Promoting the Participation of Children and Adolescents With Disabilities in Sports, Recreation, and Physical Activity
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
CLINICAL REPORT Guidance for the Clinician in Rendering Pediatric Care
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
Promoting the Participation of Children
and Adolescents With Disabilities in
Sports, Recreation, and Physical Activity
Paul S. Carbone, MD, FAAP,a Peter J. Smith, MD, MA, FAAP,b Charron Lewis, MD, FAAP,c Claire LeBlanc, MD, FAAP,d
COUNCIL ON CHILDREN WITH DISABILITIES, COUNCIL ON SPORTS MEDICINE AND FITNESS
The benefits of physical activity are likely universal for all children, abstract
including children and adolescents with disabilities (CWD). The
a
participation of CWD in physical activity, including adaptive or therapeutic Department of Pediatrics, The University of Utah, Salt Lake City, Utah;
b
Section on Developmental and Behavioral Pediatrics, The University of
sports and recreation, promotes inclusion, minimizes deconditioning, Chicago, Chicago, Illinois; cDivision of Developmental-Behavioral
optimizes physical functioning, improves mental health as well as academic Pediatrics and Psychology, Rainbow Babies and Children’s Hospital,
Cleveland, Ohio; and dDepartment of Pediatrics, McGill University,
achievement, and enhances overall well-being. Despite these benefits, CWD
Montreal, Quebec, Canada
face barriers to participation and have lower levels of fitness, reduced rates
of participation, and a higher prevalence of overweight and obesity All authors participated in conception, design, drafting, and critical
revision of the clinical report and approved the final manuscript as
compared with typically developing peers. Pediatricians and caregivers may submitted.
overestimate the risks or overlook the benefits of physical activity in CWD, This document is copyrighted and is property of the American
Academy of Pediatrics and its Board of Directors. All authors have
which further limits participation. Preparticipation evaluations often filed conflict of interest statements with the American Academy of
include assessment of health status, functional capacity, individual activity Pediatrics. Any conflicts have been resolved through a process
approved by the Board of Directors. The American Academy of
preferences, availability of appropriate programs, and safety precautions. Pediatrics has neither solicited nor accepted any commercial
Given the complexity, the preparticipation evaluation for CWD may not involvement in the development of the content of this publication.
occur in the context of a single office visit but rather over a period of time Clinical reports from the American Academy of Pediatrics benefit
from expertise and resources of liaisons and internal (AAP) and
with input from the child’s multidisciplinary team (physicians, coaches, external reviewers. However, clinical reports from the American
Academy of Pediatrics may not reflect the views of the liaisons or
physical education teachers, school nurses, adaptive recreation specialists, the organizations or government agencies that they represent.
physical and occupational therapists, and others). Some CWD may desire to The guidance in this report does not indicate an exclusive course
participate in organized sports to experience the challenge of competition, of treatment or serve as a standard of medical care. Variations,
taking into account individual circumstances, may be appropriate.
and others may prefer recreational activities for enjoyment. To reach the
All clinical reports from the American Academy of Pediatrics
goal of inclusion in appropriate physical activities for all children with automatically expire 5 years after publication unless reaffirmed,
disabilities, child, family, financial, and societal barriers to participation revised, or retired at or before that time.
need to be identified and addressed. Health care providers can facilitate DOI: https://doi.org/10.1542/peds.2021-054664
participation by encouraging physical activity among CWD and their
families during visits. Health care providers can create “physical activity To cite: Carbone PS, Smith PJ, Lewis C, et al.; AAP Council on
prescriptions” for CWD on the basis of the child’s preferred activities, Children With Disabilities, Council on Sports Medicine and
Fitness Promoting the Participation of Children and
functional status, need for adaptation of the activity and the recreational Adolescents With Disabilities in Sports, Recreation, and
opportunities available in the community. This clinical report discusses the Physical Activity. Pediatrics. 2021;148(6):e2021054664
PEDIATRICS Volume 148, number 6, December 2021:e2021054664 FROM THE AMERICAN ACADEMY OF PEDIATRICSimportance of participation in sports, recreation, and physical activity for
CWD and offers practical suggestions to health care providers.
GLOSSARY OF TERMS (including blindness), serious associated congenital heart
emotional disturbance, orthope- defect, difficulty swallowing,
Children and youth with special dic impairments, autism spec- cerebral palsy, and a urologic
health care needs (CYSHCN) are trum disorder, traumatic brain condition. This child would typi-
“children who have or are at injury, other health impairments, cally require the care of a pri-
increased risk for a chronic phys- or specific learning disabilities mary care physician; multiple
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
ical, developmental, behavioral or and who, by reason thereof, need pediatric medical subspecialists
emotional condition and who special education and related or pediatric surgical specialists,
also require health and related services.3 Although not part of home nurses, and rehabilitative
services of a type or amount the IDEA definition, the World and habilitative therapists; com-
Health Organization International munity-based services; extensive
beyond that required by children
pharmaceutical therapies; special
generally.”1 In the United States, Classification of Functioning, Dis-
ability and Health (ICF) frame- attention to his or her nutritional
19% of children have a special
needs and growth; and durable
health care need.2 CYSHCN are a work provides an important
medical equipment to maintain
diverse group of children, rang- alternative framework for dis-
health, maximize development,
ing from children with chronic ability because of its emphasis on
and promote function.
