Review Peripheral nervous system involvement in systemic lupus erythematosus: a review of the evidence
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Review
Peripheral nervous system involvement in systemic
lupus erythematosus: a review of the evidence
A. Bortoluzzi1, E. Silvagni1, F. Furini1, M. Piga2, M. Govoni1
1
Department of Medical Sciences, Section ABSTRACT ripheral neuropathies (PN) recognises a
of Rheumatology, University of Ferrara In the past years the peripheral nervous non-SLE aetiology (1).
and Azienda Ospedaliero-Universitaria system (PNS) involvement in systemic The 1999 American College of Rheuma-
Sant’Anna, Cona, Ferrara, Italy;
lupus erythematosus (SLE) has received tology (ACR) provided the definitions
2
Rheumatology Unit, University Clinic
and AOU of Cagliari, Italy. little attention despite its potential sig- for 7 peripheral manifestations related
nificant impact. The true prevalence of to SLE (2), but a revisiting of this clas-
Alessandra Bortoluzzi, MD, PhD
Ettore Silvagni, MD PNS in SLE reported in studies is vari- sification including small fibre neuropa-
Federica Furini, MD able and strongly influenced by Ameri- thy has been advised by some Authors
Matteo Piga, MD, PhD can College of Rheumatology (ACR) (1, 3). This review will focus on epide-
Marcello Govoni, MD case definition that includes seven PNS miology, pathogenesis, diagnosis, clini-
Please address correspondence to: manifestations (acute inflammatory de- cal features and treatment of peripheral
Dr Alessandra Bortoluzzi, myelinating polyradiculoneuropathy, neuropsychiatric SLE (NPSLE).
Dipartmento di Scienze Mediche, autonomic disorder, mononeuropathy,
Sezione di Reumatologia, myasthenia gravis, cranial neuropa- Epidemiology
Azienda Ospedaliero-Universitaria
Sant’Anna di Ferrara,
thy, plexopathy and polyneuropathy). The true prevalence of PNS involve-
Via Aldo Moro 8, Other peripheral manifestations, such ment in SLE reported in studies is high-
44124 Cona, Italy. as chronic inflammatory demyelinating ly variable and strongly influenced by
E-mail: brtlsn1@unife.it polyradiculoneuropathy and small fibre ACR nomenclature. The case definition
Received on October 9, 2017; accepted neuropathy, not included in the ACR included acute inflammatory demyeli-
in revised form on February 28, 2018. nomenclature, have not been well char- nating polyradiculoneuropathy (Guil-
Clin Exp Rheumatol 2019; 37: 146-155. acterised in SLE. The aim of this review lain-Barrè syndrome, GBS), autonomic
© Copyright Clinical and is to focus on epidemiology, pathogen- disorder, single/multiple mononeuropa-
Experimental Rheumatology 2019. esis, diagnosis and clinical features thy, myasthenia gravis (MG), cranial
of all possible different expressions of neuropathy, plexopathy and polyneu-
Key words: peripheral nervous PNS involvement in SLE, with the final ropathy (2).
system, neuropsychiatric lupus objective to profile the patient’s clinical The importance of the PNS involve-
erythematosus, cranial neuropathy, characteristics. ment was clearly recognised once again
myasthenia gravis, polyneuropathy, in the new 2012 Systemic Lupus Inter-
small fibre neuropathy Introduction national Collaborating Clinics (SLICC)
Systemic lupus erythematosus (SLE) classification criteria for SLE (4); here
is an autoimmune-mediated disease, the neurologic criterion was substan-
characterised by the production of au- tially implemented by including a larg-
toantibodies and immune-complexes er number of neurologic manifestations
deposition that can affect multiple or- of SLE related to a PNS involvement -
gans and systems including both the like mononeuritis multiplex, peripheral
central (CNS) and peripheral nervous or cranial neuropathy – not included
system (PNS). in the original 1997 revised classifica-
In past decades many studies have evalu- tion criteria for lupus (5). Most of the
ated the CNS manifestations, while only studies that evaluated the NP involve-
a limited number focused on the PNS ment in SLE, applying the 1999 ACR
ones. To date, little is known about the nomenclature, are typically retrospec-
actual prevalence and the demographic tive cohort and consider together the
and specific immunological factors of peripheral and central involvement (4).
peripheral neuro-lupus. In addition the The prevalence of PNS complications
final attribution of PNS involvement to ranged between 2 and 10%, with a high-
SLE is a relevant and challenging clini- er predominance of polyneuropathies
Competing interests: none declared. cal issue because up to one third of pe- (2–3%) and mononeuropathies (single
146 Clinical and Experimental Rheumatology 2019PNS involvement in SLE / A. Bortoluzzi et al. or multiple: 0.5–1%), compared to rare Recent advances in pathogenesis tions of molecules released by nocic- or unusual events like GBS (0.1%), of PNS involvement in SLE eptors and distinct afferent stimulation MG (0.1%) and plexopathy (
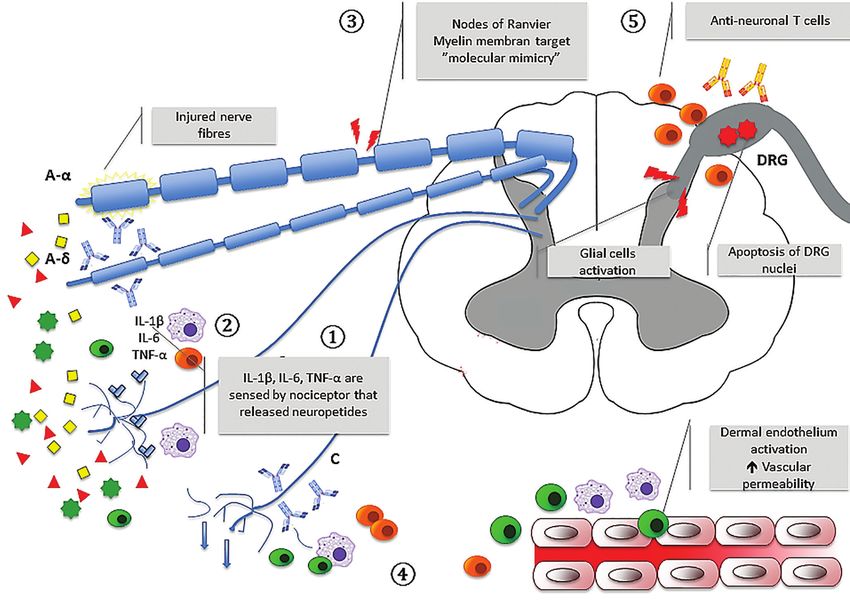
PNS involvement in SLE / A. Bortoluzzi et al. Fig. 1. Pathogenesis of peripheral nervous system involvement in systemic lupus erythematosus. Different pathogenetic mechanisms could explain large and small fibre neuropathy. The figure illustrates some emerging key concepts. Neurogenic inflammation: (1) In humans, an increased number of proinflammatory cytokines (IL-1-Beta, IL-6, TNF-alpha) is reported in nerve biopsy from patients with painful neuropathies, especially in patients with vasculitic neuropathies. IL-1-Beta, IL-6, TNF-alpha are directly sensed by nociceptors which express the cognate receptors. Nociceptors can release different neuropeptides such as calcitonin gene-related protein and substance P resulting in vasodilatation and increasing vascular permeability. (2) The mediators released from sensory neurons in periphery directly attract and activate immune in- nate cells (dendritic, mast cells) and adaptative immune cells such as T lymphocytes. Autoantibodies: (3) Nodes of Ranvier may be, interestingly, a vulnerable target for autoimmunity due to the intrinsically elevated number of potential antigens and because of the crucial permeability of blood