Preparing the healthcare workforce to deliver the digital future - The Topol Review - Health Education England
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Health Education England The Topol Review Preparing the healthcare workforce to deliver the digital future Interim Report June 2018 - A Call For Evidence Developing people for health and healthcare www.hee.nhs.uk


Contents
1.0 Preamble...........................................................................................................................................4
2.0 Approach..........................................................................................................................................6
3.0 Workforce profile ........................................................................................................................8
4.0 Educating the healthcare workforce ..............................................................................12
5.0 Ethics ................................................................................................................................................16
6.0 Health economics ......................................................................................................................17
7.0 Themes ............................................................................................................................................18
8.0 Theme 1: Genomics ..................................................................................................................19
9.0 Theme 2: Digital medicine ....................................................................................................24
10.0 Theme 3: AI and Robotics .....................................................................................................28
11.0 Open call for evidence ............................................................................................................33
3
1.0 Preamble
In 2018 the NHS celebrates its 70th Additionally, the Review Board is clear that the future of
medicine must primarily focus on the patient – and on
anniversary. While it is hard to predict the a larger scale, the public. We must consider both what
future, we know that genomics, digital patients will require from healthcare professionals as new
medicine, artificial intelligence and robotics technological advances are deployed in the NHS, and how
public and patient education can best be delivered, while
will have an enormous impact on patients and
respecting patient choice and acknowledging the diversity
the workforce over the next two decades. of the population.
Digital technologies are transforming our ability to Peel away the walls of the hospital and the doors of the
empower patients to participate actively in their own GP surgery and you are left with the essence of the NHS: a
care, with a greater focus on well-being, to prevent human interaction between the patient and clinician. On a
diseases such as cancer and hypertension, to predict typical day, the NHS workforce interacts with over a million
the most appropriate treatments and to personalise the people. Each one of these interactions impacts on the life
management of long-term conditions (also known as of an individual, their family, and often those providing
chronic diseases), such as diabetes and asthma. informal care. Each contact reflects the professionalism,
skills, compassion and empathy of the healthcare team.
The Secretary of State for Health and Social Care, Mr
Jeremy Hunt, has said1: “Every week we hear about With over 1.2 million staff in England, the NHS is the
exciting new developments surfacing in the NHS, which largest employer in Europe and one of the five largest
could help provide answers to some of our greatest employers in the world. This workforce performs over
challenges such as cancer or long-term conditions. 300 different types of jobs for more than 1,000 separate
These give us a glimpse of what the future of the whole employers in the public, private and voluntary sectors.
NHS could be, which is why in the year of the NHS’s
70th birthday I want to empower staff to offer patients In a fast changing healthcare environment, with a growing
modern healthcare more widely and more quickly.” and ageing population, the task of ensuring that the
workforce has the skills, knowledge and time to care is
Accordingly, the Secretary of State has commissioned this essential to future proofing the NHS and its ability to meet
independent Technology Review as a key strand of the patients’ needs. There is little point investing in the latest
workforce development strategy, ensuring that the NHS technology if there is not a workforce with the right roles
is at the forefront of life-saving or life-changing care for and skills to make full use of its potential to benefit patients.
decades to come.
This Review is building on existing strands of work in the
Addressing questions that are integral to the future of the NHS. The 100,000 Genomes Project, currently the largest
NHS, this Review has been asked to consider: national sequencing project in the world, was launched
• How are technological (genomics, digital medicine, by NHS England and Genomics England in 2014. The
artificial intelligence (AI) and robotics) and other Chief Medical Officer Dame Sally Davies’s 2016 annual
developments likely to change the roles and functions report ‘Generation Genome’ recognised there has been
of clinical staff and their support in all professions over a “massive change in our ability to diagnose, treat and
the next two decades? support patients with genetic diseases” and “that the UK
has become the international leader in the field”.
• What are the implications of these changes for the
skills required? For which professions or sub-specialisms There have been a number of relevant reports recently
are these likely to be particularly significant? published on the application of digital technologies
• What does this mean for the selection, curricula, to healthcare. The 2016 Wachter Review, ‘Making IT
education, training, development and lifelong learning Work’, assessed the state of NHS IT services and made
of current and future NHS staff? recommendations for what was needed to facilitate a
4
This Interim
Report is the
beginning of the
digital healthcare future. It recommended that all Trusts
should aim to achieve a high level of digital maturity conversation.
within five years. It also recommended establishing a
national programme to train Chief Clinical Information
Officers (CCIOs).
Building on these foundations, this Review is proposing This Review marks a historic opportunity for the NHS
three key principles, which should govern the NHS’s to learn from research, innovation and best practice in
future workforce strategy: digital technologies for healthcare, while considering
• Patients: If willing and able to do so, will be the implications for the education and training of its
empowered by new tools to become more actively workforce. It is essential that all healthcare professionals
involved and engaged in their care. The patient- are ready for the digital future, a future which puts care
generated data will be interpreted by algorithms at the forefront of healthcare.
enabling personalised self-management and self-care.
This Interim Report is the beginning of the conversation.
• Evidence: The introduction of any technology must Evidence and comments are being sought from any
be grounded in robust research evidence and a fit organisation or individual with an interest in workforce
for purpose and ethical governance framework that education and development, with a view to informing the
patients, public and staff can all trust. Final Report.
• Gift of time: Whenever possible, the adoption of
technology should be used to give more time for care,
creating an environment in which the patient-clinician
relationship is enhanced.
5
2.0 Approach
Dr Eric Topol is leading the Review and has formed a Review Board
of leading experts in genomics, digital medicine, AI and robotics.
Health Education England (HEE) is facilitating the Review.