conditions, to those with medical body function, pursuit of mean-
Participation, defined by the ICF,
complexity, to children with cog- ingful activities, and community
is the nature and extent of a per-
nitive, behavioral, or emotional participation as primary determi-
son’s involvement in desired
conditions. The term CYSHCN nates of the health of individuals activities, such as recreation, lei-
includes children with disabilities rather than emphasis on any par- sure activities, and community
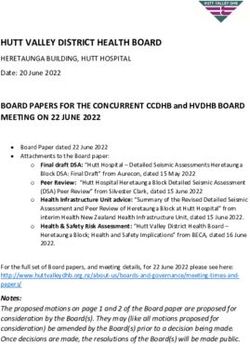
(CWD) and children with medical ticular diagnosis or deficit (Fig 2).4 life. The ICF also emphasizes the
complexity, whom are described Children with medical complexity interconnection of contextual fac-
below and shown in Fig 1. have multiple significant chronic tors, environmental and personal,
CWD are defined under the Indi- health problems resulting in that can have profound influen-
viduals with Disabilities Educa- functional limitations, high health ces on participation. For example,
tion Act (IDEA) as children with care service needs, and often the finding out what recreational
intellectual disabilities, hearing need for or use of medical tech- activities are enjoyable and fun
impairments (including deaf- nology.5 An example of a child for CWD (personal factors) and
ness), speech or language impair- with medical complexity is one supporting families (environmen-
ments, visual impairments with a genetic syndrome with an tal factors) can foster increased
community participation and bol-
ster overall health.6,7
Physical activity refers to any
body movement produced by
skeletal muscles that requires
energy expenditure.8
Exercise is planned, structured,
Cognive and behavioral
impairments
and repetitive physical activity
that aims to improve or maintain
one or more component of physi-
cal fitness.8 Exercise may be subdi-
vided into aerobic (cardiovascular
impairments
endurance), flexibility (increase
muscle and joint range of motion),
anaerobic (resistance training),
and high-impact weight-bearing
exercise (that promotes bone
FIGURE 1 Diverse subgroups within CYSHCN. CMC, children with medical complexity. health).8
2 FROM THE AMERICAN ACADEMY OF PEDIATRICSwith cognitive or behavioral
impairments. Furthermore, the
subgroups within CWD are also
overlapping and can shift over time,
such as the case in which a child
with primary motor impairments as
a young child might be more
impacted by cognitive or behavioral
impairments as an adolescent (Fig 1).
Regardless of the subgroup, CYSHCN
and all children with different
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
abilities are at risk for being “left
out,” which can adversely affect
FIGURE 2 The World Health Organization International Classification of Functioning, Disability and wellness, community integration, and
Health. Reprinted with permission from World Health Organization. Towards a Common
Language for Functioning, Disability and Health. Geneva, Switzerland: World Health Organi- full actualization of their
zation; 2002:9. individuality. Although it is hoped
that children with and without
disabilities engage in physical activity
PAVS, physical activity vital sign. provides CWD the opportunity to together, there will be times when
AAI, atlantoaxial instability. achieve better physical and mental CWD and their families opt for
health, develop skills and adaptive programs that are focused
INTRODUCTION competencies, express creativity, specifically on their needs. It must
International efforts to promote the form friendships, and improve also be noted that there is a
well-being of CWD through quality of life.20–23 Thus, the heterogeneity of adaptive recreation
participation in exercise, sports, American Academy of Pediatrics and sports programs, varying both by
Bright Futures: Guidelines for Health the type of primary impairment they
recreation, and physical activities
Supervision of Infants, Children, and are focused on and by the
began with the first competitive
Adolescents, Fourth Edition, includes competitive levels of the programs.
sporting event for individuals with
promotion of physical activity as a For example, Paralympians are high-
disabilities in 1948, followed by the
key health promotion theme and performance competitive athletes
first Paralympics competition in
includes recommendations for who generally self-identify as
1960. Special Olympics was
health care providers to help primarily having physical or visual
established in 1968 and is now the
CYSHCN and their families identify impairments, whereas Special
largest recreational program for
appropriate and enjoyable activities
children and adults with intellectual Olympians are often individuals with
and implement adaptations based
disabilities, with 5.5 million athletes intellectual and developmental
on need and ability.24
in 1930 countries.9 Despite the disabilities who compete in many
success of these programs, This clinical report discusses the different sports at various competitive
opportunities for CWD to participate importance of physical activity for levels.9,25 There are also sports
in physical activity, exercise, or CWD, reviews potential barriers to programs for people with hearing
competitive sports remain limited, inclusion, and offers practical impairments, with the most elite
and they are less likely to solutions for clinicians to facilitate being the Deaflympics.26 Although
participate compared with their participation. Of note, the terms adaptive recreation programs have
peers without disabilities.10–12 In CYSHCN, CWD, and children with existed for more than 50 years,
the absence of such opportunities medical complexity are overlapping recently there has been accelerated
and the encouragement to (Fig 1). This clinical report focuses growth in the number of programs,
participate, many CWD engage in on the needs of CWD, but many of especially those with a primary
more sedentary and solitary the comments and recommendations purpose of fostering physical activity
activities, leading to a higher apply also to the larger group of in a noncompetitive, fun environment.
