REVIEW ARTICLE Ten years of the Helsinki Declaration on patient safety in anaesthesiology An expert opinion on peri-operative safety aspects - ESAIC
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Eur J Anaesthesiol 2020; 37:521–610
REVIEW ARTICLE
Ten years of the Helsinki Declaration on patient safety
in anaesthesiology
An expert opinion on peri-operative safety aspects
Benedikt Preckel, Sven Staender, Daniel Arnal, Guttorm Brattebø, Jeffrey M. Feldman,
Downloaded from https://journals.lww.com/ejanaesthesiology by BhDMf5ePHKav1zEoum1tQfN4a+kJLhEZgbsIHo4XMi0hCywCX1AWnYQp/IlQrHD36ls6+OKM7O0UQRQJ620i51SJqzxYvZd0xNNLNiqjBK5FVF0Vcb6X/Q== on 07/02/2020
Robert Ffrench-O’Carroll, Thomas Fuchs-Buder, Sara N. Goldhaber-Fiebert, Guy Haller,
Arvid S. Haugen, Jan F.A. Hendrickx, Cor J. Kalkman, Patrick Meybohm, Christopher Neuhaus,
Doris Østergaard, Adrian Plunkett, Hans U. Schüler, Andrew F. Smith, Michel M.R.F. Struys,
Christian P. Subbe, Johannes Wacker, John Welch, David K. Whitaker, Kai Zacharowski
and Jannicke Mellin-Olsen
Patient safety is an activity to mitigate preventable patient harm are celebrating the 10th anniversary of the Helsinki Declaration
that may occur during the delivery of medical care. The Euro- on Patient Safety in Anaesthesiology; a good opportunity to look
pean Board of Anaesthesiology (EBA)/European Union of back and forward evaluating what was achieved in the recent 10
Medical Specialists had previously published safety recommen- years, and what needs to be done in the upcoming years. The
dations on minimal monitoring and postanaesthesia care, but Patient Safety and Quality Committee (PSQC) of ESA invited
with the growing public and professional interest it was decided experts in their fields to contribute, and these experts addressed
to produce a much more encompassing document. The EBA their topic in different ways; there are classical, narrative
and the European Society of Anaesthesiology (ESA) published reviews, more systematic reviews, political statements, personal
a consensus on what needs to be done/achieved for improve- opinions and also original data presentation. With this publica-
ment of peri-operative patient safety. During the Euroanaesthe- tion we hope to further stimulate implementation of the Helsinki
sia meeting in Helsinki/Finland in 2010, this vision was Declaration on Patient Safety in Anaesthesiology, as well as
presented to anaesthesiologists, patients, industry and others initiating relevant research in the future.
involved in health care as the ‘Helsinki Declaration on Patient
Safety in Anaesthesiology’. In May/June 2020, ESA and EBA Published online 1 June 2020
From the Department of Anaesthesiology, Amsterdam University Medical Centers, Academic Medical Center (AMC), Amsterdam, The Netherlands (BP), Institute for
Anaesthesia and Intensive Care Medicine, Spital Männedorf AG, Männedorf, Switzerland (SS), Department of Anaesthesiology, Perioperative Medicine and Intensive Care,
Paracelsus Medical University Salzburg, Salzburg, Austria (SS), Department of Anaesthesiology and Critical Care, University Hospital Fundaci on Alcorc
on Madrid, Spain
(DA), Department of Anaesthesia and Intensive Care, Haukeland University Hospital (GB, ASH), Department of Clinical Medicine, University of Bergen, Bergen, Norway
(GB), Department of Anesthesiology and Critical Care Medicine, Perelman School of Medicine, Children’s Hospital of Philadelphia, University of Pennsylvania, Philadelphia,
Pennsylvania, USA (JMF), Anaesthetic Department, St James’s Hospital, Dublin, Ireland (RF-OC), Department of Anesthesiology & Critical Care, University de Lorraine,
CHRU Nancy, Brabois University Hospital, Nancy, France (TF-B), Department of Anesthesiology, Perioperative and Pain Medicine, Stanford University School of Medicine,
Stanford, California, USA (SNG-F), Department of Anaesthesiology, Geneva University Hospitals, Geneva, Switzerland (GH), Department of Epidemiology and Preventive
Medicine, Monash University, Melbourne, Victoria, Australia (GH), Department of Anesthesiology, Onze-Lieve-Vrouwziekenhuis Hospital Aalst, Aalst, Belgium (JFAH),
Division of Anesthesiology, Intensive Care and Emergency Medicine, University Medical Center Utrecht, Utrecht, The Netherlands (CJK), Department of Anesthesiology,
Intensive Care Medicine & Pain Therapy, University Hospital Frankfurt, Frankfurt (PM, KZ), Department of Anaesthesiology, University Hospital Würzburg, Würzburg (PM),
Department of Anesthesiology, University Hospital Heidelberg, Heidelberg, Germany (CN), Copenhagen Academy for Medical Education and Simulation (DØ), Faculty of
Health and Medical Sciences, University of Copenhagen, Copenhagen, Denmark (DØ), Paediatric Intensive Care Unit, Birmingham Women’s and Children’s NHS
Foundation Trust, Birmingham, UK (AP), Product Management Anesthesiology, Drägerwerk AG & Co. KGaA, Lübeck, Germany (HUS), Department of Anaesthesia, Royal
Lancaster Infirmary, Lancaster, UK (AFS), Department of Anaesthesiology, University Medical Center Groningen, University of Groningen, Groningen, The Netherlands
(MMRFS), Department of Basic and Applied Medical Sciences, Ghent University, Ghent, Belgium (MMRFS), Department of Acute Medicine, Ysbyty Gwynedd Hospital,
Bangor, UK (CPS), School of Medical Science, Bangor University, Bangor, UK (CPS), Institute of Anaesthesia and Intensive Care IFAI, Hirslanden Clinic, Zurich,
Switzerland (JWa), Department of Critical Care, University College Hospital, London (JWe), Department of Anaesthesia, Manchester Royal Infirmary, Manchester, UK
(DKW) and Department of Anaesthesia and Intensive Care Medicine, Baerum Hospital, Sandvika, Norway (JM-O)
Correspondence to Benedikt Preckel, Department of Anaesthesiology, Amsterdam University Medical Centers, Academic Medical Center (AMC), Meibergdreef 9, 1105
AZ Amsterdam, The Netherlands
E-mail: b.preckel@amsterdamumc.nl
0265-0215 Copyright ß 2020 European Society of Anaesthesiology. All rights reserved. DOI:10.1097/EJA.0000000000001244
Copyright © European Society of Anaesthesiology. Unauthorized reproduction of this article is prohibited.