nerve barrier in nodal and juxtaparanodal structures. A process of molecular mimicry may act as the starting motif to target different specific antigens within nerve structure. Mechanisms implicated in small fibre neuropathy (4) Length-dependent small fibre neuropathy: immunoglobulin deposit on the surface of nerves and the activation of dermal vascular endothelium lead to decreased intraepidermal nerve fibre density of unmyelinated fibres. (5) Non-length-dependent gan- glionopathy: the hypothesised pathogenetic mechanisms include the presence of anti DRG-antibodies, apoptosis of the DRG nucleus or axons and reduced apoptosis of anti-neuronal directed T-cell. DRG, dorsal root ganglion; IL-1β, interleukin 1-beta; IL-6, interleukin-6; TNF-α, tumour necrosis factor alpha. trates in polyneuropathies (23) and a Risk factors and attribution for whole PNS events judged not-SLE re- vasculitis-associated pattern of ischae- PNS involvement in SLE lated. Mononeuritis multiplex was most mic and inflammatory damage in vas- In SLE, the correct attribution of NP likely to be SLE-related in agreement culitic neuropathy (24-26). events is of outstanding importance for with the new classification criteria for In SLE patients, sparse histopathologic the patient’s care and also to define both SLE that deemed this kind of manifes- data reported chronic axonal degenera- pathogenic mechanisms and therapeutic tation to be very specific. tion with reduction of myelinated and de- interventions (28-30). Oomatia report- Among clinical and demographic data, myelinated fibre density, demyelination, ed that from a total of 123 SLE patients comparing patients with and without inflammatory changes with mononuclear with PNS manifestations, 33.3% were PNS involvement, an older age at onset infiltration among nerve fibres, immune not attributable to SLE, due to other of the disease and a higher SLICC/ACR complexes deposition and vasculitis with non-SLE aetiologies like infectious or Damage Index (SDI) are traits that are thickening of the vessel wall, cellular in- metabolic (1). Florica et al. (10) report- associated with PNS involvement at- filtration and intimal changes (27). ed a similar result with 39.6% of the tributed to SLE (1, 10). 148 Clinical and Experimental Rheumatology 2019
PNS involvement in SLE / A. Bortoluzzi et al.
Polyneuropathy Table I. Classification of large fibre neuropathy.
Large fibre neuropathy are divided by
Classification of large fibre neuropathy
electrodiagnostic studies into axonal or
demyelinating neuropathies, and fuction- By damaged structure By functional involvement By pattern of trunk nerve involvement
ally in sensory, motor or sensorimotor - axonal - sensory - polyneuropathy
(1). The pattern of trunk nerve involve- - demyelinating - motor - multineuropathy (multiple mononeuropathy)
ment defines the distinction in poli-, mul- - sensorimotor - mononeuropathy
ti- and mononeuropathy (Table I).
Polyneuropathy is the most frequent up, which suggested adopting a mainte- or more nerves could be concomitantly
PNS manifestation in SLE, inducing nance therapy. affected (41). The involvement of the
altered sensitivity, atrophic changes or medial longitudinal fascicle is also de-
pain. Muscle strength is typically in- Cranial neuropathy scribed in SLE, resulting in internuclear
volved later in the process, with weak- Optic neuropathy (II cranial nerve - ophthalmoplegia (42). VI CN is the most
ness of toes extension, ankle dorsiflex- CN), the most frequent cranial neuropa- frequently affected among oculomotors
ion (enhanced by walking on heels) and thy described in SLE (about 1% in SLE (40). A micro-thrombotic vasculopathy
altered proprioception causing frequent cohorts), will not be discussed because related to antiphospholipid antibodies
falls. The most common form in SLE it is part of CNS (as well as the olfac- has been advocated as a possible patho-
is a symmetric distal axonal sensory or tory nerve). genetic mechanism; viral infections be-
sensorimotor neuropathy. The axonal Most common cranial neuropathies are, fore developing clinical signs are some-
forms typically follow a classic stock- in order of frequency, the eighth, the times reported. An overall good clinical
ing-glove pattern of distribution with a oculomotor (third, fourth and sixth), outcome for CN neuropathies has been
slow proximal spreading. the fifth and seventh nerve pairs (33). reported (40). Treatment protocols re-
The diagnosis of polyneuropathy im- In the Florica cohort 12.5% (26 pts) quire glucocorticoids alone (at 1 mg/kg
plies a combination of clinical symp- of the PNS-SLE were found to have a per day of prednisone equivalents) or
toms, signs and electrodiagnostic find- concomitant cranial neuropathy, with a in combination with cyclophosphamide
ings. Nerve conduction studies (NCS) rare involvement of III, V, VI and VII in refractory cases (34, 43) (Table IV).
and needle electromyography are essen- CN (10), data confirmed by Xianbin et Relapses may occur and a maintenance
tial to make a correct differential diag- al. (12.7% of PNS manifestations) (8). therapy is useful, using long-term corti-
nosis and to monitor response to therapy. Hanly et al. reported a prevalence rang- costeroids and chronic immunosuppres-
In axonal forms, treatment guidelines ing from 4.3 to 7.4% of all NP events sant regimens; anticoagulation can be
suggest to use neurotrophic agents (tri- (38). Brey et al. described a 2.2% over- considered in antiphospholipid-positive
cyclic antidepressants, serotonin-norep- all prevalence in their SLE population patients (33, 41) (Table IV). PEX is a
inephrine reuptake inhibitors, as dulox- (39), with the predominance of trigemi- useful therapeutic approach in progres-
etine and venlafaxine and anticonvulsi- nal involvement. sive palsy (44). A number of retrospec-
vants such as gabapentin and pregabalin The differential diagnosis of cranial tive studies described several cases of
(31, 32)) and glucocorticoids (33). Car- neuropathies includes Lyme disease, spontaneous recovery of oculomotor
bamazepine is used in refractory cases. neuro-sarcoidosis, MG, and mid-brain involvement (45).