The Review Board is working through three Expert Advisory Panels. This is the first
time that such an array of subject matter experts – clinicians, public health experts,
economists, educationalists, ethicists, engineers, physical scientists, lay members of HEE’s
Patient Advisory Forum and researchers – have been assembled to focus on education
and workforce development.
The work of the Review is taking a phased approach, with the Expert Advisory Panels
gathering evidence from diverse sources. The first phase has involved research and
engaging with individuals and national networks to gather knowledge and evidence, and
identify the key themes.
This Interim Report launches a wider discovery phase through summer 2018 to inform
the Review, with an open call for evidence, followed by a series of workshops with key
stakeholders, including representatives from patient groups and the public.
The Panels are taking into account realistic timeframes for making changes in workforce
development, education programmes and curricula. The Review will look at near-term
programmes (the next five years), plausible medium-term changes (the next decade) and
the potential for long-term developments (on a 20 year timescale). The focus of the Interim
Report, however, is on the here and now.
Here and +7-10 years +20 years
now
+5 years
2023 2028 2038
The challenge for the Review is to explore the options available on these different
timescales systematically, and to use the evidence it gathers to offer conclusions in the
Final Report on what this means for the education and training of the workforce.
The Final Report will be submitted to the Secretary of State for Health and Social Care in
December 2018. Wider engagement on the findings is planned from January 2019.
6
7

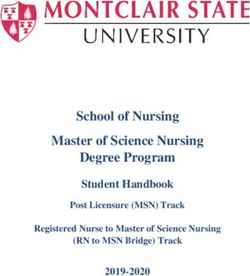
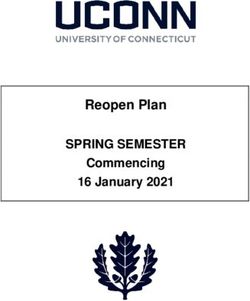
3.0 Workforce profile
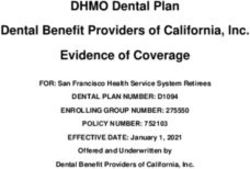
The current NHS workforce in England is comprised of the following high-level groupings
Figure 1: Numbers of staff in Hospital and Community Health Services (HCHS) and in General and
General and Personal Medical Services by group (000s)
Other HCHS
Doctors (excluding
Consultants, Consultants and GPs)
Other GP Practice staff 49 68
(direct patient care GPs (excluding
and admin), 111 Registrars, Retainers
and Locums) 34
Infrastructure
Support Staff,
342
Nurses and Health Visitors
(inc Nurses working in GP
Practices), 342
Midwives, 26
Support to Scientific, Therapeutic
Clinical Staff, and Technical (inc
Ambulance
366 AHPs, Pharmacists and
Staff, 22
Healthcare Scientists), 156
(Source: NHS Digital)
8
9

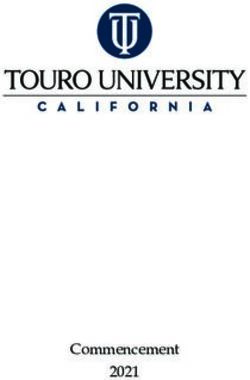
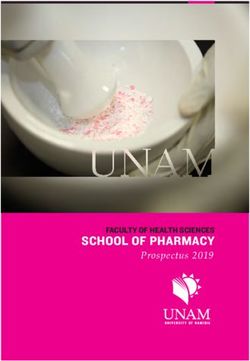
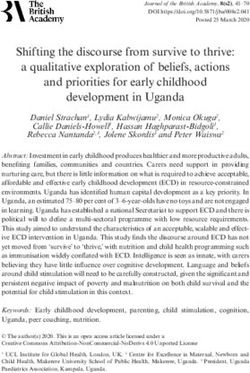
Over the last eight years there has been differential growth in different staff groups
Figure 2: Percentage increase in Hospital and Community Health Service (HCHS) staff 2009-2017
35%
Consultants
30%
Ambulance Staff
25% AHPs and Scientists
Midwives
20%
Support to clinical staff
15% Non-consultant Doctors
Nurses and health visitors
10%
5%
0%
-5%
Sep-09 Sep-10 Sep-11 Sep-12 Sep-13 Sep-14 Sep-15 Sep-16 Sep-17
(Source: NHS Digital)
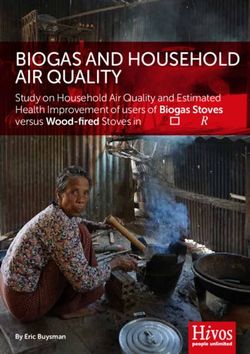
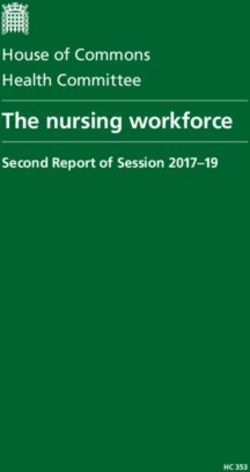
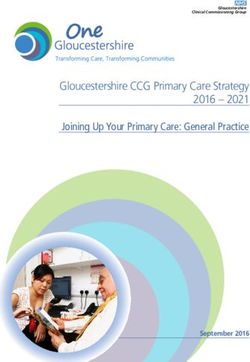
10The NHS employs more staff now than at any other time This Review will help forecast, in its Final Report, whether
in its 70 year history. Whilst the workforce has grown, it incorporating the new technologies will have an impact
has not kept up with ever increasing demand. The NHS is on the projections for the expanded workforce, with
treating a growing and ageing population that has grown different types of staff likely to be needed in different
by 2.1 million (4%) over the last five years. HEE forecasts numbers, as staff roles change or new roles emerge.
that if we fail to reduce demand and increase productivity,
then we will require at least 190,000 more staff by 2027
(Fig. 3). Maintaining the current rate of growth will
provide an additional supply of 72,000.