522 Preckel et al.
Table of Contents
Introduction (Arnal, Preckel) ..................................................................................................................................... p 522
Chapter 1: Implementation of the Helsinki Declaration on patient safety in anaesthesiology: past activities,
current European perspectives and future opportunities (Ffrench-O’Carroll, Smith) .................... p 524
Chapter 2: How to define and adequately measure peri-operative patient safety (Haller) ............................... p 531
Chapter 3: Speaking up as a vital part of a safety culture (Brattebø, Whitaker) ................................................ p 536
Chapter 4: Learning from Excellence and Safety-II: reframing patient safety (Plunkett) ................................ p 541
Chapter 5: Safety from the patient’s perspective (Mellin-Olsen) ......................................................................... p 545
Chapter 6: Teaching patient safety the project consisted of an online survey of ESA members to determine
what aspects of professional practice (Wacker, Staender) ................................................................... p 547
Chapter 7: Multidisciplinary simulation for patient safety training: putting human factors theory into action
(Neuhaus) .................................................................................................................................................. p 552
Chapter 8: Care transitions, handovers and continuity of peri-operative medical care: recent developments
and how to train residents and staff (Østergaard) ................................................................................ p 555
Chapter 9: Incident reporting in complexity (Staender) ........................................................................................ p 555
Chapter 10: Supporting healthcare individuals and teams after an adverse event: the care for the second
victim (Staender) .................................................................................................................................... p 560
Chapter 11: The role of checklists in peri-operative care (Haugen) .................................................................... p 561
Chapter 12: Emergency manuals as cognitive aids: from simulations to clinical implementations and uses
(Goldhaber-Fiebert) ............................................................................................................................... p 568
Chapter 13: Anaesthetic monitoring recommendations during general anaesthesia: how consistent are they
across the globe? (Hendrickx, Feldman, Schüler) ............................................................................. p 570
Chapter 14: Avoiding failure-to-rescue: rapid response systems (Subbe, Welch) ............................................... p 575
Chapter 15: Diagnosing the deteriorating patient: remote monitoring on the ward and beyond
(Preckel, Kalkman) ................................................................................................................................ p 579
Chapter 16: Standardisation of the ‘Cardiac Arrest Call’ telephone number 2222 (Whitaker) ......................... p 583
Chapter 17: Safe medication administration in anaesthesia practice: new developments (Whitaker) .............. p 586
Chapter 18: Safe sedation: where are we today? (Fuchs-Buder, Struys) .............................................................. p 592
Chapter 19: Patient Blood Management: an update of its effects on patient safety
(Meybohm, Zacharowski) ...................................................................................................................... p 594
References ..................................................................................................................................................................... p 597
Introduction (Arnal, Preckel) the source of the term ‘Patient Safety’ itself.5 Anaesthesia
‘Anaesthesiologists have a unique, cross-speciality oppor- care has become quite safe: an analysis of national registry
tunity to influence the safety and quality of patient care’.1 data from the United States revealed for the years 1999 to
The central role of anaesthesiologists in the acute and 2005 an estimated rate for anaesthesia-related death of 1.1
surgical patient; the safety improvements in anaesthetic per million population per year, and 8.2 per million hospital
practice, with more than 10-fold decrease of anaesthesia surgical discharges.6 However, huge regional differences
mortality since 1970 and the pioneering interest in the exist, and anaesthesia-related mortality is much higher in
topic have made anaesthesiology the leading medical low-income and middle-income countries.7,8 This differ-
speciality for addressing patient safety issues.2–4 In the ence becomes even more important if we recognise that
1999 Institute of Medicine report ‘To Err is Human’, availability of surgery is unequally distributed in the world,
Anaesthesiology rightly received the recognition it with the expectation that surgery will increase in the lower
deserved as the original leader in patient safety, and even income countries during the next decades.9
Eur J Anaesthesiol 2020; 37:521–610
Copyright © European Society of Anaesthesiology. Unauthorized reproduction of this article is prohibited.
Ten years Helsinki Declaration 523
Which risks for patient safety do we face in anaesthesiol- Anaesthesiology is the key speciality in medicine to take
ogy? today Previous publications have shown that even up responsibility for achieving the goals listed below
in high-income countries, 44 to 54% of peri-operative which will notably improve Patient Safety in Europe.
‘adverse events’ are preventable. Factors like increased
pressure on throughput, along with reduced medical Heads of agreement
staff, new drugs and devices, sicker patients, as well as (1) Patients have a right to expect to be safe and
more complex procedures all increase the opportunity for protected from harm during their medical care and
errors in our work. Are we now paying the price for the anaesthesiology has a key role to play in improving
success from previous years? Chantler10, already in 1999, patient safety peri-operatively. To this end we fully
said that ‘Medicine used to be simple, ineffective and endorse the World Federation of Societies of
relatively safe. Now it is complex, effective and potentially Anaesthesiologists International Standards for a Safe
dangerous’. Surgical and anaesthesia safety was for a long Practice of Anaesthesia.
time unrecognised as a public health issue and for numer- (2) Patients have an important role to play in their safe
ous safety topics we still lack evidence-based data. For care which they should be educated about and given
years, medical staff and policy makers failed to use opportunities to provide feedback to further improve
existing safety know-how from industry in healthcare the process for others.
systems.11 (3) The funders of health care have a right to expect that
peri-operative anaesthesia care will be delivered
Patient safety is an activity to mitigate preventable
safely and therefore they must provide appropriate
patient harm that may occur during the delivery of
resources.
medical care. The European Board of Anaesthesiology
(4) Education has a key role to play in improving patient
(EBA)/European Union of Medical Specialists (UEMS)
safety, and we fully support the development,
had previously published safety recommendations on
dissemination and delivery of patient safety training.
Minimal Monitoring and Postanaesthesia Care, but
(5) Human factors play a large part in the delivery of safe
with the growing public and professional interest it
care to patients, and we will work with our surgical,
was decided to produce a much more encompassing
nursing and other clinical partners to reliably
document.12,13 The EBA and the European Society of
provide this.