The association of immunosuppressant or base-of-skull pathologic processes
therapies (azathioprine, mycophenolate (2); diagnostic workup for CN involve- Mononeuropathy single/multiple
mofetil, cyclophosphamide) should be ment in SLE involves electrodiag- Non-compression mononeuropathy is
considered in severe forms (34) while nostic studies (electromyography and a vasculitic neuropathy characterised
high dose intravenous immunoglobu- electroneurography). Blink reflex can by the damage in one or more (multi-
lins (IVIG), plasma exchange (PEX), or be examined to investigate functional plex forms) nerves. Vasculitic insult in-
rituximab are reserved to selected and integrity of V and VII CN; Hess chart volves vasa nervorum with subsequent
refractory cases (35) (Table IV). The could help in distinguishing the correct Wallerian degeneration of nerve fibres
only controlled clinical trial designed oculomotor involvement. secondary to ischaemic infarction due
in SLE patients for severe neuropathy VIII is the most frequently affected CN to occlusion of blood vessels caused by
showed that intravenous cyclophos- in SLE, resulting in both symptomatic leukocytoclastic vasculitis. Endoneuri-
phamide treatment was more effective and asymptomatic sensorineural hear- al immune complex deposition in sural
than pulses of steroids (36), but only 7 ing defects (22). Deafness or sudden nerve biopsy in SLE neuropathy patient
cases of polyneuropathy were enrolled. sensorineural hearing loss, dtziness and would suggest their possible role in the
Stojanovich confirmed the efficacy of tinnitus are the most common symp- demyelinating process and axonal dam-
a low-dose regimen of cyclophospha- toms (40). age (27). A positive association with
mide versus methylprednisolone in PNS Oculomotor involvement causes di- antiphospholipid antibody and cryoglo-
manifestations (37), but more than 50% plopia or blurred vision (nausea and bulinaemia is also suggested (17, 46).
of the patients, previously improved, vomiting could be present) with pupil Clinically mononeuropathy can mani-
had a subsequent relapse during follow- diameter alterations in some cases; one fest as “wrist drop” in case of radial
Clinical and Experimental Rheumatology 2019 149PNS involvement in SLE / A. Bortoluzzi et al.
involvement or “foot drop” in presence occasionally described in association tion and debris-laden macrophages in
of sciatic or peroneal involvement, but with SLE (55–57). Diagnostic criteria endoneurium are enhanced (61). Elec-
manifestations can also occur in other include supportive evidence by nerve trophysiological studies (including sen-
nerves like tibial, ulnar and medial conduction block, slowing of conduc- sory and motor nerve conduction stud-
(47). Electrophysiology usually shows tion velocity and prolongation of distal ies), spine magnetic resonance imaging
a typical focal or multifocal pattern of latency. Nerve conduction abnormali- (MRI) and CSF analysis support the
involvement. As suggested by EULAR ties may be subtle in early stages and diagnosis, while nerve biopsy is useful
recommendations for the management may need repetition (2). Given the in selected cases (59).
of NPLSE, specific therapy depends usual post-infectious nature of the dis- Randomised controlled trials demon-
upon the nature of the underlying patho- ease, the first therapeutic approach for strated the effectiveness of glucocorti-
genetic process (33). The reduction of the GBS involves the use of high dose coids, IVIG, and plasmapheresis in up
inflammation around the epineurium is IVIG or PEX, in addition to respira- to two-thirds of CIDP (62, 63), but stud-
the primary goal of treatment. Induc- tory and cardio-respiratory supporting ies are needed to characterise prelimi-
tion therapy includes systemic gluco- measures. Otherwise, steroids and im- nary patterns of response to treatment.
corticoids, IV cyclophosphamide (48); munosuppressants like cyclophospha- IVIG represent the first-line treatment;
in refractory cases, rituximab, IVIG, mide could be an important treatment in IVIG-resistant diseases a response to
PEX, azathioprine or mycophenolate option in lupus-related GBS (58). PEX was found in 66% of cases and to
mofetil as a maintenance therapy have Chronic inflammatory demyelinating glucocorticoids in 58% of cases (64).
been used (49) (Table IV). polyradiculoneuropathy (CIDP) is an Among 6 patients with CIDP second-
immune-mediated non-length-depend- ary to SLE (65), Vina et al. found an
Inflammatory demyelinating ent neuropathy (prevalence of 1–7 per improvement greater than 50% (in sub-
poliardiculoneuropathy 100,000 people) characterised by pro- jective report of everyday function and
Acute inflammatory demyelinating gressive symmetric or asymmetric de- objective neurological examination) in
polyradiculoneuropathy or GBS is an myelinating polyneuropathy (although patients treated with IVIG within 1 year
acute, inflammatory and demyelinat- axonal variants could be present) and from onset of symptoms. Poor IVIG-
ing syndrome of spinal root, peripheral albumin-cytologic dissociation on cer- responders were patients with a later
and occasionally cranial nerves (2). ebro-spinal fluid (CSF) examination. IVIG course and atypical clinical pat-
In a retrospective study of 1,100 GBS It was often thought to be the chronic tern. It is reasonable that a more aggres-
patients, SLE was diagnosed only in 7 counterpart of GBS (59). The ACR case sive treatment approach could result in
cases (50). The prevalence of GBS in definition for NPSLE does not include improving the autoimmune processes
SLE patients ranges between 0.6–1.7% this condition although SLE could be on the basis of CIDP. In refractory dis-
of cases, mainly during the course of an autoimmune cause of CIDP, as well eases or to reduce the need for IVIG,
the disease. The pathogenesis of GBS as infections (Hepatitis B or C, HIV), immunosuppressants in association to
as a manifestation of active SLE is not inflammatory diseases (connective tis- steroids (59) and even rituximab can be
clearly defined and both cell-mediated sue diseases, inflammatory bowel dis- effective (66) (Table IV). No evidence-
and humoral processes are implicated. eases, thyrotoxicosis) and other het- based guidelines are available for main-
The co-occurrence with infections, fre- erogeneous conditions (lymphomas, tenance therapy that would be advisable
quently observed in immunosuppressed diabetes mellitus, transplants, inherited for the majority of patients.
patients, could represent another rel- neuropathies, nephrotic syndrome).
evant pathogenetic factor. Autoantibod- Compared to GBS, CIDP rarely in- Small fibre neuropathy
ies reacting with specific neural tissues, volves bulbar tract or autonomic system Small fibre neuropathy is frequently
such as myelin components, may be and presents maximal symptoms in usu- associated with painful burning sen-
produced as part of the broad spectrum ally more than eight weeks, while GBS sations; however, its association with
of SLE- associated autoantibodies; re- reaches nadir within four weeks from SLE is not always defined, and this con-
cently dysfunctional autophagy, a pro- the onset. Autoantibodies to Schwann dition was not included in 1999 ACR
cess linked with SLE pathogenesis and cells and myelin sheath proteins are part case definitions for NPSLE.
type I – Interferon production (51–53), of the pathogenetic mechanism in CIDP Causes of small fibre neuropathy are
is under investigation in animal models (17); autoantigens are recognised by a multiple and heterogeneous (Table II)
mimicking GBS (54). GBS is charac- phenomenon of molecular mimicry, as and no further clinical characteristics
terised by rapidly progressive mono- well as in GBS (26) and neurofascin, distinguish SLE patients. Half of the
phasic course (PNS involvement in SLE / A. Bortoluzzi et al.
Table II. Causes of small fibre neuropathy (adapted from Themistocleous et al. (67)).
