Physician Manual Home Health|Home Infusion | DME Devoted Health Arizona 2021 - Prismic
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Physician Manual
Home Health|Home
Infusion | DME
Devoted Health
Arizona
2021
Phone: 1-602-732-4027 | Fax: 1-855-441-6941
Table of Contents Physician Welcome .............................................................................................. 3 Hours and Contacts.................................................................................................. 4 Referral Criteria ................................................................................................................. 5-9 Services that require a Letter of Medical Necessity ......................................... 10 Covered and Frequently Utilized Equipment ............................................................ 11-13 Covered and Non-Covered Services ......................................................................... 14-17 CPAP Ordering Information ..................................................................................18 CPAP Order Requirements................................................................................... 19 Skilled Nursing Facility Medication Request ........................................................ 20 Equipment Information/Reference Guide ................................................................. 21-22 Ostomy Guide ................................................................................................................... 23 Urological Supply Guide ..................................................................................................24 Provider Supply & Order Forms ..................................................................................... 25-32

Dear Provider,
We would like to take this opportunity to introduce you to One
Homecare Solutions, your Home Healthcare Provider for DME,
Home Health, and Home Infusion.
We are presenting this package to provide you with information
regarding our referral process, scope of services provided, ordering
requirements and guides, and our commitment to you and our
healthcare partners.
We look forward to working with you and your staff in the provision
of excellent patient and customer care!
Sincerely,
OneHome
OneHome | Provider Manual 2020 Page 3
Hours of Operation
MONDAY THRU FRIDAY: 9:00 AM – 7:00 PM(est)
CUSTOMER SERVICE/CALL CENTER EXTENDED HOURS:
7:00 PM – 9:00 PM(est)
SATURDAY & SUNDAY : 9:00 AM – 5:00 PM(est)
AFTER HOURS & WEEKENDS – ON CALL (24/7)
Contact Numbers
Phone: 1-602-732-6900 | Fax: 1-855-441-6941
OneHome | Provider Manual 2020 Page 4
Patient Referrals/Elements Needed on “Referrals”
Fax Referral/Orders to:
1-855-441-6941
All Requests Must Have Mandatory Elements as indicated on the Universal
Order Form: This is to be used as a reference guide when ordering specific
items as indicated within. PLEASE COMPLETE ALL ITEMS TO AVOID DELAYS.
Patient’s First Name: Patient’s Last Name:
Member#: DOB:
Health Plan: Insurance Type:
Patient Phone Number: Secondary Phone Number:
Home Address: City, State & Zip Code:
Service Address: City, State & Zip Code:
Alternate Contact Name: Primary Phone Number:
Relationship to Patient: Secondary Phone Number:
Primary Diagnosis & Code: Secondary Diagnosis & Code:
Date of Discharge: Facility Name:
Diabetic? □ No □ Yes Type: □ IDDM □ PO □
Diet: Ht. Wt. Allergies:
Phone
PCP -Name of MD: Number: Fax
Following MD/Specialist (if other than PCP): Phone
Number: Fax
Referrals’ contact
Referral Source/Person Filling out form: number: Referral Fax
HOME HEALTH ORDERS
□ RN Evaluation
□ PT Evaluation & Treatment
□ HT Home Infusion (Has patient received a first dose?) Y _ N
□ Administration ‐Medication, dosage, route & frequency/ duration:
□ Wound care treatment plan and wound location
□ Ostomy , ,
□ Diabetic , ,
OneHome | Provider Manual 2020 Page 5
DME ORDERS
HCPC Code Description Length of Need
OXYGEN ORDERS CPAP/Bi-PAP CPM Lymphedema
Liter Flow per Minute Please list all items and Settings:
Route: Nasal cannula, simple mask or other
Patient visit date:
Hours of use: continuous, with exertion, hours
of sleep, bleed into CPAP/Bi-PAP or other
Delivery Device: concentrator, portable
cylinders, conserving device, liquid, portable,
or other
Date of saturation test: (MM/ DD/ YYYY)
Oxygen Saturation or PO2 results: %
Physician Signature/Date
I certify that I am the treating physician identified in this form. I have received the Certificate of Medical Necessity (including charges for items
ordered). Any statement on my letterhead attached hereto, has been reviewed and signed by me. I certify that the medical necessity
information is true, accurate and complete, to the best of my knowledge, and I understand that any falsification, omission, or concealment of
material fact in that section may subject me to civil or criminal liability.
PHYSICIAN’S SIGNATURE DATE / /
PHYSICIAN’S NAME (Please print):
If Ostomy or Urological, please list item, #’s, brand, sizes and item quantity.
(i.e. 2 Piece Drainage Pouch #1234, Hollister, 30 per month / Straight Cath 14 Fr. Item#, Bard)
Please reference needed information for Oxygen, CPAPs, IV
Medications, CPM’s, Lymphedema Pumps/Ostomy and Uro Supplies.
OneHome | Provider Manual 2020 Page 6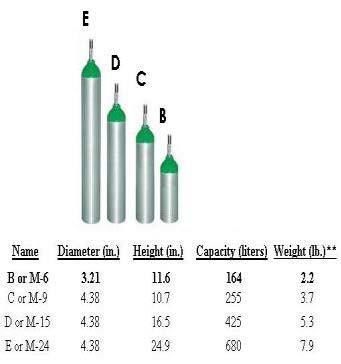
• Height and Weight:
• Used to dose or verify ordered medication dose. Note that many of the
medication doses are based on Weight. Most Chemotherapies are based on
BSA (Body Surface Area), so Height is needed.
