Risk Assessment of COVID-19 Vaccination Among Childbearing Women
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Mædica - a Journal of Clinical Medicine
MAEDICA – a Journal of Clinical Medicine
2022; 17(2): 449-457
https://doi.org/10.26574/maedica.2022.17.2.449
R eview
Risk Assessment of
COVID-19 Vaccination Among
Childbearing Women
Kyriaki TSIOROUa, Antigoni SARANTAKIa
a
Department of Midwifery, University of West Attica, Egaleo 12243, Athens, Greece
ABSTRACT
Background: Recent studies have shown that pregnant women were more likely to experience COVID-19
complications than non-pregnant women, especially during the third trimester. Thus, the objective of the
present systematic review is to investigate the literature so as to estimate the safety of COVID-19 vaccination
during gestation, regardless of the trimester of pregnancy.
Methods: This systematic review was performed based on PRISMA statement and our search included
four databases: Medline, PubMed, EMBASE and Google Scholar. Original studies were included. The
following search terms were used: coronavirus disease, coronavirus, COVID-19, SARS-CoV-2, vaccine,
vaccination, immunity, immunization, pregnancy, gestation, pregnant women, adverse outcomes, impact,
safety, risk assessment and all possible combinations between them.
Results: The search strategy identified 153 unique items. After the initial screening process, 12 studies
underwent full text review and five studies, which met all inclusion criteria, were ultimately included in our
systematic review. All four studies claim that COVID-19 vaccination does not have a negative influence on
pregnancy and can be beneficial for both the women and their newborns.
Conclusions: More clinical trials assessing pregnancy outcome and the value of COVID‐19 vaccines in
pregnant women are urgently needed. It is vital to determine the most appropriate timing of vaccination
across the three trimesters of pregnancy in order to optimize the balance between vaccine efficacy and
maternal and foetal safety. Future studies should evaluate the maternal–neonatal transfer of SARS‐CoV‐2
antibodies as well as long‐term infant outcome after administration of the COVID‐19 vaccine prenatally.
Keywords: coronavirus disease, coronavirus, COVID-19, SARS-CoV-2,
vaccine, vaccination, immunity, maternal immunization, pregnancy,
gestation, pregnant women, adverse outcomes, impact,
safety, risk assessment.
Address for correspondence:
Dr. Antigoni Sarantaki
Midwifery Department, University of West Attica, Egaleo 12243, Athens-Greece
Land line: +30 2105387403 ORCID ID: https://orcid.org/0000-0003-3316-8566
Email: sarantaki.antigoni@gmail.gr
Article received on the the 23th March 2022 and accepted for publication on the 14th of June 2022
Maedica A Journal of Clinical Medicine, Volume 17, No. 2, 2022 449Covid19 Vaccination and Pregnancy
BACKGROUND trimester. Pregnant women with COVID-19 at-
I
tending or admitted to hospital for any reason
n December 2019, a novel type of viral are less likely to manifest symptoms such as fe-
pneumonia emerged in Wuhan, China, ver, dyspnoea, and myalgia, and are more likely
which was later named coronavirus disease to either be admitted to intensive care or require
(COVID-19) (1). COVID-19 is caused by invasive ventilation than non-pregnant women
the severe acute respiratory syndrome co- of reproductive age. Pre-existing comorbidities,
rona virus 2 (SARS-CoV-2), which can lead to non-white ethnicity, chronic hypertension, pre-
acute respiratory disease. This is associated with existing diabetes, high maternal age, and high
highly non-specific symptoms, including fever, body mass index (BMI) are risk factors for severe
dry cough and dyspnoea (2), which leads to se- COVID-19 in pregnancy. It has been suggested
vere illness and requires admission to hospital for that pregnancies complicated by COVID-19 had
supportive care in around one in five people (3). a higher risk for caesarean delivery, foetal dis-
As of December 2020, nearly 64 million peo- tress, preeclampsia and perinatal death. Also,
ple have been infected with the SARS-CoV-2 pregnant women with COVID-19 are more like-
worldwide, with nearly 1.5 million deaths glo ly to deliver preterm and not only do they have
bally. The impact of this virus has continued to an increased risk of maternal death, but their ba-
overwhelm hospital infrastructure and deman bies are more likely to be admitted to the neona-
ded remodeling of healthcare systems (4). In an tal unit (8).
