Recommended Procedure Auditory Brainstem Response (ABR) testing for post Newborn and Adult - Date: November 2016 Due for review: November 2021 ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

1 2 3 4 Recommended Procedure 5 Auditory Brainstem Response (ABR) 6 testing for post Newborn and Adult 7 8 Date: November 2016 9 Due for review: November 2021

Recommended Procedure
Auditory Brainstem Response testing
post new-born and adults
BSA 2016
10 General foreword
11 This Recommended Procedure represents a brief synthesis of the current evidence-base and consensus
12 on Auditory Brainstem Response testing post new-born and adults, as prepared and reviewed by national
13 and international experts, and approved by the British Society of Audiology (BSA).
14 Although care has been taken in preparing this information, the BSA does not and cannot guarantee the
15 interpretation and application of it. The BSA cannot be held responsible for any errors or omissions, and
16 the BSA accepts no liability whatsoever for any loss or damage howsoever arising.
17 Comments on this document are welcomed and should be sent to:
18 British Society of Audiology
19 Blackburn House,
20 Redhouse Road
21 Seafield,
22 Bathgate
23 EH47 7AQ
24 Tel: +44 (0)118 9660622
25 bsa@thebsa.org.uk
26 www.thebsa.org
27
28 Published by the British Society of Audiology
29 © British Society of Audiology, 2016
30 All rights reserved. This document may be freely reproduced in full for educational and not-for-profit purposes. No
31 other reproduction is allowed without the written permission of the British Society of Audiology.
2
Page
© BSA
2016
32 Authors and acknowledgments
33
34 Produced by:
35 The BSA Electrophysiology Special Interest Group (EPSIG) and the Professional Guidance
36 Group
37
38 Key Authors:
39 Michelle Foster (Editor) Sheffield Children’s Hospital
40 Guy Lightfoot ERA Training and Consultancy Ltd
41
42 With Thanks to:
43 The EP SIG would like to thank all of the people who took time to take part in the
44 consultation, we are grateful for your input. In particular to Siobhán Brennan
45 (University of Manchester, Sheffield Teaching Hospitals), Inga Ferm (Croydon Health
46 Services NHS Trust), Amanda Hall (University of Bristol), Vivian Thorpe (NHS Greater
47 Glasgow & Hyde), John Fitzgerald (Norfolk & Norwich University Hospital NHS
48 Foundation Trust), Carolina Leal (Guys and St Thomas London NHS Foundation Trust).
49
© BSA
2016
50 1. Contents
51 General foreword................................................................................................................ 2
52 Authors and Acknowledgments………………………………………………………………………………………3
53 1. Contents ....................................................................................................................... 4
54 2. Introduction ................................................................................................................. 5
55 2.1 Abbreviations ................................................................................................. 5
56 2.2 Scope .............................................................................................................. 6
57 3. General Requirements ................................................................................................. 7
58 3.1 Equipment ...................................................................................................... 7
59 3.2 Staff training and expertise ............................................................................ 7
60 3.3 Accommodation ............................................................................................. 8
61 3.4 Appointments ................................................................................................ 8
62 3.4.1 Infants/Children .............................................................................. 9
63 3.4.2 Adults .............................................................................................. 9
64 3.5 Communication with patient, parents and/or carer ................................... 10
65 3.6 Electrodes..................................................................................................... 10
66 4. Sequence of Tests ...................................................................................................... 11
67 4.1 Introduction ................................................................................................. 11
68 4.2 Test Strategy ................................................................................................ 12
69 4.3 Changes in ABR stimulus level and testing at higher levels ......................... 14
70 4.4 Awake Patient .............................................................................................. 15
71 4.5 Sedation and theatre ................................................................................... 16
72 4.6 Definition of accepting responses ............................................................... 17
73 5. ABR in assessment for candidacy for cochlear implantation .................................... 18
74 6. Reporting ................................................................................................................... 19
75 7. References ................................................................................................................. 19
76 8. Appendices................................................................................................................. 22
77 8.1 Appendix A – Quick reference guide for when test conditions are not ideal
78 ...................................................................................................................... 22
79 8.2 Appendix B: Summary of recommended ABR parameters ........................ 24
80 8.3 Appendix C: ABR Corrections ...................................................................... 25
81 8.4 Appendix E: ABR Examples.......................................................................... 26
82 8.5 Appendix F: The Neurological ABR.............................................................. 30
4
83 8.5.1 Introduction .................................................................................. 30
Page
84 8.5.2 ABR generators and the normal ABR response ............................ 31
85 8.5.3 Factors affecting the ABR .............................................................. 32
86 8.5.4 Test procedure .............................................................................. 36
© BSA
2016
87 8.5.5 Corrections for hearing loss .......................................................... 36
88
89
90 2. Introduction
91 2.1 Abbreviations
92 ABR Auditory Brainstem Response
93
94 AC Air-Conduction
95
96 AEP Auditory evoked potentials
97
98 ANSD Auditory neuropathy spectrum disorder
99
100 AR Artefact rejection
101
102 ASSR Auditory Steady-State Responses
103
104 BC Bone-Conduction
105
106 BSA British Society of Audiology
107
108 CAEP Cortical Auditory Evoked Potentials
109
110 CCTV Closed circuit television
111
112 ckABR Click evoked Auditory Brainstem Response
113
114 CM Cochlear microphonic
115
116 CR Clear Response
117
118 dBeHL Estimated PTA from electrophysiological thresholds
5
119
Page
120 dBnHL Stimulus level relative to adult psycho acoustic threshold.
121 In these guidelines the NHSP reference equivalent
122 threshold levels are used
© BSA
2016
123
124 EEG Electroencephalogram
125
126 EP SIG Electrophysiology Special Interest Group
127
128 Inc Inconclusive
129
130 nABR Neurological Auditory Brainstem Response
131
132 NDCS National Deaf Children’s Society
133
134 OAE Otoacoustic emission
135
136 PTA Pure-Tone Audiometry / Audiogram
137
138 RA Response Absent
139
140 SNR Signal to noise Ratio
141
142 tpABR Tone pip Auditory Brainstem Response
143
144 VRA Visual Reinforcement Audiometry
145 2.2 Scope
146 The scope of this document covers testing infants, children and adults using Auditory
147 Brainstem Response (ABR), an electrophysiological technique. This document assumes
148 the testing is primarily performed when the patient is in natural sleep. Where sedation
149 or anaesthesia is necessary or when testing is performed when the patient is awake, this
150 will be stated. It will also cover the use of the Neurological ABR (nABR).
