Review Article The Effectiveness of the Bacteria Derived Extremolyte Ectoine for the Treatment of Allergic Rhinitis - Hindawi.com
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Hindawi
BioMed Research International
Volume 2021, Article ID 5562623, 16 pages
https://doi.org/10.1155/2021/5562623
Review Article
The Effectiveness of the Bacteria Derived Extremolyte Ectoine for
the Treatment of Allergic Rhinitis
Andreas Bilstein,1 Nina Werkhäuser,2 Anna Rybachuk,3,4 and Ralph Mösges 5,6
1
Ursatec GmbH, Marpinger Weg 4, 66636 Tholey, Germany
2
bitop AG, Carlo-Schmid-Allee 5, Dortmund, Germany
3
Bogomolets National Medical University, Department of Oral and Maxillofacial Surgery, Tarasa Shevchenko Blvd, 13, Kiev, Ukraine
01601
4
State Institution “O.S. Kolomiychenko Institute of Otolaryngology of the National Academy of Medical Sciences of Ukraine”,
Zoolohichna St, 3, Kiev, Ukraine 03057
5
CRI Ltd, Genter Str. 7, 50672 Cologne, Germany
6
Institute of Medical Statistics and Computational Biology, Faculty of Medicine, University of Cologne, Kerpener Str. 62,
50937 Cologne, Germany
Correspondence should be addressed to Ralph Mösges; ralph@moesges.de
Received 28 January 2021; Accepted 20 May 2021; Published 1 June 2021
Academic Editor: Luisa Brussino
Copyright © 2021 Andreas Bilstein et al. This is an open access article distributed under the Creative Commons Attribution
License, which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is
properly cited.
Nonpharmacological therapies with a good tolerability and safety profile are of interest to many patients with allergic rhinitis, as a
relevant proportion of them have reservations about guideline-concordant pharmacological therapies due to their local irritations
and side effects. Ectoine is a bacterial-derived extremolyte with an ability to protect proteins and biological membranes against
damage caused by extreme conditions of salinity, drought, irradiation, pH, and temperature. Evidence from preclinical and
clinical studies attests its effectiveness in the treatment of several inflammatory diseases, including allergic rhinitis. In this
review, we analyzed 14 recent clinical trials investigating ectoine nasal spray in patients with allergic rhinitis and/or
conjunctivitis, including sensitive patient groups like children or pregnant women. Some studies investigated monotherapy with
ectoine; others investigated combination therapy of ectoine and an antihistamine or a corticosteroid. Analysis of the study
results demonstrated that patients with mild-to-moderate symptoms of allergic rhinitis can be successfully treated with ectoine-
containing nasal spray. When applied as monotherapy, ectoine exerted noninferior effects compared to first-line therapies such
as antihistamines and cromoglicic acid. Using ectoine as an add-on therapy to antihistamines or intranasal glucocorticosteroids
accelerated symptom relief by days and improved the level of symptom relief. Importantly, concomitant treatment with ectoine
was proven beneficial in a group of difficult-to-treat patients suffering from moderate-to-severe rhinitis symptoms. Taken
together, the natural substance ectoine represents a viable alternative for allergic rhinitis and conjunctivitis patients who wish to
avoid local reactions and side effects associated with pharmacological therapies.
1. Introduction it is preferentially excluded from the hydrate shield, leading
to the alteration of the aqueous solvent structure [6, 7], which
Ectoine is a natural extremolyte found in bacteria which protects proteins from damage and irreversible denaturation
grows under extreme conditions of salinity, drought, irradia- and stabilizes biological membranes [3, 8–10]. In preclinical
tion, pH, and temperature [1, 2]. Ectoine binds strongly to studies, ectoine was shown to protect lung and skin cells
water molecules [3], thereby forming a protective hydrate against the damage induced by toxic pollution particles and
shield around proteins and other biomolecules [4]. It works to prevent the subsequent activation of inflammatory cas-
via a mechanism known as “preferential exclusion” [5]; i.e., cades [11–16]. A similar effect was observed in model2 BioMed Research International
systems for inflammatory bowel disease [17]. Promising (PRISMA) statement [41]. In order to evaluate the quality
findings from clinical trials harnessed ectoine as a therapeutic of the selected studies, a Jadad score was allocated for each
agent for several inflammatory diseases such as atopic der- trial to assess methodological quality [42] as indicated in
matitis [18], upper airway inflammations like pharyngiti- Table 1.
s/laryngitis [19, 20], rhinosinusitis and acute bronchitis [21]
as reviewed by Casale and colleagues [22], rhinitis sicca
[23], chemotherapy-induced mucositis [24], and also lung 2.1. Objectives and Search Strategy. Initial search databases
inflammation caused by environmental pollutants [25], even were PubMed, Google Scholar, and Ovid; search language
in long-term applications in children to prevent upper respi- was English. After the search in Google Scholar and PubMed
ratory infections [26] or treatment of vernal keratoconjuncti- reported several articles in Russian and Ukrainian language,
vitis [27]. we extended the search to Elibrary.ru and to the National
The global prevalence of all allergic diseases is reported to Library of Ukraine and included Russian/Ukrainian language
be 20-30% [28], resulting in a high pressure on the social eco- as search criterion. The country of origin and languages were
nomic systems. The Global Allergy and Asthma European not limited; the period was set to the beginning of 2010 to 15-
Network report indicated that cost savings of over EUR 100 Nov-2020.
billion could be realistically expected through better treat- The following key word/medical subject headings were
ment of allergic diseases [29]. The 2008 and 2020 Allergic used as search terms: “ectoine” and “nasal spray”, “ectoine”
Rhinitis and its Impact on Asthma (ARIA) guideline pro- and “allergic rhinitis”, “ectoine” and “nasal irritation”,
vides physicians with a treatment algorithm for allergic rhini- “ectoine” and “allergic rhinoconjunctivitis”, “ectoine” and
tis and conjunctivitis depending on the severity and duration “allergy”, “ectoine” and “hay fever”, “ectoine” and “nose”.
of symptoms [30, 31]. Pharmacological therapies with oral/- The search was limited to clinical trials describing the appli-
topical antihistamines, intranasal glucocorticosteroids cation of ectoine nasal spray in allergic rhinitis, independent
(INCS), oral glucocorticosteroids, decongestants, leukotriene on the design of the study (including controlled, noncon-
receptor antagonists, and cromones are considered the main- trolled, interventional, and noninterventional studies). Only
stay of allergic rhinitis treatment. However, despite the myr- studies published in peer-reviewed journals or presented on
iad of treatment options with pharmacological drugs, a scientific congresses were considered. Reference lists of the
relevant proportion of patients with moderate-to-severe selected articles were assessed, and additional references fit-
symptoms are still not sufficiently treated [32–36]. For ting the subject of this review were included. Reviews, sys-
instance, a study reported that about 60% of allergic rhinitis tematic reviews, meta-analysis, case series, publications
sufferers in the U.S. are “very interested” in trying out new containing preclinical data, letters, editorials, errata, and
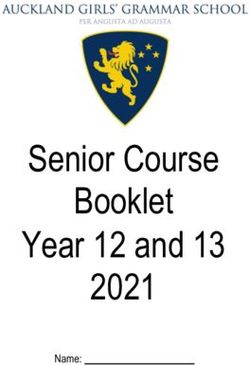
medications [37]. Furthermore, some patients are reluctant reports of pooled data were excluded (Figure 1).
to use pharmacological therapies for fear of local irritations
and side effects associated with sedative antihistamines as 2.2. Search Results. Following the search strategy described
well as tachyphylaxis under long-term use of nasal deconges- above, a total of 14 relevant human studies performed
tants, which can lead to poor medication compliance [38, between 2010 and 2019 investigating ectoine nasal spray
39]. Therefore, nonpharmacological therapies with an (ENS) in treatment of allergic rhinitis were selected and
advantageous tolerability and safety profile are of interest to further evaluated.
many patients with allergic rhinitis and conjunctivitis.