Anaesthesiology (ESA) published a consensus on what
(6) Our partners in industry have an important role to
needs to be done/achieved for improvement of peri-
play in developing, manufacturing and supplying safe
operative patient safety. During the Euroanaesthesia
drugs and equipment for our patients’ care.
meeting in 2010, taking place in Helsinki, Finland, this
(7) Anaesthesiology has been a key speciality in
vision was presented to anaesthesiologists, patients,
medicine leading the development of patient safety.
industry and others involved in health care as the
We are not complacent and know there are still more
‘Helsinki Declaration on Patient Safety in Anaesthesi-
areas to improve through research and innovation.
ology’.1
(8) No ethical, legal or regulatory requirement should
This Declaration represents a shared opinion of what reduce or eliminate any of the protections for safe
currently is worth doing and practical to improve patient care set forth in this Declaration.
safety. There are eight ‘Heads of Agreement’ and seven
‘Principal Requirements’. Principal requirements
(1) All institutions providing peri-operative anaesthesia
Helsinki Declaration on patient safety in care to patients (in Europe) should comply with the
anaesthesiology minimum standards of monitoring recommended by
Background the EBA, both in operating theatres and in
Anaesthesiology shares responsibility for quality and recovery areas.
safety in Anaesthesia, Intensive Care, Emergency Medi- (2) All such institutions should have protocols and the
cine and Pain Medicine, including the whole peri-opera- necessary facilities for managing the following:
tive process and also in many other situations inside and (a) Pre-operative assessment and preparation
outside the hospital where patients are at their most (b) Checking equipment and drugs
vulnerable.1 (c) Syringe labelling
(d) Difficult/failed intubation
(1) Around 230 million patients undergo anaesthesia for (e) Malignant hyperpyrexia
major surgery in the world every year. Seven million (f) Anaphylaxis
develop severe complications associated with these (g) Local anaesthetic toxicity
surgical procedures from which one million die (h) Massive haemorrhage
(200 000 in Europe).1 All involved should try to (i) Infection control
reduce this complication rate significantly. (j) Postoperative care, including pain relief
Eur J Anaesthesiol 2020; 37:521–610
Copyright © European Society of Anaesthesiology. Unauthorized reproduction of this article is prohibited.
524 Preckel et al.
(3) All institutions providing sedation to patients must years ago were not as prevalent as today in the clinical
comply with anaesthesiology recognised sedation practice. Of course, the list of safety topics covered by the
standards for safe practice. following chapters is not – and cannot be – exhaustive.
(4) All institutions should support the WHO Safe The reader will learn that there has been enormous prog-
Surgery Saves Lives initiative and checklist. ress and developments regarding safety tools, but it will
(5) All departments of anaesthesiology in Europe must be also be mentioned that in given areas we urgently need
able to produce an annual report of measures taken and more valuable research data. Randomised clinical trials are
results obtained in improving patient safety locally. often difficult to perform in safety topics, and newer
(6) All institutions providing anaesthesiological care to strategies might offer opportunities.15 Methods other than
patients must collect the required data to be able to clinical trials can also illuminate safety.16
produce an annual report on patient morbidity
and mortality. As this experts’ opinion compilation emanates from the
(7) All institutions providing anaesthesiological care to 10th anniversary of the Helsinki Declaration, we start by
patients must contribute to the recognised national or presenting the state of its implementation and a reflection
other major audits of safe practice and critical on the role that the Declaration has meant in the past and
incident reporting systems. Resources must be can be foreseen in the future. Following this initial chapter,
provided to achieve this. we present a mixture of a selection of Helsinki Declaration
principal requirement updates (pre-operative assessment,
incident reporting, medication safety (beyond the syringe
Conclusion labelling), monitoring standards and safe sedation) a col-
This Declaration emphasises the key role of anaesthesi- lection of chapters related to human factors (speak up,
ology in promoting safe peri-operative care. multidisciplinary simulation, handovers and cognitive
aids, exhibiting the growth of knowledge and relevance
Continuity of this Helsinki Declaration ‘head of agreement’ in the last
We invite anyone involved in health care to join us and decade); and a compendium of relevant topics to patient
sign up to this Declaration. safety that have become more relevant since the Declara-
tion was launched and that were not specifically addressed
We will reconvene to review our progress annually to
in 2010 but we consider necessary to include in 2020
implement this Declaration.
(Learning from Excellence (LfE), the patient perspective,
The presidents of EBA/UEMS, ESA and the chairperson patient safety teaching, second victim support, failure to
of the National Anesthesia Society Committee on behalf of rescue and patient blood management (PBM)). Displaying
the ESA Member Societies signed the Declaration in all these chapters in the order just presented would proba-
Helsinki on 12 June 2010. The Declaration was immedi- bly send the false message of having old and new topics.
ately endorsed by several international and national orga- We have, therefore, mixed them in a varied and eclectic
nisations/societies. Meanwhile, anaesthesia societies all hierarchy-free distribution.
over the world signed the Declaration (https://www.esah-
The experts addressed their specific topic: the reader will
q.org/uploads/media/ESA/Files/Downloads/Resources-
find classical reviews, more systematic reviews, political
PatientSafety-MapHelsinkiDeclaration/Resources-
statements, personal opinions and also original data pre-
PatientSafety-Map%20Helsinki%20Declaration.pdf).
sentation. With this publication we hope to further stim-
This year, in May/June 2020, ESA and EBA are celebrating ulate implementation of the Helsinki Declaration on
the 10th anniversary of the Helsinki Declaration on Patient Safety in Anaesthesiology in your own hospital,
Patient Safety in Anaesthesiology; a good opportunity to as well as opening the scope of the patient safety strate-
look back and forward evaluating what was achieved in the gies to address in the near future.
recent 10 years, and what needs to be done in the upcom-
ing years. Implementation of the Declaration was an Chapter 1: Implementation of the Helsinki
objective from the outset and in connection with this in Declaration on patient safety in
2011, an issue of the journal Best Practice and Research in anaesthesiology: past activities, current
Clinical the project consisted of an online survey of ESA European perspectives and future
members to s.14 A joint EBA/ESA Task Force was set up to opportunities (Ffrench-O’Carroll, Smith)
deliver this and produced a number of implementation The Helsinki Declaration on patient safety in
tools distributed at Euroanaesthesia Congresses and put on anaesthesiology
the website. A discussion in the Patient Safety and Quality The Helsinki Declaration on Patient Safety in Anaesthe-
Committee (PSQC) of the ESA has led to engagement in siology (hereafter ‘the Declaration’) was launched in 2010
an update of the safety literature, resulting in the present by the EBA/UEMS in close co-operation with the ESA.1
‘Expert Opinion’. This article will go beyond the topics It set out a vision for patient safety in anaesthesiology,
mentioned in the Helsinki Declaration on Patient Safety together with recommendations for specific activities
in Anaesthesiology, and will elaborate on topics, which 10 which could improve safety. It has four distinct elements:
Eur J Anaesthesiol 2020; 37:521–610
Copyright © European Society of Anaesthesiology. Unauthorized reproduction of this article is prohibited.