151
152 For pragmatic reasons, this document will use the following arbitrary terms: baby
153 (corrected age up to 12 weeks); infant (3 to 24 months), child (2 to 16 years) and adult
154 (over 16 years). This guidance does not concern babies. Any baby under three months
155 should be tested / managed with reference to the Guidelines for the early audiological
6
Page
156 assessment and management of babies referred from the newborn hearing screening
157 programme version 3.1. (BSA 2014c)and the related ABR guidance (BSA 2014a) (See
158 guidance at http://www.thebsa.org.uk/resources) or later versions.
159
© BSA
2016
160
161 Behavioural testing should be used to establish threshold measurements for air-
162 conduction (AC) and bone-conduction (BC) using visual reinforcement audiometry
163 (VRA), or pure-tone audiometry (PTA), as appropriate. These measurements should be
164 carried out according to BSA guidance. Where this is not possible due to developmental
165 issues, cognitive/motor issues or non-organic behaviour an electrophysiological
166 assessment should be considered to objectively establish audiological thresholds.
167
168 This document excludes other auditory evoked potentials (including cortical auditory
169 evoked potentials (CAEP) or auditory steady-state responses (ASSR)). Specific BSA
170 guidance on these techniques should be consulted.
171
172 3. General Requirements
173 3.1 Equipment
174 Calibration must be sufficiently comprehensive to allow threshold measurement using
175 clicks by both air and bone conduction, tone pips (also known as brief tones or short
176 tone bursts), and/or chirps. Equipment must be calibrated annually to the reference
177 levels given on the BSA website (http://www.thebsa.org.uk) and undergo regular safety
178 and electrical testing in accordance with BS EN IEC 60601 and local protocols. Stage A
179 listening checks must be carried out before each session.
180 3.2 Staff training and expertise
181 Within each test session as a minimum, the lead person should have the relevant
182 training and expertise to perform the testing, interpret the waveforms and discuss the
183 results with patients and carers.
184
185 The expertise should include the ability to make appropriate and clinically efficient
186 decisions for test strategy, accurately interpret ABR waveforms, accurately determine
187 thresholds (including when and how to use masking) and to know how to deal with
188 unusual or unexpected waveforms or results. In addition, staff within the team should
7
189 have expertise in the discussion of results with parents and patients, the sharing of news
Page
190 and the possible options in management. It is recommended that staff attend an
191 appropriate course such as ‘sharing the news’.
192
© BSA
2016
193 It is good practice to take part and routinely engage in the external peer review of
194 electrophysiological measurements. Guidance on this is currently in preparation by BSA.
195 Paediatric services should be aware of and strive to work within the NHS Paediatric
196 Audiology Commissioning Guidance (NHS England 2016) and any other relevant
197 standards.
198
199
200 In order to achieve and maintain standards it is recommended that staff attend a
201 specialist ABR course as well as any in-house training. To build skills and expertise it is
202 recommended that departments forge links with nearby centres of excellence, local
203 teaching hospitals or neighbouring districts to help find the best way to provide a quality
204 service for these children. It is recommended that a process for auditing of results is in
205 place, including peer review of the waveforms, threshold estimation and test
206 procedures.
207 3.3 Accommodation
208 It is preferable to have an acoustically quiet environment adequate for all
209 recommended hearing threshold test procedures. This is usually achieved by a suitable
210 sound-treated/proofed room. However, where this is not possible then it should be
211 noted that tests performed in areas where the ambient noise is above that normally
212 used in audiometry it may not be possible to detect milder hearing losses. The tester
213 should be aware of this although in an operating theatre setting, the ambient noise will,
214 to a large extent, be beyond the tester’s control. See section 4.5 for testing in sedation/
215 operating theatre.
216
217 Regardless of the age of the patient, the test environment needs to be suitable for
218 electrophysiological testing, with minimal electrical interference. A quick guide to
219 sources of interference and suggestions can be found in section 6.1 Appendix A.
220
221
222
223
8
224 3.4 Appointments
Page
225 The appointment shall be confirmed in writing by the Audiology service along with clear
226 written information about the appointment including the tests that are planned, and
227 their likely duration.
© BSA
2016228 3.4.1 Infants/Children
229 In paediatric settings there shall be family and child friendly waiting room
230 accommodation with space to feed, change and settle children. Also a travel cot or child
231 friendly bed may be appropriate.
232
233 For infants and children where testing in natural sleep is envisaged, the information
234 given prior to the appointment shall state that they need to arrive awake but tired, and
235 ready to sleep in clinic. Appointment times should be flexible within reason to fit in with
236 the child’s routine. Time shall be allowed for the child to be settled, and there must be
237 facilities for preparing feeds/feeding etc. It should be clear that this is an assessment
238 appointment and that parents are welcome to be accompanied by a friend or relative, if
239 they wish. Any practical upper limit on the number of adults wishing to attend shall be
240 stated in the appointment letter. Separation of children from their parents often
241 accentuates anxiety and results in uncooperative behaviour, especially in toddlers and
242 pre-school children. Parents should usually remain throughout the entire procedure and
243 be involved in preparation of the child, where appropriate, as the presence and
244 involvement of a parent may reduce the need for pharmacological intervention. Their
245 presence may greatly reduce the distress caused by separation anxiety. Reference
246 should be made to the National Service Framework for Children (Department of Health
247 2004).
248 3.4.2 Adults
249 For adults, a reclining chair or couch is beneficial. Electrophysiological testing of adults
250 should be in conjunction with a battery of other testing such as PTA. In suspected
251 possible non-organic patients it is worth informing the patient that the results will be
252 compared to the PTA. If ABR is going to be attempted in an awake subject extreme
253 caution should be taken interpreting and reporting the results. It is worth considering
254 CAEP testing in awake adults, for which there is a separate BSA Recommended
255 Procedure (BSA 2016). When the test is carried out from a separate room it is essential
256 to be able to monitor the patient and communicate with them through an intercom
257 system and window/CCTV system.
258
259 No more than two patients should be booked into a morning or afternoon clinical session
260 as sufficient time should be allowed for each patient. In a theatre setting it may not be
9
261 possible to book more than one patient. It is important to liaise with theatre staff when
Page
262 planning sessions to ensure sufficient time is reserved for each case.
263
© BSA
2016264 3.5 Communication with patient, parents and/or carer
265 The reason and procedure for each test should be explained to the patient and/or
266 parents/carers. It is also important to go through the test results in appropriate detail as
267 required by each individual patient or carer at the time of the appointment. When an
268 ABR threshold has been obtained it can also be useful to arrange for the parents/carer
269 to listen to the stimulus at threshold level so that they are aware of the sound level at
270 which a response is obtained (in doing this bear in mind the offset between the ABR
271 threshold and the psychoacoustic/PTA threshold). A written report should be provided
272 as per local protocol.
