Regional variations in distribution, diagnosis and treatment of chronic pancreatitis in the mainland China: a systematic review of case articles ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Regional variations in distribution, diagnosis and
treatment of chronic pancreatitis in the mainland
China: a systematic review of case articles over 40
years
Wei Wang ( wangwei_0306@163.com )
Shanghai Jiao Tong University School of Medicine
Weisong Jiang
Ruijin Hospital, Shanghai Jiao Tong University
Meng Shu
University Institute of Lisbon
Liying Luo
Ruijin Hospital, Shanghai Jiao Tong University
Ao Liu
Ruijin Hospital, Shanghai Jiao Tong University
Xunke Pan
Ruijin Hospital, Shanghai Jiao Tong University
Jingjing Liu
Ruijin Hospital, Shanghai Jiao Tong University
Chong Wang
Ruijin Hospital, Shanghai Jiao Tong University
Yizhi Cao
Ruijin Hospital, Shanghai Jiao Tong University
TungChing Wu
Ruijin Hospital, Shanghai Jiao Tong University
Pengyi Liu
Ruijin Hospital, Shanghai Jiao Tong University
Junyao Xv
Ruijin Hospital, Shanghai Jiao Tong University
Yiran Zhou
Ruijin Hospital, Shanghai Jiao Tong University
Research Article
Page 1/18
Keywords: chronic pancreatitis, case articles, pancreatic cancer, medical resources, misdiagnosis
Posted Date: January 3rd, 2023
DOI: https://doi.org/10.21203/rs.3.rs-2385994/v1
License: This work is licensed under a Creative Commons Attribution 4.0 International License.
Read Full License
Page 2/18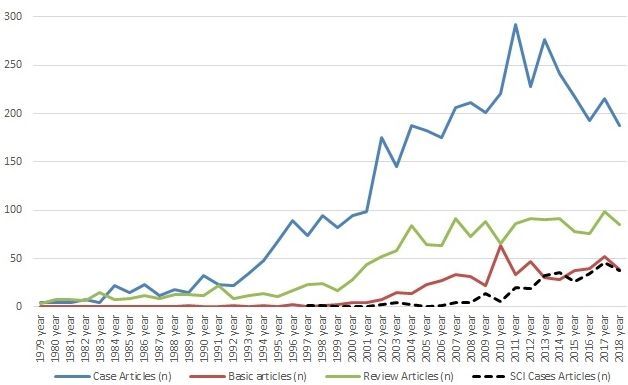
Abstract
BACKGROUND: Epidemiological data regarding the regional differences in chronic pancreatitis (CP) from
the mainland of China is lacking. We aimed to gather and combine the information concerning the
regional distribution and the risk factors associated with pancreatic cancer (PaCa) and death from
published articles.
METHODSː:Case articles on CP published in seven databases from January 1979 to December 2018
were analysed.
RESULTS: A total of 4,452 cases articles (containing 161,243 CP cases) were included. Since the mid-
1990s, the number of published articles grew rapidly, which was significantly related to the gross
domestic product of the region. In recent years, the number of CP cases of idiopathic etiology, those
receiving endoscopic treatment, those with comorbid diabetes mellitus and the number of Science
Citation Index (SCI) case articles have increased. Surgical treatment (37.4%) was closely associated to
alcoholic CP (r = 0.55, P = 0.000), idiopathic CP (r = 0.52, P = 0.000), wasting (r = 0.21, P = 0.000),
jaundice (r = 0.27, P = 0.000), PaCa and death detected during hospitalization and follow-up, and was
more common in underdeveloped areas. Endoscopic therapy (27.9%) was mainly concentrated in
developed areas, associated with non-alcoholic CP and a higher incidence of death (r = 0.48, P = 0.000)
and PaCa (r = 0.3, P = 0.000) during follow-up. The total number of PaCa in CP cases was significantly
related to the number of PaCa cases in each region (r = 0.94, P = 0.002). PaCa detected during
hospitalization was mainly related to jaundice, pain, diabetes, biliary diseases, alcoholic CP, conservative
treatment and surgical treatment.
CONCLUSIONS: The distribution of clinical features and management treasures showed obvious regional
characteristics, which closely related to the local detection level of CP and PaCa, showing that there were
likely to be many cases of misdiagnosis or delayed diagnosis of CP and PaCa. The problem of uneven
distribution of medical resources, which related to the imbalance of economic and social development,
needs to be resolved.