prevalence of overweight and CYSHCN. However, not all points or Whatever the activity or the level of
obesity, lower levels of problems apply equally to the competition, health care providers
cardiorespiratory fitness, and diverse subgroups of CWD. For can engage in shared decision-making
increasing social isolation.13–19 example, some recommendations with CWD and their families with the
Taking part in physical activity may apply more to children with goal of pursuing appropriate
through recreation and sport physical impairments or children opportunities for physical activity.27
PEDIATRICS Volume 148, number 6, December 2021 3BENEFITS OF PARTICIPATION IN families identify appropriate and as well as with improving academic
PHYSICAL ACTIVITIES enjoyable physical activities and achievements.21 For example,
The benefits of physical activity are implement adaptations on the basis of participants in Special Olympics
likely universal for all children, their needs and abilities. show heightened self-esteem,
including those with disabilities. perceived physical competence, and
CWD are underrepresented in Physical activity also has benefits for peer acceptance when compared
exercise intervention research, children with primarily cognitive with nonparticipants.47 Physically
resulting in a limited understanding and behavioral disabilities. Children active individuals with cerebral
of how research involving children with autism spectrum disorder palsy experience higher quality of
without disabilities can be (hereafter referred to as autism), life and happiness compared with
who are more likely to be diagnosed those who are less active.20 Children
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
translated into guidance for physical
activity programs for CWD. The with overweight or obesity, have with autism who have higher levels
limited research conducted to date this risk attenuated with regular of participation in organized
physical activity and sports activities, including sports, have
points to at least short-term benefits
participation.36 Short periods of better social-emotional adjustment
for CWD, such as improvements in
walking or running before as well as reduced loneliness and
aerobic capacity, muscular strength,
educational sessions also help depression.48,49 Children with
physical and cognitive function, body
children with autism increase the muscular dystrophies who
weight and composition, social skills,
proportion of correct academic participate in physical activities,
relationships, and psychological well-
responses and work tasks
being.28–30 Although many studies of such as swimming, benefit by
completed in school settings.37,38 cultivation of friendships, increased
exercise interventions for children
Other exercise interventions for self-confidence, and enjoyment.50
with physical disabilities have small
children with autism, such as Children with hearing impairment
sample sizes and lack randomization,
horseback riding, martial arts, who participated in a 3-month ice
they support safe participation and
swimming, yoga, or dance, can result skating program were found by
improvements in fitness and well-
in better social responsiveness and their parents to have improvements
being.31 Several studies rated from
decreased irritability, stereotypical in self-esteem, behavior, and sleep
moderate- to high-quality show that
behavior, and hyperactivity.39–43 quality.51
children and youth with physical
Although stimulant medication is
disabilities who participate in physical
the mainstay in addressing core Despite the physical, behavioral,
activity programs improve their
symptoms for children with cognitive, and psychosocial benefits
locomotor performance and skills,
attention-deficit/hyperactivity of physical activity for CWD, the
object control, social skills, peer disorder, aerobic exercise offers a
interactions, and self-confidence.29 incorporation of physical activity is
safe and widely beneficial adjunct in often prioritized below other
One randomized trial of an 8-month decreasing hyperactivity and
weight-bearing physical activity interventions in treatment
improving attention and executive planning.49 Yet, as the above
program for children with cerebral function.44 Youth with intellectual
palsy showed improvements in bone examples illustrate, inclusion of
disability who are overweight or physical activity into treatment
mineral density.32 In some CWD, obese benefit from participating in
exercise interventions may even be plans allows CWD real-world and
an integrative training program, enjoyable opportunities to work on
able to slow disease progression. For with improved cardiorespiratory
example, in 2 randomized trials of motor, communication, and social
fitness, balance, muscle strength, skill goals identified in traditional
assisted bicycle and upper extremity and endurance as well as lower
training, functional motor therapies, such as physical, speech,
BMI.45 Adolescents and adults with and occupational therapy.
deterioration slowed in boys with Down syndrome who receive
Duchenne muscular dystrophy.33,34 individualized progressive resistance
Ambulatory children with spina bifida BARRIERS TO PARTICIPATION
training over 10 weeks have
can also increase their walking speed increased muscular strength and Despite the potential benefits, CWD
and cardiorespiratory fitness with become more physically active.46 participate in sports, recreation, and
treadmill training programs.35 Thus, physical activity less than children
Bright Futures: Guidelines for Health Beyond the physiologic benefits, without disabilities, and they
Supervision of Infants, Children, and regular physical activity, recreation, experience barriers to participation
Adolescents, Fourth Edition, includes and sports participation are that go beyond the functional
recommendations for health care associated with both psychosocial limitations associated with their
providers to help CYSHCN and their well-being and quality of life of CWD disabilities (Table 1).52–57 Without
4 FROM THE AMERICAN ACADEMY OF PEDIATRICSTABLE 1 Benefits, Barriers, and Considerations for Participation in Sports by CWD take general physical education
Benefits of participation classes, and although physical
Improved wellness education teachers may make
Increased community integration
accommodations for some, budget
Improved muscle strength
Improved fundamental movement skills constraints and lack of training are
Enhanced psychosocial well-being cited as barriers to participation.67,68
Increased cardiorespiratory fitness Pediatricians, other professionals, and
Decreased morbidity (ie, pressure ulcers, infections, overweight and obesity, etc) parents may also overestimate the risk
Improved bone health
of injury during physical activity,
Improved motor coordination
Improved attention and focus although involvement in sports has
been shown to be reasonably safe for
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
Decreased maladaptive behaviors
Barriers to participation CWD; one recent study found a lower
False belief: no programs for this population risk of injury in CWD after controlling
False belief: participation is unsafe or too risky
False belief: rules of sports too hard to learn or cannot be adapted to accommodate CWD
for personal and environmental
Low physical literacy factors.60,69–71 Nevertheless, parents of
Lack of transportation to and from activities CWD are justified in desiring high-
Lack of needed supervision or expertise quality, accessible, and safe adaptive
Extra cost and time commitment recreation programs, yet they report
Facilitators to participation
Preparticipation evaluations to maximize safety with appropriate accommodations
marked variation in recreational
Organized sports that are focused on fun over competition activity availability, long waiting lists
Clinicians, physical education teachers, and coaches who create physical activity prescriptions for adaptive programs, absence of
and recognize individual needs suitable transport to these facilities, a
Adaptations such as longer rest periods, lower coach to athlete ratios, copious positive
reduced number of skilled instructors
feedback, and close monitoring for symptoms of fatigue or injury
to run these programs, and poor
Reproduced with permission from: American Academy of Pediatrics. Athletes with a disability. In: Bernhardt DT, Rob-
erts WO, eds. PPE: Preparticipation Physical Evaluation. 5th ed. Itasca, IL: American Academy of Pediatrics; 2019:185 advertisement of programs in the
community.60,61 Likewise, pediatricians
may be unaware of adaptive
addressing barriers to physical activity, by their peers64,65; this is especially recreation opportunities within the
CWD often fill leisure time with true for CWD with obesity, who may community or of the family’s interest
sedentary screen-based activities.18,58 experience additional weight-bias in pursuing these opportunities.72
Frequently identified barriers to stigmatization. Primary care providers
participation of CWD in sports and who have longitudinal and trusting Overall, misconceptions and
physical activity are the child’s relationships with CWD and their attitudinal barriers at the level of
functional limitations, negative self- families can be positive role models the individual, family, and
perceptions, high cost, lack of and use nonjudgmental language and community need to be addressed to
accessible facilities, lack of nearby motivational interviewing to identify integrate children of all abilities into
facilities or programs, and lack of short-term goals and strategies related recreational and physical activities.
