less, were associated with a significantly lower increase in patients undergoing revisional weight-loss surgery (35,988
postoperative C-reactive protein (CRP) levels, and had laparoscopic and 1,929 robotic), they concluded that
an overall lower rate of complications (7.3% in RRYGB robotic surgery is associated with an extended hospital
vs. 22.2%in LRYGB). However, other series have failed stay and OR times without providing a significant benefit
to corroborate these results. Snyder et al. (77) published in outcomes. Interestingly, after comparing 220 RRBS vs.
their 7-year experience with robotic-assisted conversion 220 LRBS patients in propensity-matched cohort analysis
of failed restrictive procedures to RYGB, and even though of the MBSAQIP database, El Chaar et al. (14) found a
outcomes were equivalent to the laparoscopic standard, clinically, though not statistically, significant reduction
they associated RRYGB with a significant immediate in the incidence of 30-day serious adverse events (SAE),
postoperative complications rate (17%); moreover, 24% 30-day organ-specific infections (OSI), 30-day reoperation,
of patients where readmitted 90 days after the procedure and 30-day intervention following RRBS. However, in the
due to issues related to the operation. Likewise, Clapp subgroup analysis, this was found to be true for RYGB and
et al. (20) retrospectively reviewed the MBSAQIP database not for SG, suggesting again that the robotic approach’s
from 2015 to 2016 to compare revisional laparoscopic improved outcomes could be advantageous in the more
weight loss surgery with revisional robotic weight loss technically challenging procedure.
surgery and failed to find a significant advantage of the Dreifuss et al. (81) found a significant difference in
robot in terms of postoperative complications. percentage excess weight loss (%EWL) when index
Further, after comparing data from over 35,000 procedure was LAGB vs. SG, and, although not statistically
© Digestive Medicine Research. All rights reserved. Dig Med Res 2021;4:35 | http://dx.doi.org/10.21037/dmr-21-6Page 8 of 11 Digestive Medicine Research, 2021
significant, Gray et al. (78) found a difference in the post-op by the editorial office, Digestive Medicine Research for the
complication rate between patients undergoing conversion series “Advanced Laparoscopic Gastric Surgery”. The
after a stapled index procedure (27%) and non-stapled index article has undergone external peer review.
procedure (17%). These two studies suggest there could
be some influence from the type of index procedure in the Peer Review File: Available at http://dx.doi.org/10.21037/
outcomes though no causality has been established due to dmr-21-6
lack of prospective studies. Further research is necessary
with subgroup analysis to determine the relevance of these Conflicts of Interest: All authors have completed the
findings. ICMJE uniform disclosure form (available at http://
Most available literature regarding RRBS is limited dx.doi.org/10.21037/dmr-21-6). The series “Advanced
to retrospective cohorts (RCs) or case series, with no Laparoscopic Gastric Surgery” was commissioned by the
controlled or prospective studies to establish adequate editorial office without any funding or sponsorship. ADG
statistical parameters. Also, even the large sample size served as the unpaid Guest Editor of the series and serves
studies with the MBSAQIP database are limited to 30-day as an unpaid editorial board member of Digestive Medicine
outcomes due to the nature of the data collected. Some of Research from Dec 2019 to Nov 2021. ADG has received
the studies report inconsistent follow-up with the patients, honoraria as a consultant for Levita and as a speaker for
hindering their ability to draw middle- and long-term Gore and Medtronic. Dr. ADG reports personal fees
conclusions, especially regarding weight management. Also, from Levita, personal fees from Gore, personal fees from
robotic-approach surgery may not be readily available in Medtronic, outside the submitted work. The authors have
smaller centers or lower-income settings, with results not no other conflicts of interest to declare.
being applicable everywhere.
Ethical Statement: The authors are accountable for all
aspects of the work in ensuring that questions related
Conclusions
to the accuracy or integrity of any part of the work are
Revisional bariatric surgery appears to be one of the most appropriately investigated and resolved.
promising areas for robotic development; the field is
continuously and unequivocally evolving. The discrepancies Open Access Statement: This is an Open Access article
reported in the literature may be explained by the lack distributed in accordance with the Creative Commons
of clear patient-selection guidelines for robot-assisted Attribution-NonCommercial-NoDerivs 4.0 International
interventions and by the somewhat recent introduction License (CC BY-NC-ND 4.0), which permits the non-
of robotics in the field. In all likelihood, RRBS will have commercial replication and distribution of the article with
a substantial impact in the years to come. It is a safe the strict proviso that no changes or edits are made and the
alternative that achieves comparable outcomes to standard original work is properly cited (including links to both the
laparoscopy. Widespread use will likely bring costs formal publication through the relevant DOI and the license).
down, and further research could show improved patient See: https://creativecommons.org/licenses/by-nc-nd/4.0/.
outcomes. It is our view that robotic surgery should be a
part of every surgeon's armamentarium. Knowing when to
References
choose the best approach on a patient-to-patient basis and
offering the best technology can be extremely beneficial for 1. Guerron AD, Perez JE, Risoli T Jr, et al. Performance and
future bariatric patients. improvement of the DiaRem score in diabetes remission
prediction: a study with diverse procedure types. Surg
Obes Relat Dis 2020;16:1531-42.