Primary Secondary Conditions related / matters of debate
idiopathic small fibre neuropathy impaired glucose tolerance, diabetes mellitus complex regional pain syndrome
burning mouth syndrome infections (HIV, hepatitis C, influenza) subtypes of fibromyalgia
genetic forms (Fabry’s disease, Tangier’s, drugs (antiretrovirals, Metronidazole, chronic pain syndrome
NAv1.7 mutations, NAv1.8 mutations, Nitrofurantoin, Linezolid, Bortezomib,
familial amyloid polyneuropathy) Flecainide, statins, alcohol, vitamin B6 toxicity,
TNF-alpha inhibitors)
autoimmune diseases (coeliac disease, painful channelopathies (inherited
sarcoidosis, rheumatoid arthritis, SLE, Sjögren’s erythromelalgia; paroxysmal extreme pain
syndrome, vasculitis, inflammatory bowel disease) disorder; familial episodic pain syndrome)
chronic kidney disease restless leg syndrome
vitamin B12 deficiency neurodegenerative conditions
dyslipidaemia, metabolic syndrome
hypothyroidism
paraneoplastic syndromes
monoclonal gammopathy/amyloidosis
Table III. A purpose of diagnostic criteria for small fibre neuropathy in diabetes mellitus (69).
Possible Probable Definite
presence of length-dependent symptoms presence of length-dependent symptoms, presence of length-dependent symptoms,
and/or clinical signs of small fibre damage clinical signs of small fibre damage, clinical signs of small fibre damage, normal
and normal sural NCS sural NCS, and altered IENF density at the
ankle and/or abnormal quantitative sensory
testing thermal thresholds at the foot
NCS: nerve conduction study; IENF: intraepidermal nerve fibre.
bre involvement or autonomic nerv- PN when electrodiagnostic studies are degeneration in the area of maximal
ous system dysfunction and to confirm normal (33). More recently, corneal vulnerability to different causes. In the
positive signs as allodynia, hyperal- confocal microscopy (CCM) has been second group neuropathic pain occured
gesia, hyperpathia or the presence of purposed as a diagnostic non-invasive with a patchy, asymmetric or proximal
coexisting autonomic impairment with tool for early nerve damage in diabetic pattern. In skin biopsy, the proximal leg
atrophy, dryness or oedema of the sur- patients (72). was unorthodoxically more affected
rounding area of the skin. Standard di- Recent studies have suggested small than the distal leg, suggesting a dif-
agnostic methods include Quantitative fibre neuropathies occur in SLE pa- ferent nervous target, which involves
Sensory Testing (QST) and skin biopsy tients more frequently than other PNS DRG (75, 76).
(Table III) (68, 69). manifestations described in ACR case Pathogenetic mechanisms of this selec-
QST in a non-invasive method that ex- definitions (1), but available data are tive damage to A-delta and C-fibres are
plores the function of unmyelinated and scarce. still largely unexplained; a specific im-
thinly myelynated afferent nerves as- Goransson et al. (73) described a prev- munoglobulin deposit (peripherin-IgG
sessing responses to pressure, pinprick, alence of 13% of SLE patients with (77) and antisulfatide antibodies (78))
vibration, heat; it requires the active biopsy-proven small fibre neuropathy. on the surface of nerves or an activa-
collaboration of the subject and can- Tseng et al. found a reduction in IEN- tion of dermal vascular endothelium are
not differentiate between central and FD in 82% of SLE patients, compared counted, resulting in vulnerability or
peripheral causes of sensory loss (70). to healthy controls (74). Oomatia et al. apoptosis of nerves (79). Elevated pro-
Skin biopsy assesses morphological al- characterised 5.9% of SLE patients with inflammatory cytokine-mediated dam-
terations, investigating intraepidermal PN in their John Hopkins SLE cohort age and microglial-activation have also
nerve fibre density (IENFD), showing and small fibre neuropathies occurred been advocated (80, 81) (Fig. 1).
reduction in number of fibres crossing in 17.1% of cases, 6.1% length-depend- In non-length-dependent ganglionopa-
the dermal-epidermal junction, but also ent and 11% non-length-dependent thy anti DRG-antibodies, apoptosis of
alterations in structure of fibres and ax- (1). In the first group neuropathic pain the DRG nucleus or axons or reduced
onal swelling. So far the quantification developed in the distal feet, with a apoptosis of anti-neuronal directed T-
of IENFD is the efficient technique to “stocking-glove” distribution. Skin bi- cells have been described (82), (Fig.
prove diagnosis, showing a decreased opsy showed decreased intraepidermal 1). Birnbaum evaluated MRI morphol-
IENFD (71) and it is indicated in di- nerve fibre density of unmyelinated ogy of DRG in small fibre neuropathy,
agnostic work-up of SLE patients with fibres suggesting a distal-most axonal Sjögren’s syndrome and underlined
Clinical and Experimental Rheumatology 2019 151PNS involvement in SLE / A. Bortoluzzi et al.
Table IV. Summary of treatment options available for peripheral nervous system involvement in systemic lupus erythematosus.
PNS manifestation First-line treatment approach Treatment of refractory cases
polyneuropathy neurotrophic agents (tricyclic carbamazepine
antidepressants, SNRI (duloxetine, venlafaxine), high dose IVIG, PEX, Rituximab (33,35)
anticonvulsivants (gabapentin, pregabalin)) (31,32)
glucocorticoids (1 mg/kg/day of prednisone equivalent) (33)
severe forms: immunosuppressants (azathioprine,
mycophenolate mofetil, cyclophosphamide) (33,34,36,37)
cranial neuropathy glucocorticoids (1 mg/kg/day of prednisone equivalent) cyclophosphamide (34,43)
with long-term dosage reduction (33) immunosuppressants as maintenance treatment (33)
spontaneous recovery possible for oculomotor anticoagulation in presence of aPL-ab (33,41)
involvement (45) PEX (44)
mononeuropathy single/multiple systemic glucocorticoids (1-2 mg/kg/day of prednisone Rituximab, IVIG, PEX (49,92)
equivalent or pulses of methylprednisolone 500/1000 mg mycophenolate mofetil (49)
for 3-5 days with long-term dosage reduction) (33,48,49) azathioprine (49)
IV cyclophosphamide (33,48,49)
acute inflammatory demyelinating high dose IVIG (58,92) glucocorticoids (1 mg/kg/day of prednisone
polyradiculoneuropathy (GBS) PEX (58) equivalent or pulses of methylprednisolone
cardio-respiratory supporting measures 1000 mg for 3 days) and immunosuppressants –
cyclophosphamide (58)
chronic inflammatory demyelinating IVIG (62,64,65,71,92) immunosuppressants in association with
polyradiculoneuropathy (CIDP) PEX (59,63) glucocorticoids (59)
glucorticoids (1 mg/kg/day of prednisone Rituximab (66)
equivalent) (59,62,64,65)
small fibre neuropathy neurotrophic agents (tricyclic antidepressants, immunosuppressants (80)
SNRI (duloxetine, venlafaxine), anticonvulsivants IVIG (67,84)
(gabapentin, pregabalin)) (80) psychological support (67)
topical anaesthetics (67)
analgesics
autonomic nervous system dysfunction specific symptomatic therapy (88) IVIG, PEX (88)
immunosuppressants (89)
myasthenia gravis symptomatic treatments (anticholinesterase Rituximab, eculizumab, cyclophosphamide,
agents, cardio-respiratory supporting measures). IVIG, PEX (91,92)
glucocorticoids (1-1.5 mg/kg/day of prednisone
equivalent or pulses of 500-2000 mg
of methylprednisolone for 3-5 days or 10-20
mg/day of prednisone equivalent followed by
dosage increase of 5 mg/day per week until 1
mg/kg/day) plus azathioprine (91).