Ten years Helsinki Declaration 525
standards for clinical care; protocols for the management practices and the Declaration’s impact in greater detail,
of clinical crises in anaesthesiology; critical incident by conducting telephone interviews with national leaders
reporting; and an exhortation to engage in audit and in anaesthesiology in a number of European countries.
the compilation of annual reports about local patient Interviews were semistructured and the resulting quali-
safety as well as morbidity and mortality, to reap the tative data underwent thematic analysis, with themes
benefits of measurement to improve safety. developed inductively.20 Phase III involves site visits
to hospitals throughout Europe, to examine patient safety
The Declaration was signed by all the European societies
practice ‘on the ground’. The three phases thus each
attending its launch in Helsinki and also by the European
aimed to address anaesthesiology practice at various
Patients’ Forum. A number of implementation activities
levels (Fig. 1). While the third phase is still continuing
were undertaken to promote the use of the Declaration in
at the time of writing (September 2019), the combination
practice. A joint EBA/ESA Patient Safety Task Force was
of methods used is innovative and has not previously
set up, and every year this produced materials and
been described in the exploration of patient safety. This
resources that were made freely available to every delegate
chapter thus aims to outline the methodology of this
at the Euroanaesthesia Congress. In 2011, a special edition
phase of the project, report on the current state of
of the journal Best Practice and Research in Clinical
implementation of the Declaration, outline possible
Anaesthesiology devoted to patient safety was given
future measures for improving its uptake, and reflect
out.14 A survey on syringe labelling and a template for
on possible implementation approaches that have been,
the annual safety report (available from http://html.esah-
or could be adopted.
q.org/patientsafetykit/resources/basics.html) were pub-
lished in 2012. 17 The following year, a manual of
algorithms for managing clinical crises in anaesthesiology Methodology of site visits
was issued (available from http://html.esahq.org/patient- From the beginning of the project, it was clear that, to
safetykit/resources/downloads/05_Checklists/Emergen- illuminate the subject properly, the inquiry needed to
cy_CL/Emergency_Checklists.pdf). A ‘Patient Safety extend beyond a simple assessment of whether or not
Starter Kit’ on a data stick, containing recorded lectures the Declaration had been adopted to a broader attempt
and other resources, was distributed to participants at the to set it in the practice context of European anaesthesiol-
ESA’s Euroanaesthesia meeting in June 2014 (available ogy.21–23 We adopted a case study methodology and a
from http://html.esahq.org/patientsafetykit/resources/ broadly positive stance implying a ‘Safety II’ framework
index.html). Many lectures and presentations were given (i.e., a framework which aims to understand why things go
at anaesthesiology conferences within Europe and beyond right in health care most of the time) complementing a
and such was the appeal of the Declaration that it has now traditional ‘Safety I’ framework (i.e., a framework which
been signed by approximately three-quarters of national involves learning from errors).24–28 Our approach was essen-
societies worldwide. Despite the widespread endorsement tially ethnographic, aiming to build up a picture of safety as
of the Declaration’s principles, and the promotional activ- practised which was both scientifically rigorous but which
ities described above, there remains some uncertainty also ‘made sense’ to those under study, recognising the time
regarding its usage and influence in practice, with limited constraints imposed by the short visit schedule.29–32
studies performed assessing its impact.18
Country and hospital selection
To address this gap, the ESA’s PSQC has started a project
Six European countries were chosen to reflect varying
designed to assess, understand and improve the transla-
healthcare systems across Europe. Selection of countries
tion of the Declaration’s principles and requirements into
was influenced by practicality and the presence of a
clinical practice. As part of this project, the ESA recently
‘project champion’ (a high-level sponsor, often within
commissioned one of us (AFS) to undertake a three-
the national anaesthesiology society) and a local collabo-
phase investigation (details available from https://www.e-
rator, often a senior anaesthesiology trainee or a local
sahq.org/patient-safety/hd-follow-up-project/) to assess
consultant with expertise in patient safety. Typically,
the uptake and use of the Declaration. (The study was
AFS conducts the first couple of visits in a country with
funded by ESA, supported by the following industry
the local collaborator, with subsequent visits being per-
partners of ESA: Philips Healthcare, Masimo Interna-
formed by the local collaborator. There are plans for the
tional, Fresenius Kabi and Nihon Kohden Europe. These
local contacts to perform visits outside of their home
companies played no role in data collection, analysis or
country to gain experience and also share their own
writing of the article.) Phase I OF the project consisted of
experience of visits in different health care settings.
an online survey of ESA members to determine what
aspects of the Declaration had been adopted.19 Respon- Four or five hospital sites were selected in each country.
dents were also asked to express their opinions on the Methods of selection of these hospitals varied between
Declaration, its impact on patient safety, and limitations countries. Generally, a list of hospitals in the target
and barriers to embedding its recommendations in daily country was identified, then a computer-generated ran-
practice. Phase II sought to learn about patient safety dom number sequence was used to identify hospitals, and
Eur J Anaesthesiol 2020; 37:521–610
Copyright © European Society of Anaesthesiology. Unauthorized reproduction of this article is prohibited.