providers with adaptive recreation to eating and physical activity.66 With Pediatricians can help families and
expertise.10,59–62 In addition, many negative experiences and lack of children balance the benefits of
individuals with disabilities are still, to opportunities, support, or participation with the potential
a large extent, socially segregated and encouragement, some CWD may risks, recognizing that historically,
experience negative societal become disinterested or discouraged being “too safe” and assuming that
stereotypes and low performance to participate. Older children and CWD “can’t do that,” has been a
expectations, providing them with adolescents with disabilities may lose persistent barrier to participation.
limited opportunities for participation self-confidence to participate as skill
in group-based physical gaps between them and their typically FACILITATORS TO PARTICIPATION
activities.57,60,63 Some CWD may be developing peers widen and sports The combined efforts of well-
discouraged to participate by an become more competitive. Through informed health care providers,
implicit societal bias that favors required physical education services of parents, educators, coaches, and
competitiveness and winning over a child’s Individualized Education others are needed to ensure and
participation for the sake of fun, Program (IEP), schools can develop promote the participation of all
enjoyment, and inclusion. When CWD goals to address deficits in children in sports, recreation, and
do attempt to participate in sports, fundamental movement skills to foster physical activity (Table 1). Health
they are also more likely to be bullied physical literacy. However, most CWD care providers can facilitate
PEDIATRICS Volume 148, number 6, December 2021 5participation by asking about occupational therapists that create a Parents, caregivers, and peers are
current levels of activity and using safe and fun recreational important facilitators of physical
tools, such as a physical activity vital environment while allowing activity for CWD. Parents who
sign (PAVS) in the electronic health coordination with the primary care believe in the benefits of physical
record, to start the conversation provider if medical concerns activity report higher levels of
about physical activity during occur.76 Specifically, health care activity in their CWD.70 In one
visits.23 The PAVS consists of 2 providers and care coordinators study, CWD whose parents were
screening questions that are used to within practices can partner with physically active at least 3 hours per
assess how many days per week the local adaptive recreational programs week were 4.2 times as likely to be
individual engages in physical that address traditional barriers to physically active compared with
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
activity that is moderate (causes the participation (time, cost, those whose parents were less
child or youth to sweat a little and transportation) and share this active.80 Therefore, an important
breathe harder, such as bike riding information with families. For message from pediatric health care
or playground activities) to vigorous example, many city and county providers to parents of CWD is to
(causes the child or youth to sweat parks and recreation departments prioritize their own physical activity
and be out of breath, such as offer low-cost adaptive recreation and to include CWD in family
running or swimming) and how opportunities for CWD, and some recreational activities.81 Additionally,
many minutes this level of physical adaptive recreational programs offer CWD are too often left behind
activity is maintained. Use of the scholarships and provide regarding organized sports
PAVS has been associated with a transportation to and from participation despite the clear benefit
greater likelihood of physician of participation for CWD. Parents can
activities. Therapists and coaches at
exercise counseling and improved advocate for and support organized
specialized adaptive recreation
metabolic outcomes in adults.73 sports that encourage inclusion and
programs facilitate participation for
Clinicians can then create “physical focus on fun instead of winning, such
CWD by having lower participant to
activity prescriptions” for CWD with as Special Olympics, because these
coach or instructor ratios (fewer
goals for participation and referrals are important influencers of sustained
than 4 participants for each coach),
to specific programs or resources participation by CWD.65 In addition,
using positive feedback, and
that are based on baseline physical peer-mediated interventions to
individualizing activities to the
activity, preferred activities, facilitate play skills and foster
preferences of each participant.77
functional limitations that may inclusion and acceptance of CWD by
require adaptation of the activity modeling behaviors can be an
Lastly, providers can work with
and preparticipatory planning, and effective counterbalance to the barrier
local and state public health
the evidence base of the physical of systematic exclusion that has (in
agencies to promote physical
activity regarding risks and the past) resulted in opportunities for
activity to create and strengthen
benefits.23 Providers can explore the bullying behaviors.82,83
recreational programs for CWD. The
child and family’s beliefs and
Title V Maternal and Child Health The American Heart Association has
attitudes about physical activity
Services Block Grant Program has a called for schools to play a central
through motivational interviewing
National Performance Measure on role in ensuring all students
and arrive at a treatment plan
physical activity, with only 25% of participate in enough physical
through shared decision-making
CYSHCN with more complex health
(Appendix 1).27,74 Lastly, by their activity to develop healthy
needs meeting the measure of being lifestyles.84 With only 24% of CWD
own commitment to physical
activity, health care providers can physically active at least 60 minutes engaging in 60 minutes of physical
serve as role models for CWD and per day.78 At the federal level, the activity daily, schools can help a
their families. For example, Centers for Disease Control and greater proportion reach this level
pediatricians with self-reported Prevention funds and supports 2 of activity.85 The Centers for Disease
higher levels of fitness are more national centers on disability: Control and Prevention recommends
likely to discuss physical activity Special Olympics and the National that a substantial percentage of
during health supervision visits.75 Center on Health, Physical Activity students’ overall physical activity
and Disability. These centers should be obtained through school
To facilitate participation, providers identify and expand physical activity physical education. The right of
can refer CWD to specialized programs, provide training for CWD to participate in physical
adaptive programs staffed by professionals, and provide data to activity and sports in school is