Introduction
Chronic pancreatitis (CP) is a pathologic fibro-inflammatory disorder of the pancreas, and is a lifestyle-
related disease 1. The rising incidence rate of pancreatic cancer (PaCa) has been documented in CP
patients 2. Together with the CP-associated mortality rate (0.09 deaths per 100,000 person-years), this
indicates that CP is an important global health issue 3.
The annual incidence rates of CP are approximately 5 to 10 per 100,000, with a higher incidence found in
males 2. The prevalence rates per 100,000 population are 52.4 in Japan, 25.4–98.7 in USA, and up to 143
in France 4,5,6. However, the mainland of China had only one local area survey performed 11 years ago 7.
In 2011, the reported prevalence rate of CP in the mainland of China was similar to the Japanese
Page 3/18incidence data (14.0/100,000, in 2011), where the lifestyle habits are similar to the mainland of China,
indicating that the results are likely to be underestimated 4.
An alternative method is to obtain the epidemiological information from published articles originating
from China. However, the diagnostic criteria are not consistent in these previous articles. Additionally,
many non-CP articles appeared often during literature searches, none of the journal databases contained
all the pertinent articles, and there may be overlapping articles in different journal databases. Moreover,
due to language barriers, many articles published in either a Chinese or English database are ignored by
different scholars, which makes it difficult for us to draw an objective and accurate conclusion.
In this study, we conducted a systematic review of original articles on CP involving Chinese patients
published in the last 40 years from both Chinese and English databases. Information was obtained
regarding the regional distribution, diagnosis, and treatment of CP, and the risk factors associated with
PaCa and death, in order to understand the differences in these data in the different regions of mainland
China. This study was performed to provide a useful and reliable reference for future epidemiological
investigations, disease management and policy-making decisions.
Methods
Data retrieval
We conducted database searches and reviews of the literature between April 2013 and November 2020.
The following electronic databases were searched for studies published from January 1979 to December
2018: PubMed, EMBASE, Web of Science, China National Knowledge Infrastructure (CNKI), the Chinese
Science and Technology Periodical Database (VIP), Chinese Biomedicine Literature Database (CBM-
SinoMed), and Wanfang Database (Supplementary Fig. 1).
Inclusion criteria
The case articles satisfying the following conditions were included in this study: a) availability of the full
text articles with cases of CP; b) CP was diagnosed on histopathological examination of the pancreatic
tissues, or there was cytological evidence with more than six months of follow-up for cases with mass
pancreatitis, pseudotumor pancreatitis or focal pancreatitis; c) for articles without a specific description
of the diagnostic criteria of clinical CP cases, CP was considered if the descriptions included stones in the
pancreatic ducts, multiple or numerous calcifications distributed over the entire pancreas, and irregular
dilatation of the main pancreatic duct (MPD) and/or pancreatic duct branches 8; d) autoimmune
pancreatitis (AIP) diagnosed in patients with high levels of serum IgG4 (> 2 upper limit of normal), or with
parenchymal imaging on computed tomography (CT) or magnetic resonance imaging (MRI) and a
response to corticosteroids, or based on histopathology 9. The etiologies of CP such as alcohol, biliary
(miscellaneous factor), or idiopathic, were solely based on the data included in the articles 10.
Statistics
Page 4/18The representativeness of the distribution of cases was tested using the correlation between the cases
with PaCa in the case articles and the cases with PaCa in 2015 using the available data 11. The multiple
linear regression method was employed to determine the relationship between clinical indexes and PaCa
or death.
Pearson correlation analysis was used to explore the relationship among all study variables.
Classification and regression tree (CART) analyses were utilized to detect variables, when considered
simultaneously, that can identify patients having the highest risk for cancer or death. All analyses were
conducted in R 3.6 software using the rpart package (Supplementary Fig. 2).
Results
Epidemiological and general features of the included
studies
A total of 6,686 CP articles including 4,452 case articles (containing 161,243 cases), 560 basic articles
and 1,674 review articles were selected for analysis in this study (Supplementary Fig. 1). These articles
were significantly related to each other in various regions (Supplementary Fig. 3, Supplementary Table 1).
Since the mid-1990s, the number of published articles grew rapidly, especially the number of case articles
(Fig. 1). During this period of rapid growth, the rise in the number of articles and cases were particularly
evident in the northern region represented by Beijing and the eastern region represented by Shanghai (Fig.
