Personalised Medicine in European Hospitals
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

www.pwc.com/es Personalised Medicine in European Hospitals

PwC and the European Hospital and Healthcare Federation (HOPE)
have joined forces to identify key elements in the development of Participants
personalised medicine in European hospitals. This collaboration
will help determine of the current state and the desired future state PwC and HOPE would like to express
of personalised medicine practices within European hospitals, and sincere gratitude to the European
hospitals that contributed to the
will thoughtfully facilitate the creation of a culture of customised
development of this paper with their
healthcare. knowledge, experience and time.
Personalised medicine can be defined as products and services that Special thanks go to the following
leverage the science of genomics and proteomics (directly or contributors:
indirectly) and capitalise on the trends towards wellness and
consumerism to enable tailored approaches to prevention and care. • R
aimon Belenes,
Chief Executive Officer, Hospital
Clinic de Barcelona (Spain)
The dawn of personalised medicine brings not only new advances
to our healthcare system today, but also key challenges. This new • Alain Bonnin,
Professor of Medical Parasitology and
science has led many participants in the healthcare industry, such
Mycology; Director Parasitology
as providers, to consider how best to adapt to these challenges and
Mycology Laboratory; Director
foster a consumer-focused culture. Hospitals have a clear Biological Resource Center Ferdinand
opportunity to adapt to the new healthcare paradigm and provide Cabanne – University Hospital of
services that are targeted to the individual patient. It is important Dijon (France)
to recognise, however, that different hospitals operate and require • J ulia S. Johansen,
different models. Just as doctors will no longer be able to apply the Professor, Senior Consultant, DMSc at
same forms of treatment to patients, hospitals will not be able to Herlev Hospital/Copenhagen
apply the same approach to addressing the challenges brought on University Hospital at Herlev
by personalised medicine. Hospitals and providers have many (Denmark)
options for how they respond to the changing market. And as • J orma Penttinen,
evidenced in the interviews we completed with several European Medical Director, Kuopio University
hospitals, personalised medicine can be designed and implemented Hospital (Finland)
into a hospital model in a variety of ways. • B
orut Peterlin,
Head of Clinical Institute of Medical
Many European hospitals have already begun to define what Genetics, University Medical Centre
personalised medicine means to their hospital and have developed Ljubljana (Slovenia)
their strategies for implementation. And as hospitals solidify their • G
yörgy Pfliegler,
definition and vision of personalised medicine as well as their Head of Division of Rare Diseases
approach for implementation to create a culture of customised Institute of Medicine, Medical and
Health Science Center University of
healthcare, leading practices will continue to emerge.
Debrecen (Hungary)
2 Personalised Medicine in European Hospitals
Table of contents
The impact of personalised medicine today 4
Part I. Personalised Medicine in European Hospitals
1. General overview of personalised medicine 7
2. The pressure to be personalised – Key trends
that have changed the healthcare paradigm 8
3. Next steps for hospitals and providers 11
4. Conclusions 15
Part II. Hospitals in focus
List of Participating Hospitals 18
Herlev Hospital / Copenhagen University Hospital at Herlev,
Denmark 19
Kuopio University Hospital, Finland 25
University Hospital of Dijon, France 29
Medical and Health Science Center University of Debrecen,
Hungary 34
University Medical Centre Ljubljana (UMCL), Slovenia 38
Hospital Clinic de Barcelona, Spain 42
The impact of personalised medicine tomorrow 46
Personalised Medicine in European Hospitals 3
The impact of
personalised medicine today
Personalised medicine aims to provide •G enetic screening is widely used
the timely, precise, personalised for treatment in cancer patients.
diagnosis and treatment of patients, Cardiology, neurology, radiology,
with a particular emphasis on wellness and the treatment of diabetes are
and disease prevention. Although among the key disciplines that
personalised medicine has already benefit from the genetics field.
been introduced into practice, it is still Advances in genomic and proteomic
in its early stages of implementation in science have led to more cost-
the European healthcare market. This efficient discoveries, with doctors
report outlines the move towards more inclined to use targeted
personalised medicine in six European treatments.
hospitals — located in Denmark, •S tem cell programs and
Finland, France, Hungary, Slovenia treatments are still relatively new.
and Spain — compares the path each is Although there are several programs
taking, and discusses the following underway, most of the hospitals
commonalities: surveyed are not yet applying this
field in the clinical setting.