• Also Ht. and Wt. is used to calculate CrCl (Creatinine Clearance), which is a
way to evaluate renal function.
• Allergies and First dose:
• Before an order is processed, a pharmacist should know what the patient’s
allergies are to be sure, ordered medication will not result in any harm to
patient. If patient has no drug allergies, NKDA (No Known Drug Allergies) it
does not mean that a patient will not react to medication.
• If patient is allergic to a drug class i.e. Penicillin, and a drug belonging to the
Penicillin class is prescribed, a proper documentation needs to be conducted
to indicate that either patient has been on the medication before, started
therapy already, or that MD is aware of allergy and approved the use of
ordered medication.
• If patient has received the ordered medication, we need to know when and
where therapy started (i.e. First dose at hospital on 08/01).
• Diagnosis:
• We need to obtain the right diagnosis for what is being ordered. This is
extremely important for the clinical pharmacist to evaluate the
appropriateness of the therapy and to make necessary adjustments
based on labs if applicable.
➢ Example. A patient is on Vancomycin to treat Osteomyelitis;
however, diagnosis documented is Cellulitis. Pharmacist get a
Trough result of 10, thinks it is therapeutic for Cellulitis and does not
make a dose adjustment. However, for Osteomyelitis 10 is sub
therapeutic (15-20 is the range), so by getting the wrong diagnosis,
we are misleading the pharmacist not to adjust the dose and
risking patient to an amputation, extended therapy, readmission,
etc.
• Ancillary Providers:
• Nursing Agency taking care of patient
• SNF (if patient is a resident of one). Please provide Room #
• Shipping Address:
• We need to know where the medication is going to be delivered.
• If medication is to be deliver to a Dr’s. Office or a clinic, accurate address,
hours of operation and contact person receiving the medication is required.
OneHome | Provider Manual 2020 Page 7
• Insurance (Payor Information):
• Pharmacy cannot process an order without an insurance company or payor.
• DOB:
• To properly evaluate the appropriateness of therapy and its clinical
monitoring.
• Contact Information / Emergency Contact
Please note below, very important:
• Last dose Given:
• For patients discharged from a hospital, we need to know when the last dose
was given to ensure timely delivery for next dose.
• Medication Profile:
• This include all active meds, vitamins, over the counter and supplements
patient is taking.
We encourage patient and family teaching and training and patient
independence.
OneHome | Provider Manual 2020 Page 8
When in receipt of an incomplete referral/patient order, you might receive the below Contact
Physician Form from us via fax. This is our way of expeditiously contacting you to request
information that might prevent services from being rendered to your patient. Please feel free to
provide us with your feedback, it is always welcomed and appreciated.
Urgent Information Request
Pending Order
Notification
Please note, we are in receipt of your request for home care services. We are
unfortunately UNABLE to process this request due to MISSING INFORMTION. Please send
us the information “checked” below so we can fulfill the patient order timely.
Thank you.
Patient Information Physician Information
□
Full Name □ Ordering Physician
□
Insurance Name and or ID# Name/Address/Phone
□
Height and Weight/Allergies □ Following Physician
□
Address/Phone □ PCP Information
□
Clear/Complete/Legible Order □ Other
DME Order Information
IV Pharmacy Information
□ Oxygen
LPM/Rate/Route/Saturation □ Drug Name/Dosage/Frequency
Level □ Route of Administration (Line, Sub-
Q, etc.).
□ CPAP/Bi-PAP Settings/O2 Bleed
In □ Substitution due to shortage or
Name Brand
□ CPM Settings
□ Ostomy/Foley Items and □ Has a first dose been given?
Quantities □ Diabetic Status
□ Wound Care Supplies
Additional Comments:
Please feel free to contact us at: 855-441-6900 / Fax-855-441-6941
Name
Extension
Email
IMPORTANT: This facsimile transmission contains confidential information, some or all of which may be protected health
information as defined by the federal Health Insurance Portability & Accountability Act (HIPAA) Privacy Rule. This
transmission is intended for the exclusive use of the individual or entity to whom it is addressed and may contain information
that is proprietary, privileged, confidential and/or exempt from disclosure under applicable law. If you are not the intended
recipient (or an employee or agent responsible for delivering this facsimile transmission to the intended recipient), you are
hereby notified that any disclosure, dissemination, distribution or copying of this information is strictly prohibited and may
be subject to legal restriction or sanction. Please notify the sender by telephone (number listed above) to arrange the
return or destruction of the information and all copies.
