Research paper Diagnosis of Acute Renal Colic by Imaging Tests: A Retrospective Observational Study
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
research paper Submission date: 14/03/2021
Revision date: 24/03/2021
Acceptance date: 04/04/2021
Diagnosis of Acute Renal Colic by Imaging Tests: A
Retrospective Observational Study
Pérez-Núñez, Juan Jesús1; Olea-Rodríguez, Pablo1; Palacios-López, Rafael Manuel1
1
Faculty of Medicine, University of Granada (UGR)
Abstract
Introduction
Renal colic (RC) caused by lithiasis is a common reason for presentation to the emergency department.
Its diagnosis is usually based on the patient’s clinical picture, but it is sometimes necessary to perform
complementary imaging tests. Even though the patient is exposed to high radiation doses, computed to-
mography (CT) of abdomen and pelvis is the gold standard test to confirm RC by lithiasis. That is why it is
necessary to implement and analyze the performance of other imaging tests such as abdominal ultrasound
(AUS), which is increasingly becoming more important in clinical practice. The objective of this study was
to evaluate the role of AUS in diagnosing a suspected acute RC by lithiasis and the use of other imaging
tests in clinical practice.
Methods
This is a retrospective observational study of a cohort of patients with suspected acute RC who underwent
an AUS, as requested by the emergency department of a third-level hospital. Different variables related
to the patient’s clinical picture, the performed imaging tests and their findings were analyzed. Moreo-
ver, both descriptive and analytical analysis of the main variables of interest were conducted: positive
diagnosis, use of low radiation dose protocols, and association between pain intensity and other relevant
variables.
Results
In this study, a total of 80 patients were analyzed. Of the 64 patients (80% out of the overall sample) who
underwent an abdominal radiography (AR), the radiologist was able to detect lithiasis in 18.8% of patients
(34.4%), whereas the emergency physician identified it in 7.8% of them (90.6%). The presence of lithiasis
was confirmed by AUS in 43.8% of patients. CT was complementarily conducted, diagnosing lithiasis in
38.8% of patients, of whom 90.3% had not been previously diagnosed with lithiasis. A low radiation dose
protocol was applied to 48.3% of the latter, and statistically significant differences were found between the
mean radiation dose to which those patients were exposed and the one administered when such protocol
was not applied. AUS results were neither significantly associated with the pain intensity of the patient’s
clinical picture, nor with a previous diagnosis of lithiasis.
Conclusion
AUS is a non-invasive test that offers significant diagnostic results if acute RC is suspected. Low radiation
dose protocols are employed in CT with certain frequency when the presence of acute RC is suspected.
However, it is necessary to implement intervention protocols that guarantee the appropriate use of this
imaging test in clinical practice.
Keywords: urolithiasis, renal colic, ultrasound, computed tomography, emergency department.
Translated by:
Martínez-Coronado, Celia2; Morillas-Steveaux, África2; Ruiz-Martos, Sergio2; Sánchez-Cortés-Macías, Mario3; Sillero-
Romero, Miguel2; Torregrosa-Parra, Pablo4; García-Vergara, Diego5
2
Faculty of Translation and Interpreting, University of Granada (UGR)
3
Faculty of Philosophy and Letters, University of Liège (ULiège)
4
Faculty of Translation and Interpreting, Autonomous University of Barcelona (UAB)
5
Faculty of Humanities, University Pablo de Olavide (UPO)
16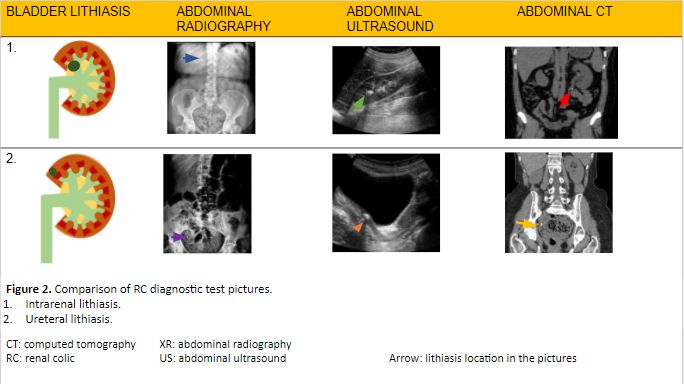
Archivos de Medicina Universitaria | Vol. 3, núm. 1
1. Introduction problem, but it presents other limitations such as
the necessary technical and practical experience of
Renal colic (RC) is an acute pathology characterized the professional conducting it, the stone size —if it
by the sudden onset of severe pain in the costover- is too small, it may not be visible—, or the patient’s
tebral angle. This pain can be located or radiated morphotype, among others (13).