attempt to stop the spread of COVID-19 pan- Despite this increased risk, and current deli
demic, mass vaccination campaigns commenced beration by the US Food and Drug Administra-
worldwide. The first mRNA vaccine was initiated tion (FDA) on whether to include pregnant wo
and, in July 2020, phases 2/3 of the leading vac- men in clinical trials, pregnant women were not
cine (Pfizer-BioNTech, BNT162b2) began, priori- included in the initial COVID-19 vaccine trials
tizing health care workers and high-risk popu (5). Also, no official recommendation was pu
lations such as elderly people and those with blished to vaccinate pregnant women due to the
comorbidities (5). The BNT162b2 vaccine is lack of evidence regarding safety, since this po
based on a novel approach that utilizes mRNA to pulation was excluded from phase II/III trial. De-
synthesize the spike protein of SARS-CoV-2, spite these recommendations and as a result of a
which is recognized by the immune system (6). sudden increase in morbidity and intensive care
Both Pfizer and Moderna have manufactured unit (ICU) admission in this population, the
mRNA-based vaccines with 95% and 94.1% ef- Israeli Ministry of Health decided not to with-
ficacy against SARS-CoV-2, respectively. Another hold vaccination from pregnant women. Initially,
type of COVID-19 vaccination has been manu- the vaccine was available only to high-risk preg-
factured by AstraZeneca using a viral vector. This nant women; however, several weeks later, the
has also demonstrated an early efficacy and this recommendations have changed and the vac-
next-generation platform has previously been cine was recommended to all pregnant women
utilized for the Ebola vaccine and administered at any gestational age due to the dramatic in-
during pregnancy with an acceptable safety pro- crease in morbidity caused by COVID-19 (9).
file. As a result of this situation affecting the The worldwide COVID-19 pandemic conti
whole planet, approval of these vaccines had a nues to spread, causing substantial morbidity
crucial impact on the ongoing pandemic. How- and mortality. To date, more than 80,000 preg-
ever, there is a lack of data regarding COVID-19 nant women have been infected in the U.S. and
vaccination during pregnancy (4). the estimated global number of pregnant women
According to the US Centers for Disease Con- infected with COVID-19 is likely to reach over
trol and Prevention (CDC), approximately 25% one million this year (10). As a result of this, the
of women of reproductive age hospitalized with World Health Organization (WHO), Centers for
COVID-19 between 1 March and 22 August Disease Control (CDC), the American College of
2020 were pregnant (7). Accumulating evidence Obstetricians and Gynecologists (ACOG) and
indicates that pregnant women are more likely to multiple national immunization advisory com-
experience COVID-19 complications than mittees state that pregnant women, who are part
non-pregnant ones, especially during the third of a high-risk group can be offered vaccination.
450 Maedica A Journal of Clinical Medicine, Volume 17, No. 2, 2022Covid19 Vaccination and Pregnancy
Since early on the pandemic, experts have con- gines and EMBASE, MEDLINE and Google Scho
sistently advocated for inclusion of pregnant lar databases. No language limits were applied
women in trials of therapeutics and vaccines and foreign texts were translated. Studies were
(11), while the German national vaccination included in the present systematic review if they
commission (Ständige Impfkommission, STIKO) had been published within the last two years.
does not recommend vaccination for pregnant Specifically, the initial results were downloaded
and breastfeeding women in general (12). Preg- in October 2021, with updated searches being
nant women now face a more difficult choice performed in January 2022.
around vaccination than the general population
(11). Their trimester, education level, employ- Search strategy
ment status, and previous live births are impor- Appropriate subject headings and special key-
tant determinants for COVID-19 vaccine accep- words were used for each database. These key-
tance among the target population. Regarding words and terms included the following subject
psychosocial predictors, media/social media use, headings: coronavirus disease, coronavirus,
trust in the government, pharmaceutical indus- COVID-19, SARS-CoV-2, vaccine, vaccination,
try, and healthcare professionals, partners, and immunity, maternal immunization, pregnancy,
the risk-benefit ratio were significant promoters gestation, pregnant women, adverse outcomes,
of COVID-19 vaccine acceptance (13). Regard- impact, safety, risk assessment and all possible
less of these factors, the safety of their unborn combination of these terms. Keywords and terms
infant was the primary women’s concern (14). were searched for in the titles, abstracts and full
Crucial data for decision-making and coun- texts of scientific studies.