526 Preckel et al.
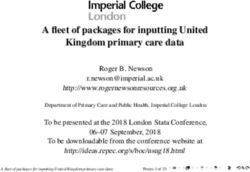
Fig. 1
EBA & ESA Anesthesia Institutions
EBA compliance in operating
NAS theatres and recovery areas
HD commitments
Appropriate facilities
Appropriate protocols
Regional
organisations ↓ Complications
Anesthesiology sedation
standards compliance
↓ Morbidity
Following the WHO Safe
Surgery initiative and Checklist
↓ Mortality
Annual reporting
Safe practice and critical
incident reporting systems
Schematic of the potential impact of the Helsinki Declaration across organisational levels of anaesthesiology practice in Europe. Reproduced with
kind permission of Grant Aaron, Masimo Company, Geneva, Switzerland. EBA, European Board of Anaesthesiology; ESA, European Society of
Anaesthesiology; HD, Helsinki Declaration; NAS, national anaesthesiology societies; WHO, World Health Organization.
departments of anaesthesia were contacted. If the first the visit, the investigators reviewed the departmental
department contacted did not wish to take part, then the protocols and guidelines with staff anaesthesiologists.
next hospital on the list was contacted, and so on. In other Second, we invited members of participating anaesthesi-
countries, the hospitals were selected by the local sponsor ology departments to fill in a questionnaire measuring
or collaborator. Hospitals were chosen to represent a mix, workplace safety culture. This, the University of Texas
both in terms of geographical spread and care provision Safety Attitudes Questionnaire (SAQ), gauges staff atti-
(district general vs. university vs. private hospitals). Fol- tudes across six patient safety-related domains and pro-
lowing agreement from the relevant anaesthetic depart- vides a snapshot of safety climate.33 The local contact
ments, several steps were taken before the visit: included person was asked to distribute these among at least 20
contacting local ethics boards to gain ethical approval and anaesthesiologists and theatre nurses prior to the visit.
establishing local rules for data sharing and confidentiality. SAQs measure staff attitudes across the domains of
teamwork, safety climate, job satisfaction, stress recogni-
tion, perceptions of unit management, perceptions of
Data collection
hospital management and working conditions. The ques-
The data collection process was designed to explore
tionnaire is a widely used tool, which can be used to
themes which emerged from earlier phases of the project.
measure staff’s attitudes to safety at a particular time
These included pre-operative assessment; checklists (in
point, prompt discussion about safety and the introduc-
particular the WHO Safe Surgery Checklist; WHO SSC);
tion of safety interventions, and act as a comparison tool
patient experience; anaesthesiologists’ working condi-
with other organisations.33–35 The third stream of data
tions and wellbeing the role of protocols; documentation
was obtained from observation. We undertook a ‘walk-
and medication prescribing; postoperative care and criti-
through’ of the operating theatre department, noting
cal incident reporting. The streams of data sought are set
facilities such as drug cupboards, emergency drugs, air-
out in the hospital visit schedule shown in Table 1.
way management, other equipment and optional moni-
The first, documentary data were collated by the local toring modalities [apart from ECG, pulse oximetry,
contact for the project, who completed the annual safety noninvasive blood pressure (NIBP)]. Such ‘safety walk-
report using the ESA’s template mentioned above, and rounds’ provided the opportunity to engage staff in the
also collected any relevant safety protocols. On the day of project, discuss safety concerns and notable safety
Eur J Anaesthesiol 2020; 37:521–610
Copyright © European Society of Anaesthesiology. Unauthorized reproduction of this article is prohibited.Ten years Helsinki Declaration 527
Table 1 Site visit process
Site visit process
1 Practical arrangements
Seek ethical approval for relevant country
Identify contact person in each hospital
Send project briefing summary to contact person
Confirm date when relevant stakeholders available
Establish rules for data sharing and confidentiality
Invite contact person to inform anaesthesiology department and theatre managers of project in advance of visit
Invite contact person to arrange open group meeting to anaesthesiology department on morning of meeting to explain purpose of project and aims of day
2. Preliminary information (by written questionnaire to be completed in advance)
Invite contact person to complete the annual departmental safety report
Further information to be sought by contact person (some contained within safety report)
Establish what staff are responsible for sedation in the hospital
Establish departmental participation in the local/regional/national incident reporting system
Reports of morbidity and mortality meetings if available
Summary of critical incident reports, if available
Are there any additional safety-related materials to guide practice in the hospital?
Establish departmental participation in major audits and local audits
Establish whether existing protocols exist for
Pre-operative assessment and preparation
Checking equipment and drugs
Syringe labelling
Difficult/failed intubation
Malignant hyperpyrexia
Anaphylaxis
Local anaesthetic toxicity
Massive haemorrhage
Infection control
Postoperative care including pain relief
Invite contact person to ask 20 to 30 people to complete SAQ before the visit
Invite contact person to suggest additional areas to explore on the visit in addition to the standard areas of interest below
3. Data collection during visit
Interviews
Two consultant anaesthesiologists (one preferably with a role in patient safety in department), one trainee and an anaesthesiology nurse, as a minimum
Review safety documents above during interview
Semistructured with open ended questions outlined in Fig. 3
Also cover suggested themes and follow-up on the information previously gathered
‘Walk-through’
Perform safety ‘walk-round’ of theatre department
Engage staff in the project
Discuss safety concerns and notable safety practices
Examine drug cupboards, emergency drugs and equipment, optional monitoring modalities (apart from ECG, pulse oximetry, NIBP)
Observation of safety practices
Checklists being performed – WHO checklist, patient check in
Pre-operative visit by anaesthesiologist
Checking of equipment – checking anaesthetic machine
Observe drug checking, preparation and labelling
Observe transfer of patient from theatre to recovery and handover to recovery staff
4. Follow-up
Write letter of thanks to contact person
Prepare report with findings
Send participation certificate
NIBP, noninvasive blood pressure; SAQ, Safety Attitudes Questionnaire.
practices and help towards promoting a safety cul- assessment, but also to allow discussion of local safety
ture.36,37 Furthermore, we observed several practices to practices and opinions.39 Typically two consultant anaes-
gain further information around safety, namely WHO thesiologists (one with a responsibility for safety in the
Safer Surgery ‘time out’ procedures, handover between department), one trainee anaesthesiologist and one
anaesthesiologists and recovery staff, and sometimes drug anaesthetic nurse were interviewed. The interviews were
and equipment checking.38 The fourth stream of data tape recorded, with the respondents’ consent.
came from several semistructured interviews. The open-
ended guide questions used in the interviews are shown Follow-up
in Table 2. Questions were developed to explore themes Following the visit, the investigators prepared a report on
mentioned above which emerged from phases I and II of their findings. This was sent to the anaesthetic depart-
the project, incorporating previous work on patient safety ment but not shared more widely, either with other
Eur J Anaesthesiol 2020; 37:521–610
Copyright © European Society of Anaesthesiology. Unauthorized reproduction of this article is prohibited.528 Preckel et al.