to the groin (1, 2). The most common cause of this
pathology is the obstruction of the ureter by a stone Several clinical guidelines recommend AUS as the
(i.e. urolithiasis). Stones composed of calcium are initial imaging test to be performed on patients
the most recurrent (3). Lithiasis accounts for 2-5% of with suspected acute RC when AR is anodyne, or
all clinical presentations to the emergency depart- the degree of hydronephrosis or other kind of com-
ment. It is the most common urological emergency plication must be assessed (7, 10). However, there
(4), affecting 5-10% of the population and presen- is a huge variability in the choice and use of ima-
ting a high relapse rate (5). ging tests when RC is suspected in the usual clinical
practice (14, 15). Occasionally, ARs are not adequa-
Sudden pain located in the flanks or radiated to the tely assessed, or the radiographic technique used is
groin is the most common clinical picture of the pa- not the most appropriate. Sometimes, the decision
tient when treated in the emergency department. of conducting a CT or an AUS is likewise erratic and
This pain can be accompanied by haematuria, uri- conditioned by different aspects. On the one hand,
nary syndrome (2) and, less frequently, by gastroin- the work overload of the on-call radiologist leads
testinal symptoms (nausea and vomiting) or fever, to decisions based on aspects such as the patient’s
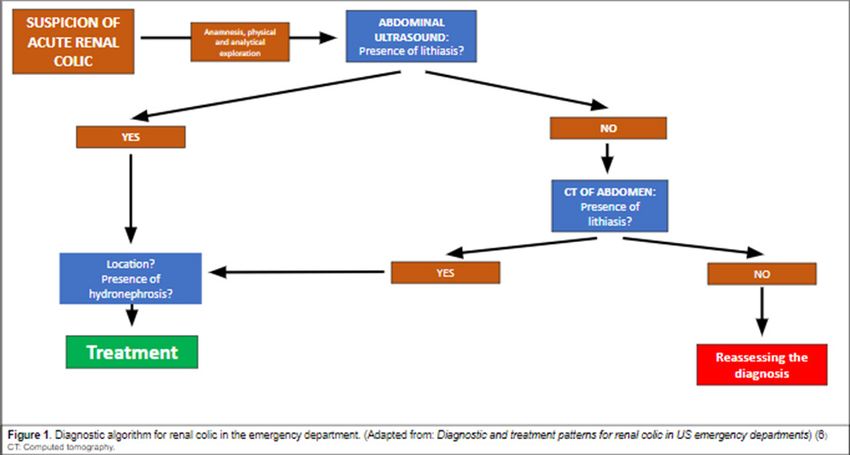
among others (1). To consider it as an acute RC, the phenotype and the degree of clinical suspicion,
patient must present any of the following: fever, re- among others. On the other hand, when the diag-
nal insufficiency (creatinine >1.5mg/dL), moderate nosis by AUS does not reveal the presence of hy-
or severe hydronephrosis, bilateral renal colic, soli- dronephrosis, a CT is complementarily performed,
tary kidney, having undergone a renal transplant, but this is not usually conducted in clinical practice.
uncontrolled pain despite treatment, or pregnancy What is more, low radiation dose protocols are nei-
(1, 6) (Figure 1). ther systematically applied in the performance of
The diagnosis of RC in emergency care is based on this complementary CT (16).
three aspects: the patient’s medical record, a uri- There are few studies that analyze the use and the
nary sediment analysis, and imaging findings (4). performance of imaging tests for suspected RC
Imaging tests are fundamental to diagnose lithiasis in the usual clinical practice. For this reason, the
in terms of identifying the location, size and hard- main objective of this paper is to analyze the role
ness of the stones. Consequently, imaging findings of AUS and other imaging tests in diagnosing sus-
help determine the most appropriate therapeutic pected acute RC in the usual clinical practice. The
options to treat RC. The most common imaging secondary objectives of this paper are to describe
tests performed are plain abdominal radiography the clinical and analytical variables of the cohort of
(AR), abdominal ultrasound (AUS), and compu- patients, and to assess the diagnostic value of the
ted tomography (CT) of abdomen and pelvis (7). A imaging tests that were performed on the patients
urine sediment analysis and an AR are systemati- by the emergency physician and the radiologist.
cally performed on the patient with suspected RC. Another secondary objective is to examine asso-
The results and the development of the patient’s ciations of potential interest for this research, such
clinical picture will be taken into consideration in as the association between high body mass index
order to assess if it is an acute RC or not (4). (BMI) and the diagnosis of lithiasis by AUS.