seling regarding COVID-19 vaccination in preg-
nancy are still limited. Thus, the aim of the pre Eligibility criteria
sent systematic review is to investigate the The present study was limited to articles that
literature so as to estimate the safety of COVID-19 were written in English and representing the
vaccination among pregnant women compared most recent literature. Every recent study that
with unvaccinated pregnant women, regardless gave information about the safety of COVID-19
of the trimester of their pregnancy. q vaccination during pregnancy was included in
the initial study selection. As for the characteris-
tics of trial participants, every pregnant woman
MATERIALS AND METHODS
who was vaccinated against COVID-19 was in-
T he Preferred Reporting Items for Systematic
Reviews and MetaAnalyses (PRISMA) guide-
lines were followed in order to conduct a sys-
cluded in the initial screening process. The fol-
lowing exclusion criteria were used: women
who were either fully vaccinated (any number of
tematic review of the literature (15). doses) before pregnancy or after birth, or had
undocumented COVID-19 disease or vaccine
Information sources status, or had pre-admission COVID-19 virus
The search strategy for the review was primarily disease or positive COVID-19 PCR test, or had a
directed towards finding papers that have been positive PCR test result during admission and
published in journals and conference procee hospitalisation; also, pregnant women were ex-
dings via widely accepted literature search en- cluded from the present study if they had preg-
TABLE 1.
Exclusion
criteria
Maedica A Journal of Clinical Medicine, Volume 17, No. 2, 2022 451Covid19 Vaccination and Pregnancy
TABLE 2. Search terms used in the study
nancies complicated by foetal aneuploidy or ge- COVID-19 vaccination and adverse
netic syndromes. All vaccinated women who maternal-foetal-neonatal outcomes
met the inclusion criteria were eligible and com- A cohort study conducted in the United King-
pared with unvaccinated pregnant women. So, dom included 1368 pregnant women who gave
all studies included both vaccinated for birth at St George’s University Hospitals National
COVID-19 pregnant women and non-vaccina Health Service Foundation Trust, London, be-
ted ones, and differences in adverse maternal-foe- tween March 1, 2020, and July 4, 2021. In total,
tal-neonatal outcomes between these two groups 140 women received at least one dose of the
were estimated. q COVID-19 vaccine and 1188 women did not;
85.7% received their vaccine in the third trimes-
RESULTS ter of pregnancy and 14.3% in the second tri-
mester. In total, 127 (90.7%) received a messen-
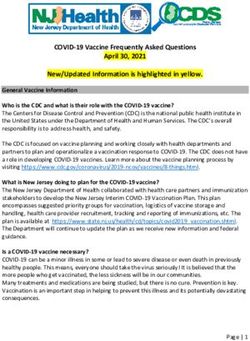
T he search strategy identified 153 unique re-
cords. After the initial screening process and
after having read the titles and abstracts of all
ger RNA vaccine and 13 (9.3%) a viral vector
vaccine. The uptake of COVID-19 vaccination
and its determinants was the primary outcome of
identified studies, 12 studies underwent full text
the study, and perinatal safety outcomes the se
review, of which seven were excluded as they
condary outcomes. We collected data on
did not meet all inclusion criteria: five of them
COVID-19 vaccination uptake, vaccination type,
because they compared pregnant women with
gestational age at vaccination, and maternal
non-pregnant ones and the remaining two stu
characteristics, including age, parity, ethnicity, in-
dies because they included women who were
positive for SARS-CoV-2 during pregnancy. Fi-
nally, five studies were found to meet the inclu-
sion criteria, being ultimately eligible for the sys-
tematic review. They were conducted between
2020 and 2022 and their sample sizes were
ranging from 213 to 15060. These studies were
conducted across several continents, including
three studies in Israel, one in the United King-
dom and one in Finland. Specifically, they were
undertaken at two university-affiliated medical
centres in Jerusalem, Israel [(The Shaare Zedek
Medical Center (SZMC) and the Bikur Holim
Medical Center (BHMC), a large state-mandated
health care organization in Israel], the St George's
University Hospitals National Health Service
Foundation Trust, London, United Kingdom, and
the local Helsinki committee. All studies aimed
to determine the safety of COVID-19 vaccina-
tion during pregnancy. FIGURE 1. Selection process of included studies
452 Maedica A Journal of Clinical Medicine, Volume 17, No. 2, 2022Covid19 Vaccination and Pregnancy
dex of multiple deprivation score, and comor- the second one. Among them, 124 were vacci-
bidities, as well as about perinatal outcomes, in- nated and 202 unvaccinated. Vaccination rate
cluding stillbirth (foetal death at ≥24 gestational increased from 25.5% to 62% within a month.