2, Supplementary Fig. 4). In recent years, the number of CP cases of idiopathic etiology, those receiving
endoscopic treatment, those with comorbid diabetes mellitus and the number of Science Citation Index
(SCI) case articles have increased (Fig. 1, Fig. 3, Supplementary Tables 2 and 3). The number of articles,
rather than the number of cases, was significantly related to the gross domestic product (GDP) of the
region but not its population (Supplementary Tables 4 and 5).
The variables associated with the highest likelihood for articles including PaCa case(s) or expired case(s)
are shown in Supplementary Fig. 2.
Author's specialty, Department or unit
The three specialties most concerned with CP were surgery (39.2.1%), internal medicine (31.4%) and
imaging (20.3%). (Table 1, Fig. 4, Supplementary Fig. 5, Supplementary Tables 6, 7 and 8). Professionals
from 1,557 hospitals, universities, institutions, faculties of medicine, or research centres (herein after
referred to as hospitals) participated in the writing of the case articles on CP, including 76 hospitals with
≥ 10 articles published per hospital. (Supplementary Table 9, Supplementary Fig. 6). Approximately
67.2% of hospitals only published one articl (Fig. 5). The top 32 hospitals (2.1%, 32/1557) published the
most articles (≥ 20 case articles/hospital), which included a total of 1374 case articles (30.9%;
Supplementary Table 10).
Page 5/18Table 1
Clinical features of cases with chronic pancreatitis in case articles reported from 1979 to
2018.
n %
Total Articles 4452 /
Total Cases 161243 /
Articles providing gender information 2667 59.9%
Cases 127829
Male 85118 66.6%
Female 40355 31.6%
Articles providing etiology information 1688 37.9%
Cases 98484
Alcohol 24876 25.3%
Bile 18718 19.0%
Idiopathic 25487 25.9%
Autoimmune 8754 8.9%
Hereditary 887 0.9%
Articles providing clinical symptoms information 2200 49.4%
Cases 98300
Pain or pancreatitis 72228 73.4%
Diabetes 15281 15.5%
Diarrhoea 12414 12.6%
Wasting 10522 10.7%
Jaundice 8118 8.3%
Articles providing treatment information 3145 70.6%
Cases 103238
Endoscopic 28823 27.9%
Surgical 38657 37.4%
Conservative 27718 26.8%
Articles providing follow-up information 1568 35.2%
Page 6/18n %
Cases 62904
Pancreatic Cancer(PaCa) 372 0.6%
Other Cancer 13 0.02%
Death 1018 1.6%
Articles containing cases combined with PaCa 316 7.1%
Cases 17830
Cases combined with PaCa 1257 7.0%
Articles containing cases combined with other cancers 33 0.7%
Cases 1661
Cases combined with other cancers 84 5.1%
Articles containing cases of death during hospitalization 56 1.3%
Cases 2802
Cases of death during hospitalization 71 2.5%
*, estimated from the age range or the standard deviation of age mean plus or minus.
Clinical features, treatments, and prognosis
Endoscopic treatment was significantly associated with idiopathic CP, alcoholic CP and a higher
incidence of death (r = 0.48, P = 0.000) and PaCa (r = 0.3, P = 0.000) during follow-up. Surgery was closely
associated to alcoholic CP, idiopathic CP, biliary diseases, hereditary pancreatitis, death (r = 0.09, P =
0.000) and other cancers (r = 0.04, P = 0.006) detected during hospitalization, and was more relevant to
wasting and jaundice, PaCa detected during hospitalization (r = 0.21, P = 0.000) and follow-up (r = 0.24, P
= 0.000), as well as death during follow-up (r = 0.39, P = 0.000). Conservative treatment was more
associated with alcoholic CP, biliary disorders, hereditary pancreatitis, idiopathic CP, autoimmune
pancreatitis, and higher incidence of PaCa detected during hospitalization (r = 0.37, P = 0.000; Fig. 4,
Supplementary Fig. 5, Supplementary Tables 7 and 8).