OneHome | Provider Manual 2020 Page 9
Services that require a
Letter of Medical Necessity
• Bariatric equipment (greater than 300 pounds)
• Bone growth stimulator
• Custom or specialized wheelchairs and scooters
• Neuromuscular stimulator
• Portable oxygen concentrator
• Ventilators covered by Medicare
• Wound Vac
• Home infusion
OneHome| Provider Manual 2020 Page 10Covered and Frequently Utilized Equipment
Quad Cane Standard Cane Walker Walker with Wheels
E0105 E0100 E0135 E0143
Alternating 3 Wheel Rollater 4 Wheel Rollator 3 in 1 Commode
Pressure Pad
E0143 E0143/E0156 E0165
Oxygen Portable Tanks (B and Liquid Oxygen with Egg Crate Mattress
Concentrator E’s) Portable
E1390 E0431 E0434/E0439
Standard Electric Wheelchair Scooter Heavy Duty W/C
Wheelchair
K0001 K0823 K0800 K0007
OneHome| Provider Manual 2020 Page 11K0003 E1039 K0005 E0114
LIGHT WEIGHT W/C Heavy Duty ULTRA LIGHT WEIGHT W/C CRUTCHES
Companion W/C
E1038 E0277 E0570 E2601
COMPANION W/C LOW AIR-LOSS MATTRESS NEBULIZER FOAM
CUSHION
E0110 E0630 E0635 E0260
FOREARM CRUTCHES HOYER LIFT (HYDAULIC) HOYER LIFT (ELECTRIC) SEMI-ELECTRIC
HOSPITAL BED
E2603 E0185 E0601 A7030
CPAP FULL FACE
GEL CUSHION GEL OVERLAY CPAP MASK
OneHome| Provider Manual 2020 Page 12CPAP NASAL MASK CPAP NASAL PILLOWS BI-PAP with Back-up BI-PAP
A7034 A7029 E0471 E0470
Humidifier E0562
CPAP Tubing A7037
CPAP Filter A7038
Water Chamber A4604
Tens Unit E0720
Nasal Cannula A4615
Heavy Duty Hospital Bed (42 in) E0303
OneHome | Provider Manual 2020 Page 13Schedule of Covered and Non-Covered Services
Durable Medical Equipment and Supplies Quick
Reference Guide
Some items do not fall strictly under the definition of DME, and are considered to
be “supplies”. This list contains both DME items and supplies.
Covered items may be subject to medical necessity review and contract
limitations. In addition, some items may require SLR (Second Level Review). Please
refer to the NCD and LCD for all covered and non-covered items. Please click on
www.cms.gov for NCD or LCD
Description Code Policy
Ambulation Aids
Canes E0100, Covered, if condition impairs
Crutches E0110, E0111, E0112, Covered
E0113, E0114, E0116,
Quad Cane E0105 Covered
Walkers E0130, E0135, E0140, Covered, if condition impairs
E0141, E0143, E0144, ambulation
E0147, E0148, E0149
Beds, Bed Equipment, Mattresses
Air Pressure Mattress E0197 Covered
Alternating Pressure Pads and E0181, E0182 Covered
Bed Cradles E0280 Covered
Bed Elevator E0315
Bed Pans E0275, E0276 Covered if patient is bed confined
Bed Side rails E0310 Covered, as part of an approved
hospital bed
OneHome | Provider Manual 2020 Page 14Beds, Bed Equipment, Mattresses continue....
Alternating Pressure Pad E0185 Covered
Hospital Beds, general E0250, E0251, E0255, Covered
E0256, E0260
Powered air flotation bed E0193 Covered
Synthetic sheepskin pad E0188, E0189 Covered
Mattress, inner spring or foam E0271 Covered as part of an approved
hospital bed
Gel pressure pad for mattress E0185 Covered
Powered Air-flotation Bed E0193 Covered
Powered Pressure-reducing mattress E0277 Covered
(alternating pressure or low air loss
Powered pressure reducing mattress, E0181, E0182 Covered
with pump
Trapeze Bar E0910 Covered
Water and Pressure Pads and E0185 Covered
Mattresses
Exercise Equipment and Supplies
Continuous Passive Motion (CPM) E0935 E0935RR Not covered (purchase) Covered
Device, Knee
Traction Equipment, standard E0830, E0840, E0849, following total knee arthroplasty
Covered
Lifts E0850, E0855, E0856, (rental)
Cushion Lift Power Seat E0860, E0870, E0629,
E0627, E0628, E0880, Covered (the mechanism only is
Hoyer Lift E2300,
E0630 E2301 covered)
Covered
Hydraulic Patient Lift E0630 Covered
Patient Lifts (i.e. Hoyer) E0630, E0635 Covered
Seat Lift Chair Mechanism E0627, E0628, E0629 Covered (the mechanism only is
Transfer Board or Device E0705 Covered
Respiratory Aids and Supplies
Bi-PAP E0470, E0471, E0472 Covered
Concentrator, Oxygen E1390, E1391, E1392 Covered
C-PAP E0601 Covered
Air Filter (CPAP/BIPAP) A7038, A7039 Covered
Nebulizer, w/compressor E0570 Covered
OneHome | Provider Manual 2020 Page 15Face Mask (oxygen) A4620 Covered
Flowmeter E0440 Covered
Masks (oxygen) A4620 Covered
Nebulizer E0570, E0575 Covered
Nebulizer (Mistogen) E0585 Covered
Nebulizer w/compressor (i.e. Devilbiss E0570 Covered
Pulmo-Aide)
Nebulizer, Portable E1399 Covered
Nebulizer, Ultrasonic only E0575 Covered
Oximeter E0445 Covered
Oxygen Humidifier E0550, E0555, E0560, Covered
E0561, E0562
Oxygen Portable Systems E0430, E0431, E0434, Covered
E0435
Oxygen Regulator E1353 Covered
Oxygen System E0424, E0425, E0439, Covered