CT is considered the gold standard test, as it ena- 2. Methods
bles a better examination of the stone than AUS
does. Since CT provides more information, the An observational retrospective study was con-
therapeutic decision-making is more appropriate. ducted following the STROBE guidelines (17). A
However, the patient undergoing this procedure is retrospective review was made to all the patients
exposed to high radiation doses (13-20 mSv) —unli- who, presenting a suspected acute RC, underwent
ke AUS— and its routine use is complicated becau- an AUS from 1st September 2020 to 31st December
se of the high relapse rate of this illness (2, 6, 7, 10, 2020. This imaging test was requested by the emer-
11). Therefore, there are low radiation dose proto- gency department of Hospital Virgen de las Nieves
cols to reduce the exposure to 6.1 mSv (11), which is (Granada, Spain). Pregnant and underage (Diagnosis of Acute Renal Colic by Imaging Tests: A Retrospective Observational Study
The database was made in Microsoft Excel®. Labo- 3.2. Use of AR
ratory data collected in the emergency department
A total of 64 sample patients (80%) underwent AR.
was included: sedimentary red blood cells, creatini-
An emergency physician examined 90.6% of these
ne, leukocytes, and C-reactive protein. Data related
radiographies, but lithiasis was only found in 7.8%.
to the pathology was also included: location and
Among those analyzed by a radiographer (34.4% of
intensity of the pain at the time of requesting the
the samples), lithiasis was reported in 18.8%, whe-
imaging test, assessed by the visual analogue scale
reas inconclusive signs were found in 15.6%.
(VAS); injured area; presence of vegetative symp-
toms; and previous diagnosis of RC. In addition, 3.3. Diagnostic performance of AUS
the database contains data from the radiography:
Obstructive lithiasis was identified by AUS in 35
the doctor’s or radiologist’s assessment indicating
patients (43.8%). It was located in the distal ureter
if lithiasis was visible or not, and variables related
with a mean size of 4.5 mm (s=2) in 62.9% of the
to AUS performance (presence of vesical filling, vi-
patients; in the middle ureter with a mean size of
sualisation, location and size of the stone, and pre-
7.5 (s=4.5) mm in 5.7%; and in the upper ureter with
sence of hydronephrosis). When conducting a CT,
a mean size of 7.98 mm (s=2.5) in 28.6%. However,
the following information was included: use of low
2.9% was not included in the database (lost data).
radiation dose protocol if applicable and effective
dose, as well as the same variables applied to AUS, 3.4. BMI impact on AUS diagnosis
excluding vesical filling.
In our study population, 2 patients (2.5%) were un-
All the variables of the database were statistically derweight, 40 (50%) were normal-weight, 22 (27.5%)
analyzed by using SPSS® Statistics 23.0. Furthermo- were overweight, and the remaining 16 (20%) were
re, BMI and its subsequent categorization were cal- obese. Upon comparison of BMI categories and the
culated: underweight (Archivos de Medicina Universitaria | Vol. 3, núm. 1
4. Discussion served in our study, as 38.8% of the patients had
to undergo a complementary CT after being unsuc-
Our study presents interesting results. To begin cessfully diagnosed with RC by AUS. The need for
with, the emergency physician identified only 7.8% a CT in order to determine with greater accuracy
of urolithiasis cases by a plain AR, whereas 18.8 % the presence and size of a stone in patients with
of lithiasis cases were identified by the radiogra- RC (13) involves exposing patients to radiation
pher. The low number of RC cases identified by the (often in several occasions), alongside the dangers
emergency physician using AR might be explained it entails for their health, mainly related to radia-
by the size of the stone, apart from a poorer training tion-induced cancer (5). As pointed out by Rob S.