other immunosuppressants (cyclosporine A,
methotrexate, micophenolate mofetil, tacrolimus) (91).
plexopathy glucocorticoids? (94)
PNS: peripheral nervous system; SNRI: serotonin-norepinephrine reuptake inhibitors; IVIG: intravenous immunoglobulins; PEX: plasma exchange;
aPL-ab: antiphospholipid antibodies; IV: intravenous; GBS: Guillain-Barrè syndrome; CIDP: chronic inflammatory demyelinating polyradiculoneuropathy.
pathological alterations of ganglions, pathic small fibre neuropathy (75, 83, SLE patients (85, 86), maybe because
describing an increase in their size, 84). Prognosis is characterised by slow symptoms of autonomic dysfunction
T2-signal and gadolinium-enhance- progression of the disease with a chron- are non-specific and vary remarkably;
ment (83). ic pain condition. moreover, tests to detect autonomic
Medication includes antidepressants, dysfunction are not routinely employed
anticonvulsants, topical anaesthetics Rare syndromes in clinical practice. Criteria for diag-
and analgesics. Poor data are available Autonomic nervous system nosis of ANS are provided in glossary
for steroidal or immunomodulatory dysfunction definition in British Isles Lupus As-
therapeutical options in autoimmune There are still controversies concern- sessment Group (BILAG) index and
diseases and are limited to case reports. ing the precise prevalence of autonomic by 1999 ACR classification (2, 87).
Recently, a randomised controlled trial nervous system (ANS) dysfunction, The general management of ANS dys-
with IVIG has been designed in idio- variously reported in 6 to 93% of all function depends on the clinical sever-
152 Clinical and Experimental Rheumatology 2019PNS involvement in SLE / A. Bortoluzzi et al.
ity. Autonomic neuropathies usually Conclusions large cohort from a single centre. Autoimmun
Rev 2017; 16: 750-5.
require specific symptomatic therapy. In this review, we have examined the
10. FLORICA B, AGHDASSI E, SU J, GLADMAN
If an autoimmune cause of the auto- peripheral involvement in SLE, from DD, UROWITZ MB, FORTIN PR: Peripheral
nomic neuropathy is found or strongly epidemiological data to pathogenetic neuropathy in patients with systemic lupus
suspected, immunomodulatory therapy new evidence and the patient’s clini- erythematosus. Semin Arthritis Rheum 2011;
41: 203-11.
may be considered. IVIG, plasmapher- cal profile and treatment. Although to a 11. BRAIN SD, WILLIAMS TJ: Interactions be-
esis (88) and oral immunosuppressant lesser extent than CNS, PNS involve- tween the tachykinins and calcitonin gene-
medications have been used success- ment is a well recognised but also un- related peptide lead to the modulation of
fully (89). derestimated manifestation of NPSLE. oedema formation and blood flow in rat skin.
Br J Pharmacol 1989; 97: 77-82.
Damage accrual and higher age are 12. HUGHES SR, WILLIAMS TJ, BRAIN SD: Evi-
Myasthenia gravis potential risk factors associated to PNS dence that endogenous nitric oxide modu-
The coexistence of MG is rare in SLE involvement. Peripheral polyneuropa- lates oedema formation induced by sub-
but is not coincidental and the preva- thy is the most common manifestation stance P. Eur J Pharmacol 1990; 191: 481-4.
13. LINDENLAUB T, SOMMER C: Cytokines in
lence of MG in SLE is estimated at throughout the studies, followed by sural nerve biopsies from inflammatory and
1.3%, which is higher than the 0.02% cranial nerve neuropathy (7). GBS and non-inflammatory neuropathies. Acta Neuro-
prevalence of MG in general population plexopathy are extremely rare in SLE pathol (Berl). 2003; 105: 593-602.
(43). In most patients MG appeared first suggesting that they may reflect the 14. SKAPER SD: Nerve growth factor: a neuroim-
mune crosstalk mediator for all seasons. Im-
and atypical presentations are reported manifestation of a distinct and coinci- munology 2017; 151: 1-15.
(90). MG expected both symptomatic dental neurologic syndrome rather than 15. KOHR D, TSCHERNATSCH M, SCHMITZ K et
treatment and immunotherapy. Corti- a SLE related manifestation (1, 2). al.: Autoantibodies in complex regional pain
syndrome bind to a differentiation-dependent
costeroids and azathioprine are consid-
neuronal surface autoantigen. Pain 2009;
ered the first-line treatment, second line References 143: 246-51.
1. OOMATIA A, FANG H, PETRI M, BIRNBAUM
immunosuppressive drugs are cyclo- J: Peripheral neuropathies in systemic lupus
16. CHIU IM, von HEHN CA, WOOLF CJ: Neuro-
sporine A, methotrexate, micophenolate erythematosus: clinical features, disease as-
genic inflammation and the peripheral nerv-
ous system in host defense and immunopa-
mofetil and tacrolimus (91). In severe sociations, and immunologic characteristics
thology. Nat Neurosci 2012; 15: 1063-7.
and refractory cases, rituximab, eculi- evaluated over a twenty-five-year study pe-
riod. Arthritis Rheumatol 2014; 66: 1000-9. 17. KLEIN CJ: Autoimmune-mediated peripheral
zumab, cyclophosphamide are used as 2. The American College of Rheumatology neuropathies and autoimmune pain. Handb
well as IVIG and PEX for prevention nomenclature and case definitions for neu- Clin Neurol 2016; 133: 417-46.
18. ANG CW, JACOBS BC, LAMAN JD: The Guil-
and therapy of myasthenic crisis (91, ropsychiatric lupus syndromes. Arthritis
lain-Barré syndrome: a true case of molecular
Rheum 1999; 42: 599-608.
92). Hydroxycloroquine is considered mimicry. Trends Immunol 2004; 25: 61-6.
3. BORTOLUZZI A, SCIRÈ CA, GOVONI M:
safe in MG patients with SLE but avail- Comment on: Diagnosing and attributing 19. SHAHRIZAILA N, KOKUBUN N, SAWAI S
able data are controversial (93). neuropsychiatric events to systemic lupus er- et al.: Antibodies to single glycolipids and
ythematosus: time to untie the Gordian knot? glycolipid complexes in Guillain-Barré syn-
Rheumatology (Oxford) 2017; 56: 856-7. drome subtypes. Neurology 2014; 83: 118-24.