HEE forecasts that if we
fail to reduce demand and
increase productivity, then
we will require at least
190,000 more staff by 2027.
Figure 3: Recent Projection for Future Demand for Staff - Beyond 2021/22
1400000
1300000
Future Demand >2021
1200000
Staff in Post - Current trend
1100000
Staff in Post - Forecast to 2021
1000000
900000 Staff in Post - Historic
800000
Mar-12
Mar-13
Mar-14
Mar-15
Mar-16
Mar-17
Mar-18
Mar-19
Mar-20
Mar-21
Mar-22
Mar-23
Mar-24
Mar-25
Mar-26
Mar-27
114.0 Educating the
healthcare workforce
The successful integration of any new Genomics in primary care
technology or system into the workplace
Healthcare professionals in primary care
requires a highly engaged and appropriately will need to be educated and trained
trained workforce. There are known barriers in genomics for a variety of purposes.
to embracing technological changes in For example, they will increasingly need
to incorporate polygenic risk scores in
healthcare. These include lack of trust in new
assessing risk of various chronic diseases
technologies, the precedent of poor previous and implementing primary prevention.
experience with electronic health records, fear
• Take genetic variation into account when
of the pace of change and the feeling of being making therapeutic choices.
unprepared to engage with new systems.
• Consider the implication of genetic
The education and training of the existing workforce, diagnosis for counselling and screening
along with the preparation of an appropriate pipeline of the extended family.
of talented future staff, will be key to the success of any • Have a sufficient knowledge of genomics
programme of change designed to empower staff to to have a sensible dialogue with patients
take advantage of the advances in technology to improve across a spectrum of questions.
service delivery. HEE has already launched a Genomic
• Know when, how and where to refer
Education Programme, initially with a £20million pound
patients to for specialist advice.
investment by the Department of Health, which includes
a multi-professional MSc in Genomic Medicine currently
commissioned in seven Higher Education Institutes.
The NHS Digital Academy has also been set up as a virtual
organisation with a brief to develop a new generation of
excellent digital leaders2. It will train 300 Chief Clinical
Information Officers in the next three years.
The continued professional development of the existing
workforce will need to be different for those ‘specialist’
members of staff who will be intimately involved in using new
technology compared to the ‘light touch’ education required
by other members of staff who will probably only need
to know general principles. For the latter, HEE has already
started Building the Digital Ready Workforce and has a well-
established Technology Enhanced Learning programme.
Additionally, it will also be crucial to address the needs of
returners if we are to retain these individuals. At the same
time, by working with schools and universities, we need
to ensure that the next generation of clinicians have the
digital literacy and patient engagement skills which the
NHS of the future will require.
12HEE has already launched a
Genomic Education Programme,
initially with a £20million
investment by the
Department of Health.
134.1 Requirements of a future workforce New areas of knowledge and skills will be required, such
as an understanding of genomics or AI algorithms and
The knowledge and skills which a future workforce will the ability to analyse and understand the implications of
require in an era of technological advancement can be big datasets in the provision of future healthcare services,
considered under the following headings: as well as a major increase in digital literacy.
• What needs to be retained?
Given the history of failure of previous technological
• What new things are needed? systems within the NHS, it will be important to engage
the hearts and minds of the workforce who, given the
• What needs to be enhanced?
intensity of the present workload, may feel beleaguered
• What could be devolved to external sources? and cynical when asked to adopt and trust new
technology. Consideration needs to be given to involving
With the advent of cognitive computing, it will be
clinicians in user-centred design and co-creation of new
important to identify what knowledge clinicians need to
ways of working.
have to provide up to date, safe healthcare. And where
should that knowledge reside – in their heads, on their The advantages of adopting new ways of working over
mobile device or from the ‘machine as part of the team’? existing systems must be made clear and sufficient time
for training and re-training will need to be incorporated
The use of small mobile ultrasound devices means that
into normal working hours. Delivering the education and
some traditional clinical skills, such as listening to heart
training for the NHS workforce in England will require a
and lung sounds, may be superseded. However, skills
significant investment in ‘educating the educators’.
and attributes such as communication, compassion,
empathy, and caring will retain a central role for clinicians. As well as the upskilling of existing clinicians,
Furthermore, the improved workflow and efficiency of consideration should also be given to the desirability
new technologies affords the opportunity for not just of developing new professional groups such as clinical
retaining, but enhancing and giving higher priority to data scientists, medical software engineers and
the patient-doctor relationship. Creativity, innovation, digital medicine specialists. New technologies and the
enterprise and an ability to embrace and lead change will emergence of increasing amounts of patient data will
need to be fostered. bring with them the need for increased training in ethics
and data governance. Delivering the positive impact
that these new technologies could have on the NHS will
require digital leadership across the health and social care
system, with a willingness to embrace new technologies.
New areas of knowledge
and skills will be required...
as well as a major increase
in digital literacy.
144.2 Methods of education and training In summary, the potential to reshape and improve
healthcare using new technologies is huge, but without a
Technology will be increasingly useful in providing highly trained workforce, confident and competent to use
education and training at scale. The development of online these new systems, in partnership with the patient and the
courses, podcasts and Massive Open Online Courses carer community, their full impact is unlikely to be realised.
(MOOCs) or Small Private Online Courses (SPOCs) is likely
to become important to reinforce or supplement face-to-
face teaching. The use of augmented reality/virtual reality
and immersive environments will also have a role, especially
in those areas which are difficult to cover in the workplace
and as their cost becomes more affordable.