273
274
275 Patients, parents and/or carers of children should be provided with appropriate verbal
276 and written information at the end of the assessment. This may include a checklist or
277 departmental leaflet, where hearing is satisfactory. Where a hearing loss is confirmed
278 the appropriate support should be given in accordance with local and national guidance.
279 If the type of hearing is yet to be determined, then contact details (telephone/
280 departmental email address) should be given together with the details of the next
281 appointment.
282
283 3.6 Electrodes
284 The skin should be prepared using an appropriate paste and/or gauze and single use
285 electrodes shall be used. All procedures must comply with local infection control
286 policies. It is essential to ensure that inter-electrode impedances are below 5k,
287 preferably below 2k and are balanced as far as practicable across pairs of electrodes.
288 This will be especially important in an operating theatre setting, where electrical
289 interference is likely to limit the quality and precision of the results.
290
291 If a single channel recording is to be used, the following electrode placement is
292 recommended:
293
10
294 Infants:
295 Positive (non-inverting) electrode: high forehead
Page
296 Negative (inverting) electrode: ipsilateral mastoid
297 Common electrode: contralateral mastoid
298
299 Children/Adults:
© BSA
2016300 Positive (non-inverting) electrode: Cz (vertex)
301 Negative (inverting) electrode: ipsilateral mastoid
302 Common electrode: contralateral mastoid
303 Either configuration should result in Wave V being plotted upwards.
304
305 Different equipment may recommend a range of electrode montages and therefore the
306 tester should ensure they know the rationale for the manufactures suggested montage
307 and be able to justify their choice of montage.
308
309 Alternatively a 4 electrode array could be used if additional testing is being considered,
310 for example 2-channel ABR or ASSR.
311
312
313 4. Sequence of Tests
314 4.1 Introduction
315 The order and range of tests undertaken will be greatly influenced by the sleep state of
316 the patient, and the diagnostic purpose of the test. Sleep or a very relaxed awake state
317 (with little muscle activity) is highly desirable for ABR testing but is often difficult to
318 achieve in older children and adults.
319
320 For the initial diagnostic appointment, it is recommended that the initial stimulus is 4
321 kHz tpABR at 40-50 dBnHL unless a more significant hearing loss is suspected, when 60
322 dBnHL may be more appropriate.
323
324 Discharge criteria should be defined locally as it will be determined by the clinical
325 picture. A suggested minimum discharge criterion could be the establishment of AC 4
326 kHz tone pip auditory brainstem responses (tpABR) thresholds predicting estimated
327 hearing thresholds ≤ 30 dBeHL in both ears. Where time allows thresholds should be
328 obtained at 20dBeHL. However this will vary depending on the clinical question being
329 addressed.
330
11
331 No other testing will usually be required if hearing is normal at 4 kHz, except in cases of
332 meningitis or where more information is needed clinically. The main reason for
Page
333 recommending starting with 4 kHz, is that the quietest parts of speech are around this
334 frequency and using a lower frequency may miss some ski slope hearing impairments. It
335 also has a practical advantage as 4 kHz is the frequency that testers are more familiar
© BSA
2016336 with using and therefore could be thought of as being the easiest of the tpABR to
337 record.
338
339 After assessing 4kHz in both ears if the threshold is significantly raised at 4 kHz then it is
340 important to test at lower frequencies AC tpABR (1 kHz is recommended).
341 4.2 Test Strategy
342 In general, the testers should use the BSA ABR testing in Babies (2018a) guidance on
343 ABR testing in babies as a reference but when performing ABR tests on infants, children
344 or adults, there can be a variety of technical challenges, most of which are related to
345 interference from the patient or from other equipment.
346
347 It is essential that the clinician maximises the information obtained to answer the
348 clinical question being addressed by the ABR assessment. In many clinical scenarios the
349 following strategy is appropriate and may be followed and solutions attempted, in the
350 following order, until satisfactory results are obtained.
351
352 Start with 4-kHz tpABR with the artefact rejection (AR) criterion initially set to 5 µV as
353 per the BSA NHSP Early Assessment Guideline (2014). See below for steps to be taken
354 when an AR of 5µV leads to total rejection. A summary of the test parameters can be
355 found in Appendix B. All the AC and BC correction factors that are stated in NHSP
356 guidance still apply for any ABR. A summary of this can be found in Appendix C.
357 Appendix D sets out the definition of ABR thresholds.
358
359 The clinician should start with the ear better ear and move onto testing the other ear.
360 Following establishing the AC threshold in one ear at 4kHz, the tester can move to test
361 the other ear by AC at 4 kHz.
362 Test by BC at 4 kHz tpABR to determine if any raised threshold is due to a conductive
363 component, though at this stage there may be insufficient information available to
364 select an appropriate level of noise for masking the non-test ear. Note that the 2-
365 channel method of determining whether cross-hearing is present, whilst valid in the
366 newborn period, should not be used for adults or children over 2 years because it may
367 give unreliable results.
12
368 This may be all that is possible to obtain on a good test session with infants and children
Page
369 but where possible, testing should continue until all the required information has been
370 obtained.
371
© BSA
2016372 Where possible use AR set to 5 µV; in good recording conditions this low AR and a
373 modest number of sweeps (e.g. 2000) can usually produce good results although the
374 requirement for an SNR of 3:1 must always be the overriding goal.
375
376 If the majority of sweeps are rejected, then the tester should attempt to identify and
377 exclude the source of the interference. Ensuring that the electrode impedances are 10 µV.
399 Failure to use an adequate number of sweeps is likely to result in inconclusive
400 waveforms.
401
402 The recommended gain is 240 000 and gain is also related to AR. The tester should have
403 knowledge of the trade –off if they are to change the gain. The analogue to digital
404 converter (ADC) of most systems permits a maximum output voltage of 5V (5,000,000
405 µV). The signal from the patient (which is mostly unavoidable noise) is nowhere as big
13
406 as this, so the signal needs to be amplified. For example, amplifying a signal of ±10 µV by
Page
[1] When a notch filter is used this must be noted in the clinical report. The available evidence is that notch filtering does not distort the new-born ABR,
with the exception of testing at 500 Hz where waveform distortion has been observed and could compromise waveform interpretation. At 500 Hz
therefore the notch filter must not be used. (Updates to NHSP guidance for post-screening diagnostic testing, Update 1: August 2015).
© BSA
2016407 a factor of 240,000 (a gain of 240,000) will result in a signal of 4.8 V, thus taking
408 advantage of almost the entire available dynamic range of the ADC. If the AR is to be
409 increased above ±10 µV the amplifier gain must be correspondingly reduced, for
410 example to 150,000, where an AR up to ±16 µV is possible.