Plexopathy 4. PETRI M, ORBAI A-M, ALARCÓN GS et al.: 20. WEBER F, RÜDEL R, AULKEMEYER P,
Plexopathies present with signs and Derivation and validation of the Systemic BRINKMEIER H: Anti-GM1 antibodies can
block neuronal voltage-gated sodium chan-
symptoms in the area of distribution Lupus International Collaborating Clinics
nels. Muscle Nerve 2000; 23: 1414-20.
classification criteria for systemic lupus ery-
of the brachial or lumbosacral plexus. 21. LABRADOR-HORRILLO M, MARTINEZ-
thematosus. Arthritis Rheum 2012; 64: 2677-
The association between neural plexus 86. VALLE F, GALLARDO E, ROJAS-GARCIA R,
injury and SLE requires further confir- 5. HOCHBERG MC: Updating the American ORDI-ROS J, VILARDELL M: Anti-gangli-
College of Rheumatology revised criteria for oside antibodies in patients with systemic
mations, in fact, only few case reports lupus erythematosus and neurological mani-
the classification of systemic lupus erythe-
were published in literature so far (1, matosus. Arthritis Rheum 1997; 40: 1725. festations. Lupus 2012; 21: 611-5.
7, 94). Oomatia et al. reported 1.2% 6. HANLY JG, SU L, FAREWELL V, McCURDY 22. GABER W, EZZAT Y, El FAYOUMY NM,
of plexopathy in their John Hopkins’s G, FOUGERE L, THOMPSON K: Prospective HELMY H, MOHEY AM: Detection of asymp-
study of neuropsychiatric events in systemic tomatic cranial neuropathies in patients with
Lupus Cohort (1 patient) (1) and sug- systemic lupus erythematosus and their rela-
lupus erythematosus. J Rheumatol 2009; 36:
gested this entity could reflect a coinci- 1449-59. tion to antiribosomal P antibody levels and
dental neurologic syndrome occurring 7. UNTERMAN A, NOLTE JES, BOAZ M, ABADY disease activity. Clin Rheumatol 2014; 33:
in SLE. The rarity and low level of at- M, SHOENFELD Y, ZANDMAN-GODDARD 1459-66.
G: Neuropsychiatric syndromes in systemic 23. EURELINGS M, van den BERG LH, WOKKE
tribution to the underlying SLE of this lupus erythematosus: a meta-analysis. Semin JHJ, FRANSSEN H, VRANCKEN AFJE, NOTER-
clinical picture arises some questions Arthritis Rheum 2011; 41: 1-11. MANS NC: Increase of sural nerve T cells
about the opportunity of maintaining 8. XIANBIN W, MINGYU W, DONG X et al.: in progressive axonal polyneuropathy and
Peripheral neuropathies due to systemic lu- monoclonal gammopathy. Neurology 2003;
its inclusion into the ACR 1999 case
pus erythematosus in China. Medicine (Bal- 61: 707-9.
definition. timore) 2015; 94: e625. 24. VRANCKEN AFJE, NOTERMANS NC, JANS-
Table IV summarises therapeutical op- 9. TOLEDANO P, ORUETA R, RODRÍGUEZ- EN GH, WOKKE JHJ, SAID G: Progressive
tions available for each PNS manifes- PINTÓ I, VALLS-SOLÉ J, CERVERA R, ES- idiopathic axonal neuropathy--a comparative
PINOSA G: Peripheral nervous system in- clinical and histopathological study with vas-
tation covered in this review, focusing culitic neuropathy. J Neurol 2004; 251: 269-
volvement in systemic lupus erythematosus:
on first-line approach and treatment of Prevalence, clinical and immunological 78.
refractory cases. characteristics, treatment and outcome of a 25. COLLINS MP, ARNOLD WD, KISSEL JT: The
Clinical and Experimental Rheumatology 2019 153PNS involvement in SLE / A. Bortoluzzi et al.
neuropathies of vasculitis. Neurol Clin 2013; ology 2002; 58: 1214-20. from: http://www.ncbi.nlm.nih.gov/pmc/ar-
31: 557-95. 40. SALEH Z, MENASSA J, ABBAS O, ATWEH S, ticles/PMC4553270/
26. MARTINEZ ARM, FABER I, NUCCI A, APPEN- ARAYSSI T: Cranial nerve VI palsy as a rare 57. BINGISSER R, SPEICH R, FONTANA A, GMÜR
ZELLER S, FRANÇA MC: Autoimmune neu- initial presentation of systemic lupus erythe- J, VOGEL B, LANDIS T: Lupus Erythematosus
ropathies associated to rheumatic diseases. matosus: case report and review of the litera- and Miller-Fisher Syndrome. Arch Neurol
Autoimmun Rev 2017; 16: 335-42. ture. Lupus 2010; 19: 201-5. 1994; 51: 828-30.
27. BÓDI I, VÁRADI P, POKORNY G et al.: Poly- 41. GENEVAY S, HAYEM G, HAMZA S, PALAZZO 58. SANTIAGO-CASAS Y, PEREDO RA, VILÁ LM:
neuropathy with endoneurial immune com- E, MEYER O, KAHN MF: Oculomotor palsy in Efficacy of low-dose intravenous cyclophos-
plex deposition as the first manifestation of six patients with systemic lupus erythemato- phamide in systemic lupus erythematosus
systemic lupus erythematosus. Acta Neuro- sus. A possible role of antiphospholipid syn- presenting with Guillain-Barre syndrome-
pathol (Berl) 1998; 96: 297-300. drome. Lupus 2002; 11: 313-6. like acute axonal neuropathies: report of two
28. GOVONI M, BORTOLUZZI A: Lupus or not lu- 42. GALINDO M, PABLOS JL, GÓMEZ-REINO JJ: cases. Lupus 2013; 22: 324-7.
pus? Neuropsychiatric symptom attribution Internuclear ophthalmoplegia in systemic 59. Joint Task Force of the EFNS and the PNS.
in systemic lupus erythematosus: Strapline: lupus erythematosus. Semin Arthritis Rheum European Federation of Neurological Socie-
Repetita iuvant. Rheumatology (Oxford) 1998; 28: 179-86. ties/Peripheral Nerve Society Guideline on
2017; 56: 1639-40 43. GOVONI M, BORTOLUZZI A, PADOVAN M et management of chronic inflammatory demy-
29. FANOURIAKIS A, PAMFIL C, REDNIC S, SIDI- al.: The diagnosis and clinical management elinating polyradiculoneuropathy: report of a
ROPOULOS P, BERTSIAS G, BOUMPAS DT: of the neuropsychiatric manifestations of lu- joint task force of the European Federation
Is it primary neuropsychiatric systemic lupus pus. J Autoimmun 2016; 74: 41-72. of Neurological Societies and the Peripheral
erythematosus? Performance of existing at- 44. KOBAYASHI S, FUJISHIRO N, SUGIYAMA K: Nerve Society--First Revision. J Peripher
tribution models using physician judgment Systemic lupus erythematosus with sensori- Nerv Syst JPNS 2010; 15: 1-9.