weeks), preterm birth, foetal and congenital ab- Maternal age, gestational age and number of
normalities and intrapartum complications. The children were similar in both groups. The results
results showed that the rates of adverse pregnan- showed that the rates of pregnancy complica-
cy outcomes of the 133 women who received at tions were similar between the vaccinated and
least one dose of a COVID-19 vaccine were unvaccinated groups (15.8% vs 20.1%). Specifi-
similar to those of the unvaccinated pregnant cally, the following complication rates were seen:
women. Specifically, the rates of the two groups foetal growth restriction (1.5% vs 0.0%), preg-
were as follows: stillbirth (0.0% vs 0.2%), foetal nancy loss up to 13 weeks (0.9 vs 0.8), postpar-
abnormalities (2.2% vs 2.5%), postpartum hae tum bleeding (1.9 vs 5.6) and premature con-
morrhage (9.8% vs 9.0%), caesarean delivery structions (1.9 vs 3.2). Also, the risk of COVID-19
(30.8% vs 34.1%), small foetus for the gestational infection was found to be almost five times lower
age (12.0% vs 12.8%), maternal high-dependen- in the vaccinated group compared to the unvac-
cy unit or intensive care admission (6.0% vs cinated one (10).
4.0%), and neonatal intensive care unit admis- Another retrospective cohort database study,
sion (5.3% vs 5.0%). Intrapartum pyrexia (3.7% which was conducted in Israel, included preg-
vs 1.0%) was significantly increased in the vacci- nant women (>18 years old) who gave birth at
nated group but the borderline statistical signifi- >24 weeks of gestation, between January and
cance was dramatically reduced after excluding April 2021. In total, 712 of them received two
women with antenatal COVID-19 infection (16). doses of a COVID-19 vaccine and they were
Another broader prospective observational compared with 1063 unvaccinated women. The
study, which was conducted in Finland, used on- study objective was to evaluate the influence of
line questionnaires to study both vaccinated and COVID-19 vaccination during the third trimester
unvaccinated pregnant women in order to com- of pregnancy on maternal and neonatal out-
pare the short-term outcomes between the two comes. The overall uptake of one or both vac-
groups during pregnancy. Specifically, they used cines was 40.2%. The results showed the follo
an online Google Forms questionnaire targeting wing adverse maternal outcomes for vaccinated
groups on Facebook and WhatsApp. A second vs non-vaccinated pregnant women: delivery
questionnaire was sent one month after the firstCovid19 Vaccination and Pregnancy TABLE 3. Characteristics of included studies Maternal and foetal antibodies against and -N) was detected during the first 45 days af- SARS-CoV-2 in infected and vaccinated ter infection. In the same period, vaccinated par- uninfected pregnant women ticipants who received the first BNT162b2 dose A multicenter study performed in eight medical showed a rapid IgG response to S1, S2, and RBD centers across Israel included three study groups but not N, resulting in high titter values by day 15 of pregnant women: vaccinated subjects after the first dose. A further rise in IgG was ob- (n = 86), PCR-confirmed SARS-CoV-2-infected served following the second dose. At the time of during pregnancy (n = 65), and unvaccinated delivery, maternal IgG for S1 and RBD were sig- non-infected controls (n = 62). Maternal and nificantly higher in vaccinated women, while IgG foetal blood samples were collected from those for S2 and N were significantly higher in groups prior to delivery and from the umbilical PCR-positive women. Foetal IgG for S2 and N cord following delivery, respectively. Serum IgG were significantly lower in cord blood samples of and IgM titters were measured using the Milli- vaccinated women, while foetal IgG for S1 and plex MAP SARS-CoV-2 Antigen Panel. A gradual RBD did not differ from those of PCR-positive rise in IgG humoral response (anti-S1, -S2, -BD, women. There were no differences between the 454 Maedica A Journal of Clinical Medicine, Volume 17, No. 2, 2022