• Most of the European hospitals • Telemedicine services are not yet
are focused on initiatives related fully deployed. Devices for
to diagnostics and therapeutics. monitoring chronic diseases are
The European landscape is working currently being developed and
in several ways to develop new implemented in various clinical
imaging technology and genetic services, such as cardiology and
tools, such as biomarkers and neurology.
biochips.
4 Personalised Medicine in European Hospitals
• Only a few European hospitals the life science and medical sectors is
focus on nutrition and physical essential in fostering innovation in
activities to encourage wellness the field of personalised medicine.
and improve the treatment of •T
he main barriers for the
patients; most do not tackle implementation of personalised
prevention as part of their medicine within the European
approach. The reason could be that hospital environment are: lack of
other factors, such as primary care research funding, lack of strong
providers and public health media scientific evidence in some fields,
campaigns, already encourage lack of knowledge among doctors,
patients to monitor their own health and lack of a clear reimbursement
status and maintain a healthier system for related services.
lifestyle.
• Developing relationships or Our study revealed that, although
affiliations with other sector Europe is starting the paradigm shift
organisations is a usual practice towards personalised medicine, many
within the European hospital barriers still need to be addressed. To
market. Public and private hospitals keep the process on track, healthcare
(EU and US hospitals), public entities professionals and policy makers must
such as the National Health Service aim to ensure that personalised
(NHS) and laboratories, universities medicine contributes to the
and biotech and pharmaceutical improvement of population health with
companies, are among the main clear and robust evidence of patient
partners to undergo personalised value, and they must remember that the
medicine projects. Cooperation shift towards personalised medicine is a
between the many stakeholders in process rather than an endpoint.
Personalised Medicine in European Hospitals 5
Part I. Personalised Medicine in European Hospitals

1. General overview of
personalised medicine
develop in the future and how the
person will respond to a given
treatment, enabling the development
of a tailored health strategy.
• I t is preventive; it facilitates a
proactive approach to health and
medicine, which shifts the focus from
illness to wellness.
Personalised medicine is broadly • I t is participatory; it empowers
defined by PwC, as “products and patients to make informed choices
services that leverage the science of and take responsibility for their own
genomics and proteomics (directly or health1”.
indirectly) and capitalise on the trends
towards wellness and consumerism to The human genome project and
enable tailored approaches to dwindling costs in genomic and
prevention and care”. This definition proteomic sequencing is creating this
encompasses everything from high- “new science” that focuses on the
tech diagnostics to low-tech foods, consumer. New science is no longer a
technologies that enable storage, and concept of the future; it is here today.
analysis and linking of patient and Key trends over the past decade have
scientific data. challenged the healthcare
environment, payers, pharmaceutical
Personalised medicine or the “new and life sciences companies, and
science”, also referred to as “P4 providers to become more consumer
Medicine” by Dr. Leroy Hood, co- focused in their own right. Providers
founder of the Institute for Systems have their own unique set of challenges
Biology, encompasses the following that will need to be addressed in order
principles: to successfully create a culture of
personalised healthcare for the patient.
• “It is personalised; it is based on an Correspondingly, it is important to
understanding of how genetic understand the key trends that have
variation drives individual pushed healthcare to be more
treatment. personalised, the challenges that
• It is predictive; it is able to identify providers face, and how hospitals are
what conditions a person might adapting to this new environment.
1
PwC, “The new science of personalized medicine: Translating the promise into practice”, 2009.
Personalised Medicine in European Hospitals 7
2. The pressure to be personalised – Key trends
that have changed the healthcare paradigm
The shift in the healthcare paradigm to model. These trends can be grouped into personalised treatment regimen and
personalised medicine did not happen four categories: cost-efficient approach to healthcare.
overnight. Over the last decade, By identifying the optimal point of
advances in genomics and technology as • Genetic trends intervention for treatment, healthcare
well as the patients´ inclination towards • Patient trends providers can improve quality of care
care that is consumer focused have • Technology trends and reduce costs by effectively timing
contributed to this development. The • Wellness trends treatment intervention and eliminating
dawn of personalised medicine brings waste from insufficient or excessive
not only new advances to our healthcare Genetic trends — Advances in treatment regimens.