Table 2 Guide questions for interviews operative preparation, and the management of crises
Guide questions for interviews
during anaesthesia.19
Talk me through what happens to a patient when they come in for an elective Our results suggest that the Declaration’s impact is
operation
What do you think it is like to be a patient here? (nurses especially)
influenced by national practice context and local safety
How would you describe the ‘safety culture’ in the department/operating culture. Many respondents commented that safety prac-
theatres/hospital in general? What does it feel like to work here? What are tices such as monitoring standards have exceeded those
relationships like between anaesthesiologists, surgeons, nurses etc.? What
are the working conditions like (trainee anaesthesiologists especially)
set out in the Declaration for many years, especially in
Could you outline the main factors that ensure safety in anaesthesia and peri- Northern Europe. It is possible that the high levels of
operative care? What keeps patients safe at present, day to day? monitoring as recommended by WHO/World Federation
Have you any particular safety or quality ‘successes’ which others might learn
and benefit from? Any particular difficulties/problems? Why have these been
of Societies of Anaesthesiology (WFSA) standards (pulse
difficult? oximetry: 99.6%, BP: 99.4%, ECG: 98.1% and capnogra-
Are there any ‘problem cases’ in the department or your own work recently you phy: 96.0% throughout Europe), would have come about
would like to talk about? How do they show a lack of safety or, conversely, how
things were kept safe despite threats to safety? without the Declaration.40 Thus the potential benefit of
How reliable do you think the systems of care are in the department/hospital? the Declaration in enabling change and improvement is
How could care be kept safe or made safer in the future? What practical steps greatest in areas where safety practices are less well
might help improve patient safety in the hospital?
What sort of education and training opportunities are there for staff here? established (such as in the use of data for improvement,
Are people responding to opportunities to learn from problems and strengthen whether they are routinely collected or reporting adverse
good practice? incidents). The Declaration’s impact has also been influ-
How do you think the Helsinki Declaration on Patient Safety in Anaesthesiology
has influenced your department and hospital? Of all the areas outlined in the enced by recent changes in anaesthesia, with anaesthe-
Declaration, which are most useful in practice? Which are least useful? siologists throughout Europe reporting greater
Do you think/is it possible that the Helsinki Declaration on Patient Safety in workloads, more complex patients, and pressures to cut
Anaesthesiology has had any unintended or unforeseen consequences?
down on pre-operative preparation. This, along with
financial austerity and staff shortages (with workforce
migration reported by many) have resulted in a percep-
participating departments or the project funder. The
tion that more time is spent reacting to patient safety
report included: a summary of the annual safety report;
threats as opposed to progressing safety practices.20 Other
discussion of organisation and staffing issues; analysis of
factors, namely an organisation’s safety culture and staff-
monitoring standards; discussion of departmental policies
ing issues, have influenced the uptake of the Declaration:
and protocols; an analysis of the results of the SAQs;
for example in the production of annual safety reports and
qualitative themes from interviews; a list of recent safety
running morbidity and mortality meetings.19 The hospi-
initiatives and notable safety practices and notes on areas
tal visit process described above aimed to explore many
for consideration for improvement or change. Within the
of these contextual factors identified in the first two
report appendices, there were also links for safety
phases of the project.
resources and examples of notable safety practices from
other institutions, which the department might choose to Survey and interview data suggested that future changes
adopt. We also invited participating hospitals to provide to the Declaration could take account of the challenges
feedback on the visit process by completing an evaluation mentioned above, as well as the increased role of simula-
questionnaire after receiving the report. tion, human factors and multidisciplinary training in
anaesthesiology. But many respondents advocated
greater adherence to the existing Declaration rather than
Results
changes to the Declaration itself. This could be brought
Material from online and interview studies about by introducing a formal checklist of items in the
Results from phases I and II of our project provide an Declaration to guide day-to-day practice, and greater
insight into current and future implementation of the publicity. Efforts could be focused on areas that are less
Declaration (full results from phases I and II have already well implemented, such as annual safety reports. The
been published in this journal).19,20 In summary, the Helsinki Declaration on Patient Safety in Anaesthesiol-
Declaration is perceived variously as a force for good, a ogy could be revitalised, by inviting signatories to confirm
standardisation framework and a catalyst for change. It their continuing commitment on the Declaration’s 10-
benefits from being broad in scope, with knowledge of year anniversary in 2020. The existing Declaration could
the themes of the Declaration being better known than also be translated into languages other than English
the more specific details. National leaders interviewed where this has not already been done. Further safety
felt that it acts as a tool to help advance patient safety, suggestions stemming from our study results are outlined
both politically and scientifically. It could be argued too in Table 3.
that the Declaration is also an improvement intervention
with 44.5% of ESA members surveyed agreeing that it Practical aspects of the visits and our experiences
had improved safety. This was felt to be largely through Having performed several site visits at the time of writ-
promoting the use of checklists in the areas of pre- ing, we can now reflect on some of the factors required for
Eur J Anaesthesiol 2020; 37:521–610
Copyright © European Society of Anaesthesiology. Unauthorized reproduction of this article is prohibited.Ten years Helsinki Declaration 529
Table 3 Suggestions for further implementation of the Helsinki safety projects. The report distributed to departments
Declaration on Patient Safety in Anaesthesiology
after the visit contained several recommendations, useful
Suggestions for further implementation of the Helsinki Declaration on safety references and suggestions from other hospitals.
Patient Safety in Anaesthesiology We hope this will serve as a useful tool for departments.
Create and maintain structures for safety education both in training curricula and
for established specialist anaesthesiologists Performing the visit was also a valuable learning experi-
Promote a ‘no blame’ culture to encourage the reporting and open discussion of ence for the investigators. Trainees taking part gained
threats to patient safety
Greater involvement of patients in the promotion of safe practice
greater understanding of recommended safety standards,
Make the scientific, clinical, humanitarian and economic case for thorough pre- safety culture and research methods; arranging the visits
operative assessment called for a level of communication, leadership and
Establish and maintain regional networks within Europe to share practice and
solutions appropriate to available resources
organisation more than is usually necessary in everyday
Encourage the participatory self/peer evaluation of safety using the site visit clinical practice.