Covid19 Vaccination and Pregnancy
correlation slopes of the SARS-CoV-2–infected unvaccinated women were as follows:
group and the vaccinated group for any type of SARS-CoV-2-associated hospitalization 0.2% vs
antibodies, suggesting similar placental antibody 0.3%, abortion 1.7% vs 1.6%, intrauterine growth
transfer following SARS-CoV-2 infection and vac- restriction 0.5% vs 0.5%, preeclampsia 0.3% vs
cination (11). 0.3%, maternal death 0% vs 0%, obstetrics pul-
monary embolism 0% vs 0% and preterm birth
Association between receipt of BNT162b2 mRNA (Covid19 Vaccination and Pregnancy
this study supported that mRNA vaccination du perinatal outcomes, but it also may be beneficial
ring pregnancy did not seem to increase the rate and protective for pregnant women. Currently,
of pregnancy complications and it was effective the Royal College of Obstetricians and Gynaeco-
in the prevention of COVID-19 infection (9). logists (RCOG) does not specify any stage of ges-
In the third study, the authors assessed the tation at which to avoid COVID-19 vaccination
impact of SARS-CoV-2 BNT162b2 mRNA vacci- but mentions that pregnant women can choose
nation in the third trimester on maternal and to delay vaccination until 12 weeks of gestation
neonatal outcomes. Women who received both in low-risk situaions: COVID-19 vaccines can be
doses of the vaccine were older and had higher given at any time in pregnancy (12).
rates of previous miscarriages, CD and fertility Another significant factor that should be con-
treatments. Maternal outcomes were compara- sidered is the gestational period in which preg-
ble and the uptake of the COVID-19 vaccine nant women should get vaccinated so as to have
was not associated with poorer maternal out- the greatest protection. Recently, Mithal et al
comes. However, the authors found that the up- found that the antibody transfer ratio seemed to
take of two doses of the vaccine was associated increase with latency from vaccination, sugges
with a higher rate of elective cesarean delivery ting that earlier vaccination may produce greater
and a lower rate of vacuum assisted vaginal de- infant immunity (21). Studies on other vaccina-
livery (VAVD). By contrast, the risk of composite tions supported that placental transfer ratios in-
neonatal outcomes was lower. Thus, even in the creased when there was a longer time between
setting of pre-existing conditions the vaccine maternal infection and delivery (22). However,
would still be recommended, as that study sup- some other studies have found that the Tdap vac-
ported that the uptake of COVID-19 vaccination cine may be more effective when administered
during the third trimester of pregnancy was not during the second trimester of pregnancy (23).
associated with an increased risk of adverse ma- Some side effects have been correlated with
ternal outcomes and lowered the risk of adverse COVID-19 vaccines, such the association be-
neonatal outcomes (17). tween thrombosis and the AstraZeneca vaccine
According to the fourth study, there is a ro- (24). Although these events are rare, the inten-
bust maternal humoral immune response cou- sive coverage of COVID-19 side effects on social
pled with a rise in protective antibodies in the media and other platforms might have had a
foetal circulation as early as 15 days after the first negative influence on decisions of the public re-
BNT162b2 mRNA vaccination. The results fur- garding vaccine safety (25). Pregnant women
ther showed that mid-pregnancy SARS-CoV-2 should be informed of their risk of severe
infection resulted in prolonged maternal and COVID-19-associated illness and the warning
foetal humoral immunity presented at the time signs of severe COVID-19. To reduce the risk of
of delivery (10). acquiring SARS-CoV-2 infection, pregnant wo
In the last study, approximately 69% of preg- men should limit unnecessary interactions with
nant women in the health fund had received the people who might have been exposed to or are
first dose of the vaccine. The benefit from the infected with SARS-CoV-2 as much as possible.