system, but also distinct challenges. genomic and proteomic sequencing As genome sequencing costs decline,
This new science has led many players have resulted in cost-efficient doctors and patients alike are more
in the healthcare industry, such as discoveries that are bending the inclined to seek treatments that are
providers, to consider how best to adapt cost curve targeted to the patient’s illness. Today,
to these challenges and foster a Advances in genomic and proteomic genome sequencing costs are
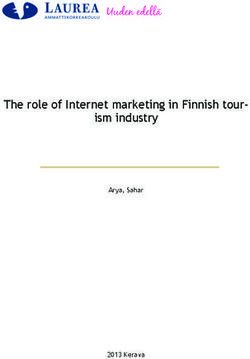
consumer-focused culture. But before sequencing over the past decade have approximately $20,000 per genome, a
the industry can address these led to the development of “targeted” stark contrast to 2001 sequencing costs
challenges, it must first understand the diagnostics and therapeutics that of almost $100,000,000 per genome (see
trends that have pushed healthcare to leverage knowledge of an individual’s Figure 1).
evolve towards a more personalised genetic makeup to create a more
Figure 1:
Cost per genome from the National Human Genome Research Institute
$ 100.000.000
$ 10.000.000
$ 1.000.000
$ 100.000
$ 10.000
$ 1.000
01 02 0 3 0 4 0 4 0 5 0 5 0 6 06 07 t- 07 08 08 09 - 09 0 0
p- p- t- r- t- r- t- r- t- pr- r- ct- r- l r-1 ct-1
se se oc ap oc ap oc ap oc a oc ap o ap ju ap o
Source: Wetterstrand KA. DNA Sequencing Costs: Data from the NHGRI Large-Scale Genome Sequencing Program
available at: www.genome.gov/sequencingcosts. Accessed 19 April 2011.
8 Personalised Medicine in European Hospitals
Patient trends — Accessibility advice available online and more A few key examples of recent progress
creates consumer-focused patients/consumers becoming well made in healthcare technology in
healthcare educated on health management, Europe are described in Figure 3.
Patient empowerment is part of a individuals will expect one-on-one
broader trend towards consumer- customised service from physicians.
focused healthcare, enabled by easy
access to health information that was
previously available only to medical Technology trends — Connectivity
professionals.2 Not surprisingly, patients fosters treatments in non-
are looking to various online resources traditional settings and
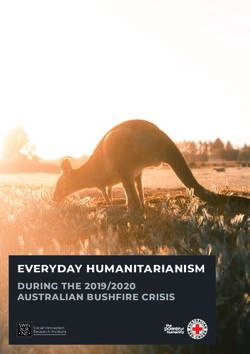
for medical advice or diagnosis. In fact, encourages the “anytime,
global consumers surveyed online by anywhere” mind set
PwC said their top information source Connectivity allows for customised
on health was online websites (See solutions both inside and outside the
Figure 2).3 Social networking sites home. Developments such as telehealth,
ranked eighth in this survey. Physicians home health, and web applications
and providers are no longer viewed as enable a new paradigm of personalised
the primary source for medical care outside the confines of a doctor’s
information as online resources create office or clinic. Consumers are becoming
educated patients that can now form empowered to predict their own medical
their own opinion on how to handle risks, detect diseases, and track/manage
their health. Online websites allow their health status overall through
patients to feel as if they are in control of genetic testing products for in-home use
their health and that advice is targeted — furthering the concept of health
to their needs. With more medical management “anytime or anywhere”.
Figure 2:
Where do you go to find information to make decisions about your healthcare? (Select
all that apply)
Health website 48%
Doctors 43%
Through friends or family 30%
Magazines or newspapers 27%
TV or radio 24%
The hospital 22%
Government 21%
Social networking websites 17%
Community services 14%
Health clubs (e.g., gymnastic, yoga) 8%
Schools 7%
0% 10% 20% 30% 40% 50% 60%
Source: PwC’s Health Research Institute Global Consumer Survey. HealthCast 2010.
2
PwC Health Research Institute, “Health Cast: The customization of diagnosis, care and cure”, March 2010.
3
PwC’s Health Research Institute Global Consumer Survey in “HealthCast: The customization of diagnosis, care and cure”, March 2010.
Personalised Medicine in European Hospitals 9
Figure 3:
Examples of care-anywhere networks through technology
Territory Experience
The government is making a progressive attempt to mobilise care from the hospital to homes equipped with electronic monitoring
France
devices.