E0440
Postural Drainage Board E0606 Covered
Suction Pump E0600 Covered
Ventilators E0450, E0460, E0461, Covered
E0463, E0464
Toilet Equipment
Bed Pan E0275, E0276 Covered, if bed confined
Standard Raised Toilet Seat E0244 Covered, 1 per member every year
Standard Tub Seat E0240, E0245 Covered, 1 per member every year
Wheelchairs/Chairs
3 to 4-wheel scooter and other similar E1230 Covered
scooters
Rollabout Chairs and Mobile Geriatric E1031 Covered, if to be used in lieu of a
Chair wheelchair
Wheelchairs, Power Operated Multiple Covered
OneHome | Provider Manual 2020 Page 16Wheelchairs, Standard Multiple Covered
Miscellaneous
Catheters and Supplies A4344, A4346, A4349, Covered
A4351, A4352, A4353,
A4354, A4355
Colostomy Bags and Supplies A4361, A4362, A4363, Covered
A4364, A4367, A4405,
A4406
Portable Infusion Pumps/Devices E0781, E0782, A4305, Covered
A4306
Mobile Infusion Pump E0781 Covered
Ambulatory/Stationary
Wound Vac E2402 Covered (Varies per health plan)
OneHome | Provider Manual 2020 Page 17Dear Physician,
Below you will find a listing of the HCPCS codes and items that are routinely utilized
by CPAP patients. Please ensure that you include all necessary item codes when
sending your orders to One Homecare Solutions. It is imperative that you submit
the authorization/request appropriately so therapy and equipment orders may
be fulfilled in their entirety.
CPAP
Item Description Qty
E0601 Cpap, Device 1
A7034 Cpap Nasal Mask 1
A7035 Cpap, Headgear/Each 1
A7037 Cpap Tubing, Long, each 1
A7038 Cpap Filter disposable/each 2
E1499 Cpap carrying case 1
A7027 Combination Oral/Nasal M 1
A7029 Repl Nasal Pillow Comb Mask 1
BiPap
Item Description Qty
E0470 Bipap S system 1
A7034 Bipap Nasal Mask 1
A7035 Bipap, Headgear/Each 1
A7037 Bipap Tubing, Long, each
1
A7038 Bipap Filter disposable/each 2
E1499 Bipap carrying case 1
OneHome | Provider Manual 2020 Page 18C-PAP/Bi-PAP Order Requirements
1) Settings (cm H2O) – Remember that the CPAP System requires only one
pressure level for therapy but the Bi-PAP System requires two different
pressure levels for therapy.
2) Sleep Study
3) Prescription/Physician orders
4) If a Humidifier is needed the script must identify if heated or non-heated
• HCPC code for Non-heated is E0561
• HCPC code for Heated humidifier E0562
6) Chin Strap (Optional) HCPC code A7036
7) If a full face mask is needed HCPC code is A7030
8) The HCPCS for a Bi-PAP ST with Back up Rate is E0471
9) When ordering supplies must include the code for replacement of water
chamber. A7046 Replacement water chamber for positive airway
device.
10) Rx should suggest if nasal mask or nasal pillows.
11) Rx should state “bleed in to oxygen” when necessary.
OneHome | Provider Manual 2020 Page 19SNF Infusion Order
NECESSARY INFORMATION NEEDED TO PROCESS ANY NEW ORDER FOR SNF PATIENTS.
SNF INFORMATION:
Nursing Home Facility: Contact Nurse:
Phone # Ext. Floor Fax:
PATIENT INFORMATION:
Patient Name: DOB: Room #:
ID #: Insurance:
Relative Name: Phone#: Relation:
MEDICAL INFORMATION:
Height: Weight: Diabetic Status (Type):
Allergies: Is Ordering Physician Aware of Allergy:
(If patient is allergic to ordered medication or its drug class)
First Dose Given (Y/N): When:
Activity: Relevant Medical History:
IV Access Type: Diagnosis:
ORDERED MEDICATION (s):
Drug: Dose: Route:
Frequency: Next Dose Due:
Drug: Dose: Route:
Frequency: Next Dose Due:
VERBAL ORDER TAKEN BY: RN / LPN (READ BACK)
***Must be signed***
Name of Ordering MD: Phone #
***Attached to this page, PLEASE FAX COPIES OF THE MDs ORDERS, LABS, MAR and
FACE SHEET to 855- 441-6941. Thank you for your cooperation. ***
a
OneHome | Provider Manual 2020 Page 20OXYGEN (Gas) All patients get a Concentrator which plugs into an outlet in
Need script or orders to state: the home. These patients also get tanks to take with them
Concentrator and move about in the home. Some patents require a
LPM (liters per minute) Portable Oxygen Concentrator for travel and they are small
and need Medical Director Approval/Second Level Review,
Nasal Cannula (N/C) Clinical Documentation and authorization.
Mask Saturation needs to be below 88%
Humidifier (Second Level Review if saturation not below 88%).
Frequency( PRN/Continuous/At
night)
Liquid Oxygen They are stationary units called RESERVIORS and get filled
Different than gas (concentrator weekly or depending on patients use. With the stationary
and tanks) and needs a Reservoir comes a portable, usually an H300/Helios or
prescription specifying LIQUID Marathon. Needs Medical Necessity Documentation
OXYGEN. and Review.