155.0 Ethics
Whilst technological developments promise At the same time, the NHS is founded on a commitment
to equal and equitable access to healthcare for all UK
very significant benefits to improve
citizens. However, the health and well-being gap was
healthcare, many rely critically on the ability highlighted in NHS England’s Five Year Forward View as
to collect, store, access and share health one overarching reason why the NHS needs to change.
related data, including data gathered via
Although access to digital technologies has the potential to
pervasive surveillance techniques (through improve and streamline patient care within the NHS, there
continuous monitoring and tracking) that is a real risk that existing inequalities may be exacerbated
many consider highly intrusive. unless consideration is given as to how technological
innovations affect equality and equity in healthcare.
Within constitutional democratic societies, surveillance,
even for laudable purposes, is not acceptable unless These ethical concerns are shared in the Nuffield Council
it is undertaken in ways that are consistent with the of Bioethics’ Briefing Note on artificial intelligence in
fundamental rights to privacy and data protection. healthcare and research. It is very important to focus on
how equal access to advanced healthcare can be assured.
Without transparent, resilient, robust and legally Indeed, the new technologies could either improve or
enforceable data governance structures3, policies and worsen health inequities; the objective should always be
practices that the British public regard as ethical, rights- to maximise the positive impact.
respecting and trustworthy, the promised benefits of
data-driven technological innovations in healthcare and
medicine will not be realised.
166.0 Health economics
The introduction of new technological
developments in genomics, digital medicine, The adoption of a new
artificial intelligence and robotics in
healthcare has the objective of improving technology in one part of a
the care of patients either directly or health service may have
indirectly by using health service resources
more productively. ramifications for care provided
However, efficiency alone is not sufficient and may be in other parts of the service.
traded off against effectiveness and equity. This has
implications for which technologies are developed and how
they are used. A technology seeking to maximise efficiency A narrow consideration of the costs and benefits of
may look very different to a technology addressing the adopting a technology that only takes the perspective of
same issue but also seeking to improve equity. an individual provider for the NHS will miss these spillover
effects. This runs the risk that any policy based upon a
The adoption of a new technology in one part of a health narrow perspective will not be an efficient use of society’s
service may have ramifications for care provided in other resources and may increase inequalities within society.
parts of the service. It may also spill over into effects
beyond healthcare. For example, a new genomic test that The value of any new technology is also dependent upon
characterises the underlying causes of bone development the ease in which that technology can be implemented
abnormalities in children may directly allow earlier into practice. A technology that can be readily slotted
treatment and therefore alter the subsequent need for into care and practice may be able to realise productivity
orthopaedic surgery on the children affected. improvements relatively quickly and so improve patient
outcomes, efficiency and reduce inequalities. The more
An indirect impact on the health service is that the disruptive a technology, then the longer it may achieve
introduction of this test may reduce the ability to provide these benefits in practice. It was only in the 1980s that IT
certain types of surgery other than in specialised centres. was used in the majority of industries and it took time to
A further indirect impact is that it may reduce the need for learn how to use the technology to its best advantage.
long-term social care support as children have less disability.
Similar issues may be expected within health care. For
In this case, the spillovers are positive, but in other cases example, if a new test is better able to determine the risk
it is possible that they might be negative. For example, a of recurrence or progression for those who have been
new technology to treat stroke may increase the number treated for cancer, this could provide some immediate
of stroke survivors but still leave these people with improvements in the care of patients but without fully
considerable disability. This would in turn increase the understanding how the technology is best used, its full
need for rehabilitation services and social care services, as benefits may not be immediately realised.
continuing care is typically provided in the community.
There would also be a wider impact on patients and families,
because an important component of care for someone who
has had a stroke is that informally provided by friends and
family. These informal care costs will be disproportionately
more important to those who are less well off.
177.0 Themes Expert Panels have been convened to provide expert evidence on the following three themes: (i) genomics; (ii) digital medicine; (iii) AI and robotics. Their early findings are summarised in the sections below. Of the technologies considered, genomics is the most advanced, in terms of research evidence, implementation, and workforce development, with a new MSc programme and newly created NHS roles. This is followed by digital medicine, which is rapidly advancing with the spread of smartphones and computer tablets, although uptake remains uneven. More research is needed to evaluate clinical pathways that take advantage of digital technologies within optimised health systems. Further training will inevitably be required if the workforce is to benefit fully from digital medicine. At the other end of the innovation pipeline, we are only just beginning to discover the potential for AI, in particular machine learning, to personalise care, improve patient outcomes and reduce the workload of healthcare professionals. The real power of these technologies is likely to lie at their intersection. The fusion of genomics, digital medicine (including patient generated data) and AI, could deliver a more holistic approach to personalised healthcare and disease prevention. Although the type and amount of data will vary and change at very different rates (from once in a lifetime for genetic data to once a second for some types of wearable data), AI algorithms will become increasingly important to extract clinically useful information from such disparate data. The impact of this integration will also vary from one medical specialty to another. In oncology, for example, the integration of multi-omics with clinical phenotypes to analyse data will enable the prediction of a patient’s response to new cancer therapies. 18
8.0 Theme 1: Genomics
The UK is a world leader in genomic
research and medicine and well placed
to remain in the vanguard of future
developments. Over the next 20 years,
there will be major advances in the use of
genomics across diverse areas of medicine.
For example, rapid sequencing first approaches in
sick newborns – along with children or even adults –
Genomics will revolutionise with unknown but serious conditions will reduce the
multiple aspects of cancer ‘diagnostic odyssey’ – the long delays and marked
care, from prediction expense of traditional medical evaluation. Genomics
will revolutionise multiple aspects of cancer care, from
through to screening, prediction through to screening, diagnosis, treatment and
diagnosis, treatment and post-treatment surveillance. Preventative strategies for the
common diseases of ageing will be bolstered and made
post-treatment surveillance. more precise through improved quantification of genetic
predisposition based on polygenic risk scores.
Genetic diagnostics will enable more efficient targeting
of drugs maximising efficiency, optimising dose and
minimising side effects. New forms of treatment,
especially for inherited diseases, will emerge based on
genome editing and cellular replacement.