For treatment of allergic rhinoconjunctivitis, ectoine
nasal sprays and eye drops are already on the market as med- 2.3. Study Design and Study Population. Except for one trial
ical devices in several countries. Eichel and colleagues have [43], all trials were real-life studies applying the ectoine prod-
published a meta-analysis on selected clinical studies recently uct (s): a preservative-free nasal spray containing 2% ectoine,
[40]. Since the ectoine nasal spray was the first ectoine- 0.9% sea salt, and water in the 3K System and, where applica-
containing product envisioned as a nonpharmacological ble, preservative-free eye drops containing 2% ectoine, 0.35%
therapeutic agent for allergic rhinitis, a considerable number hydroxyethyl cellulose, 0.35% sodium chloride, citrate buffer,
of clinical trials with this product have meanwhile been per- and water, according to the instruction for use over a rather
formed. Following the initial controlled trials comparing short period of time (1 week to 4 weeks, depending on trial)
ectoine to standard pharmacological therapies, several real- either as monotherapy or in combination with other inter-
life, interventional, or noninterventional trials have been ventions. All studies were performed with patients (adults
conducted. In this article, we systematically reviewed the lit- and children) manifesting clinical symptoms characteristic
erature on treatment of allergic rhinitis with ectoine-based of allergic rhinitis, which had been diagnosed by radioaller-
nasal sprays to disseminate the most current evidence for gosorbent or skin prick test.
the treatment of allergic rhinitis with this interesting Patient-reported symptoms (diary) were used as a pri-
substance. mary outcome parameter in all studies. These scoring dif-
fered greatly and ranged from combined visual analogue
2. Methods scales for all symptoms, to individual scales for up to 8 symp-
toms. Consequently, summary scores were calculated differ-
This review was conducted in accordance with the Preferred ently. Several trials applied additional methods, such as
Reporting Items for Systematic Reviews and Meta-Analyses rhinocytogram, rhinoscopy, or eosinophil counting [44, 45].Table 1: Details on the selected studies. ACT: asthma control test; AE: adverse event; AR: allergic rhinitis; ASIT: allergen-specific immunotherapy; IAR: intermittent allergic rhinitis; INS:
intranasal steroids; SAE: serious adverse event; TNNSS: total nonnasal symptom score; TNSS: total nasal symptom score; TOSS: total ocular symptom score.
Patient
Inclusion Treatment
Authors, year, population, Jadad
Study N of patients (total and by criteria/exclusion duration, Reported side
study location Indication of study Comparator age (years) Outcome parameters scale
design groups) criteria (only AR- dosage, and effects
[reference] of (criteria)
specific criteria listed) number of visits
participants
21-day (3 weeks)
Children & Inclusion: diagnosis of treatment
Minaeva and adolescents seasonal AR, Ectoine: 3-4
Total: 50 Nasal congestion,
Shiryaeva, Oral R, C, Age range: sensitization to tree times daily 3 (A, B,
Allergic rhinitis Ectoine + antihistamine: 30 rhinorrhea, itching, No AE reported
2015, Russia antihistamine OL 3-17 pollen, received an Antihistamine: E)
antihistamine alone: 20 sneezing
BioMed Research International
[50] Mean age: antihistamine product age-appropriate
10.6 Exclusion: taking INS dose
3 visits
Inclusion: diagnosed
intermittent AR,
during a period of
Sneezing, itching,
exacerbation of
rhinorrhea, nasal
symptoms, admissible
congestion, dry
accompanying
60-day mucosa, cough, fatigue, No AE reported for
pharmacotherapy
treatment eosinophils, unpleasant the ectoine
Adults Exclusion: pregnant
Total: 90 Ectoine: 1-2 smell in the treatment, 4
Abdulkerimov Age range: and nursing women,
Intranasal R, C, Ectoine alone: 30 sprays 3 times a rhinopharynx, patients from the
et al., 2016, Allergic rhinitis 18-65 intolerance to one of 2 (A, B)
glucocorticoid OL INS alone: 30 day rhinoscopy status, INS-alone group
Russia [46] Mean age: the substances, usage
Ectoine + INS: 30 INS: 2 doses video endoscopic reported increased
not assessed of other antiallergy
once a day investigation status of dryness of the
agents, nose surgery
4 visits the nasal cavity, nasal mucosa
within 6 weeks before
cytological
the study, signs of
investigation status of
bacterial disease, flu,
the nasal secretion
antibacterial
treatment, stomatic
disease
Inclusion: diagnosed
seasonal allergic
28-day
rhinitis,
treatment Rhinorrhea,
Children & Exclusion: AR flare-
Anti- Total: 60 (4 weeks) paroxysmal sneezing,
adolescents ups associated with an
Kayb et al., inflammatory Ectoine + anti − inflammatory Ectoine: as nasal congestion
Age range: acute respiratory
2016, Russia Allergic rhinitis therapy C, OL therapy: 30 prescribed clinical manifestations No AE reported 1 (E)
5-17 disease with increased
[51] (standard of Anti-inflammatory therapy Anti- of the flare-ups and the
Mean age: body temperature, as
care) alone: 30 inflammatory: as severity of AR in the
not assessed well as children with
prescribed course
an AR flare-up, atopic
4 visits
dermatitis, and
bronchial asthma
Inclusion: diagnosis of 3 AEs were
21-day TNSS, rhinoscopy
all year-round AR reported. 2
Children & treatment status, rhinocytogram
(mild and moderate increased sneezing
adolescents Ectoine: 2 doses status, tolerability,
Bardenikova Total: 30 severity) with immediately
Age range: per nostril, 3 compliance, adverse
et al., 2016, Allergic rhinitis INS OL, C Ectoine: 17 clinically significant following 1 (E)
7-17 times per day effects, blood test,
Russia [52] Ectoine + INS: 13 sensitization to house application of the
Mean age: INS: as cytomorphology (cell
allergens. The patients spray; 1 short nasal
12.4 prescribed count), pediatric ACT,
were enrolled while bleeding during
2 visits eosinophilic cytosis
experiencing the administration
34
Table 1: Continued.