The total number of PaCa in CP cases was significantly related to the number of PaCa cases in each
region (r = 0.94, P = 0.002; Supplementary Tables 11, Supplementary Fig. 8). PaCa detected during
hospitalization was significantly related to jaundice, pain, diabetes and biliary diseases, alcoholic CP,
idiopathic CP, conservative treatment, surgery and endoscopic treatment. PaCa detected during follow-up
was associated with pain (r = 0.31, P = 0.000), diabetes (r = 0.26, P = 0.000), diarrhoea and wasting, and
other type of CP. Death during follow-up was closely related to idiopathic CP (r = 0.48, P = 0.000), alcoholic
CP (r = 0.31, P = 0.000) and PaCa detected during follow-up (r = 0.62, P = 0.000). Death during
Page 7/18hospitalization was associated with jaundice and surgical treatment. PaCa and death detected during
follow-up were mainly associated with endoscopy therapy (r = 0.3, 0.48; P = 0.000), followed by surgical
treatment and conservative treatment ( Fig. 4, Supplementary Fig. 5, Supplementary Tables 7 and 8).
Geographical distribution
Idiopathic CP, hereditary pancreatitis and alcoholic CP were more common in the eastern regions, where
they related to pain, diabetes and diarrhoea, represented mainly by Shanghai, which had a high
proportion (46.7%) of idiopathic CP. AIP was more common in the northern regions, where it related to
jaundice and was represented by Beijing (r = 0.12, P = 0.000). In addition, 19.0% of CP cases had
associated biliary disorders. The two provincial regions with the lowest proportions of biliary disorders
were Shanghai (10.2%) and the three provincial regions with the highest proportions were Guangxi
(55.3%), Xizang (47.1%), Xinjiang (44.6%). Biliary disorders were weakly associated with Shanghai, and
Xinjiang province (Table 1, Fig. 4, Supplementary Tables 6–8, Supplementary Fig. 5).
Discussion
Basic characteristics of the CP case studies
This is the first comprehensive analysis of all case articles on CP published over a period of 40 years in
the Chinese mainland. With improvements to the understanding of CP and advances in imaging
technology, the apparent incidence of CP has been increasing, including early and probable CP cases 5,12.
The economic development, improved standards of living and the increased intake of meat or high fatty
foods may have accelerated this trend, especially after 1990. (http://data.stats.gov.cn/easyquery.htm?
cn=C01) 1,13,14 On the other hand, in this study, we found that the number of research teams have
gradually expanded. However, in the entire country, most hospitals (67.2%) have only published one case
article and there are three high-volume dedicated centers for CP diagnosis and treatment, located in
Beijing, Shanghai and Sichuan, while the level of CP diagnosis and treatment in provinces with a higher
economic development level was greater (Figs. 1, 2 and 5, Supplementary Figs. 3–6, Table 1,
Supplementary Table 3–6, 9 and 10). These findings demonstrate that the inequities in health resources
is incredibly significant 15,16. Furthermore, the level of diagnosis and treatment of CP is closely related to
the detection of PaCa, which showed that the incidence rate of PaCa is likely to be missed due to the
imbalance of development among different regions (Supplementary Fig. 8, Supplementary Table 11).
Clinical manifestations and geographical distribution
Patients with alcoholic CP are more symptomatic than patients with non-alcoholic CP (Fig. 4,
Supplementary Fig. 5, Supplementary Tables 7 and 8) 17. Some developed areas have started to diagnose
and treat more difficult types of CP, such as AIP and idiopathic CP, which further indicated that the
inequities in health resources appear to be expanding (Fig. 4, Supplementary Fig. 5, Supplementary
Tables 6–8) 13,14.
Page 8/18Interestingly, this study found that female cases ≥ 2 is one of the significant variables for publications
that included cases of PaCa detected during follow-up (Supplementary Fig. 2A), which appeared to
suggest that females were more likely to be diagnosed with PaCa. However, this is only true in female
patients who had a low rate of drinking and smoking. PaCa is more likely to be the cause of symptoms
and signs that are commonly suggestive of CP, and we caution that a diagnosis of CP should not be
made before reliably excluding PaCa, especially in female patients 18. Moreover, data remind us to pay
attention to PaCa in patients with CP complicated with biliary diseases in hospital and after discharge
(Fig. 4, Supplementary Fig. 5, Supplementary Tables 7 and 8, Supplementary 2A, 2C) 19.
Treatment of CP and geographical distribution
A stepwise approach has been advocated to treat CP, with medical therapy and lifestyle changes as the
first line of therapy, followed by progressively more invasive therapies such as extracorporeal shock wave
lithotripsy (ESWL) and endoscopic therapy with approximately a 50% chance of long-term pain
resolution. Surgery is associated with potentially more serious complications (6–50% morbidity, 0–6%
mortality) 20,21. Therefore, surgery should only be recommended if symptoms recur and/or there is
endoscopic failure or suspicion of a malignant (cystic) lesion 12,20.