recreational, physical, or establish best practices.79 rooted in several federal laws. The
6 FROM THE AMERICAN ACADEMY OF PEDIATRICSIDEA mandates free, appropriate activity.91 School-based physical linked to improvement in
public education in the least activity programs, such as recess or cardiovascular fitness scores and
restrictive environment, and Section physical education, that are focused on BMI.93 Thus, CWD who have
504 of the Rehabilitation Act of fun and enjoyment are strongly decreased gross motor function or
1973 requires that no individual associated with daily physical activity other developmental delays may
shall be excluded because of in CWD.88 lack fundamental movement skills,
disability in programs that receive may have low physical literacy, and
federal funds.86 Physical education PREPARTICIPATION CONSIDERATIONS are subsequently at risk for
is a federally mandated component It is important that all CWD developing a low preference for
of special education services, participate in activity-related physical activity during childhood
including the promotion of physical and later in life.23,94 Physical
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
recreational programs while
fitness, fundamental movement skills, minimizing risks of illness or injury. literacy assessments by health care
and skills in individual and group Well-designed programs can target providers are essential to allow
games and sports.67 However, many fundamental movement skills early identification of any deficits.95
school districts allow exemption from (throwing, catching, kicking, jumping, Physical literacy assessments for all
physical education requirements for running, hopping, balance), flexibility, children begin in early childhood
students with cognitive and other cardiorespiratory endurance, and and encompass surveillance and
disabilities.87 Physical education muscular strength while maximizing screening for motor delay and
curricula for CWD can promote enjoyment and safety. Rather than exploring the child and family’s
enjoyment of movement and skill being excluded from sports knowledge, motivation, and feelings
development that can be incorporated participation, all children can be related to physical activity and
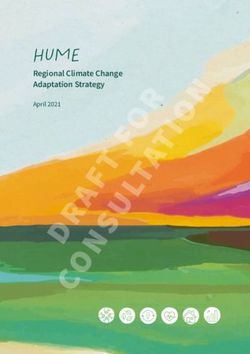
before, during, and after school empowered to take part with a can-do movement.23,96,97 Figure 3 provides
hours.88 Pediatric providers and attitude, enjoying the dignity of taking an adaptation of the ICF framework
parents can partner with the acceptable risk during participation for pediatricians to use in assessing
educational team to include physical just as individuals without disabilities physical literacy and promoting
activity goals in progress metrics are allowed to do. It is also important physical activity in CWD.7 For CWD
within a child’s IEP to facilitate to involve parents and caregivers early who have motor delays, referrals to
participation in physical activity at and often in discussions of the exercise-related specialists (physical
school.86 Physical activity can be importance of participation in sports, therapist, physical medicine and
accurately measured for CWD through recreation, and physical activity for rehabilitation physician, recreation
subjective and objective measures.89 CWD. therapist, sports medicine physician)
Adaptive physical education teachers for structured programming may
can address physical activity goals by A first step toward regular physical help to maximize the child’s
modifying recreational programs to activity of all children, including potential in developing fundamental
accommodate the motor skills, muscle CWD, is achieving physical literacy, movement skills, which in turn may
strength, and fitness of each child. which is the “the ability, confidence, foster confidence and desire to
Strategies physical education teachers and desire to be physically active for participate in sports and
use to accommodate CWD may life.”92 For children with typical recreation.98,99 Furthermore, young
include simplified instruction, development, fundamental CWD can be given the same
additional skill modeling, peer movement skills emerge in early opportunities as other children to
teaching, equipment modification, and childhood after the attainment of participate in free play and recess to
coordinating activities with a special gross and fine motor milestones in develop fundamental movement
education teacher.68 Beyond physical infancy. Later in childhood, provided skills and to foster the notion that
education, the Comprehensive School the child has opportunities to physical activity is fun.100,101 One
Physical Activity Program developed engage regularly in active play and such program to include students
by the Centers for Disease Control and physical activity throughout the day, with autism with typically
Prevention and the Society of Health additional competences are gained developing peers during recess
and Physical Educators, is a in coordination, balance, running, activities led to improvements in
framework to capture all opportunities kicking, throwing, and catching.23 peer engagement.102
for school-based physical activity for The attainment of these
CWD.90 School nurses can coordinate fundamental movement skills How Much Physical Activity to
with pediatricians in developing and influences physical literacy, is a Recommend?
implementing health care plans that strong predictor of future physical All children, including CWD, are
promote safe participation in physical activity levels of children, and is encouraged to strive to follow
PEDIATRICS Volume 148, number 6, December 2021 7Health condition
625 Fitness Function Friendships
• 626 • family and child's •
627
•
628
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
•
629
630
631
632
Family factors Fun
• •
• decision-making •
•
FIGURE 3 Adaptation of the International Classification of Function as a framework of assessing physical literacy and promoting participation of CWD in
sports, recreation, and physical activity.7 Adapted from World Health Organization. Towards a Common Language for Functioning, Disability and
Health. Geneva, Switzerland: World Health Organization; 2002:9.
guidelines established by the 2018 encouraging children and families to The concepts of self-determination
Physical Activity Guidelines do whatever they can through a and shared decision-making have
Advisory Committee, which gradual exploration of increases in emerged as important themes in the
recommends that children and time, intensity, and duration.104 By care of CWD.27 Discussions with
adolescents (6–17 years) take part asking CWD and their families about children and families may start with
in at least 60 minutes of moderate usual weekly duration and intensity a query about the child’s current
to vigorous physical activity daily as of physical activity, health care level of physical activity and the
well as in bone and muscle providers can adapt physical activity importance the family and child
strengthening activities at least 3 guidelines to accommodate for place on being physically active.