Foley Supplies
Catheters (14 FR-22FR) Used for patients who are unable to pass urine on their
own. Need to be catheterized, either continuously
Bags / Leg Bags (foley) or sporadically/intermittent (Self cath/Straight
Lubricant cath).
Gloves, etc.
CPAP and BiPAP Continuous Positive CPAP’s and BiPAP’s used for those with Sleep Apnea. This is
Airway Pressure/Bi-level positive when patients stop breathing in their sleep. It causes unhealthy,
airway pressure) disruptive sleep patterns and can even cause death. The
CPAP Mask: Small, Medium, machine forces air through the patients airway at all times to
Large (Masks are used for ensure proper breathing, and better sleep.
months at a time). Medicare Doctor’s orders must include settings, pressure, Script with
limitations, 1 every 3 months. Diagnosis, and Sleep Study.
Need type. IF OXYGEN BLEED IN: LPM a must or O2%.
Headgear, need size
Patients are usually sent for a sleep study to assess their specific
(Nasal Pillows/Full Mask) needs. We do need a copy of the sleep study.
Visit to be performed by a Respiratory We also monitor their usage of the machine via “SD Card” in
Therapist. RT sets up and instructs on the machine which is downloadable and sent to MD upon
the machine and “FITS” the patient request/order.
properly for the mask and necessary
supplies.
a OneHome | Provider Manual 2020 Page 21Tracheostomy Care Used for patients who have had a tracheostomy/TRACH.
Adult/Pediatric/Neonatal
A tracheostomy is the surgical construction of an opening
Suction Catheters (6FR – 16FR)
in the trachea, usually by making an incision in the front of
Trach Care Kits
the neck, for the insertion of a catheter or tube to facilitate
Trach Tube Holders
Trach Mask breathing.
Yankauers
50 psi Compressor/Humidity
Large Nebulizer Bottles
Spare Trach Tube/ Inner
Cannulas
O2 Adapter/O2 Connection
Tubing
Suction Pump: Adult/Pediatric Used for those with trachs or vent patients. Used to clear the
Suction Tubing airway. These are very important and are to be treated with
urgency. Breathing can be blocked if patient is not suctioned.
Suction Catheters
There are Portable and Stationary Units.
Suction Canisters
Apnea Monitor Used on newborns: Sometimes babies do not breathe the way
Need Rx they are supposed to an experience periods of “Apnea” where
they stop breathing. This machine alarms when the baby
Need settings experiences the periods of Apnea so the parents can check
the baby, perform CPR or call 911 if necessary.
Belt/Electrodes/Gel Delivery to be made to the hospital so RT can train
Electrodes/PT Cable/Charger and instruct parents.
Respiratory Therapist Need parents to have had a CPR class prior to
NECESSARY discharge.
Nebulizers: Adult/Pediatric Used frequently for patients who need breathing treatments
either chronic or acute. Bronchitis, Asthma, etc. Need same
Neb Kit/Mask day delivery. Also in our consignment closets for easy patient
access. (See consignment process/program info. Pg. 18-19)
Diabetic/Insulin Pumps and Need to know items type and quantities needed. (i.e.
Supplies Quick Set – MMTxxx, Reservoir type and quantities).
Continuous Passive Motion Utilized After lower extremity surgeries.
Device (CPM) Need script to state settings. (i.e. 90 degrees flexion and
50 degrees knee extension. -60, -20
Power Operated Vehicles Need prescriptions, physician face to face, CMN,
Physical Therapy Assessment, Measurements, and Health
(POV) /Custom Equipment
Plan Approval. Submission Timeframe Critical
a
OneHome | Provider Manual 2020 Page 22Ostomy Guide/Standard Ostomy Items with
Medicare Allowable
Please note that the Medicare allowable is indicated below. Requests above the allowable
require clinical documentation.
HCPC
Supplies ITEM #'S/REF Allowable for month
Pouches for a 2-Piece system
Drainable 12 Inch A5063 20
Drainable 10 Inch A5063 20
Drainable 6 Inch A5063 20
Closed with Filter A5054 60
Closed No Filter A5054 60
Urostomy with flip flow valve A5073 20
Other:
Wafer for 2-Piece System
Standard wear with flexible tape collar A4414 20
Standard wear without tape collar A4414 20
Extended wear with flexible tape collar A4414 20
Extended wear without flexible tape collar A4414 20
Extended wear with convexity A4414 20
Other:
1 Piece system
1 Piece drainable pouch 12 inch A5061 20
1 Piece drainable 6 inch A5061 20
1 Piece closed pouch with filter A5051 60
Stoma Cap A5055 60
HCPC
Misc Supplies ITEM #'S/REF Allowable for month
Paste 2 oz tube A4364 4 oz per month
Conformable Seal A4385 20 per month
Convex Insert A5093 10 per month
Deodarant 8oz A4395 16 oz per month
Belt A4367 1 per month
Skin barrier wipes A5120 100 per month
Adhesive remover A4456 100 per month
Bedside drain bag A4357 2 per month
Tape, waterproof or non-waterproof A4450
Gauze, non-sterile, urostomy only A6402
Foley Cathedar A4338 2 per month
Other:
a
OneHome | Provider Manual 2020 Page 23Urology Supply Guide
Please note that the Medicare allowable is indicated below. If patient requires additional
supplies more than Medicare allowable, clinical documentation is required. Please attach to
order.