as the gold standard. Clin Exp Rheumatol neural hearing loss and improvement after 60. NG JKM, MALOTKA J, KAWAKAMI N et al.:
2016; 34: 910-17. plasmapheresis using the double filtration Neurofascin as a target for autoantibodies
30. BORTOLUZZI A, FANOURIAKIS A, APPEN- method. Intern Med Tokyo Jpn 1992; 31: in peripheral neuropathies. Neurology 2012;
ZELLER S et al.: Validity of the Italian algo- 778-81. 79: 2241-8.
rithm for the attribution of neuropsychiatric 45. JOHNSON RT, RICHARDSON EP: The neuro- 61. LATOV N: Diagnosis of CIDP. Neurology
events in systemic lupus erythematosus: a ret- logical manifestations of systemic lupus ery- 2002; 59 (12 Suppl. 6): S2-6.
rospective multicentre international diagnos- thematosus. Medicine (Baltimore) 1968; 47: 62. HUGHES R, BENSA S, WILLISON H et al.:
tic cohort study. BMJ Open 2017; 7: e015546. 337-69. Randomized controlled trial of intravenous
31. FINNERUP NB, ATTAL N, HAROUTOUNIAN S 46. RIVIÈRE E, AUBART FC, MAISONOBE T et immunoglobulin versus oral prednisolone in
et al.: Pharmacotherapy for neuropathic pain al.: Clinicopathological features of multiple chronic inflammatory demyelinating poly-
in adults: a systematic review and meta-anal- mononeuropathy associated with systemic radiculoneuropathy. Ann Neurol 2001; 50:
ysis. Lancet Neurol 2015; 14: 162-73. lupus erythematosus: a multicenter study. 195-201.
32. ATTAL N, CRUCCU G, BARON R et al.: EFNS J Neurol 2017; 264: 1218-26. 63. HAHN AF, BOLTON CF, PILLAY N et al.:
guidelines on the pharmacological treatment 47. KEANE JR: Multiple cranial nerve palsies: Plasma-exchange therapy in chronic inflam-
of neuropathic pain: 2010 revision. Eur J analysis of 979 cases. Arch Neurol 2005; 62: matory demyelinating polyneuropathy. A dou-
Neurol 2010; 17: 1113-e88. 1714-7. ble-blind, sham-controlled, cross-over study.
33. BERTSIAS GK, IOANNIDIS JPA, ARINGER 48. MATHEW L, TALBOT K, LOVE S, PUVANARA- Brain J Neurol 1996; 119 (Pt 4): 1055-66.
M et al.: EULAR recommendations for the JAH S, DONAGHY M: Treatment of vasculitic 64. KUITWAARD K, HAHN AF, VERMEULEN M,
management of systemic lupus erythemato- peripheral neuropathy: a retrospective analy- VENANCE SL, van DOORN PA: Intravenous
sus with neuropsychiatric manifestations: sis of outcome. QJM Int J Med 2007; 100: immunoglobulin response in treatment-naïve
report of a task force of the EULAR standing 41-51. chronic inflammatory demyelinating polyra-
committee for clinical affairs. Ann Rheum 49. MUANGCHAN C, van VOLLENHOVEN RF, diculoneuropathy. J Neurol Neurosurg Psy-
Dis 2010; 69: 2074-82. BERNATSKY SR et al.: Treatment algorithms chiatry 2015; 86: 1331-6.
34. NEUWELT CM, LACKS S, KAYE BR, ELLMAN in systemic lupus erythematosus. Arthritis 65. VINA ER, FANG AJ, WALLACE DJ, WEISMAN
JB, BORENSTEIN DG: Role of intravenous Care Res 2015; 67: 1237-45. MH: Chronic inflammatory demyelinating
cyclophosphamide in the treatment of severe 50. LENEMAN F: The Guillain-Barré syndrome. polyneuropathy in patients with systemic lu-
neuropsychiatric systemic lupus erythemato- Definition, etiology, and review of 1,100 pus erythematosus: prognosis and outcome.
sus. Am J Med 1995; 98: 32-41. cases. Arch Intern Med 1966; 118: 139-44. Semin Arthritis Rheum 2005; 35: 175-84.
35. LEVY Y, UZIEL Y, ZANDMAN G et al.: 51. ZHONG Z, SANCHEZ-LOPEZ E, KARIN M: 66. QUEROL L, ROJAS-GARCÍA R, DIAZ-MANE-
Response of vasculitic peripheral neuropa- Autophagy, NLRP3 inflammasome and auto- RA J et al.: Rituximab in treatment-resistant
thy to intravenous immunoglobulin. Ann N Y inflammatory/immune diseases. Clin Exp CIDP with antibodies against paranodal pro-
Acad Sci 2005; 1051: 779-86. Rheumatol 2016; 34 (Suppl. 98): S12-6. teins. Neurol Neuroimmunol Neuroinflam-
36. BARILE-FABRIS L, ARIZA-ANDRACA R, 52. RÖNNBLOM L: The importance of the type I mation 2015; 2: e149.
OLGUÍN-ORTEGA L et al.: Controlled clini- interferon system in autoimmunity. Clin Exp 67. THEMISTOCLEOUS AC, RAMIREZ JD, SERRA
cal trial of IV cyclophosphamide versus IV Rheumatol 2016; 34 (Suppl. 98): S21-4. J, BENNETT DLH: The clinical approach to
methylprednisolone in severe neurological 53. WU H, FU S, ZHAO M, LU L, LU Q: Dysregula- small fibre neuropathy and painful channelo-
manifestations in systemic lupus erythema- tion of cell death and its epigenetic mecha- pathy. Pract Neurol 2014; 14: 368-79.
tosus. Ann Rheum Dis 2005; 64: 620-5. nisms in systemic lupus erythematosus. Mol 68. CRUCCU G, AMINOFF MJ, CURIO G et al.:
37. STOJANOVICH L, STOJANOVICH R, KOS- ecules 2016; 22: pii: E30. Recommendations for the clinical use of
TICH V, DZJOLICH E: Neuropsychiatric lupus 54. MULLER S, BRUN S, RENÉ F, de SÈZE J, somatosensory-evoked potentials. Clin Neu-
favourable response to low dose i.v. cyclo- LOEFFLER J-P, JELTSCH-DAVID H: Autophagy rophysiol Off J Int Fed Clin Neurophysiol
phosphamide and prednisolone (pilot study). in neuroinflammatory diseases. Autoimmun 2008; 119: 1705-19.