Leading the trend towards home automation, where sensors, central locking systems, radio frequency identification (RFID), ringing-
Netherlands
mats and cameras are used to monitor patients.
P’ASMA is a web-based application that helps patients manage their asthma. The physician registers the patient’s clinical data, asthma
Portugal control data and a specific treatment plan. At home, the patient downloads his or her data and receives immediate graphic and written
feedback based on the defined treatment plan. The system also delivers automatic messages and alerts online to each patient.
Capio Health Care has a daily dialogue with its psychiatric patients via email, for example, by using Montgomery-Åsberg Depression
Sweden Rating Scale (MADRS) or comprehensive psychopathological rating scale (CPRS). And for orthopaedic rehabilitation patients, Capio
sends their patients animated training programs via email.
Toumaz Technology is conducting a clinical trial with the Imperial College Healthcare NHS Trust to test a digital “patch”, a disposable
United
device with a wireless sensor that sticks to a patient’s chest and can monitor, in real time, vital signs such as temperature, heart rate
Kingdom
and respiration.
Source: PwC Health Research Institute, “Health Cast: The customization of diagnosis, care and cure”, March 2010.
Wellness trends — With greater allow them to feel greater ownership in higher quality of service. Patients are
focus on the consumer, healthcare the responsibility for their health. researching more on the Internet for
is trending from diagnostics to information on healthcare and
wellness Today’s trend towards consumerism healthcare coverage. As Figure 4 shows,
Personalised medicine encourages attempts to inject something that’s been the share of online health information
patients to be more active in the decision missing from health benefits — a seekers has doubled since 2004.
making responsibilities of managing their consumer who cares more about cost
health, and therefore enables a consumer- and quality. By providing financial
focused market. Today, patients can incentives and information to patients,
search online for symptoms they are the healthcare system can encourage
experiencing; find individuals who may them to assume a greater role in
share the same disease state; monitor managing their own healthcare and the
their health within the confines of their associated costs, with the intention of
own home; or become more enabling patients to make more value-
knowledgeable on how to avoid, prevent, driven healthcare decisions. As patients
or treat a certain illness. These factors are asked to contribute more towards
typically push healthcare decisions and their healthcare coverage costs, they are
treatments closer to the consumer and pushing for more information and
Figure 4:
Individuals from EU-27 using the Internet for seeking health-related information –
Percentage of individuals aged 16 to 74.
50
40 33% 34%
28%
30 24%
19%
17% 16%
20
10
0
2004 2005 2006 2007 2008 2009 2010
Source: Eurostat 2010. Note: Health-related information: injury, disease, nutrition, improving health, etc.
Within the last three months before the survey.
10 Personalised Medicine in European Hospitals3. Next steps for hospitals
and providers
proteomics specialists with holistic generation of doctors on personalised
knowledge of many different diseases medicine techniques and create
and an understanding of gene curricula that are actionable by a
interactions, eliminating the need for physician. The European Personalised
patients to see a variety of specialists to Medicine Association (EPEMED) is a
treat their ailments”.4 To educate the not-for-profit organisation that puts this
next generation of physicians and nurses very idea into action. EPEMED brings
The steep learning curve must be in the complex issues raised by genomic together key leaders across the
met with education and expertise and proteomic science, universities need healthcare industry to discuss
Hospitals must adapt to the changing to update their programs. personalised medicine, its key
healthcare paradigm and take on the challenges, and best practices. It aims to
aggressive learning curve by educating In addition to formalised training, provide a proactive platform for the
their healthcare providers on the science conversations with leaders in the field of harmonisation of personalised medicine
and clinical application of genomics and personalised medicine across the development and implementation across
proteomics. Doctors will no longer be healthcare industry (e.g. government, Europe, focusing on the crucial role of
able to apply one approach to a set of provider, payer) and academia could diagnostics, to make personalised
patients with a disease state that is offer considerable value. Conversations medicine a reality.5 Key players from the
seemingly similar. These patients may and working groups between payers and healthcare industry, regulators, payers
have a dozen different gene-based providers, for example, could identify and government have an avenue to
variations of the disease, each of which the most efficient reimbursement foster collaboration, learn from one
could require a variation of the methods for diagnostic tests. another and improve patient care
treatment. With formal schooling or Discussions between physicians and through EPEMED.
training programs, “some physicians academics/professors could identify the
might be trained as genomics and best approach to educating the next
Personalised Medicine in Action: Hospital Spotlight
• T he multidisciplinary staff of the Experimental Cancer Therapy Unit at the
Herlev Hospital in Copenhagen, Denmark is trained in handling blood
samples for pharmacokinetics pharmadynamics and translational
research.