Allowable
HCPC per Quantity
Urology Supplies Requested Codes Month Needed
28mm 31mm 33mm 35mm
Male External Cath Self Adhesive 40mm A4349 35
Intermittent Uretheral Catheter Up to
(Each) Red Rub Plastic FR. A4351 200
Up to
Self Cath (Changes per day ) FR. A4353 200
Coude Tip Cath (Changes per day Up to
) FR. A4352 200
Foley Catheter Silicone Coated
(Each) 5 cc 30 cc FR. A4338 2
Foley Insertion Tray (Each) 10 cc 30 cc A4310 2
Lubricant A4320 2
Bedside Drainage Bag 2000cc
(Each) A4357 2
Leg Bag (each) Sm Med Lg A4358 2
Irrigation Tray Kit A4320 2
Adhesive Remover Wipes (Box) A4456 2
Skin Prep Wipes (Box) A5120 2
Other Supplies Requested
a
OneHome | Provider Manual 2020 Page 24AGENCY NAME:
DATE OF REQUEST:
Member MUST be receiving Skilled Services in Home in order to receive Wound Care Supplies
WOUNDCARE SUPPLY FORM (Part 1 or 2)
MEMBER’S NAME:
HEALTH PLAN: MEMBER ID#:
NAME OF PCP (PRIMARY CARE PHYSICIAN)
MEMBER’S ADDRESS:
CITY: STATE: ZIP CODE:
COUNTY:
PATIENT’S TELEPHONE NUMBER:
MOST RECENT PRIMARY PHYSICIAN APPOINTMENT FOR WOUND was with DATE:
MOST RECENT HOME HEALTH VIST FOR WOUND was with DATE:
MOST RECENT WOUND CARE SPECIALIST VISIT was with
WOUND CARE DESCRIPTION(S) Frequency of care: (circle one) QD 2xWeek Every Week
WOUND #1 WOUND #2 WOUND #3
LOCATION:
MEASUREMENTS:
DESCRIPTION:
STAGE:
ADDITONAL INFO:
STANDARD WOUND CARE SUPPLIES
✓ ITEM/HCPC U/M ✓ ITEM U/M
ABD Pads 5x9, 8x10 A6252 Bx/Ea Vaseline Gauze 3x9 A6223 Each
Non-adh Pads (Telfa) 3x4 A6402 Each Micropore Tape 2” A4452 Each
Paper tape 1”, 2”, 3” Each Each Transparent Film 2x3 100/BX , 4x4(50/bx) Ea/bx
A4450 A6257(58)
0.9% Normal Saline 100ml Each Hydrocolloid 4x4, 6x6 OTHER (5/bx) A6234 Ea/BX
A4217 (35)
Gauze Roll Sterile 4x ½” A6446 Each Coban 3", 4" A6454 (53) Each
Elastic Bandage 2”, 3”, 4” A6448 Each Cotton-tip Applicators 6”-Str 2/Pkg Each
*******for Packing Only******* A4649
Gauze Non Sterile 4x4 A6416 Loaf Dressing retention tape (Mefix) 2”, 4”A4452 Each
Gauze St 4x ,2x2 A6402 BX/E Foam Dressing 4x4, 6X6 Other (10/BX)A6209 Each
A (10) 10/BX
Conforming bandage 4” A6447 Each Kerlix/Bandage Roll A6449
For Specialty Wound Care Supplies, Please see Page 2
WOUND CARE ORDER FORM V150330 © 2020 One HomeCare Solutions, LLC Page 1 of 2
OneHome | Provider ManualAGENCY NAME:
DATE OF REQUEST:
Member MUST be receiving Skilled Services in Home in order to receive Wound Care Supplies
WOUNDCARE SUPPLY FORM (Part 2 of 2)
SPECIALTY WOUND CARE SUPPLIES
Disclaimer: These items are considered specialty items, and should only be used under the supervision of a clinician trained in their use. One Homecare
Solutions assumes no liability for their use without clinical management skilled in wound care
✓ ITEM/HCPC U/M ✓ ITEM U/M
Silver Hydrogel A6248 1oz Each Silver dressing : Algicell Ag/Aquacel Ag A6197 10/bo
x Each
Hydrocolloid 4x4, 6x6 OTHER Ea/BX Calcium Alginate 2X2, 4X4, ROPE A6197 Ea/bx
(5/bx) A6234 (35)
Collagen Dressing A6201 Collagen Each Transparent Film 2x3 100/BX , 4x4(50/bx) Ea/bx
Dressing W/Silver A6214 A6257(58)
Hydrogel Dressing A6231 Each Dressing retention tape (Mefix) 2”, 4”A4452 Ea/BX
Hydrogel 25 grams (1oz) A6248 Each Adaptic A6222 Each
Xeroform A6223 E
Packing strips-plain ¼” ½” 1” Each Foam Dressing 4x4, 6X6 Other (10/BX)A6209 Each
A6407 (10) 10/B
Packing Strips-Iodoform ¼” ½” 1” X
A6266
Foam Adh (square)2X2, 4X4, Ea/BX Foam Adh(oval) 2X2, 4X4, Other Ea/BX
Other A6212(13) A6212 (13)
NAME OF PERSON COMPLETING FORM (PLEASE PRINT)
DATE PHONE #
IF FORM COMPLETED BY MEMBER (Specialty Wound Care Supplies):
I understand that I am receiving these specialty wound care supplies for my personal use and by my
request, and I further understand their incorrect use, or use outside of oversight by trained clinical
wound care professionals is not recommended, nor sanctioned by One Home Care Solutions, LLC.