Patient
Inclusion Treatment
Authors, year, population, Jadad
Study N of patients (total and by criteria/exclusion duration, Reported side
study location Indication of study Comparator age (years) Outcome parameters scale
design groups) criteria (only AR- dosage, and effects
[reference] of (criteria)
specific criteria listed) number of visits
participants
exacerbation of
persistent AR, with a
total score for nasal
symptoms (TNSS) of
2 points or more
Exclusion: seasonal
exacerbations caused
by associated
pollinosis
Children & 10-day
Itchiness, periodic
Skosarev et al., adolescents treatment
Total: 36 sneezing, coughing,
2015, Age range: Inclusion: children Ectoine: as No information
Allergic rhinitis Standard of care OL, C Ectoine: 18 voice changes, night 0
Kazakhstan not assessed with diagnosis of AR prescribed given
Standard of care: 18 snoring, emotional
[53] Mean age: Standard of care:
profiles
not assessed as prescribed
Primary: TNSS
14-day
(including sneezing,
treatment per
Inclusion: history of itchy nose, runny nose
treatment type
seasonal AR, positive and nasal congestion) 6 AEs reported
Salapatek et al., Adults crossover after
skin prick test, TNSS and TOSS (including during ectoine
2011, Canada Age range: 7 days washout
Total: 46 ≥ 6/2, TOSS ≥ 4/9 watery eye, itchy eye, treatment. During
[43] Allergic 18-65 Ectoine: 1
Placebo R, C Ectoine: 46 Exclusion: usage of red eye) placebo treatment, 5 (A-E)
(manuscript rhinoconjunctivitis Mean age: spray/nostril 3
Placebo: 46 antiallergic Secondary: TNNSS 5 AEs were
accepted for 43:9 ± 11:3 times per day
medication before (including watery eye, reported. No SAEs
publication) Placebo: 1
study start and itchy eye, red eye, and occurred
spray/nostril 3
throughout the study itchy ear/palate), and
times per day
acoustic rhinometry
5 visits
measurements
14-day
Primary: nasal
Inclusion: 18-70 years, treatment 3 AEs, 2 in the
Adults obstruction,
diagnosed seasonal Ectoine: 3 times ectoine group (not
Sonnemann Total: 50 Age range: rhinorrhea, nasal
OL, allergic rhinitis, TNSS daily, related), 1 in the
et al., 2014, Allergic rhinitis Beclomethasone Ectoine: 25 18-65 itching, sneezing 1 (E)
NI, C >6 Beclomethasone beclomethasone
Germany [47] Beclomethasone: 25 Mean age: Secondary: itchy
Exclusion: not (0.05 mg): 2 group (probably
33.3 ear/palate, efficacy,
described times daily, related)
tolerability
2 visits
7-day treatment 8 AEs: 2 cases of
Inclusion: patients
Ectoine: one eye burning of eyes
aged 18-70, proven
drop per eye and and itching of the
allergy in prick test,
one puff of the throat in the
acute symptoms in Nasal obstruction,
Adults nasal spray per ectoine group, and
nose and eyes rhinorrhea, sneezing
Werkhäuser Total: 48 Age nostril four 6 (4 cases of
OL, Exclusion: pregnant nasal itching,
et al., 2014, Allergic rhinitis Azelastine Ectoine: 22 range:18-65 times per day burning of eyes, 1 1 (E)
NI, C and nursing women, conjunctivitis, eye
Germany [49] Azelastine: 26 Mean age: Azelastine: One case of nausea, and
drug addicts, patients itching, tearing, palate
35 eye drop, one 1 case of headache)
with intolerance itching
puff nasal spray, in the azelastine
against ingredients of
both twice per group
treatments, previous
day
eye or nose surgery No SAE occurred
2 visits
BioMed Research InternationalTable 1: Continued.
Patient
Inclusion Treatment
Authors, year, population, Jadad
Study N of patients (total and by criteria/exclusion duration, Reported side
study location Indication of study Comparator age (years) Outcome parameters scale
design groups) criteria (only AR- dosage, and effects
[reference] of (criteria)
specific criteria listed) number of visits
participants
Inclusion: patients During the study,
14-day
aged 18-70, proven no SAE occurred
treatment
allergy in prick test,
crossover after 7
acute symptoms in the Nasal obstruction,
Adults days No AEs were
nose and eyes rhinorrhea, sneezing
Werkhäuser Total: 50 Age range: Ectoine: 5 times observed for
Cromoglicic OL, Exclusion: pregnant nasal itching,
et al., 2014, Allergic rhinitis Ectoine: 25 18-65 per day, ectoine containing 1 (E)
acid NI, C and nursing women, conjunctivitis, eye
BioMed Research International
Germany [49] Cromoglicic acid: 25 Mean age: cromoglicic acid
drug addicts, patients itching, tearing, palate nasal spray; 15 AEs
35 (20 mg/ml): were recorded for
with intolerance itching
nasal spray 4 the cromoglicic
against ingredients of
times per day acid nasal spray
treatments, previous
3 visits
eye or nose surgery
Inclusion: sensitized
14-day
Children & to pollen allergens,
treatment
adolescents sufficient compliance,
Kryuchko Total: 60 Ectoine: as Activity, sleep, nasal
OL, Age range: patients applying No adverse effects
et al., 2014, Allergic rhinitis Sea salt solution Ectoine: 38 prescribed symptoms, ocular 0
NI, C 6-14 antihistamines on reported
Ukraine [55] Sea salt solution: 22 Control: as symptoms, emotions
Mean age: demand
prescribed
not assessed Exclusion: not
5 visits
described
Inclusion: pregnancy,
proven case of AR at
the time of
examination, aged 18
to 40 years, presence
of 2 or more typical
signs of AR, bright-
red mucosa in
aggravated seasonal
allergic rhinitis,
cyanotic or gray
mucosa in perennial
Pregnant All patients
allergic rhinitis, the
Total: 45 women received 1-2
mucosa spotting
Ryabova et al., Group persistent allergic Age range: doses of ectoine Rhinoscopy status,
(“marbling”)
2019, Russia Allergic rhinitis None OL rhinitis: 25 18-40 3-4 times a day laboratory tests, None reported 1 (E)
(Voyachek’s
[54] Group intermittent allergic Mean age: or for 10 days mucociliary clearance
symptom)
rhinitis: 20 30:7 ± 0:7 before contact
Exclusion: present
with allergens
infectious diseases,
history of alcohol or
drug abuse, problems
that may limit the
patient’s ability to
follow the protocol
requirements,
participation in
another clinical trial
during the three
months preceding the
screening visit, any
56
Table 1: Continued.
Patient
Inclusion Treatment
Authors, year, population, Jadad
Study N of patients (total and by criteria/exclusion duration, Reported side
study location Indication of study Comparator age (years) Outcome parameters scale
design groups) criteria (only AR- dosage, and effects
[reference] of (criteria)
specific criteria listed) number of visits
participants
other conditions that
make it difficult to
participate in the
study
Inclusion: diagnosis of
Children & persistent AR, Rhinocytogram status, AEs reported
4 weeks of
adolescents domestic or epidermal eosinophil count during the study
Kamaev and Total: 50 treatment
Age range: sensitization, (laboratory test), result were resolved
Трусоbа, 2015, Allergic rhinitis None OL Ectoine + antihistamine: 22 Treatments as 0
not assessed exacerbation of the of the anterior completely by days
Russia [48] Ectoine + INS: 28 prescribed
Mean age: disease at the first visit rhinoscopy, result of 8 to 15 of
3 visits
not assessed Exclusion criteria not the TNSS administration
described
Inclusion: confirmed Nasal obstruction,
mono allergy to tree Max. 37-daysneezing, nasal itching,
Adults pollen, mild-moderate treatment skin test, laboratory test
Mokronosova Age range: IAR, two courses of with specific serum IgE
Ectoine: 1-2
OL, Total: 34
et al., 2017, Allergic rhinitis None 20-45 ASIT sprays 3-4 times
antibodies, cytological No AE reported 1 (E)
NI Ectoine: 34
Russia [45] Mean age: Exclusion: severe IAR, daily (or as analysis of nasal
not assessed noncompliance, nose necessary) secretions,
surgery, use of 2 visitsotorhinolaryngological
antiallergic drugs examination
Nasal obstruction,
Inclusion: tree pollen
sneezing, nasal itching,
sensitization 7-day treatment
Adults skin test, laboratory test
confirmed positive Ectoine: 1-2
Mokronosova Age range: with specific serum IgE
OL, Total: 30 test for IgE antibodies sprays 3-4 times
et al., 2019, Allergic rhinitis None 18-60 antibodies, cytological No AE reported 0
NI Ectoine: 30 Exclusion: severe IAR, daily (or as
Russia [44] Mean age: analysis of nasal
noncompliance, nose necessary)
not assessed secretions,
surgery, use of 2 visits
otorhinolaryngological
antiallergic drug
examination
Study design: randomized (R); controlled (C); open-label (OL); noninterventional (NI).