compared to that of the radiographer. According to et al. (22), the frequent use of radiological images
Sung Li Jung et al. (19), there is an association be- in subjects suffering from RC relapses results in
tween a bigger size of the stone and the AR sensiti- exceeding the yearly recommended dose of ra-
vity (50%) to detect a case of lithiasis. Its sensitivi- diation administered to each patient. Therefore, it
ty drops to 23.6% when the stone is smaller than 5 supports our idea of encouraging the use of AUS
mm. The mean stone size diagnosed by AUS in our when a case of acute RC is suspected so as to avoid
study is 5.6 mm. This would explain a decrease in the radiation excess by CT. Low dose (Diagnosis of Acute Renal Colic by Imaging Tests: A Retrospective Observational Study
program and an inadequate clinical management of M, et al. ACR appropriateness criteria® acute onset flank pain-suspi-
cion of stone disease. Vol. 28, Ultrasound Quarterly. 2012.
the patient. On the other hand, the plain AR sensi- 10. Mark L Zeidel M, W Charles O’Neill M. Clinical manifestations
tivity is remarkably conditioned by the stone size, and diagnosis of urinary tract obstruction and hydronephrosis -
as the diagnosis is very limited with small stones. UpToDate [Internet]. 2021 [Last access: 5 March 2021].
11. van der Molen AJ, Miclea RL, Geleijns J, Joemai RMS. A Survey
Despite this limitation, the radiographer diagnoses of Radiation Doses in CT Urography Before and After Implemen-
more urolithiasis than the emergency physician, so tation of Iterative Reconstruction. Am J Roentgenol. 2015 [Last
access: 29 March 2021];205(3):572–7.
cross-consultation with the former should be facili- 12. RadiologyInfo.org | Español [Internet]. [Last access: 29 March
tated in order to aid the diagnosis. No associations 2021]. Available at: https://www.radiologyinfo.org/sp/
between a high BMI and a lower ability to visualize 13. Smith D, Patel U. Ultrasonography vs computed tomogra-
phy for stone size. BJU Int. 2017 Mar 1 [Last access: 7 March
urolithiasis in AUS have been found. This would 2021];119(3):361–2. Available at: http://doi.wiley.com/10.1111/
support the use of this technique in patients with bju.13735
a high BMI despite clinical guides advising to per- 14. Arrabal Martín M, Barrero Candau R, Campoy Martínez P, Car-
nero Bueno J, Del Río Urenda S. Urolitiasis: proceso asistencial
form CT as an initial diagnostic imaging test on this integrado [Internet]. Junta de A. 2012 [Last access: 12 March 2021].
group of patients. 230 p. Available at: https://www.juntadeandalucia.es/organis-
mos/saludyfamilias/areas/calidad-investigacion-conocimiento/
gestion-conocimiento/paginas/pai-urolitiasis.html
Statements 15. Robledo Aburto ZA, Borja Aburto VH, Lira Romero JM, Arizmen-
di Urise E, Peña viveros R. Diagnóstico y tratamiento del cólico
Acknowledgements renoureteral en el servicio de urgencias. Durango 289-1A Colonia
Roma; 2019 [Last access: 29 March 2021].
The authors of this paper would like to thank the in- 16. Nicolau C, Salvador R, Artigas JM. Diagnostic management of re-
volvement of the coordinating and teaching staff of nal colic. Radiología. 2015. 57(2):113–22.
17. Cuschieri S. The STROBE guidelines. Saudi J Anaesth. 2019 (Suppl
the “Producción y traducción de artículos científicos
1):S31–4.
biomédicos (III ed.)” and the “Traducción inversa 18. F.Xavier P-S, D DMBS, Bouchard C, A R. The Practical Guide
de artículos científicos biomédicos (español-inglés)” Identification, Evaluation, and Treatment of Overweight and
Obesity in Adults NHLBI Obesity Education Initiative. 2000 [Last
courses, especially Antonio Jesús Láinez Ramos-Bos- access: 29 March 2021]. 94 p.
sini for providing us with the radiological images, as 19. Jung SI, Kim YJ, Park HS, Jeon HJ, Park HK, Paick SH, et al. Sen-
well as the English translation team. sitivity of digital abdominal radiography for the detection of ure-
ter stones by stone size and location. J Comput Assist Tomogr.
2010;34(6):879–82.