In the present study the proportion of patients receiving surgical treatment was more than that of patients
receiving endoscopic treatment (37.4% vs. 27.9%) and most of the provinces offering surgical treatment
were in less-developed areas. The main reasons for performing surgery in most regions were PaCa
detection during hospitalization, weight loss and jaundice, and discovery of a mass in the northeast
region, which were alarm symptoms of PaCa 22. These findings suggest that surgery has undoubtedly
become a preferred choice of treatment 12,20, but it was directly associated with an increase in deaths
during hospitalization. On the other hand, endoscopic therapy had a weak association with wasting and
jaundice, and a strong association with idiopathic CP and the economically developed areas such as
Shanghai in the east of China. This suggests that the patients receiving endoscopic therapy tend to be
relatively mild cases, perhaps with fewer warning signs of PaCa. Endoscopic therapy was provided in
economically developed areas since it requires relatively newer technologies with advanced endoscopic
expertise and higher expenses 23, which promoted the early diagnosis of CP and the establishment of
follow-up review systems after discharge 14,24. In these less-developed areas, our study revealed that the
number of PaCa and death cases detected during hospitalization and the number of cases of surgical
treatment have decreased in recent years. Therefore, many cases were attracted to large-scale medical
centres in central cities since most patients have higher requirements and standards for medical
treatment. Medical reform still has a long way to go 25,26.
However, the risk of PaCa still exists for patients with CP 2, as shown by that study that cases with PaCa
detected during follow-up were more significantly associated with endoscopic therapy compared to
surgical treatment (0.3 vs. 0.24). Finally, conservative treatment has a strong correlation with jaundice
and PaCa during hospitalization, suggesting that many of these cases might have been diagnosed and
treated extremely late when surgery would have been not possible. In addition to the above, the finding
Page 9/18that conservative treatment was associated with AIP may be another reason for conservative treatment
having a strong correlation with jaundice, since the main treatment of AIP is corticosteroids 9(Figs. 3 and
4, Supplementary Figs. 2 and 5, Supplementary Tables 6, 7, and 8).
PaCa and prognosis
Clinical recognition of new or worrisome symptoms is critical 1, but the correlation between CP and PaCa
is complex 27. Firstly, there is an inevitable overlap between CP and PaCa, and PaCa may sometimes be
mistaken for CP 1. In a study performed by Munigala et al. 18, the authors found that approximately 5% of
patients with PaCa are initially misdiagnosed as CP. Another study performed by Birgin et al. reported that
30.8% of patients with CP who underwent surgery also had synchronous PaCa 28. Secondly, PaCa may be
an incidental finding of CP during pancreatic surgery. PaCa was found by histopathology in 7.1% of the
CP surgical specimens reported by Malinka et al. 29. This was approximately equal to the rate in our
study, in which the proportion of cases with PaCa detected during hospitalization was 7.0% among the
articles that provided data on PaCa or death alone. Compared with endoscopic therapy (r = 0.06), PaCa
detected during hospitalization was more closely related to surgery (r = 0.21). Surgery may be more likely
to detect hidden PaCa compared to endoscopic therapy. Thirdly, PaCa can arise against a background of
CP, although the relative risk varies considerably due to other contributing factors including duration of
the disease, tobacco consumption, excess alcohol consumption, diet and physical activity, and late onset
diabetes mellites 30. Regular follow-up is of great significance, especially in cases with pain, diabetes,
diarrhea and wasting, idiopathic CP, alcoholic CP, hereditary pancreatitis, and cases combined with biliary
diseases during follow-up (Fig. 4, Supplementary Figs. 2C and 5, Supplementary Tables 7 and 8).
Cases of death during hospitalization were directly associated with surgical treatment, and the latter was
related to jaundice, wasting and other suspected risk factors of PaCa. Death during follow-up was related
to all types of CP (except AIP, especially idiopathic and alcoholic CP) (Fig. 4, Supplementary Figs. 2D and
5, Supplementary Tables 7 and 8). Moreover, the number of deaths during follow-up is still very high,
indicating that CP is a serious disease with a high mortality rate, even in patients with a relatively early
diagnosis and admission (Fig. 3) 2,10. It should be noted that PaCa accounts for only 3% of all deaths and
complications due to CP. Comorbid diseases and the effects of alcoholism are the primary cause of death
10
, due to which the variable “PaCa not detected during follow-up” was one of the variables related to
cases of death during follow-up (Supplementary Fig. 2B). Measures to reduce the risk of death should
include early treatment and an interdisciplinary approach and annual follow-ups and evaluations to
monitor disease progression 6.