411
412 If the equipment has Bayesian averaging then this should be employed.
413
414 AC click ABR (ckABR) should be considered for threshold estimation purposes only if it is
415 clear that it may not be possible to measure AC tpABR thresholds, where it is important
416 to quickly get some estimate of hearing threshold or where there is no tpABR response
417 at the normal maximum stimulus level. In the latter case, it may be considered clinically
418 useful to see if an ABR response to click stimuli can be recorded (the ckABR response
419 may be recordable at high stimulus levels with absent tpABR). Such additional
420 assessment is important when the testing conditions are not ideal (e.g. in operating-
421 theatre setting) and behavioural testing is unobtainable and the main aim of the
422 procedure is to get an approximate baseline for the hearing thresholds.
423
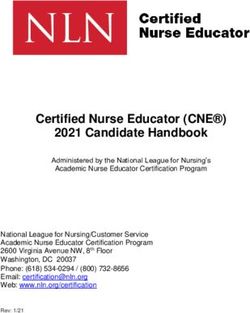
424
425 Figure 1: Flow diagram illustrating a possible clinical decision making process for
426 determining the optimum artefact rejection level to use and the number of sweeps
427 needed.
428
14
Page
429 4.3 Changes in ABR stimulus level and testing at higher levels
430 Changes in stimulus level should normally be in 10 dB steps depending on the nature of
431 the case. Occasionally, e.g. where there is strong recruitment, a 5 dB step may be useful,
© BSA
2016432 but care should be taken not to spend time on small changes in stimulus levels at the
433 expense of producing definitive outcomes at 10dB intervals around threshold. There
434 may also be occasions when it is better to use larger steps, for example where an infant
435 may stay asleep for only a few test levels. As an illustration of this, by testing at 40, 60
436 and 80 dBnHL and determining that the ABR threshold lies between 60 and 80 dBnHL, a
437 more useful outcome is achieved than by having increased the level in 10 dB steps from
438 40 dBnHL and being able to determine only that the ABR threshold is above 60 dBnHL.
439
440 If there is no response at the normal maximum permissible stimulus level to tpABR (as
441 defined in BSA NHSP Early Assessment Guideline (20142) or only abnormal waveforms at
442 high stimulus levels (≥75 dBeHL), then Auditory Neuropathy Spectrum Disorder (ANSD)
443 may be present. Tests should then be carried out for cochlear function. Refer to the BSA
444 guidelines on Cochlear Microphonic (CM) (BSA 2018b)or testing and guidelines for the
445 assessment and management of ANSD in young infants (BSA 2018c ) which should be
446 followed. Note that ANSD can be confirmed only when, using the same stimulus level
447 and transducer, a CM is present but a ckABR is absent.
448 4.4 Awake patient
449 It is always preferable to test the patient using ABR whilst asleep. However this is
450 sometimes not possible.
451
452 tpABR or ckABR testing can be attempted with a patient who is awake, but only if they
453 are physically very relaxed, with a quiet background EEG3. Extra care must be taken to
454 ensure that any results collected are of good quality (residual noise below 40 nV) and
455 replicated. One of the most important issues will be to know when to stop averaging at
456 a given stimulus level. It is better to collect a few results of high quality that can add
457 value to the clinical test battery than report on inconclusive or inaccurate results that
458 are degraded by noise. The advice given in section 4.2 applies. If accurate results are
459 needed and the patient does not sleep or settle then sedation should be considered in
460 collaboration with medical staff and in line with local hospital procedures for
461 administration and after care. If the patient is awake and the background “EEG” is too 15
2 For adults and children over 2 years the maximum stimulus levels for both inserts and supra-
aural earphones are those quoted for supra-aural earphones in the Early Assessment guidance
Page
since there is no age-related correction for age for these groups.
3 “EEG” in this context means the incoming electrical activity sensed by the electrodes from brain.
In practice what we see is usually dominated by muscle activity, cardiac activity and electrical
interference rather than true EEG activity.
© BSA
2016462 noisy, ABR testing is unlikely to yield reliable results. In such circumstances it is
463 appropriate to reconsider behavioural testing and/or re-testing the patient at a time of
464 the day when they are more likely to sleep naturally, or consider sedation in line with
465 local policy. With an adult patient, CAEP or 40 Hz ASSR testing should be considered as
466 viable alternatives.
467 A recent audit at Sheffield Children’s NHS Foundation Trust looked at the outcomes of
468 patients who were referred for ABR testing during a 6 month period. It was found that
469 in infants (3-24 months) it was possible to obtain satisfactory tpABR results in 87% of
470 occasions under natural sleep. However, for the children (> 2 years), it was possible to
471 obtain a reliable result under natural sleep in only 27% of cases. For the remaining
472 children, no useful tpABR results were obtained as the patient did not sleep or settle
473 sufficiently to obtain reliable results.
474 4.5 Sedation and theatre
475 Sedation is not necessary in babies and should be used in infants only in exceptional
476 circumstances. One of the advantages of early assessment is that babies/infants can be
477 tested relatively easily during natural sleep. Parents need to be made aware of the
478 requirements for a sleeping or settled infant and where possible appointments should
479 be timed appropriately.
480 Where sedation or general anaesthesia is being considered, the patient should be under
481 the care of an appropriate physician. Each centre must adhere to their hospital
482 requirements and gain consent from patients as required according to each hospital’s
483 policy and make necessary arrangements for admission onto an appropriate ward if
484 necessary. The patient and/or carer should give their consent for the audiology
485 assessment. The patient will need to be given separate information about the
486 admission times on the ward, nil by mouth procedure, etc. The clinician should aim to
487 coordinate the appointment with any other treatment the patient may be receiving, as
488 it is often favourable to have everything carried out at the same time.
489
490 The operating theatre is not an ideal environment for ABR measurements, but if care is
491 taken, good results can usually be obtained. It is essential that the patient is kept
492 anesthetised for the duration of the test and this will require communication between
493 the audiologist and the anaesthetist, in particular with regard to the anticipated
16
494 duration of the procedure. Some equipment commonly used in theatre (warming
Page
495 blankets, pulse oximeters) may create additional interference and if this is the case
496 should be avoided, following consultation with the anaesthetist. The ABR equipment
497 should be plugged directly into a mains socket and not an extension. If a mains
498 extension is unavoidable, no additional equipment shall be connected to the extension.