NAME (PRINTED)_ SIGNATURE DATE
SERVICES WILL NOT BE APPROVED UNLESS ALL APPLICABLE DOCUMENTATION IS ATTACHED PER CMS
GUIDELINES; CHAPTER 7, HOME HEALTH MANUAL. # PAGES ATTACHED:
WOUND CARE ORDER FORM V150330 © 2020 One HomeCare Solutions, LLC Page 2 of 2
OneHome | Provider ManualPhysician Oxygen Order
Please fax with Demographics to 1-855-441-6941
Date:
Patient Name Insurance ID# Date
of Birth: Insurance Name:
Oxygen Type: GAS Liquid (Please circle one)
Liter Flow per Minute: LPM Continuous PRN (Please Check One)
Route: Nasal Cannula Simple mask Other
Qualifying Diagnosis: Last Patient office visit date:
Hours of use: Continuous With exertion
During hours of sleep Bleed into CPAP/Bi-PAP
Other
Delivery Device: Concentrator
Portable cylinders
Conserving device Other :
Oxygen Saturation or PO2 results: % Date of saturation test:
X
Physician Signature Physician Name
Please note, prescription is valid for one year of signature unless orders change.
Oxygen Discontinuation Order
Patient Name: Date:
Please discontinue and pick up Oxygen.
X
Physician Signature Physician Name
OneHome | Provider ManualO2 Desaturation Report
Date:
Patient Name: Insurance ID#:
Date of Birth: Insurance Name:
Type □ Hallway □ Arm Exercise □ Other (Please Check One)
TIME (min) SaO2 (%) HR (bpm)
REST
1 MIN
2 MIN
3 MIN
4 MIN
5 MIN
FIO2
RECOVERY Approximate feet walked
1 MIN
2 MIN
3 MIN
Interpretation/Results:
If additional documentation attached, please provide member demographics & date on each and number below.
OHS O2 Desat Form v 150911 © 2020 One Homecare Solutions, LLC Pages Attached
OneHome | Provider ManualPORTABLE OXYGEN CONCENTRATOR FOR TRAVEL REQUEST
PATIENT’S NAME:
HEALTH PLAN: MEMBER ID#: LOB:
NAME OF PCP (PRIMARY CARE PHYSICIAN)
PATIENT’S ADDRESS:
CITY: STATE: ZIP CODE:
COUNTY:
PATIENT’S TELEPHONE NUMBER:
MOST RECENT SPECIALTY PHYSICIAN APPOINTMENT FOR O2 Rx Review was with
DATE:
MOST RECENT PRIMARY PHYSICIAN APPOINTMENT FOR O2 Rx Review was with
DATE:
For consideration of TRAVEL POC, the following minimum information must be provided:
Current ambulation status: □ Scooter/electric wheelchair □ Manual wheelchair □ walker/cane
Physical restrictions/Pertinent Medical Conditions (describe):
Current O2 therapy Status: □ Liquid □ Gas
Settings: □ Pulse □ Continuous LPM □ O2 Adjunct Home (conserver, etc)
Hours/day used for mobility
Current Use of □ B tanks □ E tanks □ CPAP/BiPAP □ Other :
Efficacy (how well is patient with current home O2 therapy)
Dates of Travel
Mode of Travel □ Car □ Plane □ Train □ Ship □ Other:
Location(s) of travel □ Domestic □ International
POC settings: □ Pulse □ Continuous LPM % Saturation
Approval and provision is based on provider attestation that the patient is able to manage the physical requirements of
the system, that medical record documentation exists supporting that O2 mobility and transportability is medically
necessary and that CMS guidelines for the medical necessity of the POC have been consistently and appropriately
followed
Ordering Physician Signature Date
Note: Out of Service Area and International Travel may require patient deposit on devices and disclaimers for repair and
service and cost of return
TRAVEL POC v150513 ©2020 One Homecare Solutions, LLC
OneHome | Provider ManualPermanent Portable Oxygen Request
PATIENT’S NAME: Date of Referral:
HEALTH PLAN: MEMBER ID#: LOB:
NAME OF PCP (PRIMARY CARE PHYSICIAN)
PCP Contact Information – Phone: Point of Contact:
PATIENT’S ADDRESS:
CITY: STATE: ZIP CODE:
COUNTY:
PATIENT’S TELEPHONE NUMBER:
MOST RECENT SPECIALTY PHYSICIAN APPOINTMENT FOR O2 Qualifying Condition
was with on (date)
MOST RECENT PRIMARY PHYSICIAN APPOINTMENT FOR O 2 Qualifying Condition was on (date)
Note: Review of a request for a PERMANENT POC is a non-medical necessity determination beyond meeting
CMS guidelines for in home oxygen and adjunct home portable oxygen. Submission does not guarantee
provision and requires, at a minimum, documentation of (Complete ALL □):
□ Diagnoses: , , ,
□ Oxygen saturations at rest and with mobility (i.e. 6 min test)-form available on request
At Rest After Mobility (time) ( _) FI02 = □ Room Air □ % O2
□ Estimated in home hours/day , and days/month needed for portable use
□ Use/Failure of portable O2 cylinder (3.5# B tank) in home? □Y □N Rationale for inadequacy for
mobile use in home: (attach documentation)
□ Use/Failure of wheeled O2 cylinder (8# E tank) in home? □Y □N Rationale for inadequacy for
mobile use in home: (attach documentation)
□ Use/Failure of liquid O2 in home (if using home Liquid O2)? □Y □N Rationale for inadequacy for
mobile use in home: (attach documentation)
□ Current ambulation status: □ Scooter/power wheelchair □ standard wheelchair □walker □cane
□ Physical restrictions, home conditions, other (describe)
□ Current Stationary O2: □ Pulse □ Continuous LPM % Saturation □ Liquid □ Gaseous
□ O2 Adjuncts □ CPAP □ Nebulizer □ Other □ Hours/day used
□ Recommended POC settings: □ Pulse □ Continuous LPM % Saturation
Approval and provision is based on provider attestation that the patient is able to manage the
physical requirements of the system, that medical record documentation exists supporting that
mobility/transportability is medically necessary and that CMS guidelines for the medical necessity of
the portable oxygen in the home have been consistently and appropriately followed.