Lupus 2003; 12: 3-7. Rev 2017; 16: 856-74. 69. TESFAYE S, BOULTON AJM, DYCK PJ et al.:
38. HANLY JG, UROWITZ MB, SU L et al.: 55. BUKHARI S, TABOADA J: A Case of Miller Diabetic neuropathies: update on defini-
Prospective analysis of neuropsychiatric Fisher Syndrome and Literature Review. tions, diagnostic criteria, estimation of sever-
events in an international disease inception Cureus 2017; 9: e1048. ity, and treatments. Diabetes Care 2010; 33:
cohort of patients with systemic lupus erythe- 56. OKOH HC, LUBANA SS, LANGEVIN S, 2285-93.
matosus. Ann Rheum Dis 2010; 69: 529-35. SANELLI-RUSSO S, ABRUDESCU A: A Case 70. BACKONJA MM, ATTAL N, BARON R et al.:
39. BREY RL, HOLLIDAY SL, SAKLAD AR et al.: of Systemic Lupus Erythematosus Present- Value of quantitative sensory testing in neu-
Neuropsychiatric syndromes in lupus: preva- ing as Guillain-Barré Syndrome. Case Rep rological and pain disorders: NeuPSIG con-
lence using standardized definitions. Neur- Rheumatol [Internet]. 2015;2015. Available sensus. Pain 2013; 154: 1807-19.
154 Clinical and Experimental Rheumatology 2019PNS involvement in SLE / A. Bortoluzzi et al.
71. LAURIA G, HSIEH ST, JOHANSSON O et al.: lar damage in human diabetic neuropathy. 87. ISENBERG DA, RAHMAN A, ALLEN E et al.:
European Federation of Neurological Socie- Diabetologia 1993; 36: 454-9. BILAG 2004. Development and initial vali-
ties/Peripheral Nerve Society Guideline on 80. HOEIJMAKERS JG, FABER CG, LAURIA G, dation of an updated version of the British
the use of skin biopsy in the diagnosis of small MERKIES IS, WAXMAN SG: Small-fibre Isles Lupus Assessment Group’s disease
fiber neuropathy. Report of a joint task force neuropathies--advances in diagnosis, patho- activity index for patients with systemic lu-
of the European Federation of Neurological physiology and management. Nat Rev Neurol pus erythematosus. Rheumatology (Oxford)
Societies and the Peripheral Nerve Society. 2012; 8: 369-79. 2005; 44: 902-6.
Eur J Neurol 2010; 17: 903-12, e44-49. 81. UÇEYLER N, KAFKE W, RIEDIGER N et al.: 88. SCHROEDER C, VERNINO S, BIRKENFELD
72. JIANG M-S, YUAN Y, GU Z-X, ZHUANG S-L: Elevated proinflammatory cytokine expres- AL et al.: Plasma exchange for primary au-
Corneal confocal microscopy for assessment sion in affected skin in small fiber neuropa- toimmune autonomic failure. N Engl J Med
of diabetic peripheral neuropathy: a meta- thy. Neurology 2010; 74: 1806-13. 2005; 353: 1585-90.
analysis. Br J Ophthalmol 2016; 100: 9-14. 82. MURATA Y, MAEDA K, KAWAI H et al.: 89. MODONI A, MIRABELLA M, MADIA F et al.:
73. GØRANSSON LG, TJENSVOLL AB, HERIG- Antiganglion neuron antibodies correlate Chronic autoimmune autonomic neuropathy
STAD A, MELLGREN SI, OMDAL R: Small- with neuropathy in Sjögren’s syndrome. responsive to immunosuppressive therapy.
diameter nerve fiber neuropathy in systemic Neuroreport 2005; 16: 677-81. Neurology 2007; 68: 161-2.
lupus erythematosus. Arch Neurol 2006; 63: 83. BIRNBAUM J, DUNCAN T, OWOYEMI K, 90. LESZCZYNSKI P, PAWLAK-BUS K: Vocal
401-4. WANG KC, CARRINO J, CHHABRA A: Use of cords palsy in systemic lupus erythematosus
74. TSENG M-T, HSIEH S-C, SHUN C-T et al.: Skin a novel high-resolution magnetic resonance patient: diagnostic and therapeutic difficul-
denervation and cutaneous vasculitis in sys- neurography protocol to detect abnormal ties. Rheumatol Int 2013; 33: 1577-80.
temic lupus erythematosus. Brain J Neurol dorsal root Ganglia in Sjögren patients with 91. MELZER N, RUCK T, FUHR P et al.: Clinical
2006; 129: 977-85. neuropathic pain: case series of 10 patients features, pathogenesis, and treatment of my-
75. GORSON KC, HERRMANN DN, THIAGARA- and review of the literature. Medicine (Balti- asthenia gravis: a supplement to the Guide-
JAN R et al.: Non-length dependent small more) 2014; 93: 121-34. lines of the German Neurological Society.
fibre neuropathy/ganglionopathy. J Neurol 84. de GREEF BTA, GEERTS M, HOEIJMAKERS J Neurol 2016; 263: 1473-94.
Neurosurg Psychiatry 2008; 79: 163-9. JGJ, FABER CG, MERKIES ISJ: Intravenous 92. MAGRO-CHECA C, ZIRKZEE EJ, HUIZINGA
76. GEMIGNANI F, GIOVANELLI M, VITETTA F immunoglobulin therapy for small fiber neu- TW, STEUP-BEEKMAN GM: Management of
et al.: Non-length dependent small fiber neu- ropathy: study protocol for a randomized neuropsychiatric systemic lupus erythemato-
ropathy. a prospective case series. J Peripher controlled trial. Trials 2016; 17: 330. sus: current approaches and future perspec-
Nerv Syst JPNS 2010; 15: 57-62. 85. MILOVANOVIĆ B, STOJANOVIĆ L, MILI- tives. Drugs 2016; 76: 459-83.
77. CHAMBERLAIN JL, PITTOCK SJ, OPRESCU ĆEVIK N, VASIĆ K, BJELAKOVIĆ B, KROTIN 93. JALLOULI M, SAADOUN D, EYMARD B et al.:
A-M et al.: Peripherin-IgG association with M: Cardiac autonomic dysfunction in pa- The association of systemic lupus erythema-
neurologic and endocrine autoimmunity. tients with systemic lupus, rheumatoid ar- tosus and myasthenia gravis: a series of 17
J Autoimmun 2010; 34: 469-77. thritis and sudden death risk. Srp Arh Celok cases, with a special focus on hydroxychlo-
78. DABBY R, WEIMER LH, HAYS AP, OLARTE Lek 2010; 138: 26-32. roquine use and a review of the literature.
M, LATOV N: Antisulfatide antibodies in neu- 86. STOJANOVICH L, MILOVANOVICH B, de J Neurol 2012; 259: 1290-7.
ropathy: clinical and electrophysiologic cor- LUKA SR et al.: Cardiovascular autonomic 94. BLOCH SL, JARRETT MP, SWERDLOW M,
relates. Neurology 2000; 54: 1448-52. dysfunction in systemic lupus, rheumatoid GRAYZEL AI: Brachial plexus neuropathy as
79. MALIK RA, TESFAYE S, THOMPSON SD et arthritis, primary Sjögren syndrome and other the initial presentation of systemic lupus ery-
al.: Endoneurial localisation of microvascu- autoimmune diseases. Lupus 2007; 16: 181-5. thematosus. Neurology 1979; 29: 1633-4.
Clinical and Experimental Rheumatology 2019 155You can also read