This study has several limitations. Firstly, due to the different objectives of the researchers or each author,
the clinical data provided were drastically different, which made it difficult to compile the data. Secondly,
most articles had no record of smoking, an independent risk factor for CP, and therefore a correlation
analysis could not be carried out for this important factor 17. Also, due to the great differences in medical
expertise found in the different regions, the diagnostic criteria of alcoholic CP and idiopathic CP used by
Page 10/18many studies could not be obtained or unified. The data was instead recorded according to the authors’
description in the articles. These were the reason for the small correlation coefficients in our results.
Conclusions
In conclusion, with economic and social development, the CP diagnosis, treatment methods and research
has entered a fast-track mode and many regions have gradually formed their own unique approaches
and characteristics. The different clinical characteristics of CP determine the risk of PaCa during
hospitalization or after discharge. Safe endoscopy was primarily found only in economically developed
areas where a variety of complex or rare cases of CP were being treated. Furthermore, the level of the
development determines the level of management of CP, and the latter is closely related to the local
detection level of PaCa, showing that there were likely to be many cases of misdiagnosis or delayed
diagnosis of CP and PaCa. Importantly, the problem of uneven distribution of medical resources, which
related to the imbalance of economic development, needs to be resolved.
Declarations
Ethical Approval
Not applicable.
(This study was a retrospective analysis of clinical case data. All the data in the manuscript came from
the published literatures. The study does not involve any human body research, does not have any
participants, and will not have any impact on clinical decision-making and follow-up. The researchers do
not know the name, gender, age and other identity information of any case. And the study does not
involve any human body research, does not have any specific participants. Therefore, it is not applicable
to the review scope of the ethics committee.)
Competing interests
The authors declare that there are no competing interests associated with the manuscript.
Authors' contributions
Conceptualization, investigation and writing: Wei Wang; Data curation: Weisong Jiang; Methodology and
Formal analysis: Meng Shu, Wei Wang; Resources: Wei Wang, Weisong Jiang; Liying Luo, Ao Liu, Xunke
Pan, Jingjing Liu, Chong Wang, Yizhi Cao, Dongjing Wu, Pengyi Liu, Junyao Xv Yiran Zhou; Supervision
and Project administration: Yiran Zhou and Wei Wang.
Funding
None
Page 11/18Availability of data and materials
Not applicable.
(This study was a retrospective analysis of clinical case data. All the data in the manuscript came from
the published literatures, such as PubMed, EMBASE, Web of Science, China National Knowledge
Infrastructure (CNKI), the Chinese Science and Technology Periodical Database (VIP), Chinese
Biomedicine Literature Database (CBM-SinoMed), and Wanfang Database.)
References
1. Gupte A, Goede D, Tuite R, Forsmark CE. Chronic pancreatitis. BMJ. 2018;361: k2126.
2. Raimondi S, Lowenfels AB, Morselli-Labate AM, et al. Pancreatic cancer in chronic pancreatitis;
aetiology, incidence, and early detection. Best Pract Res Clin Gastroenterol. 2010;24(3):349-58.
3. Amy Y Xiao, Marianne L Y Tan, Landy M Wu, et al. Global Incidence and Mortality of Pancreatic
Diseases: A Systematic Review, Meta-Analysis, and Meta-Regression of Population-Based Cohort
Studies. Lancet Gastroenterol Hepatol. 2016;1(1):45-55.
4. Hirota M, Shimosegawa T, Masamune A, et al; Research Committee of Intractable Pancreatic
Diseases. The seventh nationwide epidemiological survey for chronic pancreatitis in Japan: clinical
significance of smoking habit in Japanese patients. Pancreatology. 2014;14(6):490-6.
5. Beyer G, Habtezion A, Werner J, et al. Chronic pancreatitis. Lancet. 2020;396(10249): 499-512.
6. Lévy P, Domínguez-Muñoz E, Imrie C, et al. Epidemiology of chronic pancreatitis: burden of the
disease and consequences. United European Gastroenterol J. 2014;2(5):345-54.
7. Luo-Wei W, Zhao-Shen LI, Shu-De Li, et al. Prevalence and Clinical Features of Chronic Pancreatitis in
China: A Retrospective Multicenter Analysis Over 10 Years. Pancreas. 2009;38(3):248-54.