Substantial progress in service transformation to
incorporate genomic medicine has already occurred
throughout the NHS. In England, preparation for the
implementation of genomic medicine has been led
by NHS England and Genomics England, through the
100,000 Genomes Project4,5 and the establishment of
Genomic Medicine Centres. In parallel, the HEE Genomics
Education Programme has been responsible for preparing
the NHS workforce to deliver genomic medicine through
knowledge, skills and experience. There are a growing
number of examples where patient management has
been transformed through genomics.
198.1 The citizen and the patient Genomic medicine is likely to impact citizens in many different ways and at different stages of their life-course. If they are to become more active contributors to their health and care, they must be supported to develop their understanding of genomics. This will require easy access to relevant knowledge resources, as well as a ‘socialisation’ of genomics that allows them and their relatives to interpret the personal implications of findings arising from genetic and genomic information. Citizens will need to be supported to engage with decisions around risk, ethics, privacy, insurance, employment and fertility. Genomics needs to be factored into school and workplace education, with parallel approaches to inform the adult population. Individual patient decisions regarding the use of sensitive data for clinical and research purposes must be based on transparent discussion about the costs and benefits of data sharing, and updating of the social contract underpinning delivery of a national health service. This will involve clear articulation of the benefits in terms of better, more tailored care, more accessible and effective interactions with the health system, and the fostering of further advances through research. Patients and carers must have confidence that there is adequate regulatory protection in the public and the private (including direct to consumer) sectors, with respect to data misuse and unsupported claims. These advances will require a more equitable relationship between the patient and their clinician, recognising that wider access to information and personal empowerment will result in citizens who are ever more informed about their health and any condition which they may have, and who also expect shared decision making. 20
8.2 Healthcare professionals Undergraduate and postgraduate curricula for all
healthcare professionals must include genomics and its
We anticipate a gradual, but substantial, reconfiguration relevance. Education and training should also be rolled
of clinical roles to meet the new challenges associated out to existing healthcare professionals as part of a
with the introduction of complex, evolving genomic system for life-long learning, accreditation, and retraining.
technologies. The pace of change will differ by speciality Given the rapid pace of technical development and
and by individual medical practice, but will ultimately knowledge accumulation, healthcare professionals will –
impact on all healthcare professionals. in addition to generic training and tailored accreditation
schemes – need access to real time resources to support
Individual workforce training needs will depend less dynamic, up to date, interpretation and decision making.
on traditional role demarcations, and more on specific
responsibilities related to ‘real-world’ implementation. Clinical education should emphasise, not the burden of
For example, for a given genetic test, members of the acquiring additional knowledge, but opportunities for
workforce will be variously contributing to commissioning, improvements in the overall quality, productivity and
gaining consent (of patients), ordering, genetic test data equity of care.
generation, interpretation, patient communication and
family support. This will require training that supports their
specific activities. This will be associated with acceleration
of the shift towards multi-disciplinary working and a
change in many professional roles.
Widespread introduction of genomic technologies
within the NHS will require a combination of distributed
(‘mainstreaming’) and centralised procedures (e.g.
related to ordering and interpretation of a genetic test). Genetic Diabetes Nurse
Healthcare professionals of all kinds will increasingly be
involved in aspects of care previously devolved to more The Genetic Diabetes Nurse (GDN) role has been
specialised colleagues, such as those related to ‘routine’ developed to support the integration of genomic
genomics (e.g. pharmacogenetics, and risk prediction for testing into diabetes care. GDNs are experienced
common diseases). diabetes specialist nurses who raise awareness,
understanding and recognition of monogenic
Given the evolution of knowledge and the relevance forms of diabetes. An accurate genetic diagnosis
of genetic information to the health status of relatives, is essential to identify those patients who may
clinical responsibility will extend beyond the index benefit from treatment tailored to their genetic
consultation. This includes ‘dynamic reporting’, subtype. GDNs work as a national network with
supporting re-contact with patients when updates in training provided by an expert multi-disciplinary
knowledge mandate revision of previous clinical advice. team of clinicians, nurses and scientists based
This long-term duty of care extends beyond the index in Exeter. The GDNs liaise with local healthcare
cases to their wider families. teams to advise about genomic tests, help co-
ordinate genetic testing for family members and
Counselling6 and broader support mechanisms will require support patients through treatment changes.
expansion to address the complex task of conveying risk and
other probabilistic information to patients and their families.
21Clinical Bioinformatician available tools and choose those most appropriate
to meet the needs of the clinical service, as well
A Clinical Bioinformatician works within multi- as analyse data using appropriate software tools.
disciplinary teams to understand the needs of the Bioinformatics training in the NHS will be an
services and communicate genomic data today, evolving programme of workforce development
and phenotypic data in the future, in the context of and transformation, starting with genomics and
patient care. Clinical Bioinformaticians are able to broadening out to include phenotypic information,
evaluate, validate and understand the limitations of including patient-generated data.
8.3 Health system counselling, bioinformatics, computing, data sciences,
health economics and commissioning. This will require
Reconfiguration of the health system is essential if appropriate training, and robust structures for career
genomic medicine is to be implemented in ways that progression and staff retention. It will involve a marked
ensure patient safety and data privacy, improve equity and expansion of opportunities for the re-training of existing
productivity, reduce unacceptable variation in quality and staff, recognising that workforce requirements for some
outcomes, and enable sustainability. specialised roles will decline.