days a week.103 Parents of infants neuromuscular deficits and Families of CWD may experience
are encouraged to keep them active cardiorespiratory profiles associated high levels of day-to-day stress and
several times a day through with specific conditions. may consider time for physical
interactive floor-based play, and activity a lower priority. Using
parents of preschool-aged children The Preparticipation Evaluation: behavioral techniques, such as
(3–5 years) are encouraged to have Special Concerns for CWD motivational interviewing, providers
their children accumulate at least 3 Families of CWD will sometimes can explore the family’s beliefs and
hours of light- to moderate-intensity schedule mandatory develop achievable physical activity
activity throughout the day to preparticipation physical evaluations goals. Once the wishes of the child
develop movement skills.23,104–106 or recommended health supervision and family are known, conditions
For CWD, some modifications may visits. In either case, these visits that may interfere with participation
be required to the frequency, allow opportunities for families and or predispose the child to injury can
intensity, and/or duration of providers to discuss medical and be collaboratively discussed
physical activity. Goals need to be psychosocial issues that are relevant between the child, family, provider,
realistic, with an emphasis on for participation in physical activity. and other treatment team members.
8 FROM THE AMERICAN ACADEMY OF PEDIATRICSThe child’s current health status and the sport or the child’s participation to headache, high blood pressure, or
functional ability, demands of the prevent injury to the athlete or other bradycardia, and these symptoms
sport (including level of participants.107 Children with prompt immediate removal of the
competition), and whether the sport neurologic conditions who use precipitating factor and prompt
can be modified with protective or wheelchairs for ambulation are at medical care.107 Children with spinal
adaptive equipment to allow for higher risk of upper extremity overuse cord injuries and cerebral palsy are
safer participation are important injuries, peripheral nerve entrapment also at risk for abnormal
considerations. Given the (eg, carpal tunnel syndrome), and thermoregulation and exertional
complexity, the preparticipation pressure sores affecting the sacrum heat illness resulting from impaired
evaluation for CWD may not occur and ischial tuberosities.108 The sweating and control of peripheral
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
in the context of a single office visit preparticipation evaluation presents blood flow as well the use of certain
but rather over a period of time an opportunity to screen for skin medications (such as those with
with the assistance of care ulcerations and, when present, initiate anticholinergic properties).107,111 As
coordination from the primary care appropriate treatment before sports is the current practice for most
medical home to obtain input from participation.109,,110 Inspecting the adaptive and therapeutic sports
the child’s multidisciplinary team, adaptive or medical equipment used organizations, coaches can modify
which may include subspecialists by CWD participating in sport so that the activity as needed, provide
such as physical medicine and braces are appropriately fitted and frequent breaks of appropriate
rehabilitation or sports medicine sports wheelchairs are in proper duration, have ready access to
physicians; school nurses, coaches, working order promotes optimum fluids, and use appropriate clothing
and physical education teachers; and performance and injury prevention. and equipment, which can mitigate
recreation, physical, and Families can be encouraged to bring this risk.107,111,112
occupational therapists. Ideally, all equipment used during physical
members of the multidisciplinary activity to the preparticipation visit so Children with developmental
team can periodically reassess CWD that these assessments can be disabilities also benefit from
to update treatment plans, including conducted. If needed, referrals to preparticipation planning and
recommendations about sport exercise-related subspecialists anticipatory guidance. For example,
participation, adaptations, and any (physical therapist, physical medicine children with autism may have
restrictions deemed necessary. and rehabilitation physician, apraxia and motor coordination
recreation therapist, sports medicine deficits, increasing the risk for
The goal of the preparticipation physician) can be made for injuries.113 This risk can be
evaluation is to review the desired equipment adjustments or other managed by adaptations to the
activities of the child and family and equipment concerns. activity or the equipment or with
the current state of disability-specific additional neuromotor training to
and co-occurring conditions to provide The preparticipation evaluation also develop kinesthetic awareness.114
an appropriate menu of activities and allows for the provision of Children with intellectual disability
potential accommodations or anticipatory guidance that promotes may have lower muscle strength,
precautions that may be needed. safe participation for children with balance, flexibility, and endurance
Tables 2 and 3 show elements of a physical disabilities. For example, and may benefit from exercise that
preparticipation history and physical athletes with spinal cord pathology is of lower intensity as well as
examination that can be used for above the sixth thoracic level may preparatory conditioning, such as
CWD. For example, children with develop autonomic dysreflexia, resistance training, to reduce the
physical disabilities, such as cerebral which is excessive and uncontrolled risk of injury.108 Children with
palsy, may have decreased flexibility sympathetic nervous system output. Down syndrome are at slight
with joint contractures, muscle This condition, which can be life- increased risk of symptomatic
strength imbalances, and lack of motor threatening, may be triggered by atlantoaxial instability (AAI).
control, coordination, and equilibrium, bladder infections, sunburns, and Neurologic manifestations of AAI
which may increase the risk of lower other stimuli or may be self-induced with cervical cord myelopathy
extremity overuse injuries, strains, and by an act such as occluding a include significant neck pain,
sprains. If a child with cerebral palsy bladder catheter in an attempt to radicular pain, weakness, spasticity
wishes to play baseball and there are improve sport performance (also or change in tone, gait difficulties,
limitations in skills (catching, known as “boosting”). Autonomic hyperreflexia, and change in bowel
throwing, and using a bat), it may be dysreflexia may present with or bladder function or other signs
advisable to consider ways to adapt symptoms and signs such as or symptoms of myelopathy. In the
PEDIATRICS Volume 148, number 6, December 2021 9TABLE 2 Elements of a History During Preparticipation Evaluation for CWD
History Comments
Is there a history of seizures? Children with uncontrolled seizures or implantable devises (eg,
ventriculoperitoneal shunt, vagal nerve stimulator) may benefit from
consultation with a neurologist or neurosurgeon, respectively, to assist
with medical eligibility. Although there is no universal exclusion for
participation in contact sports for children with epilepsy, some
families may choose to avoid sports in which seizure activity would
pose risk to self or others (eg, archery, riflery, weightlifting, and
sports that involve heights). There are considerations related to
prevention of drowning in children with epilepsy who swim.118 In
addition, some antiepilepsy drugs can impair normal sweating.