BioMed Research InternationalBioMed Research International 7
Initial database search
results “ectoine”
(up to 15 Dec 2020):
PubMed = 527
Elibrary.ru = 928
Google Scholar = 6650
Refined search strategy to combine
“ectoine” with “nasal spray” and “allergic
rhinitis
111 identified reports
Excluded from review:
- Abstract does not refer to a study
with allergic rhinitis (79)
- Double hits removed after elucidating
that the same study is reported (17)
14 trials selected for - Meta-analysis (1)
review
Figure 1: PRISMA diagram of the systematic search performed.
In all selected studies, a saline-based nasal spray with 2% reported a serious adverse effect. Among the very low rate
ectoine was applied. Comparator products are listed as of reported adverse effects which have been reported in total,
follows: no irreversible AE has been documented. All authors attri-
Intranasal corticosteroids (INS) (mometasone, flutica- bute an excellent safety profile towards the ENS (Table 1).
sone, beclomethasone) [46–48]
Oral or local antihistamine or local cromoglicate [49, 50]
3.2. Efficacy and Effectiveness of Ectoine Nasal Spray. The 14
Standard of care (guideline conform use of antihistamine
studies analyzed can be categorized into three main groups:
and cromoglicate) [51–53]
Intranasal isotonic salt solution [43, 54, 55] (a) Application of ENS concomitantly with drugs com-
Only 3 of the selected studies applied a randomization pared to application of drugs alone [46, 50–
[43, 46, 50], whereas 3 did not carry out randomization due 53](Table 2)
to local regulatory restrictions [47, 49]. Two studies were
single-arm trials [44, 45], and the remaining studies did not (b) Application of ENS alone compared to other thera-
present any information regarding randomization. pies or placebo [43, 47, 49, 55] (Table 3)
From the 14 studies, 2 have been single-armed [44, 45],
(c) Application of ENS only without comparator [44, 45,
and one triple-armed [46]. The 11 other studies were 2-
48, 54] (Table 4)
armed. Of those 11 studies, 2 studies applied a crossover
design [43, 49], and two studied 2 arms, but not comparative
[48, 54]. The other 7 studies applied a comparative design 4. Discussion
including various comparators [47, 49–53, 55].
A total of 681 subjects were studied in the 14 selected tri- 4.1. Study Design. In this systematic review, several studies
als. Overall, out of the 462 patients applying ENS, 319 reporting on the effect of ectoine nasal spray in allergic rhini-
patients used ENS alone, and 171 in total used ENS com- tis were analyzed. Although many of the studies were not
bined with other pharmacotherapies. 315 patients used a published internationally (especially the Russian/Ukrainian
study-specific comparator. Six clinical trials specifically stud- studies), the studies were comparable regarding the studied
ied the effect in children and adolescents (286/681), with the indication (allergic rhinitis) and the primary outcome
youngest child being 3 years old. All trials except one parameter (patient-reported symptoms). However, they dif-
included both male and female patients (excluding pregnant fered in terms of efficacy readout, study population (children,
women). Ryabova et al. carried out a study on pregnant adults, pregnant women), study duration (1 to 8 weeks), and
women (45/681). also design (comparative studies, add-on studies, noncom-
Three studies were conducted in Germany, one in Can- parative studies, studies with parallel treatments of the eyes
ada, one in Ukraine, one in Kazakhstan, and the remaining and nose). Only one trial was placebo controlled, and the
8 in Russia. overall number of patients per trial with medium 48 patients
Additional details are listed in Table 1. was rather small. Furthermore, many study details were
missing, e.g., information whether the trial was blinded or
3. Results from the Reviewed Clinical Trials randomized (e.g., Kayb et al. [51]), or only limited informa-
tion was given regarding the presence of adverse effects in
3.1. Safety of Ectoine Nasal Spray. All studies evaluated the most trials. A CONSORT description was also missing in 9
safety of ENS, covering also the very sensitive patient groups of 14 studies, which is in line with the fact that most of the
of children and pregnant women. None of the studies studies were not randomized clinical trials. These limitations8
Table 2: Application of ectoine in combination with drugs compared to treatment with drugs alone. AR: allergic rhinitis; ENS: ectoine nasal spray; GC: glucocorticoid; INS: intranasal
steroids; TNSS: total nasal symptom score.
Author Treatment groups Patient reported outcome (nasal symptom scores) Additional treatment effects observed (nonexhaustive)
Group 1: ENS + oral In group 1, TNSS was reduced from 4:6 ± 0, (day 1) to 0:4 ± 0:1 (day
Reduction of ocular itching was higher for group 1 on day 18 (p = 0:007
antihistamine 21). In group 2, TNSS was reduced from 3:9 ± 0:3 (day 1) to 3:5 ± 0:2
). Conjunctival hyperemia was significantly more severe in group 1 at
(day 21), respectively. The difference between the groups was
Minaeva and baseline and became comparable between the two groups on day 10
significant (p = 0:003)
Shiryaeva, and significantly milder in group 1 on day 19 (p = 0:015). Additional
Group 2: oral Significant differences of single symptoms:
2015 [50] symptomatic medication for rhinitis was used significantly less in
antihistamine For nasal congestion on day 14 (p = 0:01), rhinorrhea on day 15
group 1 (2 out of 30 patients), compared to group 2 (10 out of 20
(p = 0:036), and nasal itching and sneezing on day 17 (p = 0:02), all
patients) (p = 0:002).
favoring group 1.
Group 1: ENS All 3 treatments reduced nasal symptoms (sneezing, itchy nose,
Group 2: ENS + INS discharges, nasal congestion, unpleasant smell, cough, fatigue) Diminution of symptoms (in days) reflected the results from the
Abdulkerimov
significantly (p < 0:05), group 2 had the highest effect, followed by symptom score: In group 2, symptoms diminished faster than in group
et al., 2016 [46]
Group 3: INS group 3, with group 1 having the lowest, but still a significant effect 3, followed by group 1.
against baseline.
Group 1: ENS + In group 1, a positive dynamic of disease symptoms was observed in
standard of care 92.3% (p < 0:05) of mild cases after 2 weeks, and in 60% (p < 0:05) in
group 2. For the moderate form of AR, the efficacy of combined In group 1, intranasal GCs could be stopped at week 4 of observation in
therapy in group 1 was 67% versus 50% in group 2 (p < 0:05). Based on 100% of cases with the mild form of AR and in 81.8% of cases with the
Kayb et al., patient questionnaires, the symptoms in mild AR were down by day 3 moderate form of AR. In group 2, most children with the moderate
2016 [51] Group 2: Standard of to day 5. In group 2, a positive dynamic in AR symptoms was observed form of AR (78.6%) continued to take intranasal GCs intermittently. In
care by day 7. the severe form of AR in children in the group receiving ENS, the dose
After 4 weeks, in both groups, 100% of the mild AR patients were free of intranasal GCs was able to be reduced, in contrast to group 2.
of symptoms. No significant effect was observed in children with mild
or severe AR in both groups.
Group 1: ENS + oral The reduction of AR symptoms was significant for both groups
antihistamine (р < 0:001): patients in group 1 had stronger changes, as their TNSS
In 62% of pediatric patients of group 2, the TNSS drop was more
was reduced from 2:56 ± 0:2 to 0:79 ± 0:1 after 3 weeks of treatment
significant (2-3 points). A similar significant TNSS decrease (2-3
versus 2:92 ± 0:2 to 1:0 ± 0:1 in group 2 (p > 0:05). Before enrolment,
Bardenikova points) in group 1 was only demonstrated in 35% of patients.
patients in group 2 had more severe AR symptoms (2:92 ± 0:2 points)
et al., 2016 [52] Rhinoscopy showed improved results for both groups after treatment.