8. Shimosegawa T, Kataoka K, Kamisawa T, et al.
The revised Japanese clinical diagnostic criteria for chronic pancreatitis. J Gastroenterol. 2010;
45(6): 584-91.
9. Madhani K, Farrell JJ. Autoimmune Pancreatitis: An Update on Diagnosis and Management.
Gastroenterol Clin North Am. 2016;45(1):29-43.
10. Braganza JM, Lee SH, McCloy RF, et al. Chronic pancreatitis. Lancet. 2011;377(9772):1184-97.
11. Zhao C, Gao F, Li Q, et al. The Distributional Characteristic and Growing Trend of Pancreatic Cancer
in China. Pancreas. 2019;48(3):309-314.
12. Voiosu T, Boškoski I, Tringali A, et al. Chronic Pancreatitis: An Overview of Diagnosis and
Management. Expert Rev Gastroenterol Hepatol. 2020 Jun 8;1-11.
13. Jing-Nan Li, Ya-Min Lai, Jia-Ming Qian, et al. Trends in Etiologies of Chronic Pancreatitis Within 20
Years: Analysis of 636 Cases. Chin Med J (Engl). 2011;124(21):3556-3559.
14. Hao L, Zeng XP, Xin L, et al. Incidence of and risk factors for pancreatic cancer in chronic
pancreatitis: A cohort of 1656 patients. Dig Liver Dis. 2017;49(11):1249-1256.
Page 12/1815. Xi Li, Jiapeng Lu, Shuang Hu, et al. The Primary Health-Care System in China.
Lancet.2017;390(10112):2584-2594.
16. Wenqiang Wei, Hongmei Zeng, Rongshou Zheng, et al. Cancer registration in China and its role in
cancer prevention and control. Lancet Oncol. 2020;21(7): e342-e349.
17. Machicado JD, Chari ST, Timmons L, et al. A Population-Based Evaluation of the Natural History of
Chronic Pancreatitis. Pancreatology. 2018;18(1):39-45.
18. Munigala S, Kanwal F, Xian H, et al. New diagnosis of chronic pancreatitis: risk of missing an
underlying pancreatic cancer. Am J Gastroenterol. 2014; 109(11): 1824-1830.
19. Xiaojie Bo, Jianwei Shi, Rui Liu, et al. Using the Risk Factors of Pancreatic Cancer and Their
Interactions in Cancer Screening: A Case-Control Study in Shanghai, China. Ann Glob Health.
2019;85(1):103.
20. Díte P, Ruzicka M, Zboril V, et al. A Prospective, Randomized Trial Comparing Endoscopic and
Surgical Therapy for Chronic Pancreatitis. Endoscopy.2003;35(7): 553-558.
21. Tillou JD, Tatum JA, Jolissaint JS, et al. Operative Management of Chronic Pancreatitis: A Review.
Am J Surg. 2017;214(2):347-357.
22. Kamisawa T, Wood LD, Itoi T, et al. Pancreatic cancer. Lancet. 2016 Jan 29. pii: S0140-
6736(16)00141-0.
23. LH Hu, Xin L, Zhuan L, et al; Endoscopy Audit of the Chinese Society of Digestive Endoscopy. ERCP
development in the largest developing country: a national survey from China in 2013. Gastrointest
Endosc. 2016;84(4):659-666.
24. Zhao-Shen LI, Wei W, Zhuan L, et al. A long-term follow-up study on endoscopic management of
children and adolescents with chronic pancreatitis. Am J Gastroenterol. 2010;105(8):1884-1892.
25. Ya-min LAI; Tao GUO; Hui DING; et al. Demographic Features, Etiology Trend and Clinical
Characteristics of Chronic Pancreatitis:A Respective Study of 346 Cases in Peking Union Medical
College Hospital Medical Journal of Peking Union Medical College Hospital, 2015; 6(2): 89-95.
26. Wei Wang, Zhuan Liao, Zhao-shen LI, et al. Risk factors of mortality in painful chronic pancreatitis.
Chinese Journal of Pancreatology. 2009; 9(2): 75-78.
27. Harlozinska-Szmyrka A, Strutynska-Karpinska M. The diagnostic dilemmas in discrimination
between pancreatic carcinoma and chronic pancreatitis. Gut. 2004;53(3):469-70.
28. Birgin E, Hablawetz P, Téoule P, et al. Chronic pancreatitis and resectable synchronous pancreatic
carcinoma: a survival analysis. Pancreatology. 2018; 18:394–398.