© BSA
2016499 The grouping (braiding or twisting together) of electrode leads and their physical
500 separation from other cables is particularly important in theatre as a means of
501 minimising electrical interference. Headphone covers should be used with supra-aural
502 earphones after any surgical ear procedure. There are advantages of using inserts:
503 1. If the ear has been aspirated or cleared of wax and there is still some fluids then
504 elevating the tubing could reduce infection control risks and the tubing is easier to
505 change.
506 2. Inserts can help reduce the level of ambient noise if the ear tip has been fitted well.
507 Clinicians should be aware that following middle ear surgery there may be a temporary
508 threshold shift or a conductive loss associated with a blood-filled ear canal. It is also
509 possible to see a conductive loss reappear during testing if unaspirated fluid refills the
510 middle ear cavity.
511 4.6 Definition of accepting responses
512 ABR threshold is defined as the lowest level at which a clear response (CR) is present,
513 with a response absent (RA) recording at a level 5 or 10dB below the threshold,
514 obtained under good recording conditions. For definitions of CR and RA refer to the BSA
515 guidance on ABR testing in babies (BSA 2018a ).
516
517 For CR there must be a high degree of correlation between the replications and the
518 waveforms should show the expected characteristics in terms of amplitude, latency and
519 morphology. The size/amplitude of the response (as judged from the wave III/V to the
520 following SN10 trough) should be a minimum of 40 nV and at least 3 times the
521 background noise level (the noise level can be estimated from the average difference
522 between optimally superimposed waveforms). The waveform should be judged over the
523 whole time window excluding any stimulus artefact.
524 Waveforms should be compared with those at other stimulus levels (where available) to
525 confirm that they follow the expected changes with stimulus level.
526 The SNR could be relaxed to 2.5 to 1 in difficult testing conditions such as in the
527 operating theatre but in so doing, the tester must acknowledge the increased risk in
528 mistaking noise for a valid response and thus underestimating the ABR threshold.
529
530
17
531 For RA the waveforms must be appropriately flat, with no evidence of a response and
Page
532 the average difference (noise) between a pair of optimally superimposed waveforms
533 should be less than or equal to 25 nV (using the same method for measuring
534 background noise for CR described above). All other responses not meeting either
535 criteria should be marked Inconclusive (Inc). The residual noise criterion could be
© BSA
2016536 relaxed (but to no more than 40 nV) in difficult testing conditions such as in the
537 operating theatre but in so doing, the tester must acknowledge the increased risk in
538 failing to identify a small response obscured by noise and thus overestimating the ABR
539 threshold.
540
541
542 5. ABR in assessment for candidacy for cochlear implantation
543 ABR testing can be performed as part of the audiological assessment of candidacy for CI
544 in infants and children. In adults, CAEP testing may be used as an adjunct to behavioural
545 assessment of their hearing.
546
547 Frequency specific results are required for CI implantation. Nice Guidelines (NICE 2009)
548 state that the minimum that should be tested is 2 at 4 kHz bilaterally. TpABR at 2 kHz
549 and 4 kHz should be considered carefully in conjunction with other test results (e.g.
550 otoacoustic emissions (OAEs), tympanometry and behavioural hearing tests).
551
552 In patients were ABR results are absent or of abnormal waveform morphology, the
553 possible presence of ANSD must be considered and the appropriate investigations
554 employed (re: OAE, ABR-CM and tympanometry (BSA 2014b). These patients may
555 benefit from a cochlear implant. However, there is a wide variation in the behavioural
556 responses and actual hearing ability between individuals with ANSD. Thus the ABR alone
557 would not be enough to ascertain the appropriateness of cochlear implantation for a
558 patient with ANSD.
559
560 It should be recognised that it is possible that maturation of the ABR response can be
561 delayed by up to 18 months or more (Spitzer et al. 2015). Cases of recovery of the ABR
562 up to 6-24 months after an initial diagnosis of ANSD have been reported (Psarommatis
563 et al. 2006; Raveh et al. 2007). It is therefore recommended that the ABR is repeated. To
564 help differentiate neural maturation changes from other causes of ANSD, whenever
565 possible ABR should be repeated before a definitive initial diagnosis is made.However
566 each case must considered individually for CI and departments should liaise with CI
567 centres over specific cases to avoid unnecessary delays.
568
18
569 As improvements in ABR and in behavioural thresholds over the early months of life
Page
570 have been reported in some infants, a further repeat ABR at a later age may be helpful
571 in order to confirm the diagnosis. If this is felt to be helpful for the management of the
572 individual case, then a re-test at around 12-18 months of age should be considered as
573 per the BSA guidance.
© BSA
2016574
575
576
577
578
579 6. Reporting
580 At each test session results should be documented in detail as the session proceeds. It is
581 important that appropriate professionals are kept informed of the outcome of each
582 episode of the assessment (even if few or no results are obtained). An example of a
583 report is available on the BSA website. Non-attendance and the subsequent plans
584 should be reported appropriately.
585
586 The report should include:
587 A summary of the reason for the test session.
588 A brief medical history of relevant factors relating to hearing loss.
589 A summary of the electrophysiological results, including warnings where the threshold
590 has not been accurately determined, where threshold is above the maximum available
591 stimulus level or where the results are subject to poor recording conditions. The
592 consistent use of ≤, = & > when reporting results is preferable to phrases such as
593 “responses seen down to…”
594 A description of any sedation or anaesthetic used.
595 A description of the test environment including information regarding any factors which
596 may have influenced test interpretation.
597 A full outline of any adjustments to parameters required and information written for a
598 lay reader on the impact these may have on result interpretation.
599 A note of any other factors that might affect the estimate of the hearing threshold, as
600 measured by the ABR (e.g. possible ANSD, evidence from other tests of possible
601 neurological damage to the brain).
602 A report of any consistent behavioural reactions taking account of their limitations.
603 A comment on any other test results obtained at the same session.
604
19
605 7. References
Page
606
607 BRITISH SOCIETY OF AUDIOLOGY (2018a) Recommended Procedure Auditory Brainstem
608 Response (ABR) Testing in Babies, [Online]. Available from:
© BSA
2016609 https://www.thebsa.org.uk/wp-content/uploads/2019/04/Recommended-
610 Procedure-for-ABR-Testing-in-Babies-FINAL-Feb-2019.pdf. Accessed 17/04/2019
611 BSA, (NHSP), 2018b. Guidelines for Cochlear Microphonic Testing, Available at:
612 http://www.thebsa.org.uk/wpcontent/uploads/2015/02/CM_Guidance_v2_21091
613 1.pdf.
614 BSA, (NHSP), 2014c. Guidelines for the Early Audiological Assessment and Management
615 of Babies Referred from the Newborn Hearing Screening Programme, Version 3.1,
616 July, 2103, Available at: http://www.thebsa.org.uk/wp-
617 content/uploads/2014/08/NHSP_NeonateAssess_2014.pdf.