Group 2: ENS + INS when compared to group 1 (2:56 ± 0:2, р > 0:05), mainly due to nasal
Analysis of the AR control index showed better values in patients in
congestion severity. An overall trend in the direction of a reduction in
group 1.
TNSS during the observation supports the efficacy of both groups
(p < 0:001).
Group 1: ENS + s Interestingly, emotional profiles have been evaluated: analysis
Nasal breathing and mucous secretion were markedly reduced in
standard of care performed in the study demonstrated that the most important feature
group 1. Analysis of nasal itchiness, periodic sneezing, coughing, voice
in the evaluation of emotional conditions was the anxiety level, which
Skosarev et al., changes, and night snoring showed also definite positive trends
was found in percent in 84:9 ± 4:8, 32:4 ± 3:1, and 7:4 ± 0:86 of
2015 [53] Group 2: Standard of (p < 0:001). As for group 2, positive trends but not statistically
patients in group 1 for days 1, 5, and 10 of observation, accordingly. In
care significant differences were shown for the occurrence of itchiness,
group 2, the trend was less prominent: 82:3 ± 5:21, 65:4 ± 3:2, and
periodic sneezing, coughing, voice changes, and night snoring.
12:3 ± 1:61 cases, accordingly.
BioMed Research InternationalTable 3: Studies comparing ectoine nasal spray against other therapy or placebo. AR: allergic rhinitis; AUC: area under the curve; EEC: environmental exposure chamber; EED: ectoine eye
drops; ENS: ectoine nasal spray; GC: glucocorticoid; INS: intranasal steroids; LSMD: least square mean difference; QoL: quality of life; RQLQ: rhinitis quality of life questionnaire; TNNSS:
total nonnasal symptom score; TNSS: total nasal symptom score; TOSS: total nasal symptom score.
Study treatment
Author Treatment effect patient reported outcome (nasal symptom scores) Interesting treatment effect on other parameters (nonexhaustive)
distribution
Group 1: ENS/EED Patients in group 1 had a mean 1.54-fold lower TNSS during
posttreatment EEC exposures than placebo patients, though the TNSS
decreased not only in group 1 but also in group 2 when compared to
baseline. The mean AUC TNSS score was 25:02 ± 0:722 at the EEC
In both treatment groups, the TOSS and TNNSS after EEC exposure in
screening visit, which was significantly reduced to 20:10 ± 1:31 (-19.7%;
comparison to baseline was reduced, but in group 1, we have seen an
BioMed Research International
Salapatek p = 0:0003) in group 1 at the posttreatment EEC visits. In group 2, the
improvement in ARC symptoms: the mean change from baseline AUC of
et al., 2011 Group 2: drop was by 12.2% to 21:96 ± 1:21. Intergroup comparison showed that
TNNSS was also significantly lower in group 1 compared to group 2.
[43] placebo/placebo the mean change from baseline AUC of TNSS for group 1 was 61.2%
Mean cross-sectional areas of the nasal cavity were reduced to a lesser
greater compared to group 2 (LSMD: -4.92 vs. -3.05). This difference
extent in group 1.
showed clinically meaningful improvement in group 1 in comparison to
group 2 but did only approach statistical significance (p = 0:065).
Treatment in group 1 resulted in significantly greater relief of the
symptom “sneezing” (p = 0:020).
Group 1: ENS After 14 days of treatment, in the investigator’s assessment, both groups
According to the patients’ assessment, TNSS values decreased clearly in
showed a significant reduction in TNSS levels.
group 1 (p = 0:072, decrease by -12.86%) and a significant decrease was
Single symptom score and ear/palate itching analysis and QoL
observed in group 2 (p < 0:001, decrease by 39.69%).
Sonnemann questionnaire revealed only significant changes for group 2 for sneezing
In order to study the time of onset of both treatments, TNSS development
et al., 2014 and brushing the nose. In group 1, mean values of 1:09 ± 0:78 (mean
Group 2: INS within the first 12 hours of treatment was analyzed. Both groups showed a
[47] values of entire study period) reflected moderate efficacy assessed by
significant decrease of TNSS from the first site visit until the first patient
patients and a value of 1:44 ± 1:00 showed similar judgment by the
assessment at the end of the first day of treatment (p < 0:001 for both
physicians. In group 2, the efficacy was judged as good by patients
groups).
(1:73 ± 0:94) and as very good by investigators (2:60 ± 0:58).
Group 1: ENS/EED The sum of nasal symptom scores showed a significant decrease from visit
1 to visit 2 (as assessed by physicians): sum scores in group 1 decreased As for nasal symptoms, a clear decrease of the symptom palate itching was
from 20:71 ± 3:52 to 8:52 ± 4:74 (p < 0:001) and sum scores in group 2 observed from visit 1 to visit 2: p = 0:024 for group 1 and p = 0:018 for
Werkhäuser
et al., 2014 Group 2: azelastine decreased from 21:73 ± 3:34 to 9:32 ± 6:24 (p < 0:001). According to the group 2. Values of the patients’ documentation did only reach statistical
nasal spray and eye patients’ assessment, values decreased by 23.05% in group 1 (p = 0:076) significance in group 2 (p < 0:001).
[49]
drops and by 33.14% in group 2 (p = 0:02). All single symptoms (nasal The TOSS decreased significantly from visit 1 to visit 2 in both groups
obstruction, rhinorrhea, sneezing, nasal itching) decreased significantly in (p < 0:001 for group 1, p = 0:009 for group 2).
both groups.
Group 1: ENS According to the physician’s assessment, TNSS scores decreased
significantly for both groups both from visit 1 to visit 2 (p < 0:001) and
The development of the sum of TOSS was assessed by the investigator. It
Werkhäuser from visit 1 to visit 3 (p < 0:001). Scores assessed by patients showed that
Group 2: could be confirmed that ocular symptoms decreased significantly from
et al., 2014 decreases in TNSS from day 1 to day 7 were not significant, whereas
[49] cromoglicate nasal significant decreases in TNSS scores from day 1 to day 14 were shown for visit 1 to visit 2 (p < 0:001 for group 1; p = 0:008 for group 2) as well as
spray from visit 1 to visit 3 (p < 0:001 for group 1; p = 0:003 for group 2).
group 1 (p < 0:001) as well as group 2 (p < 0:001). Single symptom scores
also decreased significantly in both groups.
i-
910
Table 3: Continued.
Study treatment
Author Treatment effect patient reported outcome (nasal symptom scores) Interesting treatment effect on other parameters (nonexhaustive)
distribution
Group 1: ENS + Applying the RQLQ, 81.5% of patients in group 1 scored the treatment
saline solution results as “good,” 15.8% scored the treatment results as “fair,” and only
Kryuchko At the end of the treatment course, overall improvement was achieved for 2.7% continued to use topical antihistamine products due to polyvalent
et al., 2014 both groups but was more prominent in group 1 (improvement of the sensitization and the persistent course of allergic rhinitis. In group 2, a
[55] Group 2: saline TNSS by 4.6 vs. 4.2; p < 0:05). “good” score was achieved for 58% of patients, “fair” score was achieved
solution for 25%, and 17% of pediatric patients had to continue intranasal therapy
due to persistent symptoms.
BioMed Research InternationalBioMed Research International 11
Table 4: Studies applying ectoine nasal spray without comparator. AR: allergic rhinitis; ENS: ectoine nasal spray; ENT: ear-nose-throat; INS:
intranasal steroids; TNSS: total nasal symptom score.