methodology and process described in this article. Even simple but repeated
measures such as using the annual safety report year on year can allow
changes to be made visible and possibly attributable to interventions made Discussion
Consider a concurrent, specific evaluation plan if the Declaration is revised and/ As we mark the 10th anniversary of the launch of the
or relaunched Declaration, we have, with hindsight, an opportunity to
ask some fundamental conceptual questions which have
not been previously asked but which are relevant to any
consideration of the Declaration’s impact. The first is,
a successful visit, some of the difficulties we have expe- what was (is) the Declaration exactly? Is it a statement of
rienced and the benefits to host departments. vision or intent, similar, for instance, to a resolution from
the United Nations or WHO? Is it a standard of care (it
The visits require considerable organisation and plan-
certainly refers to published international standards and
ning. Early work involves contacting anaesthesiology
invites compliance)? Is it a guideline? (This is more
departments and requesting their participation. Many
contested perhaps, as the word ‘guideline’ can encompass
departments contacted raised concerns that the visit
care standards too and there are different challenges to
was an ‘inspection’, or that data collected might result
uptake).41 Is it in some sense a care ‘bundle’ (a set of
in negative publicity for the organisation. It was impor-
interventions implemented together for a synergistic
tant at this stage to stress that the project is an attempt to
effect on outcomes)?42,43 These questions may seem
learn about safety in everyday anaesthesiology work
theoretical, but are important, because how the Declara-
(especially what is done well) and how the Declaration
tion is framed will affect how we perceive it, our expec-
fits into this, rather than an assessment of compliance
tations of what it can achieve, and how it should be
with any particular standard. A successful visit depends
evaluated. What is clear, both from the initial documen-
on close liaison with the local contact person, who will be
tation at the time of the launch, and from the interview
required to gather protocols, fill out the safety report,
responses and visits so far, is that the Declaration is not
distribute the SAQs and inform relevant staff in the
explicitly seen as a quality/safety improvement interven-
hospital of the visit. We are extremely grateful for the
tion. Maybe this is because it is complex (it has a broad
enthusiasm and time dedicated by our local hosts.
focus and includes drug, equipment, individual and
We found that providing an open education session to the organisational elements). Alternatively, it may simply
host anaesthesiology department about the project (on be that those who met and drafted it did not refer to
the morning of the visit) was useful in engaging staff, quality improvement science, although it must be said
many of whom were later keen to chat to us during our that this science was neither so well developed, nor so
theatre walk-through. Ideally this meeting should be widely applied, as it is today.44 This is not just conceptu-
multiprofessional, including anaesthesia nurses and ally important; viewing the Declaration as an intervention
theatre managers. allows us to invoke the science of implementation
referred to above, both as an analytical framework but
Early feedback suggests several immediate benefits to
also to enhance future uptake into practice. The text of
hospitals from taking part in the project. Staff reported
the original Declaration shows little evidence of planning
promotion of a safety culture through the planning and
as to outcomes, timelines or accountability, and only
execution of the visit. Multidisciplinary staff were keen
vaguely deals with what change is desired, though even
to complete SAQs, although for some the questionnaires
this lacks any prediction of the effect any change might
were seen more as an opportunity to express their opi-
be expected to have.44
nions on problems with the organisation. Anaesthesiology
departments learnt much about their safety systems; for There is a note that ‘we’ (not explicitly defined, but
example, they identified protocols that needed updating possibly the three organisations represented by the
or revision, and they reviewed their position with regard signatories in the printed version of the Declaration)
to contributing to national audits of practice. In some would reconvene annually to review progress. This
cases, the visit provided an impetus to commence new apparent lack of specificity in setting out a framework
Eur J Anaesthesiol 2020; 37:521–610
Copyright © European Society of Anaesthesiology. Unauthorized reproduction of this article is prohibited.530 Preckel et al.
for evaluation is not necessarily a problem, especially if (indeed, this is in the title of the project as presented to its
the Declaration is conceived as a ‘vision statement’. funders and various research governance bodies). This
However, if it is seen as a quality improvement tool entails not only discovering new knowledge and under-
greater attention to the design of the intervention at the standing specific problems, but also facilitating action and
start of its ‘lifetime’ can help avoid disappointing generating knowledge about that action.56 This implied a
results later. mixed methods approach drawing on both quantitative
and qualitative data, which has allowed us to construct an
The second question is, to what extent can changes in
account of patient safety in anaesthesiology, which
practice be attributed to the Declaration? It is clear from
reflects participants’ perceptions of, and meanings attrib-
the various streams of data collected during the project
uted to patient safety within the social context of anaes-
that there have been many changes since 2010, and it is
thesiology practice.57 We believe that this is one of the
not possible to establish fully which have come about as
main strengths of our approach, which falls broadly within
a result of the Declaration and which were happening
the emerging field of sociology of healthcare safety and
anyway. (The interview data refer to the latter phenom-
quality as recently delineated by Allen at al.55 It was
enon, known in quality improvement science as a ‘mat-
argued that patient safety is not simply about individual
uration’ effect.44) Selection bias in respondents in all
or team psychology, but is subject to the sociocultural and
three phases of this project could have coloured the data
political context of healthcare work. According to them, ‘a
we hold, and this is inevitable. Evidence for maturation
sociological perspective . . . reveals how these problems
could have been captured by repeated measurements
might be managed and by whom, as well as the everyday
over time (an ‘interrupted time series design’), had an
– and often invisible – situated practices through which
implementation and evaluation plan for the Declaration
quality and safety are accomplished’.55
been conceived as part of its launch.44 (A further ana-
lytical approach to uptake and coverage of the Declara- A further point on our data collection approach deals with
tion, drawing on the basic foundational categories of how we conceptualised and presented the project. We
implementation science, might also be fruitful in the did not see it (especially for the hospital site visits) as an
future.45) In any case, there was variation in uptake, both ‘inspection’ in the sense that we were directly assessing
of the same elements between countries, but also of ‘compliance’ with the Declaration’s standards (as noted
different elements of the Declaration. Compliance with above, there is more to it than this is any case). We
essential monitoring standards was very high through- introduced it, both in our initial contact with potential
out Europe though there was variable use of other sites, and during the briefing at the start of the visit, as an
modalities such as bispectral index and neuromonitor- attempt to understand how safety is ‘created’ in day to