Acknowledgments
2. Maciejewski ML, Arterburn DE, Van Scoyoc L, et al.
Funding: None. Bariatric surgery and long-term durability of weight loss.
JAMA Surg 2016;151:1046-55.
3. Jung MK, Hagen ME, Buchs NC, et al. Robotic bariatric
Footnote
surgery: a general review of the current status. Int J Med
Provenance and Peer Review: This article was commissioned Robot 2017. doi: 10.1002/rcs.1834.
© Digestive Medicine Research. All rights reserved. Dig Med Res 2021;4:35 | http://dx.doi.org/10.21037/dmr-21-6Digestive Medicine Research, 2021 Page 9 of 11
4. American Society for Metabolic and Bariatric Surgery. robotic surgery. Surg Clin North Am 2020;100:461-8.
Estimate of Bariatric Surgery Numbers, 2011-2018. 2018. 19. Veilleux E, Ponce J, Lutfi R. A review of the role of
Available online: https://asmbs.org/resources/estimate-of- robotics in bariatric surgery: finding our future? J
bariatric-surgery-numbers Laparoendosc Adv Surg Tech A 2020;30:36-9.
5. Iranmanesh P, Bajwa KS, Felinski MM, et al. Robotic 20. Clapp B, Liggett E, Jones R, et al. Comparison of robotic
primary and revisional bariatric surgery. Surg Clin North revisional weight loss surgery and laparoscopic revisional
Am 2020;100:417-30. weight loss surgery using the MBSAQIP database. Surg
6. Angrisani L, Santonicola A, Iovino P, et al. IFSO Obes Relat Dis 2019;15:909-19.
Worldwide Survey 2016: primary, endoluminal, and 21. Dykstra MA, Switzer NJ, Sherman V, et al. Roux en
revisional procedures. Obes Surg 2018;28:3783-94. Y gastric bypass: how and why it fails. Surg Curr Res
7. Qiu J, Lundberg PW, Javier Birriel T, et al. Revisional 2014;4:1000165.
bariatric surgery for weight regain and refractory 22. Moon RC, Frommelt A, Teixeira AF, et al. Indications and
complications in a single MBSAQIP accredited center: outcomes of reversal of Roux-en-Y gastric bypass. Surg
what are we dealing with? Obes Surg 2018;28:2789-95. Obes Relat Dis 2015;11:821-6.
8. Brethauer SA, Kothari S, Sudan R, et al. Systematic review 23. Guerron AD, Sudan R. Evaluation and treatment of the
on reoperative bariatric surgery American Society for patient who is regaining weight. In: Patti M, Di Corpo
Metabolic and Bariatric Surgery Revision Task Force. Surg M, Schlottmann F. editors. Foregut surgery: achalasia,
Obes Relat Dis 2014;10:952-72. gastroesophageal reflux disease and obesity. Cham:
9. Park JY, Song D, Kim YJ. Causes and outcomes of Springer Nature Switzerland, 2020:295-307.
revisional bariatric surgery: Initial experience at a single 24. Tran DD, Nwokeabia ID, Purnell S, et al. Revision
center. Ann Surg Treat Res 2014;86:295-301. of Roux-En-Y gastric bypass for weight regain: a
10. Acevedo E, Mazzei M, Zhao H, et al. Outcomes in systematic review of techniques and outcomes. Obes Surg
conventional laparoscopic versus robotic-assisted revisional 2016;26:1627-34.
bariatric surgery: a retrospective, case-controlled study of 25. Ortega CB, Guerron AD, Portenier D. Endoscopic abscess
the MBSAQIP database. Surg Endosc 2020;34:1573-84. septotomy: a less invasive approach for the treatment of
11. Clapp B, Harper B, Dodoo C, et al. Trends in revisional sleeve gastrectomy leaks. J Laparoendosc Adv Surg Tech A
bariatric surgery using the MBSAQIP database 2015-2017. 2018;28:859-63.