Study treatment Treatment effect patient reported outcome (nasal
Author Additional other treatment effect (nonexhaustive)
distribution symptom scores)
Group 1: ENS The ENT examination showed a decrease in the
(persistent allergic severity of inflammatory events in the nasal cavity
rhinitis) (p < 0:05).
After 10 days of treatment, both groups showed a
Cytological evaluation of nasal secretion in both
significant reduction in complaints: the total
Ryabova et al., groups revealed an increase in the relative count
clinical score developed from 4:6 ± 0:7 points to
2019 [54] Group 2: ENS of eosinophils and the absolute count of
0:7 ± 0:4 points in group 1 and from 5:3 ± 1:0
(intermittent leukocytes. This was mainly due to an increase in
points to 0:4 ± 0:2 points in group 2.
allergic rhinitis) neutrophils.
A significant decrease in the amount of secretory
IgE was observed in group 1 and group 2 (p < 0:05).
Group 1: ENS plus As a result of combination therapy in both groups,
antihistamines a marked decrease in both clinical and laboratory
and/or activities of inflammation was achieved between
cromoglicate visits 1 and 3: a decrease in eosinophil count
A decrease in the severity of AR symptoms on the
(−0:7 ± 0:4 in group 1 and −0:6 ± 0:5 in group 2);
Kamaev et al., TNSS scale in both groups (−3:2 ± 0:4 points in
a decrease in the overall assessment score of the
2015 [48] group 1 and −4:5 ± 0:6 points in group 2) was
rhinocytogram (−1:1 ± 0:6 in group 1 and −0:9
Group 2: ENS + observed.
± 0:5 in group 2); a decrease in the score of AR
INS
exacerbations according to the anterior
rhinoscopy data (−3:1 ± 0:9 in group 1 and −3:6
± 1:1 in group 2).
Most of the patients (20/34) benefited from
treatment with ENS. In 6 out of 34 participants,
Mokronosova the disease worsened and 8 patients expressed no
Group 1: ENS —
et al.,2017 [45] difference. Thus, there were 2.6 and 3.3 times
more patients in whom use of ENS spray led to
decreases in symptoms.
After a week of use of ENS, the range of
Mokronosova eosinophils in the rhinocytogram has not
All patients except one showed a decrease in the changed. However, the average number of
et al., 2019 Group 1: ENS
intensity of all clinical symptoms of AR. eosinophils tended to decrease from 29% ± 9% to
[44]
22% ± 10%:
nfluence the quality of the studies, resulting in an average “over the counter” treatment regimens. These results are in
Jadad score of 1-2 points (see Table 1). line with those from the other studies reviewed here. Salapa-
The differences in study designs impede to cluster and tek et al. [43] proved in their placebo-controlled trial that
meta-analyze the data. Nevertheless, the 14 selected trials hallmark symptoms of AR can be significantly improved by
show a clear picture on the potential efficacy/effectiveness monotherapy with ENS.
and safety of ectoine nasal spray in the treatment of allergic Results of the study conducted by Abdulkerimov et al.
rhinitis. [46] demonstrated that treatment with ENS alone improved
nasal symptoms significantly, but it was less effective than
4.2. Monotherapy with Ectoine. Results from real-life studies treatment with INS alone. Likewise, results from the study
constitute an important element of evidence-based medicine conducted by Sonnemann et al. [47] confirmed that ENS is
since they reflect the effectiveness of the treatment with all less effective than beclomethasone nasal spray. Given that
the confounding factors as per routine medical practice. INS are the most efficacious pharmacological treatment for
Eichel et al. [40] conducted a meta-analysis of four clinical allergic rhinoconjunctivitis [30], it is not surprising that the
trials comparing ectoine to azelastine [49], cromoglicic acid effectiveness of ENS alone, which still showed an impressive
[49], beclomethasone [47], and placebo. These studies were >50% symptom improvement, does not match up to that of
also included in the review presented here. Results from the INS.
meta-analysis by Eichel and colleagues show that, after seven Mokronosova et al. showed in 2 studies that treatment for
days of treatment with ectoine nasal spray, both nasal and 14 days with ENS resulted in successful treatment of 58.8%
ocular symptoms were significantly alleviated and an espe- and >90% of patients, respectively [44, 45]. According to
cially marked improvement was observed in the symptom Abdulkerimov et al. [46], significant nasal symptom relief
of nasal obstruction. The authors concluded that the was evident within 18 to 21 days in moderate-to-severe rhini-
effectiveness of ectoine was noninferior to that of standard tis patients who underwent treatment with ENS. According12 BioMed Research International
to Sonnemann et al., ENS reduced the nasal symptoms of cromoglicate, and/or INS), in which monotherapy using
mild-moderate patients already significantly within the first either ectoine or pharmacotherapy was used as a comparator.
day of treatment [47]. Furthermore, it has been shown in Regardless of treatment regimens, combination therapy with
other trials that patients with severe rhinitis symptoms are ENS consistently elicited not only greater but also faster
difficult to treat. Even with the most effective intranasal for- symptom relief than did antihistamine alone and INS alone
mulation, combined azelastine and fluticasone furoate, [46, 50, 51]. In the study by Minaeva and Shiryaeva [50],
patients with moderate-to-severe allergic rhinitis showed a rel- treatment with oral antihistamine alone showed only modest
atively low responder rate of 12.4% [56] or 16.7% [57] after 14 effects in children and adolescents with mild-to-moderate
days of treatment. In general, only 30.3% of grass pollen- symptoms of allergic rhinitis, whereas those applying ENS
allergic patients and 54.3% of those suffering from birch pollen additionally were mostly “cured” after treatment end.
allergy attain symptom control with guideline-concordant According to Abdulkerimov et al. [46] and Bardenikova
pharmacotherapy [58]. All studies investigating a monother- et al. [52], ENS improved the effectiveness of INS. The study
apy with ectoine invariably attested positive effects of ectoine of Abdulkerimov et al. was of particular interest to us as the
monotherapy in alleviating symptoms of allergic rhinitis. Tak- combination of ectoine and INS showed the best treatment
ing the baseline symptom scores into consideration, these effect in difficult-to-treat patients with moderate-to-severe
results permit the conclusion that patients with mild-to- rhinitis symptoms. This trend was also observed for the most
moderate symptoms could be successfully treated with ectoine effective intranasal formulation (azelastine and fluticasone
alone; however, monotherapy with ectoine should not be con- furoate) in patients with moderate-to-severe rhinitis who
sidered in patients with severe symptoms. In head-to-head exhibited complete or near-complete symptom relief faster
comparison studies, ectoine was proven superior to isotonic than those receiving either fluticasone furoate or azelastine
(sea) salt solutions [43], equivalent to antihistamines (azelas- alone [46].
tine) and cromoglicic acid [49] but less effective than INS Compared to the combinations of antihistamines with
(beclomethasone, mometasone, fluticasone) [46, 47]. INS or nasal decongestants with INS, the advantages of the
combination with ENS lie in its excellent tolerability and
4.3. Combination Therapy with Ectoine. In accordance with safety profile, given that most pharmacological drugs are
various guidelines, combination therapy is commonly used associated with considerable local irritations and side effects
to treat allergic rhinitis. A large-scale, real-world survey on [65, 66]. For instance, it is well known that oxymetazoline
the prescribing behavior of UK physicians showed that 20- might trigger rhinitis medicamentosa, and intranasal steroids
40% of patients who used monotherapy with antihistamines might cause stunted growth in children [65, 67]. The combi-
at the beginning of the pollen season and 25-50% of those nation of fluticasone furoate and azelastine is not indicated
who used INS used add-on therapy during the pollen season for patients under 12 years old because of lack of correspond-
[36]. In patient-based surveys, the percentage of patients who ing data, but the combination of ectoine and antihistamine is
used both, prescription and nonprescription products, was suitable for children, as shown by different studies [50–53].
higher (53.0-70.4%), because patients commonly purchase Taken together, the increased effectiveness and time
symptomatic medication for allergic rhinitis over the counter advantage observed in the combination therapy with ectoine
in addition to the prescribed drugs [59–61]. These figures were consistent across all studies described above. Thus,
warrant the search for an effective treatment combination ectoine can be deemed a safe and effective add-on to
for patients who suffer from rhinitis symptoms despite the guideline-concordant therapy with antihistamines, cromo-
use of first-line therapy. glicic acid, or INS.