ing.46,47 Protocols for pre-operative assessment and day anaesthesiology work, as above, and gauge the role
preparation were more widely used than those for the played by the Declaration within this. Patient safety can
management of postoperative pain, but sedation easily be overshadowed by a strong ‘normative’ element,
remains problematic.19,40,48 – 52 Both ‘human factors’ with negative moral overtones and intimations of blame
elements such as communication, and critical incident and recrimination.26 Adopting the more positive note of
reporting were recognised as important throughout Eur- ‘Safety II’, with its emphasis on understanding how and
ope, but the degree to which they featured in practice why things usually go right in safety terms, and seeing
and training varied.53,54 safety as a natural part of the anaesthesiologist’s profes-
sional identity complement this.27,58
The third question deals with the nature of the project we
have conducted. Right from the start it was clear to the The action research approach described above also
investigating team that, although the impetus for the implies that those participating are not simply passive
ESA was to establish the uptake and impact of the providers of data, but are also being facilitated in further
Helsinki Declaration, a wider reaching enquiry was pref- action in the name of promoting patient safety. The
erable, for two main reasons. Despite the ESA’s efforts, project could be said to have had a ‘transformative’ goal
we knew that some anaesthesiologists had not heard of from its inception.45 Scientific purists might label this
the Declaration, and many were not familiar with its ‘contamination’ or invoke the Hawthorne effect, but as
contents. Further, any safety initiative needs to fit into the ultimate aim of the Declaration and its associated
the practice context for which it is intended, if it is to be activities is to promote patient safety, we do not see this
adopted and used.55 Asking closed questions such as as a shortcoming. We believe that it was possible to find
‘does this department of anaesthesiology comply with out what was happening but also at the same time to
the Declaration?’ yields some information, but less than stimulate interest and activity in safety and raise aware-
asking ‘why?’ (if they do) or ‘why not?’ (if they do not). ness of the Declaration. The project (especially phase III)
Thus the project has been more an attempt to understand has indeed promoted the Declaration and patient safety;
the context (or indeed, multiple contexts) of safety in our initial informal intelligence (supported by the initial
anaesthesiology in Europe.22 Methodologically, we postvisit evaluation questionnaires completed by our
designed it too as ‘action research’ right at the beginning local contacts) suggests that the mere fact of taking part
Eur J Anaesthesiol 2020; 37:521–610
Copyright © European Society of Anaesthesiology. Unauthorized reproduction of this article is prohibited.Ten years Helsinki Declaration 531
in the visits has heightened departments’ awareness of Several tools have been developed to measure adverse
patient safety. Sharing of safety practices between hos- outcomes related to anaesthesia care and human errors
pitals will probably also benefit sites and in the future, we and/or deviations. These tools can be divided into tradi-
hope that departments may be able to use the visit tional safety measurement methods, developed by clin-
schedule we have described to perform their own self- icians, and alternative methods, developed by IT
assessment of their safety practices. Establishing a net- specialists or quality assurance organisations.
work of safety peer-reviewers, who could then potentially
cover more sites, as more anaesthesiologists within the Traditional patient safety measurement methods
network gain experience and confidence with the visit
Anaesthesia-related mortality
tool, could provide the benefit of having an external view.
Anaesthesia-related mortality refers to any death occur-
We hope that such activities will help implement the
ring during or following the care from an anaesthetist. For
Declaration in themselves.
analysis, cases are extracted from coroners’ registries,
voluntary reports, surveys and malpractice reports/autop-
Chapter 2: How to define and adequately sies.60–63 Information is usually forwarded to peer review
measure peri-operative patient safety (Haller) committees of expert practitioners, usually senior anaes-
Since the early development of anaesthesia, manipulat- thetists. Experts then determine whether adverse out-
ing powerful drugs, thereby altering physiological func- comes are related to anaesthesia or not, and whether any
tions, taking control of the circulation as well as the errors have occurred.
airway in unconscious patients have been recognised as
intrinsically challenging to patient safety. As a conse- The peer review process is largely based on implicit
quence, the speciality has been at the forefront of many criteria: individual reviewers determine the standard of
developments, particularly in-patient safety measure- care, including their personal opinions regarding what
ment, according to the rule: ‘One can only address what should be defined as an error.
one can see’. However, before patient safety is reliably This has been a preferred method since the beginning of
assessed, it first needs to be accurately defined. the speciality. Some examples include the National
Confidential Enquiry into Peri-Operative Deaths in
the United Kingdom, the survey of anaesthesia-related
Definition of patient safety death in France, the study of deaths associated with
Many patient safety definitions exist but all include the anaesthesia in Taiwan, the review of anaesthesia-related
presence of adverse outcomes/injuries stemming from mortality reporting in Australia and New Zealand, and
the processes of anaesthesia care and are related to errors, the study of anaesthesia-related mortality in the United
or deviations from expected care. Cooper et al.59 defined States.6,64 – 66 In all these studies, reviewers assess
the concept of patient safety as ‘the avoidance, preven- whether adverse outcomes are related to anaesthesia
tion, amelioration of adverse outcomes or injuries stem- or not. They identify which factors contributed to the
ming from the processes of health care (i.e. anaesthesia death of the patient, including human errors and case
care). Patient safety should address events that span the mismanagement. The latest figures report a mortality
continuum from what may be called errors and deviations rate related solely to anaesthesia of 2.96 per million
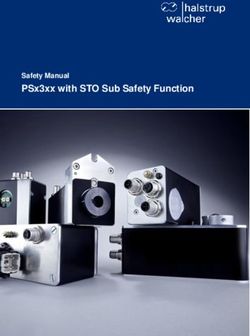
to accidents’. This concept can be modelled as a triangle population per year. Depending on countries and stud-
integrating all these three dimensions (Fig. 2). ies, the contribution of error and mismanagement to the
number of patients dying as a consequence of anaesthe-
Fig. 2 sia has been found to vary between 77 and 97% of
cases.65,67
Adverse outcomes
or injuries Although used over decades, mortality reviews have a
number of limitations. The first is a lack of a standar-
dised definition for anaesthesia-related mortality. In a
number of studies, mortality includes only cases of intra-
operative or immediate postoperative death to which
human error of the anaesthesia provider has contributed,
Patient
safety
while for others anaesthesia-related mortality refers to
all potential causes of deaths occurring during or fol-
lowing anaesthesia.61,62,68 The second limitation relates
Associated with human Related to
to peer review as a method to assess the contribution of
errors & deviations anaesthesia care human error. There is often variability among peer
reviewers’ opinion on ‘preventability’ of adverse out-
Model for the definition for patient safety in anaesthesia. comes and their level of agreement is sometimes only
slightly better than chance.69 The third limitation
Eur J Anaesthesiol 2020; 37:521–610
Copyright © European Society of Anaesthesiology. Unauthorized reproduction of this article is prohibited.You can also read