618 BRITISH SOCIETY OF AUDIOLOGY (2018d) Recommended Procedure Assessment and
619 Management of Auditory Neuropathy Spectrum Disorder (ANSD) in Young Infants
620 [Online]. Available from: insert web link. 'in consultation'. [Accessed date].
621 BSA, 2016. Cortical Auditory Evoked Potential (CAEP) Testing, Available at:
622 http://www.thebsa.org.uk/wp-content/uploads/2016/05/Cortical-ERA.pdf
623 [Accessed September 15, 2016].
624 BS EN, 2015. 60601-1-11:2015 Medical electrical equipment – Part 1-11: General
625 Requirements for Basic Safety and Essential Performance.
626 Burkard, R. & Don, M., 2012. The Auditory Brainstem Response. In K. Tremblay & R.
627 Burkard, eds. Translational Perspectives in Auditory Neuroscience. Hearing Across
628 the Lifespan —Assessment and Disorders. San Diego: Plural Publishing, pp. 161–
629 200.
630 Bush, M.L., Jones, R.O. & Shinn, J.B., 2008. Auditory Brainstem Response Threshold
631 Differences in Patients with Vestibular Schwannoma: A New Diagnostic Index. Ear,
632 Nose, & Throat Journal, 87(8), pp.458–62.
633 Department of Health, 2004. National Service Framework for Children, Young People and
634 Maternity Services, Available at:
635 http://webarchive.nationalarchives.gov.uk/20130401151715/http://education.gov.
636 uk/publications/eorderingdownload/dh-40493pdf.pdf [Accessed September 18,
637 2016].
638 Gorga, M.P. et al., 1987. Auditory Brainstem Responses from Graduates of an Intensive
639 Care Nursery: Normal Patterns of Response. Journal of Speech and Hearing
640 Research, 30(3), pp.311–8.
641 Hall, J.W., 2007. New Handbook of Auditory Evoked Responses 1st ed., Pearson.
642 Hyde, M.L. & Blair, R.L., 1981. The Auditory Brainstem Response in Neuro-otology:
20
643 Perspectives and Problems. The Journal of Otolaryngology, 10(2), pp.117–25.
644 Jewett, D.L. & Williston, J.S., 1971. Auditory-evoked Far Fields Averaged from the Scalp
Page
645 of Humans. Brain : A Journal of Neurology, 94(4), pp.681–96.
646 Kirsh, I. et al., 1992. The Effect of Cochlear Hearing loss on Auditory Brain stem
647 Response Latency. Ear and Hearing, 13(4), pp.233–5.
648 Lightfoot, G., 1992. ABR Screening for Acoustic Neuroma: the Role of Rate-induced
© BSA
2016649 Latency Shift Measurements. British Journal of Audiology, 26, pp.217–227.
650 Lightfoot, G., 1993. Correcting for Factors Affecting ABR Wave V Latency. British Journal
651 of Audiology, 27, pp.211–220.
652 Lightfoot, G. & Stevens, J., 2014. Effects of Artefact Rejection and Bayesian weighted
653 Averaging on the Efficiency of Recording the Newborn ABR. Ear and Hearing, 35(2),
654 pp.213–20.
655 Møller, A.R. et al., 1995. Contribution from Crossed and Uncrossed Brainstem Structures
656 to the Brainstem Auditory Evoked Potentials: A Study in Humans. The
657 Laryngoscope, 105(6), pp.596–605.
658 NHS England, 2016. SCHEDULE 2 – THE SERVICES A. Service Specifications, Available at:
659 https://www.england.nhs.uk/wp-content/uploads/2016/07/P37-CYP-Service-
660 Specification-Template.pdf [Accessed November 5, 2016].
661 NICE, 2009. Cochlear implants for children and adults with severe to profound deafness.
662 Guidance and guidelines., NICE. Available at:
663 https://www.nice.org.uk/guidance/ta166 [Accessed November 4, 2016].
664 Psarommatis, I. et al., 2006. Transient Infantile Auditory Neuropathy and its Clinical
665 Implications. International Journal of Pediatric Otorhinolaryngology, 70(9),
666 pp.1629–37. Available at: http://www.ncbi.nlm.nih.gov/pubmed/16769129.
667 Raveh, E. et al., 2007. Auditory neuropathy: clinical characteristics and therapeutic
668 approach. American Journal of Otolaryngology, 28(5), pp.302–8. Available at:
669 http://www.ncbi.nlm.nih.gov/pubmed/17826530 [Accessed September 18, 2016].
670 Selters, W.A. & Brackmann, D.E., 1977. Acoustic Tumor Detection with Brain Stem
671 Electric Response Audiometry. Archives of Otolaryngology (Chicago, Ill. : 1960),
672 103(4), pp.181–7.
673 Spitzer, E. et al., 2015. Continued Maturation of the Click-evoked Auditory Brainstem
674 Response in Preschoolers. Journal of the American Academy of Audiology, 26(1),
675 pp.30–5. Available at: http://www.ncbi.nlm.nih.gov/pubmed/25597458 [Accessed
676 September 18, 2016].
677 Stevens, J. et al., 2013. Predictive Value of Hearing Assessment by the Auditory
678 Brainstem Response Following Universal Newborn Hearing Screening. International
679 Journal of Audiology, 52(7), pp.500–6.
680
681
21
Page
© BSA
2016682 8. Appendices
683 8.1 Appendix A – Quick reference guide for when test
684 conditions are not ideal
685 1) Ensure optimum test conditions e.g. impedances low, interference limited,
686 patient is asleep where possible.
687 DON’T’s:
688 Don’t wake a sleeping patient (associated with excessive muscle activity).
689 Don’t test in a noisy room.
690 Don’t use florescent lighting, low energy lighting or light dimming controls as
691 these can cause interference.
692 Don’t have non-essential electrical equipment turned on. In cases where
693 electrical interference proves to be detrimental to recording quality, attempt to
694 limit electrical background noise levels by switching off any that is in the test
695 room or within close proximity to the recording electrodes issue to recording
696 quality.
697
698 DO’s:
699 Do place equipment at least 1m away from the patient and not near any
700 electrical trunking or power sockets.
701 Do physically separate leads/cabling, especially electrode / transducer / power
702 supply leads.
703 Do ensure mobile phones are switched off or are in flight mode.
704 Do run electrode leads close together. If stimulus artefact is a problem plait
705 longer electrode leads or use short electrode leads, gathered or twisted
706 together.