Surg Obes Relat Dis 2020;16:908-15. 26. Hallowell PT, Stellato TA, Yao DA, et al. Should bariatric
12. Switzer NJ, Karmali S, Gill RS, et al. Revisional bariatric revisional surgery be avoided secondary to increased
surgery. Surg Clin North Am 2016;96:827-42. morbidity and mortality? Am J Surg 2009;197:391-6.
13. Inabnet WB, Belle SH, Bessler M, et al. Comparison 27. Chaar ME, Lundberg P, Stoltzfus J. Thirty-day outcomes
of 30-day outcomes after non-LapBand primary of sleeve gastrectomy versus Roux-en-Y gastric bypass:
and revisional bariatric surgical procedures from the first report based on Metabolic and Bariatric Surgery
Longitudinal Assessment of Bariatric Surgery study. Surg Accreditation and Quality Improvement Program
Obes Relat Dis 2010;6:22-30. database. Surg Obes Relat Dis 2018;14:545-51.
14. El Chaar M, King K, Pastrana M, et al. Outcomes of 28. Ikramuddin S, Kellogg TA, Leslie DB. Laparoscopic
robotic surgery in revisional bariatric cases: a propensity conversion of vertical banded gastroplasty to a Roux-en-Y
score-matched analysis of the MBSAQIP registry. J Robot gastric bypass. Surg Endosc 2007;21:1927-30.
Surg 2021;15:235-9. 29. Bindal V, Gonzalez-Heredia R, Elli EF. Outcomes of
15. Wittgrove AC, Clark GW, Tremblay LJ. Laparoscopic robot-assisted Roux-en-Y gastric bypass as a reoperative
gastric bypass, Roux-en-Y: preliminary report of five cases. bariatric procedure. Obes Surg 2015;25:1810-5.
Obes Surg 1994;4:353-7. 30. Sweeney JF, Goode SE, Rosemurgy AS. Redo gastric
16. Wilson EB, Sudan R. The evolution of robotic bariatric restriction: a higher risk procedure. Obes Surg
surgery. World J Surg 2013;37:2756-60. 1994;4:244-7.
17. Sudan R, Puri V, Sudan D. Robotically assisted biliary 31. Díaz R, Narvaez A, Welsh L, et al. Endoscopy after
pancreatic diversion with a duodenal switch: a new bariatric surgery: what the endoscopist must know. Rev
technique. Surg Endosc 2007;21:729-33. Med Chil 2020;148:83-92.
18. Jara RD, Guerrón AD, Portenier D. Complications of 32. Lee Bion A, Le Roux Y, Alves A, et al. Bariatric revisional
© Digestive Medicine Research. All rights reserved. Dig Med Res 2021;4:35 | http://dx.doi.org/10.21037/dmr-21-6Page 10 of 11 Digestive Medicine Research, 2021
surgery: what are the challenges for the patient and the 2013;206:145-51.
practitioner? J Visc Surg 2021;158:38-50. 46. Köckerling F. Robotic vs. standard laparoscopic technique
33. Ortega CB, Guerron AD, Yoo JS. The use of fluorescence - what is better? Front Surg 2014;1:15.
angiography during laparoscopic sleeve gastrectomy. JSLS 47. Acevedo E, Mazzei M, Zhao H, et al. Outcomes in
2018;22:e2018.00005. conventional laparoscopic versus robotic-assisted primary
34. Welsh L, Guerron AD. The use of near-infrared bariatric surgery: a retrospective, case–controlled study of
fluorescence in sleeve gastrectomy. In: Aleassa E, El- the MBSAQIP database. Surg Endosc 2020;34:1353-65.
Hayek K. editors. Video atlas of intraoperative applications 48. Beckmann JH, Bernsmeier A, Kersebaum JN, et al. The
of near infrared fluorescence imaging. Cham: Springer impact of robotics in learning Roux-en-Y gastric bypass:
Nature Switzerland, 2020:87-94. a retrospective analysis of 214 laparoscopic and robotic
35. Ma P, Reddy S, Higa KD. Revisional bariatric/metabolic procedures: robotic vs. laparoscopic RYGB. Obes Surg
surgery: what dictates its indications? Curr Atheroscler 2020;30:2403-10.
Rep 2016;18:42. 49. Lainas P, Kassir R, Benois M, et al. Comparative analysis
36. Sudan R, Nguyen NT, Hutter MM, et al. Morbidity, of robotic versus laparoscopic Roux-en-Y gastric bypass in
mortality, and weight loss outcomes after reoperative severely obese patients. J Robot Surg 2021. [Epub ahead of
bariatric surgery in the USA. J Gastrointest Surg print]. doi: 10.1007/s11701-020-01181-5.