Ordering Physician _Signature Date
□ Supporting Documentation Attached Number of Pages Attached_
Permanent Portable Oxygen Request v150803 ©2020 One Homecare Solutions, LLC
OneHome| Provider ManualCPAP/BiPAP Order/VPAP Authorization Form
PATIENT’S NAME: Date of Referral:
HEALTH PLAN: MEMBER ID#: DOB:
NAME OF PCP (PRIMARY CARE PHYSICIAN)
PCP Contact Information – Phone: Point of Contact:
PATIENT’S ADDRESS:
CITY: STATE: ZIP CODE:
COUNTY:
PATIENT’S TELEPHONE NUMBER:
ICD/Diagnosis: Length of Need:
Device (s) (HCPCS) requested: (Check all that apply)
□ E0470 BiPAP w/o B/U rate □ E0471 BiPAP S/T w/ B/U rate
□ E0562 Hum Heated □ E0601 CPAP/Auto CPAP Device
□ A7034 Nasal Pillows □ A7030 Full Face Mask
□ A7034 Nasal Mask □ A7036 Chin Strap
□ E0470 BiPAP AUTO / VPAP AUTO
Settings:
CPAP @ cmH20 Auto CPAP @ Min - Max_cmH20
BiPAP @ I/ E cmH20 BiPAP S/T @ I/ E cmH20 WITH BPM
O2 BLEED IN @ LPM VPAP AUTO (RESMED) @ IPAP MAX, EPAP MIN
PRESSURE SUPPORT
BiPAP AUTO (RESPIRONICS) @ IPAP MAX, IPAP MIN
PS MAX, PS MIN
Physician Signature Date:
Please note: prescription is valid for one year of signature unless orders change
OHS CPAP BPAP FORM VPAP FORM V170109 Copyright 2020 OneHome, LLC pages
AttachedPMD/POV/PWC Referral
PATIENT’S NAME: Date of Referral:
HEALTH PLAN: MEMBER ID#: LOB:
NAME OF PCP (PRIMARY CARE PHYSICIAN)
PCP Contact Information – Phone: Point of Contact:
PATIENT’S ADDRESS:
CITY: STATE: ZIP CODE:
COUNTY:
PATIENT’S TELEPHONE NUMBER:
MOST RECENT SPECIALTY PHYSICIAN APPOINTMENT FOR Qualifying Condition was with
on (date)
MOST RECENT PRIMARY PHYSICIAN APPOINTMENT FOR Qualifying Condition was on (date)
For consideration of authorization for a power mobility device (PMD) includes power operated
vehicles (POVs, aka scooters) and power wheelchairs (PWCs, aka motorized wheelchair)
Letter of Medical Necessity (LOMN) – Summary of request, rationale and supporting information
Questionnaires with YES, NO responses will require documentation and full description of all pertinent qualifying
answers, and are not acceptable as a LOMN
Supporting documentation (Face to Face encounter with detailed physical examination and/or Physical
Therapy Evaluation) to include ALL the following at a minimum (attach physical exam for all qualifying):
Nature of request □ POV □ PWC Current PMD Use □ POV □ PWC # Years
Current Qualifying Medical Conditions: , _, _,
Limitations to upper extremity strength and ROM
Lower extremity limitations
Ambulatory status □Wheelchair □POV □Walker □Cane □ Other
Pertinent mobility and ADL issues
Balance and stability concerns
Pertinent global health concerns
Ability to manage the physical requirements of the POV □ Y □ N
Special or unique considerations
Approval and provision is based on provider attestation that the patient is physically unable to
manage the mobility requirements of a manual wheelchair, that UE and LE mobility restrictions are
supported by medical record documentation, PMD is medically necessary, and that CMS guidelines
for the medical necessity of the PMD have been applied, periodically reviewed and are documented
consistently.
Ordering Physician Signature Date
□ Supporting Documentation Attached Number of Pages
PMD/POV/PWC Referral v150415 ©2020 OneHome, LLCYou can also read