707
708 2) tpABR following NHSP early guidance should be followed.
709 3) If the AR level is increased also increase the number of sweeps collected
710 appropriately (see Fig 1); note that the relationship is not linear. If the AR level
711 has to be relaxed above 10 µV in order to record anything then very large
22
712 number of sweeps will be necessary and this will influence test strategy (e.g.
Page
713 require 20 dB steps). It is usually false economy to “try a different
714 frequency/ear”; it is better to resolve the current test than to obtain many
715 waveforms, all of which are inconclusive.
© BSA
2016716 4) Apply a notch filter only if this helps (notch filter should not be used when
717 testing at 500Hz), otherwise, troubleshoot for other sources of interference.
718 5) Stimulus artefact “blocking” (flat line display option) can help reduce the effect
719 of a large stimulus artefact at high stimulus levels but may compromise
720 interpretation in low-frequency tpABR. This option should not be selected for
721 CM testing.
722 6) Attempt ckABR instead of tpABR only when necessary and be aware of the
723 limitations of this type of testing.
724 7) Maximise the available time by obtaining the most clinically crucial information
725 first at as high a quality as possible. For example, is there any hearing?
726 8) Know when to stop. If test conditions are poor and the results are very unclear it
727 is better to bring the patient back and try again. This approach has merit only if
728 the problems encountered in the first session have been identified and steps
729 taken to avoid their recurrence.
730
731 It is better to collect a few good/high quality results than many that are inconclusive
732 or of questionable reliability.
733
734
735
23
Page
© BSA
2016736 8.2 Appendix B: Summary of recommended ABR threshold
737 assessment parameters
Click, NB chirp & 2 kHz / 4 kHz 0.5 kHz / 1 kHz tone pip
tone pip
Electrode location Positive : Cz or High forehead (as close to vertex as possible but
avoiding fontanelle)
Negative : Ipsilateral mastoid
Common : Contralateral mastoid
Stimulus type Alternating polarity
Stimulus timing Click: 100µs.
Tone pip: 2-1-2 cycles (linear rise–plateau–fall) or 5-cycle
Blackman
Stimulus rate 45.1 - 49.1/s 35.1 - 39.1/s
17.1 - 19.1/s for wave I on BC
Calibration values for Refer to NHSP calibration data
0dBnHL
Amplifier reject levels ±3 to ±10 µV where possible peak-to-peak. Start at ≤±5 µV peak-
to-peak. Exceed ±10 µV only after reducing interference
Amplifier filters Low frequency: 30 Hz
High frequency: 1500 Hz
Window length4 20 ms 25 ms
Number of sweeps If the artefact rejection level is ±5 µV:
averaged per replication Typically: 2000 click & NBchirp, or 3000 for TP
Minimum: 1500 click & NBchirp, or 2000 for TP
If the artefact rejection level is >±5 µV see Fig 1
Display scales Within range 25-100 nV ≡ 1 ms
See equipment specific settings.
Display Wave V up
738 Table 1 (http://www.thebsa.org.uk/wp-content/uploads/2014/08/NHSP_ABRneonate_2014.pdf.)
24
739
Page
© BSA
2016740 8.3 Appendix C: ABR corrections
Click Tone pip Chirp
0.5kHz 1kHz 2kHz 4kHz 0.5kHz 1kHz 2kHz 4kHz
Insert phones 0 20 15 10 5 15 10 5 0
Headphones 5 20 15 10 10 15 10 5 5
Bone conductor 5 0 0 10 5 -5 -5 5 0
741 Table 2: Infants tested between 12 weeks and 24 weeks corrected age (85 to 168 days).
742 Value in dB to be subtracted from the ABR nHL threshold to give eHL thresholds.
743
Click Tone pip Chirp
>24wk 0.5kHz 1kHz 2kHz 4kHz 0.5kHz 1kHz 2kHz 4kHz
Insert phones 5 20 15 10 10 15 10 5 5
Headphones 5 20 15 10 10 15 10 5 5
Bone conductor 5 5 5 10 10 0 0 5 5
744 Table 3: Infants tested between 24 weeks and 2 years (168 to 730 days) corrected age.
745 Value in dB to be subtracted from the ABR nHL thresholds to give eHL thresholds.
746
Click
Tone pip Chirp
0.5kHz 1kHz 2kHz 4kHz 0.5kHz 1kHz 2kHz 4kHz
Insert earphones 5 20 15 10 10 15 10 5 5
Headphones 5 20 15 10 10 15 10 5 5
Bone conductor 5 20 15 10 10 15 10 5 5
747 Table 4: Children/Adults tested over 2 years (730 days). Value in dB to be subtracted
748 from the ABR nHL thresholds to give eHL thresholds.
25
749
Page
© BSA
2016750 8.4 Appendix E: ABR Examples
751
752
753
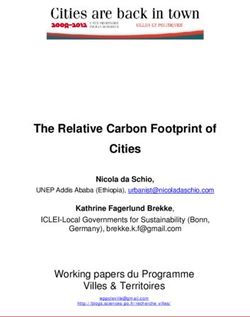
754 Figure 2: Sine wave interference.
755 The rolling sine wave is at 450Hz so probably unrelated to mains interference. It is not
756 possible from these waveforms to establish threshold. It would be appropriate to spend
757 time trouble shooting and attempting to eliminate the source of interference. One
758 strategy worth trying with periodic interference is to slightly reduce the stimulus
759 repetition rate: whatever the period of the interference, our stimulus rate should be
760 mathematically unrelated to it.
26
Page
© BSA
2016761
762 Figure 3: Difficult Test conditions in Theatre: Results are inconclusive because the
763 waveforms are dominated by excess noise since a very lax AR level was used without an
764 appropriate increase in the number of sweeps.
27
Page
© BSA
2016765
766 Figure 4: ABR carried out in Theatre, in good conditions
767 28
768 Figure 5: Repeatable ABR results from an awake patient on the left. On the right only
769 65dBnHL can be accepted as a clear response. At lower levels there is excess residual
Page
770 noise and the morphology of the ABR does not follow the expected pattern.
© BSA
2016771
772 Figure 6: Notch filter used to improve quality. The upper waveforms do not have the
773 notch noise filter applied whereas the lower waveforms do have the notch noise filter
774 applied.
775
29
Page
© BSA
2016776 8.5 Appendix F: The neurological ABR
777 8.5.1 Introduction
778 The main body of this document describes the threshold application of the auditory
779 brainstem response (ABR) to provide an objective estimate of the auditory threshold,
780 which can be thought of as a surrogate for the pure-tone audiogram (PTA). This
781 appendix describes the use of the ABR to access and evaluate the functional integrity of
782 the ascending auditory neural pathways. The neurological ABR (nABR) is therefore less
783 concerned with the status of the ear but can instead be considered a neurological test.