Evidence supports the use of combination therapy in
allergic rhinitis, specifically combinations of pharmacological
4.4. Concomitant Use of Ectoine Eye Drops. In two of the
drugs. The combination of oxymetazoline and mometasone
selected studies [43, 49], ectoine-containing eye drops were
furoate nasal spray showed greater reductions in allergic rhi-
applied together with the ENS in order to treat ocular symp-
nitis symptoms than mometasone furoate nasal spray alone
toms (allergic rhinoconjunctivitis). Results showed signifi-
[62]. Likewise, the combination of oxymetazoline and flutica-
cant and clinically relevant improvement of allergic ocular
sone furoate was also superior to both monotherapies [63].
symptoms such as watery eyes and itching. Although this
Greiwe and Bernstein [64] conducted a systemic review of
review concentrates on allergic rhinitis and ectoine nasal
combination pharmacotherapy for rhinitis: they concluded
spray, it is worth to mention that these results are in line with
that two combinations—intranasal antihistamine (azelas-
other studies showing positive effects of ectoine-based eye
tine) with INS and INS with nasal decongestants—are advan-
drops for the treatment of allergic conjunctivitis [68–71].
tageous for patients with complex rhinitis symptoms in terms
of symptom control and a preponderance of benefit over
harm. The ARIA guidelines 2016 revision recommends the 4.5. Treatment of Sensitive Patient Groups. A total of seven
combination of intranasal/oral antihistamines and INS for studies examined the effects of ectoine nasal spray in the very
patients with seasonal allergic rhinitis; the combination of sensitive patient groups of children and adolescents (6 stud-
INS and intranasal antihistamines acts faster than INCS ies, [48, 50–53, 55]) and pregnant women (1 trial, [54]).
alone and thus might be preferred by patients [31]. The results show that ENS shows efficacy/effectiveness in
We reviewed five studies investigating ENS (nonpharma- these sensitive patient groups and combines this with its
cotherapy) as add-on to pharmacotherapy (antihistamine, excellent safety profile of a nonpharmacological treatment.BioMed Research International 13
5. Conclusions Ethical Approval
In this review, we provide evidence based on the review of 14 Ethical approval is not applicable.
independent studies from 4 countries that patients with
mild-to-moderate symptoms of allergic rhinitis can be suc- Consent
cessfully treated with ectoine-containing nasal spray. ENS
alone exerts noninferior effects compared to first-line ther- Consent is not applicable.
apy such as antihistamines and cromoglicic acid. Using
ENS as an add-on therapy to antihistamines or INS acceler-
Disclosure
ated symptom relief by up to 7 days. This combination
strategy was proven to be beneficial in a group of difficult- All authors had full access to all of the data in this study and
to-treat patients suffering from moderate-to-severe rhinitis take complete responsibility for the integrity of the data and
symptoms. accuracy of the data analysis.
This review of 14 studies extends our knowledge about
the substance ectoine and their potential applicability in the
treatment of allergic rhinitis by providing mainly patient-
Conflicts of Interest
reported outcomes in real-world settings under different AB reports personal fees from bitop AG. NW is an employee
regional settings with different allergen exposure, standard of bitop AG. RM reports personal fees from ALK, grants
of care, and different patient groups including very sensitive from ASIT biotech, personal fees from Allergopharma, per-
patient groups. Especially, the combination of different treat- sonal fees from Allergy Therapeutics, grants and personal
ment approaches like ectoine treatment in combination with fees from Bencard, grants from Leti, grants, personal fees
other medications (such as antihistamines or INS) showed and nonfinancial support from Lofarma, nonfinancial sup-
additional potential for increased efficacy in patients with port from Roxall, grants and personal fees from Stallergenes,
allergic rhinitis. grants from Optima, personal fees from Friulchem, personal
Although the studies have their limitations in design, fees from Hexal, personal fees from Servier, personal fees
patient number, and reporting, the following final conclusion from Klosterfrau, nonfinancial support from Atmos, per-
can be made: ectoine is a natural substance with an excellent sonal fees from Bayer, nonfinancial support from Bionorica,
tolerability and safety profile and thus is maybe a viable alter- personal fees from FAES, personal fees from GSK, personal
native for allergic rhinitis patients who wish to avoid local fees from MSD, personal fees from Johnson & Johnson, per-
reactions and side effects associated with pharmacological sonal fees from Meda, personal fees and nonfinancial support
therapy. Larger scale controlled and randomized studies from Novartis, nonfinancial support from Otonomy, per-
would be desirable to further verify the obtained results. sonal fees from Stada, personal fees from UCB, nonfinancial
support from Ferrero, grants from bitop AG, grants from
Abbreviations Hulka, personal fees from Nuvo, and grants from Ursa-
pharm, outside the submitted work.
ACT: Asthma control test
AE: Adverse event
AR: Allergic rhinitis
Authors’ Contributions
ASIT: Allergen specific immunotherapy AB performed the review, evaluated the data, and wrote the
ARIA: Allergic Rhinitis and its Impact on Asthma manuscript together with NW and RM. All authors approved
AUC: Area under the curve the final version of the manuscript before submission.
EEC: Environmental exposure chamber
EED: Ectoine eye drops
ENS: Ectoine nasal spray Acknowledgments
ENT: Ear-nose-throat The authors are grateful to Anja Heinrich (bitop AG) for her
GC: Glucocorticoid valuable comments on the manuscript as well as Dr. Esther
INS: Intranasal glucocorticosteroids Raskopf (ClinCompetence Cologne GmbH) for her editorial
LSMD: Least square mean difference assistance. Sponsorship for the article processing charges
QoL: Quality of life were funded by bitop AG.
RQLQ: Rhinitis quality of life questionnaire
SAE: Serious adverse event
TNSS: Total nasal symptom score References
TNNSS: Total nonnasal symptom score
[1] A. Bownik and Z. Stepniewska, “Ectoine as a promising pro-
TOSS: Total ocular symptom score. tective agent in humans and animals,” Arhiv za higijenu rada
i toksikologiju, vol. 67, no. 4, pp. 260–265, 2016.
Data Availability [2] G. Lentzen and T. Schwarz, “Extremolytes: natural com-
pounds from extremophiles for versatile applications,” Applied
Data sharing is not applicable to this article as no datasets Microbiology and Biotechnology, vol. 72, no. 4, pp. 623–634,
were generated or analyzed during the current study. 2006.14 BioMed Research International
[3] G. Zaccai, I. Bagyan, J. Combet et al., “Neutrons describe [17] H. Abdel-Aziz, W. Wadie, D. M. Abdallah, G. Lentzen, and
ectoine effects on water H-bonding and hydration around a M. T. Khayyal, “Novel effects of ectoine, a bacteria-derived
soluble protein and a cell membrane,” Scientific Reports, natural tetrahydropyrimidine, in experimental colitis,” Phyto-
vol. 6, no. 1, article 31434, 2016. medicine, vol. 20, no. 7, pp. 585–591, 2013.