29. Malinka T, Klein F, Le Thu T, et al. A binational analysis of 252 pancreatic resections for chronic
pancreatitis with regard to incidental carcinoma sequence and overall postoperative outcome.
Anticancer Res. 2018; 38:4947–4952.
30. Greenhalf W, Lévy P, Gress T, et al, Working group for the International (IAP – APA – JPS – EPC)
Consensus Guidelines for Chronic Pancreatitis. International Consensus Guidelines on Surveillance
for Pancreatic Cancer in Chronic Pancreatitis. Recommendations From the Working Group for the
Page 13/18International Consensus Guidelines for Chronic Pancreatitis in Collaboration With the International
Association of Pancreatology, the American Pancreatic Association, the Japan Pancreas Society, and
European Pancreatic Club. Pancreatology.2020; S1424-3903(20)30162-30169.
Figures
Figure 1
Trends in the published articles on chronic pancreatitis from the mainland of China during the period
from 1979 to 2018.
Page 14/18Figure 2
The regional distribution of the reported cases of chronic pancreatitis in the mainland of China based on
the case articles published between 1979 and 2018.
Page 15/18Figure 3
The number of various clinical features reported in chronic pancreatitis articles from the mainland of
China between 1979 and 2018.
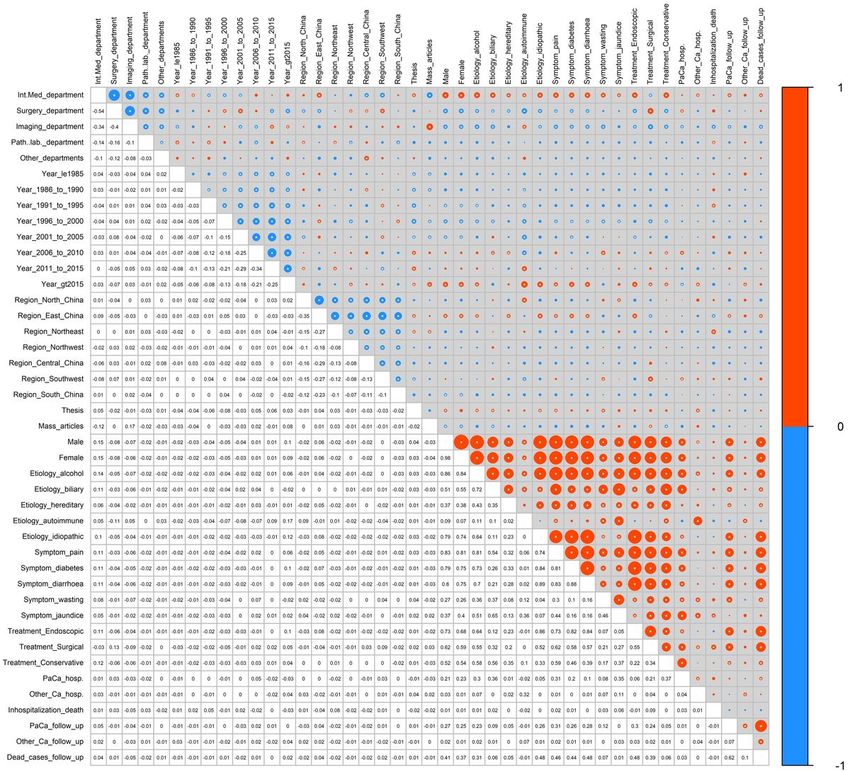
Page 16/18Figure 4
Administrative region level variables - attributable fraction of each variable and related risk factors. The
variables included in the analysis of case articles were divided into two parts. The first part included the
year of publication, the author's department, and the author's region. The second part consisted ofclinical
data including the sex, etiology, clinical manifestations, treatment, incidence of pancreatic cancer (PaCa)
and other cancers, and follow-up. The “*” in the dot indicates a p value < 0.05. The p values were shown
in the Supplementary Table 7. All abbreviations are detailed in Supplementary Table 12.
Page 17/18Figure 5
The proportion of articles on chronic pancreatitis written by different hospitals. [n = the number of
articles, the number of hospitals (percentage)]
Supplementary Files
This is a list of supplementary files associated with this preprint. Click to download.
Supplementarymaterial.zip
Page 18/18You can also read

















