784
785 In the threshold ABR, the main test objective is to determine whether a response to a
786 particular audiological stimulus is present (inferring that the stimulus has been detected
787 by the ear and is therefore above the hearing threshold) or absent (stimulus not
788 detected by the ear and therefore below the hearing threshold) and the test
789 parameters, procedure and waveform interpretation techniques are optimised to that
790 end. Briefly, an ABR waveform is recorded at a variety of stimulus levels until the ABR
791 threshold becomes apparent. In the nABR, the test focuses not on response detection
792 but rather on analysis of the nABR waveform as a barometer of neurological function. It
793 is therefore unsurprising that the two ABR tests differ in terms of test parameters,
794 procedure and analysis.
795
796 In the nABR, a high-level click stimulus, often at a single stimulus level (such as 80
797 dBnHL) is employed to evoke a large action potential in the auditory nerve (ABR wave I).
798 The latency and amplitude of the ensuing ABR waves and the inter-peak latencies can
799 provide evidence of the function or dysfunction of the ascending neural pathway. A
800 wide variety of pathologies may influence the recorded nABR, including space-occupying
801 tumours (e.g. vestibular schwannoma), hydrocephalus, and diffuse or systemic disorders
802 that affect neural synchrony such as multiple sclerosis and ANSD. Analysis of the nABR
803 waveform can sometimes provide useful information about the approximate location or
804 severity of a disorder.
805
806 When using the threshold ABR to assess hearing peripheral hearing sensitivity we would
807 like to be able to assume that any abnormal response is the result of a raised hearing
30
808 threshold rather than any neurological abnormality. Conversely in the nABR we would
809 like to assume that any abnormal response is the result of a neurological rather than any
Page
810 audiological problem. In reality we can make no such assumptions and must be careful
811 to examine the case history for valuable clues and exploit other, independent, indicators
812 of audiological and neurological status. Knowledge of the ways in which a hearing loss
813 can influence the ABR is important when considering nABR test strategy and waveform
© BSA
2016814 interpretation, as is our willingness to perform separate threshold ABR and nABR tests
815 to aid diagnosis when necessary.
816
817 8.5.2 ABR generators and the normal ABR response
818
819 The ascending auditory pathway comprises fast and slow fibres so the mapping of ABR
820 peaks (or waves) to anatomical generators becomes increasingly confounded as we
821 progress up the pathway. That said, the main contributors of the following ABR waves
822 are generally thought to be:
823 Wave I: distal portion of the auditory nerve
824 Wave II: proximal portion of the auditory nerve
825 Wave III: cochlea nucleus
826 Wave IV: superior olivary complex
827 Wave V: lateral lemniscus
828 Wave VI: inferior colliculus
829 This is a very simplistic view and uses the popular peak labelling convention first
830 suggested by Jewett and Williston (1971). The generators of waves I to III are on the side
831 ipsilateral to the side of stimulation whereas 90% of ascending fibres beyond the
832 cochlea nucleus cross to the opposite side of the brainstem (Møller et al. 1995; Burkard
833 & Don 2012).
834
31
Page
© BSA
2016835
836
837 Figure 7 A normal adult nABR. Waves I, III & V have been labelled; waves II, IV & VI are
838 not always marked because they are less reliably identifiable than I, III & V.
839
840
841 8.5.3 Factors affecting the ABR
842
843 In the normal adult tested using high-level clicks we usually observe wave V at a latency
844 of typically 6 ms or a little less; we know from the threshold ABR that peak latencies
845 increase as the stimulus is reduced towards the audiological threshold or when lower
32
846 frequency stimuli are employed (a delay associated with the travelling wave within the
847 cochlea). For a description of the mechanisms see Burkard & Don (2012). Other factors
Page
848 affect latency, including age, gender, degree of hearing loss and audiometric slope
849 (Lightfoot, 1993). Some of these factors also influence the latency difference between
850 peaks (the inter-peak latency, IPL) though the effects of hearing loss and stimulus level
851 on IPLs are far less than for absolute latencies (Kirsh et al. 1992). For example, the
© BSA
2016852 female I-V IPL is typically a little less than 4 ms whereas that of males is a little over 4 ms
853 (the mechanisms of the gender difference are believed to be nerve length and core
854 temperature). The infant I-V ILP is typically 5.0 ms at birth (normal term) (Gorga et al.
855 1987), reducing as myelination of the auditory pathway occurs in the first few years of
856 life towards adult values.
857
858 The issues of patient age, physical size, and core temperature all disappear if we
859 consider the inter-aural latency difference (ILD) of either absolute latency
860 measurements (e.g. wave V latency) or IPLs (e.g. I-V). Here, the patient is acting as their
861 own control but there are two important considerations:
862 this approach is valid for unilateral pathologies but may be insensitive to bilateral or
863 systemic pathologies;
864 the effect of an asymmetric hearing loss (which may be unrelated to any neurological
865 pathology) must be considered since this will result in ear-specific increases in absolute
866 latency. For that reason, it is appropriate to apply a latency correction to cases of
867 asymmetric hearing loss if possible.
868
869 Many abnormalities affecting the auditory neural pathway will result in changes to the
870 nABR. Firstly, prolonged latencies (absolute and inter-peak) may be seen and secondly,
871 desynchronization in the firing of the individual nerve fibres can result in degraded
872 response morphology and reduced peak amplitudes; in extremis the ABR can be absent.
873 The above abnormalities may apply to the entire waveform or only for those peaks
874 generated medial to the site of a focal pathology. Whereas prolonged latencies can be
875 measured, degraded morphology is more difficult to quantify.
876
877 8.5.3.1 Test and stimulus parameters
878
879 Timebase (or window, recording epoch): Since high stimulus levels are used we expect
880 to record peak latencies less than 10 ms, even in pathological cases, so a timebase of 10-
881 12 ms is appropriate. This shorter timebase provides greater measurement resolution
882 for subsequent data analysis.
883
884 Stimulus repetition rate: A timebase of 12 ms would in theory allow a rate up to 83 /s to
885 be used. However, to record the IPLs we need to record all peaks and the amplitude of
33
886 wave I is known to diminish and the latencies of ABR peaks increase as the rate is
Page
887 increased above about 20 /s (Lightfoot, 1992). To preserve our ability to record wave I a
888 rate below 20 /s is therefore used. The rate must not be harmonically related to the
889 mains power frequency (50 Hz in Europe) and a rate of 11.1/s is commonly used.
890
© BSA
2016You can also read