• Genetic diagnostics is done at the University of Eastern Finland, Kuopio,
which collaborates closely with the Kuopio University Hospital. Knowledge
on monogenic forms of diseases and the potential of modern genetics is
part of the course work for medical students.
• T he Medical and Health Science Center University of Debrecen in Hungary
trains new doctors to practice personalised medicine. There are PhD
courses on the field.
• T he University Medical Centre Ljubljana, Slovenia, has a Clinical Institute
of Medical Genetics, which aims to develop tests and counselling as it
relates to personalised medicine.
PwC, “The new science of personalized medicine: Translating the promise into practice”, 2009.
4
Association European Personalised Medicine, EPEMED, retrieved 4 May 2010, from http://www.epemed.org/index.html.
5
Personalised Medicine in European Hospitals 11Effective technology is the Due to different needs among interoperable countrywide, due to
foundation for personalised specialities, hospitals find it more various restrictions such as technology,
medicine difficult to integrate EHR systems, lack of standards or legal frameworks.
The foundation for personalised although a few countries have more This lack of standardisation also results
medicine will be distributed access to than 50% of their hospitals supported by in challenges for cross-border care in
health information, not just for health EHR systems.9 Most installed EHR Europe.
professionals.6 With the institution of systems in European countries are not
electronic health records (EHRs),
genomic, proteomic and personalised
medicine data could be shared. Greater
sharing of data that is instantaneous Figure 5:
could accelerate research efforts In the next five years, which of the following changes, if any, are most likely to
dramatically. Results from a PwC survey affect your health system? (multiple response question)
demonstrated that a majority of
respondents felt that within the next five Merging of information technology & healthcare 84
years, “merging of information
Relaxation of scope of practice laws that will enable
technology and healthcare” will most clinicians to provide more primary care
58
likely affect their health system (See
Increased use of virtual health communities 56
Figure 5).
Personalised medicine 45
Technology alone, however, will not be
sufficient. A great deal of thought will More travel/tourism among patients 45
need to be put into what data will be Relaxation of country restrictions on foreign
44
captured, where it will come from, what medical graduates
the appropriate data types and formats More health insurance coverage for travel/tourism 43
will be, and how it should be presented
to a physician.7 0 10 20 30 40 50 60 70 80 90
Because medical and academic research Source: PwC’s Health Research Institute Global Health Leaders Survey
centres often work in information silos,
connecting EHRs is challenging due to
differing data standards. Agreement on
common data formats and standards
will serve to reduce complexity and
Personalised Medicine in Action: Hospital Spotlight
allow doctors and hospitals to share
data among one another.8 • T
he Experimental Cancer Therapy Unit, Department of Oncology at HEH, has
access to MRI, CT and PET-scans and a variety of other interventional
Although the agreement on common diagnostic radiology and clinical physiological assessments.
data and data consistencies is a huge • G
enetics offers the possibility to diagnose monogenic diseases accurately at
task that requires time, effort and Kuopio University Hospital.
money, there are some promising • N
ew imaging technologies, such as 3 Tesla MRI and PETscan, are available at
initiatives from the European the University Hospital of Dijon.
perspective such as EUROREC Institute • T
he Medical and Health Science Center University of Debrecen uses
(EuroRec). This is an independent telemedicine to remotely monitor cardiology patients with remote ECG
not-for-profit organisation that promotes (holter).
the use of high-quality Electronic Health
• T
he University Medical Centre Ljubjana develops and uses their own analysis
Record systems (EHRs) in Europe.
software tools for the application of personalised medicine techniques.
EuroRec has also developed some tools
to exploit its repository and has • T
he Hospital Clinic in Barcelona uses remote monitoring devices for cardiac
elaborated (standard) procedures for pathologies and chronic diseases.
the certification of eHealth products.
6
PwC, “The new science of personalized medicine: Translating the promise into practice”, 2009.
7
HealthcareLeaders Media in collaboration with PwC, “Breakthroughs: The Impact of Personalized Medicine Today”, 2010.
8
PwC, “The new science of personalized medicine: Translating the promise into practice”, 2009.