This will require infrastructural developments that The Genomics Education Programme will continue to
capitalise upon existing efforts, for example, to integrate play a key role in developing an educational framework
clinical genetics services nationally, to extend genomic for the workforce and undertaking workforce planning
multi-disciplinary teams, and to develop a national and modelling.
genomic laboratory network underpinned by the genomic
testing directory. There will need to be substantial revision There need to be parallel mechanisms for supporting
of service provision to ensure that the NHS meets its methodological and mechanistic research in the academic
obligations regarding the follow up and management of sector which uses NHS data to advance translational
significant findings in the relatives of index cases. objectives. Above all, the NHS needs to ensure that the
efficiencies in healthcare delivery that result from the
Genomic medicine will necessitate development of introduction of genomic medicine lead to manifest and
new specialisms (and/or substantial expansion of tangible benefits in the quality of care delivered.
existing workforce) in diverse areas including genomic
22Genomics in Cardiology
Cardiologists and other health care professionals
in cardiovascular medicine will encounter
patients and families who may have an inherited
cardiac condition. They therefore need to be
trained and educated about genomics, when
it could be relevant, know when and how to
refer to a Specialist Inherited Cardiac Conditions
service and be aware of the importance of taking
a family history. The ability to tailor cardiac drug
treatment to an individual’s genetics is rapidly
increasing, and so education and training for
healthcare professionals will need to be agile and
adapt to this rapidly progressing field.
239.0 Theme 2: Digital medicine
The fast changing pace of digital medicine 9.1 The patient
is already having a positive impact on the
Digital medicine is increasingly empowering patients
NHS, although the rate of take-up and to manage their own health and well-being, and this
benefits are unevenly distributed amongst will naturally transform the traditional patient-clinician
the population. relationship. There is a growing acceptance of the use of
smartphones and wearables to track vital signs, such as
In this report, digital medicine is defined as digital heart rate and abnormal rhythms, blood glucose and blood
technologies and products that directly impact diagnosis, pressure8. Amongst those who use digital technologies to
prevention, monitoring and treatment of a disease, manage their health, use of wearables went up from 22%
condition or syndrome. This includes telemedicine, to 31% between 2016 and 2018. Launched in April 2017,
wearables, digital diagnostic tests, bionanotechnology, the NHS Apps Library provides digital tools for patients with
digital therapeutics and immersive technologies such as a range of conditions, from diabetes, chronic obstructive
virtual and augmented reality. pulmonary disease and cancer to depression. There are
currently 47 ‘trusted and assessed’ apps available in the
Today, an estimated 89% of UK adults have used the Library (https://apps.beta.nhs.uk).
internet in the previous three months7 and use among
women aged 75 and over has almost trebled since 2011. Cognitive Behavioural Therapy (CBT) is increasingly being
NHS England, in May 2018, estimates that 24% of delivered digitally, for example for the management of
patients in England (13.9 million people) are now sleep disorders. Activist patients are co-developing new
registered for online services with their family doctor to digital technologies to meet their needs, such as the
book appointments, order repeat prescriptions and view #Wearenotwaiting movement for diabetes.
their records – saving time for themselves and busy GP
practices. Half of all adults access health information To increase the adoption of digital health technologies,
online; each day, there are approximately 1.6 million public health campaigns should include education
online searches for health information on NHS Choices on modifiable risk factors and training on how such
(82% via search engines and 75% of visits on a mobile or technologies can be used to prevent common conditions
tablet device). NHS England also estimates that 60% of such as obesity and hypertension. There is a need for
the people who use the internet to check a condition do investment in national digital literacy public health
not then go on to access a frontline service. campaigns to educate everyone, from children in primary
schools, to young adults and the elderly. For those
without direct access to the technologies, digital health
learning tools should be made accessible in schools,
89% of UK adults have used the internet public libraries and GP surgeries. The adoption of digital
medicine must not have the unintended consequence of
in the previous three months
increasing health inequalities.
24% of patients in England With this in mind, NHS Digital has recently released
for commissioners and designers of digital health
(13.9 million people)
technologies a ‘Digital inclusion guide for health and
are now registered for social care’ (https://digital.nhs.uk/about-nhs-digital/our-
online services work/digital-inclusion).
There are approximately 1.6 million
online searches for health information
on NHS Choices
249.2 Healthcare professionals Mechanisms by which the existing healthcare workforce
could be given dedicated time to learn how digital
The Wachter Review highlighted the need for digital technologies can enhance their practice of medicine
leadership in the NHS, and this year the first national NHS should be introduced, for example through immersive
Chief Clinical Information Officer was appointed. virtual reality for trainee doctors prior to new rotations,
To deliver the benefits of digital medicine throughout the mentoring apps and agile MOOCs for lifelong learning.
NHS, healthcare professionals will need to learn about
data management, data privacy, data quality, ethics and
regulation. They will have to be trained in how to interpret
patient-generated data (including data from wearables
acquired over several weeks or months) alongside
traditional health data such as X-rays and blood tests.
Emerging technologies, including smartphone-connected
Diabetes specialist midwives
diagnostic tests, will enable earlier diagnosis of disease,
more personalised/stratified treatments, and could also Gestational diabetes affects between five and
reduce the unnecessary prescribing of antibiotics. Doctors 16% of all pregnancies in the UK. It is important
will need to learn how to prescribe digital therapeutics, for the health of the mother and baby that
for example evidence based apps available from the glucose control is maintained, but as a result
NHS Apps library as an alternative to drugs. In future, of the dynamic physiology of pregnancy, it is
interventions will increasingly focus on disease prevention, difficult to predict how blood glucose levels
health and well-being. will respond. The GDm-HealthTM management
system, developed by researchers from Oxford
Online consultations9 and video calls, as an enhancement
University and clinicians from Oxford University
of telephone triage, will gradually become accepted
Hospitals NHS Foundation Trust, provides real-
within primary care and potentially secondary care, for
time management of gestational diabetes
example in Accident and Emergency. The number of online
and reduces the number of clinic visits. The
consultations may eventually supersede the number of
system was designed with extensive input from
face-to-face consultations, necessitating new training in
both patients and clinicians. It comprises a
remote patient management. Benefits will include increased
smartphone app for the patient and a secure
productivity, both for patients who will not need to take
website, with optimised data presentation and
time off work to visit the clinic, and for clinicians, with more
alerting algorithms for healthcare professionals.