[4] E. A. Galinski, M. Stein, B. Amendt, and M. Kinder, “The kos- [18] A. Marini, K. Reinelt, J. Krutmann, and A. Bilstein, “Ectoine-
motropic (structure-forming) effect of compensatory solutes,” containing cream in the treatment of mild to moderate atopic
Comparative Biochemistry and Physiology Part A: Physiology, dermatitis: a randomised, comparator-controlled, intra-
vol. 117, no. 3, pp. 357–365, 1997. individual double-blind, multi-center trial,” Skin Pharmacol-
[5] T. Arakawa and S. N. Timasheff, “The stabilization of proteins ogy and Physiology, vol. 27, no. 2, pp. 57–65, 2014.
by osmolytes,” Biophysical Journal, vol. 47, no. 3, pp. 411–414, [19] D. Müller, T. Lindemann, K. Shah-Hosseini et al., “Efficacy
1985. and tolerability of an ectoine mouth and throat spray com-
[6] M. B. Hahn, T. Solomun, R. Wellhausen et al., “Influence of pared with those of saline lozenges in the treatment of acute
the compatible solute ectoine on the local water structure: pharyngitis and/or laryngitis: a prospective, controlled, obser-
implications for the binding of the protein G5P to DNA,” vational clinical trial,” European Archives of Oto-Rhino-Laryn-
The Journal of Physical Chemistry B, vol. 119, no. 49, gology, vol. 273, no. 9, pp. 2591–2597, 2016.
pp. 15212–15220, 2015. [20] V.-A. Dao, S. Overhagen, A. Bilstein, C. Kolot, U. Sonnemann,
[7] J. Smiatek, R. K. Harishchandra, O. Rubner, H. J. Galla, and and R. Mösges, “Ectoine lozenges in the treatment of acute
A. Heuer, “Properties of compatible solutes in aqueous solu- viral pharyngitis: a prospective, active-controlled clinical
tion,” Biophysical Chemistry, vol. 160, no. 1, pp. 62–68, 2012. study,” European Archives of Oto-Rhino-Laryngology,
vol. 276, no. 3, pp. 775–783, 2019.
[8] A. Roychoudhury, D. Haussinger, and F. Oesterhelt, “Effect of
[21] B. H. Tran, V. A. Dao, A. Bilstein, K. Unfried, K. Shah-Hos-
the compatible solute ectoine on the stability of the membrane
seini, and R. Mosges, “Ectoine-containing inhalation solution
proteins,” Protein and Peptide Letters, vol. 19, no. 8, pp. 791–
versus saline inhalation solution in the treatment of acute
794, 2012.
bronchitis and acute respiratory infections: a prospective, con-
[9] R. K. Harishchandra, S. Wulff, G. Lentzen, T. Neuhaus, and trolled, observational study,” BioMed Research International,
H. J. Galla, “The effect of compatible solute ectoines on the vol. 2019, Article ID 7945091, 8 pages, 2019.
structural organization of lipid monolayer and bilayer mem-
[22] M. Casale, A. Moffa, S. Carbone et al., “Topical Ectoine: a
branes,” Biophysical Chemistry, vol. 150, no. 1-3, pp. 37–46,
promising molecule in the upper airways inflammation—a
2010.
systematic review,” BioMed Research International, vol. 2019,
[10] L. Czech, L. Hermann, N. Stöveken et al., “Role of the extremo- 10 pages, 2019.
lytes ectoine and hydroxyectoine as stress protectants and [23] U. Sonnemann, O. Scherner, and N. Werkhäuser, “Treatment
nutrients: genetics, phylogenomics, biochemistry, and struc- of rhinitis sicca anterior with ectoine containing nasal spray,”
tural analysis,” Genes, vol. 9, no. 4, p. 177, 2018. Journal of Allergy, vol. 2014, Article ID 273219, 10 pages,
[11] M. Kroker, U. Sydlik, A. Autengruber et al., “Preventing car- 2014.
bon nanoparticle-induced lung inflammation reduces [24] V. A. Dao, A. Bilstein, S. Overhagen, L. Géczi, Z. Baráth, and
antigen-specific sensitization and subsequent allergic reactions R. Mösges, “Effectiveness, tolerability, and safety of ectoine-
in a mouse model,” Particle and Fibre Toxicology, vol. 12, no. 1, containing mouthwash versus those of a calcium phosphate
p. 20, 2015. mouthwash for the treatment of chemotherapy-induced oral
[12] H. Peuschel, U. Sydlik, S. Grether-Beck et al., “Carbon nano- mucositis: a prospective, active-controlled, non-
particles induce ceramide- and lipid raft-dependent signalling interventional study,” Oncology and Therapy, vol. 6, no. 1,
in lung epithelial cells: a target for a preventive strategy against pp. 59–72, 2018.
environmentally-induced lung inflammation,” Particle and [25] K. Unfried, U. Krämer, U. Sydlik et al., “Reduction of neutro-
Fibre Toxicology, vol. 9, no. 1, p. 48, 2012. philic lung inflammation by inhalation of the compatible sol-
[13] H. Peuschel, U. Sydlik, J. Haendeler et al., “c-Src-mediated ute ectoine: a randomized trial with elderly individuals,”
activation of Erk 1/2 is a reaction of epithelial cells to carbon International Journal of Chronic Obstructive Pulmonary Dis-
nanoparticle treatment and may be a target for a molecular ease, vol. 11, pp. 2573–2583, 2016.
preventive strategy,” Biological Chemistry, vol. 391, no. 11, [26] A. Moffa, S. Carbone, A. Costantino et al., “Potential role of
pp. 1327–1332, 2010. topical ectoine for prevention of pediatric upper respiratory
[14] U. Sydlik, I. Gallitz, C. Albrecht, J. Abel, J. Krutmann, and tract infection: a preliminary observational study,” Journal of
K. Unfried, “The compatible solute ectoine protects against Biological Regulators and Homeostatic Agents, vol. 33, no. 6,
nanoparticle-induced neutrophilic lung inflammation,” Amer- pp. 1935–1940, 2019.
ican Journal of Respiratory and Critical Care Medicine, [27] P. Allegri, G. Marrazzo, C. Ciurlo, A. Mastromarino,
vol. 180, no. 1, pp. 29–35, 2009. S. Autuori, and U. Murialdo, Eds., Retrospective study to eval-
[15] K. Unfried, M. Kroker, A. Autengruber, M. Gotic, and uate the efficacy on vernal kerat-conjunctivis (VKC) of 2%
U. Sydlik, “The compatible solute ectoine reduces the exacer- ectoine versus 0, 05% ketofinen eye drops, ARVO, 2014.
bating effect of environmental model particles on the immune [28] R. Pawankar, G. W. Canonica, S. T. Holgate, R. F. Lockey,
response of the airways,” Journal of Allergy, vol. 2014, Article M. S. Blaiss, and WAO, White Book on Allergy: Update 2013
ID 708458, 7 pages, 2014. Executive Summary, 2013.
[16] U. Sydlik, H. Peuschel, A. Paunel-Görgülü et al., “Recovery of [29] T. Zuberbier, J. Lotvall, S. Simoens, S. V. Subramanian, and
neutrophil apoptosis by ectoine: a new strategy against lung M. K. Church, “Economic burden of inadequate management
inflammation,” The European Respiratory Journal, vol. 41, of allergic diseases in the European Union: a GA (2) LEN
no. 2, pp. 433–442, 2013. review,” Allergy, vol. 69, no. 10, pp. 1275–1279, 2014.You can also read