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
Is there a history or concern for hearing or vision loss? Boxing and full-contact martial arts are not recommended for functionally
one-eyed athletes.119 Visually asymptomatic CWD are encouraged to
have a vision screening based on the Bright Futures periodicity table.
Those with ocular signs or symptoms are recommended to have a
complete examination by a pediatric ophthalmologist.120
Is there a history or concern for cardiopulmonary disease? Children with stage 2 hypertension are recommended to refrain from
high-static sports (weightlifting, gymnastics). Children with congenital
heart disease, structural heart disease, and dysrhythmias are
encouraged to have consultation with a cardiologist.119
Is there history of symptomatic AAI? Children with symptomatic AAI may report or demonstrate fatigue, gait
abnormalities, neck pain, limited neck range of motion, changes in
coordination, spasticity, hyperreflexia, clonus, or extensor-plantar
reflex. Parents can be advised that participation in contact sports,
such as football, soccer, and gymnastics, places children at risk for
spinal cord injury.115
Is there a history of heat stroke or heat exhaustion? Thermoregulation in children with spinal cord injuries can be impaired
because of skeletal muscle paralysis (impaired shivering and reduced
ability to produce heat) and a loss of autonomic nervous system
control (impaired sweating and vasodilation to dissipate heat). Athletes
who have a history of heat illness are more at risk to develop the
condition again.
Is there a history of fractures or dislocations? Ligamentous laxity and joint hypermobility are more common in some
disabilities, such as Down syndrome and Ehlers-Danlos syndrome.
Children with obesity, those with osteogenesis imperfecta, and athletes
in wheelchairs may have reduced bone mineral density with increased
fracture risk.
Are there adaptive devices used during sports participation? Health care providers are encouraged to be aware of the child’s need for
adaptive equipment. Athletes using wheelchairs are at increased risk
for shoulder and wrist injuries and upper extremity peripheral nerve
entrapment syndrome.
Is there a need for bladder catheterization? Athletes with spinal cord injuries or other neurologic conditions may have
neurogenic bladder and need an indwelling catheter or require
intermittent catheterization.
Is there a history of pressure sores or ulcers? Children who use wheelchairs are prone to pressure ulcers over the
sacrum and ischial tuberosities.
What medications is the child taking? Medications used for pain and bladder dysfunction can interfere with the
normal sweating response; medications that alter QT intervals also
may require special assessments.
Is there a history of autonomic dysreflexia? Autonomic dysreflexia is acute onset of excessive, unregulated
sympathetic output that can occur in children with spinal cord injuries
at or above the sixth thoracic spinal cord level. This condition may
occur spontaneously or may be self-induced (boosting) in an attempt
to improve performance.121
Adapted from American Academy of Pediatrics. Athletes with a disability. In: Bernhardt DT, Roberts WO, eds. PPE: Preparticipation Physical Evaluation. 5th ed. Itasca, IL: American
Academy of Pediatrics; 2019:182–183.
absence of myelopathic signs and Children and youth with Down may place them at increased risk of
symptoms during the syndrome can be encouraged to spinal cord injury.115
preparticipation evaluation, routine participate in activities they enjoy,
radiographic evaluation of the although contact sports, such as As the above examples illustrate, for
cervical spine is not recommended. football, soccer, and gymnastics, each child and youth with a
10 FROM THE AMERICAN ACADEMY OF PEDIATRICSTABLE 3 Elements of a Physical Examination During Preparticipation Evaluation for CWD a. Adding a PAVS to visits can
Physical Examination help start conversations about
Components Items to Screen physical activity with CWD
Ocular Decreased visual acuity and their families.
Ocular health
Strabismus Communicate the physical,
Abnormalities in ocular appearance beha-vioral, cognitive, and social-
Cardiovascular Cardiovascular heart disease
emotional benefits of participation
Hypertension
Neurologic Peripheral neuropathies in sports, recreation, and physical
Inadequate motor control activity to CWD and their caregivers
Inadequate coordination and balance (Table 1).
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
Clonus a. Promotion of physical activity is
Impaired hand-eye coordination
Sensory dysfunction
a Bright Futures key health
AAI promotion theme to be aware
Hyperreflexia of in each stage of child
Ataxia development.24
Muscle weakness
Health care providers can make a
Spasticity
Upper motor neuron and posterior column signs and symptoms difference when they agree to “take
Dermatologic Abrasions the pledge” to talk to their patients
Lacerations about physical activity (https://www.
Blisters nchpad.org/pledge/doctalk).
Pressure ulcers
Rashes
Encourage parents to be physically
Musculoskeletal Limited neck range of motion active and encourage inclusion of
AAI CWD in family recreational activities.