Conflicts of interest 20. Semins MJ, Shore AD, Makary MA, Magnuson T, Johns R, Matla-
ga BR. The Association of Increasing Body Mass Index and Kid-
The authors of this paper declare no conflicts of interest. ney Stone Disease. J Urol. 2010;183(2):571–5.
21. Ganesan V, De S, Greene D, Torricelli FCM, Monga M. Accura-
Ethical concerns cy of ultrasonography for renal stone detection and size deter-
mination: is it good enough for management decisions? BJU Int.
This paper has been approved by the Research Re- 2017;119(3):464–9.
search Ethics Committee of the Province of Grana- 22. Rob S, Bryant T, Wilson I, Somani BK. Ultra-low-dose, low-dose,
and standard-dose CT of the kidney, ureters, and bladder: is there
da (code 1235-N-20). a difference? Results from a systematic review of the literature.
Vol. 72, Clinical Radiology. W.B. Saunders Ltd; 2017. p. 11–5.
References 23. Smith-Bindman R, Aubin C, Bailitz J, Bengiamin RN, Camargo CA,
Corbo J, et al. Ultrasonography versus Computed Tomography for
1. Francisco Javier Ancizu FD-C. Cólico renal. [Internet]. [Last access: Suspected Nephrolithiasis. N Engl J Med. 2014;371(12):1100–10.
29 March 2021]. Available at: https://docplayer.es/111525020-Co-
lico-renal-francisco-javier-ancizu-fernando-diez-caballero.html
2. Gary C Curhan, MD S, Mark D Aronson M, Glenn M Preminger
M. Diagnóstico y manejo agudo de la sospecha de nefrolitiasis en
adultos - UpToDate [Internet]. 2021 [Last access: 5 March 2021].
3. Singh P, Enders FT, Vaughan LE, Bergstralh EJ, Knoedler JJ,
Krambeck AE, et al. Stone Composition Among First-Time Symp-
tomatic Kidney Stone Formers in the Community. Mayo Clin
Proc. 2015; 90(10):1356–65.
4. Sánchez-Carreras Aladrén F, Verdú Tartajo F, Herranz Amo F, Es-
cribano Patiño G, María Díez Cordero J, Moncada Iribarren José
Jara Rascón I, et al. Urgencias urológicas [Internet]; 2014 [Last
access: 8 March 2021]. Available at: https://www.aeu.es/UserFi-
les/files/Urgencias_Urologicas.pdf
5. Aller Rodríguez M, Álvarez Castelo L, Asensi Pernas A, Cabana
Cortizas MT, Caeiro Castelao JM, Calvo Quintela L, et al. Aborda-
je práctico de la patología urológica [Internet]. María Sánchez J,
Venancio M, Abal C, editors. EdikaMed, S.L; 2014 [Last access: 8
March 2021]. 277 p. Available at: www.cedro.org
6. Brown J. Diagnostic and treatment patterns for renal colic in US
emergency departments. Int Urol Nephrol. 2006;38(1):87–92.
7. Susaeta R, Benavente D, Marchant F, Gana R. Diagnóstico y ma-
nejo de litiasis renales en adultos y niños. Rev Médica Clínica Las
Condes. 2018;29(2):197–212.
8. Fwu C-W, Eggers PW, Kimmel PL, Kusek JW, Kirkali Z. Emergen-
cy department visits, use of imaging, and drugs for urolithiasis
have increased in the United States. Kidney Int. 2013 ;83(3):479–86.
9. Coursey CA, Casalino DD, Remer EM, Arellano RS, Bishoff JT, Dighe
20Archivos de Medicina Universitaria | Vol. 3, núm. 1
TABLES
95 %CI
Mean Standard deviation
Inferior Superior
VAS 7.3 1.9 6.8 7.7
BMI 25.7 5.6 24.5 26.9
Size* (mm) 5.7 2.9 4.6 6.7
mSv dose** 9.2 6.6 6.7 11.7
* Only the cases where AUS detected lithiasis (N=30)
** Only the cases where it was necessary to conduct a CT (N=31)
VAS: visual analogue scale
BMI: body mass indexl
Table 1. Quantitative variables.
BMI Category
Underweight Normal- weight Overweight ObesityDiagnosis of Acute Renal Colic by Imaging Tests: A Retrospective Observational Study FIGURES 22
Archivos de Medicina Universitaria | Vol. 3, núm. 1
23You can also read