time becoming available for them to care for more complex,
serious cases through face-to-face appointments. Local care pathways have been changed to allow
a reduction in unnecessary clinic visits. Similarly,
The deployment of digital technologies within the NHS
the job plans for midwifes are being modified to
should be user centred and have as one of its main
accommodate new ways of working with remote
objectives the reduction of the administrative burden
management of pregnant women.
on healthcare professionals. For example, automatic
speech recognition technologies, also known as ‘smart
speakers’10, and other ‘machines in the team’, should
allow doctors and nurses to spend less time entering
information using their computer keyboards during
face-to-face consultations, and so free them to focus and
connect more with the patient.
259.3 Health system
The benefits of digital medicine will only be realised at
scale, within a fit for purpose, trusted NHS governance
framework. More interdisciplinary research, with large scale
test beds, is needed to evaluate the impact of the new
technologies, and their implications for data governance.
Today, the delivery of care largely centres around
the attendance of patients in clinics for face-to-face
consultations. In future, remote delivery of care to
patients in their homes will become more prevalent via
telemedicine. The healthcare workforce and patients will
need to be trained in how to use telemedicine in new
online care pathways to diagnose, monitor, educate and
treat patients.
More acute care will also be possible through the expansion
of ‘hospital at home’ schemes, which enable patients to stay
in their own homes whilst receiving extra care and attention
from the multidisciplinary hospital at home team. These
schemes are designed to give patients extra support at home
using technology, to ensure that they are not admitted to
hospital or that their admission is as short as possible. The
aim is to reduce the pressure on emergency departments Support Hope and Recovery Online
and manage demand for acute care.
Network (SHaRON)
The vision should be to deliver high-quality personalised
SHaRON is a peer to peer ehealth therapeutic network
care regardless of location (home, care home, pharmacy,
connecting various individuals and supported by NHS
community hospital or acute hospital). This will be
clinicians, for people who have mental health conditions.
enabled by appropriate patient monitoring technology
(a combination of wearables, smartphones and their SHaRoN helps clinicians track and monitor clients’ mood
accessories), supported by the deployment of community and progress 24/7, and spot possible signs of deterioration
nurses, and paramedics for rapid response when needed. or changes in behaviour suggesting a relapse, for timely
interventions. Clinicians are able to provide psycho-
New professional groups will need to be grown within
education to individuals and groups as indicated.
the NHS (e.g. behavioural psychologists, human factors
experts, medical virtualists11) to extract maximum benefit Clients provide peer education which keeps them actively
both for patients and for the workforce. New roles and engaged with their care and is beneficial to recovery.
career pathways will emerge for clinical bioinformaticians
and healthcare data specialists with an interest in In addition to reading governance and policy documents,
developing machine learning algorithms to analyse NHS clinicians receive two hour practical training sessions to
datasets to support public health research, for example to develop confidence and skills in moderating an online
predict influenza epidemics. platform. Clinicians who are not digitally savvy are
offered individual and group clinical and management
supervision through Skype to introduce them to the use
of a digital intervention.
https://www.sharon.nhs.uk/
26In future, remote delivery
of care to patients in their
homes will become more
prevalent via telemedicine.
2710.0 Theme 3: AI and Robotics
Over the next two decades there is great 10.1 The patient
potential for AI to improve healthcare12.
The introduction of AI enabled virtual health coaches
The remarkable promise of AI is particularly which incorporate behavioural science can nudge patients
centred on machine learning, including towards a better lifestyle and help them to manage
deep learning13. their medications, reducing the overall risk specific to an
individual patient. Unified personal records that integrate
Machine learning is a branch of AI that allows computer the increasing amount of patient-generated data with
systems to learn directly from examples, data, and electronic health records will benefit patients by allowing
experience. Deep learning enables computational models health prompts to be delivered remotely, enabling
that are composed of multiple processing layers to learn patients with long-term conditions such as asthma,
representations of data with multiple levels of abstraction. diabetes, or heart failure to self manage better. Patient
specific prediction of disease progression and smarter
As computer processing power continues to progress, appointment scheduling will also be possible.
machine learning will generate patient, clinician
and health system benefits from the vast amount of AI is enabling patients with mental health illness to access
healthcare data available today. Machine learning is therapy services from any internet enabled location
advancing at such a rate that it can now outperform (including the patient’s smartphone) at a time of their
humans on some specific tasks. Actionable intelligence choice. Natural language processing technology, a form
will be extracted to better predict, prevent, screen, and of AI, is being used to enhance CBT through real-time
diagnose disease. AI and machine learning will facilitate online conversation with therapists16.
treatment tailored to each patient.
Emerging robotics technology includes an advanced
Carefully designed AI algorithms will also enhance NHS bionic arm, small enough to fit children as young as nine.
productivity, through large-scale process optimisation, New manufacturing techniques based on 3D scanners
clinical pathway streamlining and public health and printers, radical reduction in fitting time, and the
applications. By offloading some human tasks to advanced functionality of the limb are gradually changing
machines, when appropriate and properly validated, the way prosthetists, orthotists, occupational therapists
clinical workflow and productivity could be greatly and physiotherapists work with patients.
improved throughout the NHS.
Patients must be able to access education and technical
Advances in medical software and hardware are support in how to set up and best use new digital
accelerating the field of clinical robotics. Current uses technology. Improved patient education and support could
of robotics in the NHS extend significantly beyond be facilitated either by creating new professional roles or
automating repetitive tasks and include minimally invasive through upskilling clinicians in the community, for example
prostate cancer surgery, a robotic radiotherapy system pharmacists, primary care nurses and health visitors.