2015;19:171-8; discussion 178-9. 50. Economopoulos KP, Theocharidis V, McKenzie TJ, et
37. Sudan R, Kasotakis G, Betof A, et al. Sleeve gastrectomy al. Robotic vs. laparoscopic Roux-En-Y gastric bypass:
strictures: technique for robotic-assisted strictureplasty. a systematic review and meta-analysis. Obes Surg
Surg Obes Relat Dis 2010;6:434-6. 2015;25:2180-9.
38. Himpens J. Strictures after sleeve gastrectomy. In: Gagner 51. Bailey JG, Hayden JA, Davis PJB, et al. Robotic versus
M, Cardoso A, Palermo M, et al. editors. The perfect laparoscopic Roux-en-Y gastric bypass (RYGB) in obese
sleeve gastrectomy. Cham: Springer Nature Switzerland, adults ages 18 to 65 years: a systematic review and
2020:325-35. economic analysis. Surg Endosc. 2014;28:414-26.
39. Chang PC, Tai CM, Hsin MC, et al. Surgical 52. Beckmann JH, Aselmann H, Egberts JH, et al. Robot-
standardization to prevent gastric stenosis after assisted vs laparoscopic gastric bypass: first experiences
laparoscopic sleeve gastrectomy: a case series. Surg Obes with the DaVinci system in bariatric surgery. Chirurg
Relat Dis 2017;13:385-90. 2018;89:612-20.
40. Cadiere GB, Himpens J, Vertruyen M, et al. The world’s 53. Iranmanesh P, Fam J, Nguyen T, et al. Outcomes of
first obesity surgery performed by a surgeon at a distance. primary versus revisional robotically assisted laparoscopic
Obes Surg 1999;9:206-9. Roux-en-Y gastric bypass: a multicenter analysis of ten-
41. Horgan S, Vanuno D. Technical report robots in year experience. Surg Endosc 2020. [Epub ahead of print].
laparoscopic surgery. J Laparoendosc Adv Surg Tech doi: 10.1007/s00464-020-08061-x.
2001;11:415-9. 54. Talamini MA, Chapman S, Horgan S, et al. A prospective
42. Parini U, Fabozzi M, Brachet Contul R, et al. analysis of 211 robotic-assisted surgical procedures. Surg
Laparoscopic gastric bypass performed with the Da Vinci Endosc 2003;17:1521-4.
Intuitive Robotic System: preliminary experience. Surg 55. Bindal V, Bhatia P, Dudeja U, et al. Review of
Endosc 2006;20:1851-7. contemporary role of robotics in bariatric surgery. J Minim
43. Hubens G, Balliu L, Ruppert M, et al. Roux-en-Y gastric Access Surg 2015;11:16-21.
bypass procedure performed with the da Vinci robot 56. Cadière GB, Himpens J, Germay O, et al. Feasibility of
system: is it worth it? Surg Endosc 2008;22:1690-6. robotic laparoscopic surgery: 146 cases. World J Surg
44. Sanchez BR, Mohr CJ, Morton JM, et al. Comparison of 2001;25:1467-77.
totally robotic laparoscopic Roux-en-Y gastric bypass and 57. Sudan R, Desai S. Conversion of laparoscopic adjustable
traditional laparoscopic Roux-en-Y gastric bypass. Surg gastric band to robot-assisted laparoscopic biliopancreatic
Obes Relat Dis 2005;1:549-54. diversion with duodenal switch. Surg Obes Relat Dis
45. Benizri EI, Renaud M, Reibel N, et al. Perioperative 2011;7:546-7.
outcomes after totally robotic gastric bypass: a 58. Protyniak B, Jorden J, Farmer R. Multiquadrant robotic
prospective nonrandomized controlled study. Am J Surg colorectal surgery: the da Vinci Xi vs Si comparison. J
© Digestive Medicine Research. All rights reserved. Dig Med Res 2021;4:35 | http://dx.doi.org/10.21037/dmr-21-6Digestive Medicine Research, 2021 Page 11 of 11
Robot Surg 2018;12:67-74. switch. Ann Surg 2012;255:940-5.
59. Toro JP, Lin E, Patel AD. Review of robotics in foregut 71. Schauer P, Ikramuddin S, Hamad G, et al. The learning
and bariatric surgery. Surg Endosc 2015;29:1-8. curve for laparoscopic Roux-en-Y gastric bypass is 100
60. Esposito C, El Ghoneimi A, Yamataka A, et al. Work- cases. Surg Endosc 2003;17:212-5.
related upper limb musculoskeletal disorders in paediatric 72. Buchs NC, Pugin F, Bucher P, et al. Learning curve for
laparoscopic surgery. A multicenter survey. J Pediatr Surg robot-assisted Roux-en-Y gastric bypass. Surg Endosc
2013;48:1750-6. 2012;26:1116-21.