vaccine may be somewhat attenuated among When they go out or interact with others, preg-
this population compared with the general pu nant women should wear a mask, keep social
blic, because pregnant women have been gene distance, avoid people who are not wearing a
rally advised to take extra precautions during the mask, and wash their hands frequently. In addi-
pandemic and to adhere particularly strongly to tion, they should take measures to ensure their
social distancing guidelines, regardless of the general health, including staying up to date with
vaccination status. In this retrospective cohort annual influenza vaccination and prenatal care.
study of pregnant women, BNT162b2 mRNA Providers who care for pregnant women
vaccination was associated with a significantly should be familiar with guidelines for medical
lower risk of SARS-CoV-2 infection compared management of COVID-19, including conside
with no vaccination (18). rations for management of COVID-19 in preg-
All of the above mentioned studies support nancy. As the COVID-19 vaccine is relatively
COVID-19 vaccination during pregnancy, since new, advice on vaccination changes very often.
not only does it not have a negative impact on When vaccination first started in the United
456 Maedica A Journal of Clinical Medicine, Volume 17, No. 2, 2022Covid19 Vaccination and Pregnancy
Kingdom, many pregnant women turned to their nant women are urgently needed. It is crucial to
midwives and obstetricians for advice, but given determine the most appropriate timing of vacci-
the lack of clear guidance at that point, it was nation across all three trimesters in order to opti-
difficult for healthcare professionals to counsel mize the balance between vaccine efficacy and
these women (26). q maternal and foetal safety. Furthermore, with the
aim of providing evidence-based recommenda-
CONCLUSIONS tions, future studies should evaluate maternal-neo-
C OVID-19 vaccination does not seem to lead natal transfer of SARS-CoV-2 antibodies as well
to an increased risk during pregnancy but it as long-term infant outcome after administration
can have a beneficial and a protective impact on of a COVID-19 vaccine during pregnancy. q
pregnant women and their infants. However,
more clinical trials assessing pregnancy outcomes Conflicts of interest: none declared.
and the efficacy of COVID-19 vaccines in preg- Financial support: none declared.
References
1. Hui DS, I Azhar E, Madani TA, et al. The et al. Early exploration of COVID-19 BJOG 2021;129:248-255.
continuing 2019-nCoV epidemic threat of vaccination safety and effectiveness during 18. Goldshtein I, Nevo D, Steinberg DM, et al.
novel coronaviruses to global health – The pregnancy: interim descriptive data from a Association Between BNT162b2 Vaccination
latest 2019 novel coronavirus outbreak in prospective observational study. and Incidence of SARS-CoV-2 Infection in
Wuhan, China. Vaccine 2020;22;39:6535-6538. Pregnant Women.
Int J Infect Dis 2020;91:264-266. 10. Beharier O, Plitman Mayo R, Raz T, et al. JAMA 2021;24;326:728-735.
2. Wang Y, Li X, Ren L, et al. Clinical features of Efficient maternal to neonatal transfer of 19. Theiler RN, Wick M, Mehta R, et al.
patients infected with 2019 novel coronavirus antibodies against SARS-CoV-2 and Pregnancy and birth outcomes after
in Wuhan, China. BNT162b2 mRNA COVID-19 vaccine. SARS-CoV-2 vaccination in pregnancy.
The Lancet 2019;395:10223. J Clin Invest 2021;131:150319. Am J Obstet Gynecol MFM 2021;3:100467 .
3. Lim SM, Allard NL. Devereux J, et al. The 11. Heath PT, Le Doare K, Khalil A. Inclusion of 20. Sutton D, D'Alton M, Zhang Y, et al.
COVID Positive Pathway: a collaboration pregnant women in COVID-19 vaccine COVID-19 vaccine acceptance among
between public health agencies, primary care, development. pregnant, breastfeeding, and nonpregnant
and metropolitan hospitals in Melbourne. Lancet Infect Dis 2020;20:1007-1008. reproductive-aged women.