(that minimises damage to healthy tissue) and 3D printed
bionic arms for amputees14.
On the horizon are robotic technologies including soft
robotics, robotic platforms for microsurgery, advanced
robotic endoscopy, capsule robots and wearable robots
including exoskeletons. Rehabilitation and assisted living
robots which can help patients recover from stroke or
support people with dementia are also being developed15.
28Patients must be able
to access education and
technical support in how
to set up and best use
new digital technology.
2910.2 Healthcare professionals
Healthcare professionals spend anywhere between 15
and 70% of their working time performing administrative
tasks. AI systems will in the near future be capable of
ordering tests, compiling medical notes and completing The AI-enabled future
other administrative tasks. These AI systems will provide ophthalmologist
the NHS with the biggest productivity gains and will allow
healthcare professionals to focus on the clinical tasks that The number of optical coherence tomography
patients consider uniquely human, giving more time for (OCT) scans in the UK needing analysis is set to
patient-clinician interaction and communication. rise dramatically and scans are increasingly being
performed by community optometrists. Deep
AI, machine learning and robotics technology will support learning algorithms have been trained to identify
clinicians in delivering safer, higher quality care. Machine pathology automatically from OCT scans, enabling
learning enabled early warning systems are used in hospitals robust early detection and triage of sight-threatening
to alert clinicians to patients at risk of deterioration, allowing diabetic retinopathy and age-related macular
them to deliver treatment that prevents severe illness, as degeneration. The use of this technology in clinical
recently demonstrated for sepsis management17. practice would greatly enable both ophthalmologists
and optometrists, streamlining their capacity and
Deep learning technologies have already shown capability to treat the most at-risk patients, and
expert-level performance in medical image analysis, allowing them to enhance their own diagnostic skills
in domains such as screening for breast cancer, skin through learning from the technology.
cancer or eye diseases18. Whilst radiology, pathology and
ophthalmology are frequently cited as the disciplines
most likely to be influenced by AI tools, the impact will
inevitably affect all specialties and every clinician from
doctors to nurses, pharmacists to paramedics and beyond.
All clinicians should be educated in the ethical standards
and good practice of working with AI, best practice in
data curation and governance and the interpretation of
clinical statistics and recommendations generated by AI Chief Clinical Information Officer
systems. The NHS needs AI specialists who understand
the requirements of patients and healthcare professionals The NHS appointed the first Chief Clinical
and are keen to be embedded in all care settings, so that Information officer (CCIO) in 2016. The CCIO
AI systems designed for healthcare are fit for purpose. role has subsequently been rolled out across NHS
Provider Trusts. CCIOs support the strategic aims
of the Trust for clinical engagement and adoption
of technology, focusing on patient outcomes
and productivity to continuously improve patient
care. CCIOs are providing a clinical voice to the
implementation of Electronic Health Records.
CCIOs usually have over 10 years’ experience as
a healthcare professional, usually as a doctor or a
nurse with additional experience in direct clinical
systems and process re-design.
3010.3 Health system potential benefits of analysing these datasets, the NHS
needs a high quality, secure, information infrastructure,
Potential applications of AI to improve systems efficiency explicitly co-designed and agreed with the public,
and productivity include optimisation and prediction which has the ability to aggregate and integrate patient
of patient flow through the hospital; improvements to generated information with data across different health
the current efficacy and efficiency of procurement; and and care settings.
enhancement of workforce logistics and service planning.
AI will also increasingly be used to monitor public health The NHS is starting to develop this infrastructure through
trends, identifying initiatives that have a positive impact its local health and care record exemplar programmes.
on population health. Since 2016, Chief Clinical Information Officers - clinicians
with additional experience in re-designing health systems -
A key goal of using AI technologies must be to integrate, have been appointed in the NHS to try to ensure that only
analyse and personalise digital data in order to provide user-friendly electronic health records meeting current and
health services in the community, such that treatment in future patient needs are implemented.
hospital becomes increasingly unnecessary. Advances in
the vision abilities of machines, if sensitively deployed, and Using better integrated electronic health datasets, machine
remote monitoring should enable patients to be safely cared methods have been shown to better predict clinical risks
for in the comfort of their own homes, by staff educated in various, particularly complex, diseases. These methods
and trained in ways of working in modern, non-centralised, are also capable of better tailoring therapy to the needs of
health systems. Remote monitoring has the clear potential to an individual patient. Additionally, machine learning could
reduce the need for acute hospital services. facilitate research that reduces health inequalities through
finding therapies for complex patients frequently excluded
One of the NHS’s greatest assets is its comprehensive from clinical trials; for example the elderly, or patients with
datasets. For AI and machine learning to realise the multiple health problems.
31While it’s hard to predict the future, we know artificial intelligence, digital medicine and genomics will have an enormous impact on improving efficiency and precision in healthcare. This review will focus on the extraordinary opportunities to leverage these technologies for the healthcare workforce and power a sustainable and vibrant NHS.” Dr Eric Topol Dr Eric Topol at work with the Technology Review Panel 32
11.0 Open call for evidence
We have identified a series of questions as
part of an open call for evidence. We invite
responses from any organisation or individual
able to inform the thinking of the Review.
Please join in the conversation at
Topol.hee.nhs.uk where you will
be able to find a set of questions
to start the conversation.
The closing date is Wednesday
29th August at 12.00 noon.
This Interim Report is the beginning of the conversation.
Evidence and comments are being sought from any
organisation or individual with an interest in workforce
education and development, with a view to informing
the Final Report.
This will be submitted to the Secretary of State for Health
and Social Care in December 2018. Wider engagement
on the findings is planned from January 2019.
33You can also read