61. Janki S, Mulder EEAP, IJzermans JNM, et al. Ergonomics 73. Vilallonga R, Fort JM, Gonzalez O, et al. The initial
in the operating room. Surg Endosc 2017;31:2457-66. learning curve for robot-assisted sleeve gastrectomy:
62. Adair MJ, Alharthi S, Ortiz J, et al. Robotic surgery is more a surgeon's experience while introducing the robotic
expensive with similar outcomes in sleeve gastrectomy: technology in a bariatric surgery department. Minim
analysis of the NIS database. Am Surg 2019;85:39-45. Invasive Surg 2012;2012:347131.
63. Hagen ME, Pugin F, Chassot G, et al. Reducing cost of 74. van der Schans EM, Hiep MAJ, Consten ECJ, et al. From
surgery by avoiding complications: the model of robotic Da Vinci Si to Da Vinci Xi: realistic times in draping and
Roux-en-Y gastric bypass. Obes Surg 2012;22:52-61. docking the robot. J Robot Surg 2020;14:835-9.
64. El Chaar M, Gacke J, Ringold S, et al. Cost analysis 75. Senellart P, Saint-Jalmes G, Mfam WS, et al. Laparoscopic
of robotic sleeve gastrectomy (R-SG) compared with versus full robotic Roux-en-Y gastric bypass: retrospective,
laparoscopic sleeve gastrectomy (L-SG) in a single single-center study of the feasibility and short-term results.
academic center: debunking a myth! Surg Obes Relat Dis J Robot Surg 2020;14:291-6.
2019;15:675-9. 76. Beckmann JH, Mehdorn AS, Kersebaum JN, et al. Pros
65. Moon RC, Segura AR, Teixeira AF, et al. Feasibility and and cons of robotic revisional bariatric surgery. Visc Med
safety of robot-assisted bariatric conversions and revisions. 2020;36:238-45.
Surg Obes Relat Dis 2020;16:1080-5. 77. Snyder B, Wilson T, Woodruff V, et al. Robotically
66. Niclauss N, Morel P, Jung MK, et al. A comparison assisted revision of bariatric surgeries is safe and
of the da Vinci Xi vs. the da Vinci Si Surgical System effective to achieve further weight loss. World J Surg
for Roux-En-Y gastric bypass. Langenbecks Arch Surg 2013;37:2569-73.
2019;404:615-20. 78. Gray KD, Moore MD, Elmously A, et al. Perioperative
67. Schraibman V, Macedo ALV, Epstein MG, et al. outcomes of laparoscopic and robotic revisional bariatric
Comparison of the morbidity, weight loss, and relative surgery in a complex patient population. Obes Surg
costs between robotic and laparoscopic sleeve gastrectomy 2018;28:1852-9.
for the treatment of obesity in Brazil. Obes Surg 79. Rebecchi F, Ugliono E, Allaix ME, et al. Robotic Roux-
2014;24:1420-4. en-Y gastric bypass as a revisional bariatric procedure:
68. Cook JA, Ramsay CR, Fayers P. Statistical evaluation a single-center prospective cohort study. Obes Surg
of learning curve effects in surgical trials. Clin Trials 2020;30:11-7.
2004;1:421-7. 80. Nasser H, Munie S, Kindel TL, et al. Comparative analysis
69. Tekkis PP, Senagore AJ, Delaney CP, et al. Evaluation of robotic versus laparoscopic revisional bariatric surgery:
of the learning curve in laparoscopic colorectal surgery: perioperative outcomes from the MBSAQIP database.
comparison of right-sided and left-sided resections. Ann Surg Obes Relat Dis 2020;16:397-405.
Surg 2005;242:83-91. 81. Dreifuss NH, Mangano A, Hassan C, et al. Robotic
70. Sudan R, Bennett KM, Jacobs DO, et al. Multifactorial revisional bariatric surgery: a high-volume center
analysis of the learning curve for robot-assisted experience. Obes Surg 2021;31:1656-63.
laparoscopic biliopancreatic diversion with duodenal
doi: 10.21037/dmr-21-6
Cite this article as: Ponce CJ, Guerron AD, Sudan R. Robot-
assisted revisional bariatric surgery. Dig Med Res 2021;4:35.
© Digestive Medicine Research. All rights reserved. Dig Med Res 2021;4:35 | http://dx.doi.org/10.21037/dmr-21-6You can also read