The Medical Journal of Australia 2022. 12. American College of Obstetricians and Am J Obstet Gynecol MFM 2021;3:100403.
4. Craig AM, Hughes BL, Swamy GK, et al. Gynecologists’ Immunization, I.D., and 21. Mithal LB, Otero S, Shanes ED, et al.
Coronavirus disease. Vaccines in pregnancy. Public Health Preparedness Expert Work Cord blood antibodies following maternal
Am J Obstet Gynecol MFM 2021;3:100295 Group. Vaccinating Pregnant and Lactating coronavirus disease 2019 vaccination during
5. Polack FP, Thomas SJ, Kitchin N, et al. Patients Against COVID-19 2021. pregnancy.
Safety and Efficacy of the BNT162b2 mRNA 13. Riad A, Jouzová A, Üstün B, et al. COVID-19 Am J Obstet Gynecol 2021;225:192-194.
Covid-19 Vaccine. Vaccine Acceptance of Pregnant and 22. Madhi SA, Polack FP, Piedra PA, et al.
N Engl J Med 2020;383:2603-2615. Lactating Women (PLW) in Czechia: An Respiratory syncytial virus vaccination
6. Pardi N, Hogan MJ, Naradikian MS, et al. Analytical Cross-Sectional Study. during pregnancy and effects in infants.
Nucleoside-modified mRNA vaccines induce Int J Environ Res Public Health 2021;18:13373. N Engl J Med 2020;383:426-439 .
potent T follicular helper and germinal center 14. Geoghegan S, Stephens LC, Feemster KA, 23. Eberhardt CS, Blanchard-Rohner G,
B cell responses. et al. This choice does not just affect me. Lemaître B, et al. Maternal immunization
J Exp Med 2018;4;215:1571-1588. Attitudes of pregnant women toward earlier in pregnancy maximizes antibody
7. Delahoy MJ, Whitaker M, O'Halloran A, COVID-19 vaccines: a mixed-methods study. transfer and expected infant seropositivity
et al. Characteristics and maternal and birth Hum Vaccin Immunother 2021;3:3371-3376. against pertussis.
outcomes of hospitalized pregnant women 15. Moher D, Liberati A, Tetzlaf J, et al. Clin Infect Dis 2016;62:829-836.
with laboratory‐confirmed COVID‐19— Preferred reporting items for systematic 24. Bookstein Peretz S, Regev N, Novick L,
COVID‐NET, 13 states, reviews and meta-analyses: et al. Short-term outcome of pregnant
March 1–August 22, 2020. the PRISMA statement. women vaccinated with BNT162b2 mRNA
MMWR Morb Mortal Wkly Rep Thembj 2009;339. COVID-19 vaccine.
2020;25;69:1347-1354. 16. Blakeway H, Prasad S, Kalafat E, et al. Ultrasound Obstet Gynecol 2021;58:450-456.
8. Allotey J, Stallings E, Bonet M, et al. Living COVID-19 vaccination during pregnancy: 25. Solís Arce JS, Warren SS, Meriggi NF, et al.
Systematic Review Consortium. Clinical coverage and safety. COVID-19 vaccine acceptance and hesitancy
manifestations, risk factors, and maternal and Am J Obstet Gynecol 2021;226:236.e1-236. in low- and middle-income countries.
perinatal outcomes of coronavirus disease 17. Rottenstreich M, Sela HY, Rotem R, et al. Nat Med 2021;27:1385-1394.
2019 in pregnancy: living systematic review Covid-19 vaccination during the third 26. Wang EW, Parchem JG, Atmar RL, et al.
and meta-analysis. trimester of pregnancy: rate of vaccination SARS-CoV-2 Vaccination During Pregnancy:
BMJ 2020;1;370:m3320. and maternal and neonatal outcomes, a A Complex Decision.
9. Bleicher I, Kadour-Peero E, Sagi-Dain L, multicentre retrospective cohort study. Open Forum Infect Dis 2021;10;8:ofab180.
Maedica A Journal of Clinical Medicine, Volume 17, No. 2, 2022 457You can also read