Torticollis Recognize, identify, and address
Decreased flexibility, often with contractures; decreased strength; barriers to participation at the
and muscle strength imbalance
Wrist and elbow extensor tendinitis in athletes using wheelchairs individual, family, community, and
Rotator cuff tendinitis and impingement in athletes using societal levels to increase the
wheelchairs opportunities for CWD to be
Pelvic dysfunction caused by lower extremity prosthetic device physically active (Table 1).
causing unequal leg lengths
a. Refer CWD to local adaptive
Reproduced with permission from: American Academy of Pediatrics. Athletes with a disability. In: Bernhardt DT, Rob-
erts WO, eds. PPE: Preparticipation Physical Evaluation. 5th ed. Itasca, IL: American Academy of Pediatrics; 2019:185 and therapeutic recreation
programs that decrease the
barriers to participation. If
disability, pediatricians can review titled “Athletes with Disability.” A there is limited access to local
condition-specific information, supplemental history form for programs, home-based
current medications, and other athletes with a disability and a programs with adapted
individualized aspects of the history Special Olympics medical form are exercises and movements can
to offer recommendations that available for download at https:// be recommended. Free-to-
promote safe participation. Concerns www.aap.org/en-us/advocacy-and- access videos are available
or questions that arise during the through the National Center
policy/aap-health-initiatives/Pages/
preparticipation visit can be on Health, Physical Activity
PPE.aspx or in Supplemental Fig 4.116
addressed through consultation with and Disability (https://www.
a sports medicine or physical nchpad.org/Videos).
RECOMMENDATIONS Pediatricians can partner with
medicine and rehabilitation
physician, who can provide Pediatricians can promote participation families, schools, and community
additional guidance. Although a of children and adolescents with organizations in advocating for safe,
comprehensive review of disabilities in sports, recreation, and affordable, accessible, and inclusive
preparticipation considerations is physical activity in the following ways: recreational programs for CWD to
beyond the scope of this report, reduce disparities in participation in
health care providers are encouraged 1. Assess motor development, physical activity;
to refer to the publication PPE: physical literacy, and physical Encourage participation by
Preparticipation Physical Evaluation, activity levels at all health discu-ssing physical activity goals
Fifth Edition, which has a chapter supervision visits with CWD. with CWD and their families and
PEDIATRICS Volume 148, number 6, December 2021 11partnering with interdisciplinary keep athletes safe and healthy while and benefits, particularly among
team members to develop physical participating in sports and includes individuals with higher levels of
activity prescriptions that can be condition-specific preparticipation disability, clinicians should not
incorporated within an after-visit considerations for athletes with hesitate to promote physical activity
summary within the electronic disabilities. for CWD. Well-informed decisions
medical record. If a handwritten The use of a preparticipation form regarding each child’s participation
paper note is preferred, a free can promote the documentation of are made through consideration of
physical activity prescription pad is relevant medical issues that can be individual activity preferences,
available through the Americans with shared with therapeutic recreation overall health status, motor skills,
Disabilities Fund at http:// programs, schools, and coaches balance, muscle strength, bone
foundationforpmr.org/old/physicians/ (Supplemental Fig 4; https://www.aap. strength, fitness level, and the
Downloaded from http://publications.aap.org/pediatrics/article-pdf/148/6/e2021054664/1210931/peds_2021054664.pdf by guest on 11 February 2022
diagnostic- org/en-us/advocacy-and-policy/ availability of adaptive programs.
population/rx-for-exercise- aap-health-initiatives/Pages/PPE.aspx). Child, family, and societal barriers to
pediatrics-new/. Partner with children, parents, and participation continue to exist and
a. Participation in recreation, educational teams to include physical need to be directly identified and
sports, and physical activity activity goals and modifications in a addressed through advocacy at the
has inherent risk for all. student’s IEP and advocate for school- local, state, and federal levels.
Rather than exclusion from based physical activity programs for Pediatric health care providers are
sports participation, CWD. urged to promote healthy, active
pediatricians can encourage Be aware of and actively refer to living for CWD through physical
CWD to adopt a can-do local school and community-based activity, exercise, recreation, and
attitude, enjoying the dignity organizations that offer appropriate organized sport by creating specific
of taking acceptable risk physical activity programs and physical activity prescriptions suited
during participation just as sports for CWD. to the child’s interests and ability. The
individuals without disabilities a. Local and state disability benefits are substantial not only for
are allowed to do. organizations, such as family- the children who participate but also
While striving to meet to-family health information for communities that welcome them.
the 2018 Physical Activity Guidelines centers and Family Voices,
Advisory Committee may have up-to-date lists of RESOURCES FOR HEALTH CARE
recommendations for physical adaptive recreation programs PROVIDERS AND FAMILIES
activity, some CWD will require (https://familyvoices.org/).
Web sites of national organi-
modifications to the frequency, National centers on health pro-
intensity, and/or duration of physical zations, such as Special Olympics,
motion for people with disabil-
activity. Realistic goals can be based the National Center on Health,
ities: National Center on Health,
on gradual increases in baseline Physical Activity and Disability, and
Physical Activity and Disability
duration and intensity of physical Move United, can provide
(http://www.nchpad.org) and
activity. information on local activities (see
Special Olympics (https://www.
Perform preparticipation Resources for Health Care Providers
specialolympics.org);
and Families).
evaluations for CWD, in collaboration Paralympics (https://www.
with the child, family, pediatric Advocate at the local, state, and
paralympic.org);
national levels for policies that that
specialists, and therapists, leading to US Association of Blind Athletes
opportunities to participate in sports promote inclusion of CWD in sports,
(usaba.org);
recreation, and physical activity and
and recreational activities with Miracle League (http://www.
appropriate adaptation to minimize for surveillance systems that include
themiracleleague.net);
CWD to track participation and
risk of injury Move United (https://www.
(Tables 2 and 3). access.117
moveunited.org);
a. Encourage families to bring Achilles International
ada-ptive equipment used SUMMARY AND CONCLUSIONS (achillesinternational.org);
during physical activity to visits Participation in free play, sports, National Wheelchair Basketball
to assess need for adjustments recreational programs, and physical Association (nwba.org);
or referrals. activity improves health, well-being, Easter Seals (http://www.
PPE: Preparticipation Physical and quality of life for CWD and their easterseals.com/our-programs/
Evaluation, Fifth Edition, serves as a families. Although more research is camping-recreation/
resource for medical providers to needed to confirm specific outcomes recreation-and-sports.html);
12 FROM THE AMERICAN ACADEMY OF PEDIATRICSYou can also read