9
Electronic Health Record Systems-A Main Pillar in European e-Health Developments for Better Delivery of Care. G. Comyn, Head of Unit “ICT for Health”, DG INFSO,
European Commission, 2007.
12 Personalised Medicine in European HospitalsChanges in the healthcare medical education and clinical care treatment. This has reduced the cost of
paradigm create opportunities to makes them well positioned to identify treatment for key populations.11
innovate and bend the cost curve unmet market needs and discover new
As the emphasis on wellness grows and targeted therapies. Academic medical Willingness to collaborate will give
payers and consumers seek alternative, centres also have access to massive providers the competitive edge
less expensive forms of care, hospital amounts of patient data, which While these changes in the healthcare
admissions will likely decrease. accelerates the discovery process. paradigm have posed challenges to
Providers will be challenged to deliver Moreover, this creates an hospitals and providers, they may have
new forms of care in order to maintain unprecedented opportunity to redefine also created opportunities for key
consistent revenue. But through the new the research data continuum by participants in the healthcare industry
wave of preventative medicine and launching an exchange of data that overall, particularly for non-traditional
wellness, hospitals may be able to create goes full circle — from a researcher’s healthcare participants. Personalised
new sources of revenue by launching laboratory to a patient’s bedside medicine, specifically, is a highly
new services and products focused on back to the researcher’s laboratory complex field, and no one organisation
wellness and disease prevention, which again. or industry has the requisite resources,
will in turn create greater demand for knowledge and tools needed to
molecular tests to determine The introduction of personalised implement solutions in this field. This
predispositions and/or therapeutics as medicine at the point of care will require new science not only creates
well as the corresponding health a huge change in the way healthcare is opportunities for hospitals and the
services required.10 organised. How this might be done is industry to innovate, but also to
illustrated by a system in France for the collaborate within or outside their
Hospitals linked to universities may treatment of cancer. France’s National industries to create the best possible
have brighter prospects, as they are Cancer Institute has set up a network of solutions.12
prepared to take the lead in 28 regional centres, linked with
personalised medicine research. Their hospitals, where the tumours of cancer The following are a few examples of the
unique combination of academic patients can be rapidly analysed to types of innovation emerging through
research, state-of-the-art technology, establish their suitability for drug collaborative relationships:
Personalised Medicine in Action: Hospital Spotlight
• S
everal departments at the Herlev Hospital/Copenhagen University in
Denmark have focused on nutrition and physical activity to improve
wellness and treatment of patients.
• T
he Medical and Health Science Center University of Debrecen in
Hungary has a special nutrition centre where patients receive a personal
diet, and they are currently building a wellness centre focused on
rheumatologic services.
10
HealthcareLeaders Media in collaboration with PwC, “Breakthroughs: The Impact of Personalized Medicine Today”, 2010.
11
European Perspectives in Personalised Medicine, May 2011. European Commission.
12
PwC, “The new science of personalized medicine: Translating the promise into practice”, 2009.
Personalised Medicine in European Hospitals 13European universities and medical centres for national networks of clinical (EATRIS) is based on translation centres
schools form partnerships with research centres and clinical trials units, created by clinics and biomedical
research centres abroad to enhance and is able to provide support and research institutions with translational
innovation. services to multinational clinical experience.
• The University of Minnesota and Mayo research.
Clinic, under the mantle of the • Biobanking and Biomolecular Resources We expect to see complex networks of
Minnesota Partnership for Biotechnology Research Infrastructure (BBMRI) forms collaboration to emerge, within and across
and Medical Genomics, have formed a an interface between specimens and industries and between the public and
strategic research relationship with the data (from patients and European private sectors, as individual organisations
Karolinska Institute of Stockholm, populations) and top-level biological and or industries deal with the complex
Sweden, the top-rated medical research medical research. During the past three challenges that come with this new focus
university in Europe. Leaders of each years, BBMRI has grown into a on personalised medicine.17 As
institution signed memoranda of 53-member consortium with over 280 collaborative partnerships develop, it will
understanding to commit to the formal associated organisations (largely be important to consider how these
ongoing collaboration, called the biobanks) from over 30 countries, complex alliances can be appropriately
Frontiers of Biomedical Research.13 making it the largest research managed so that all parties can benefit
infrastructure project in Europe. from the innovations that emerge.
Pharmaceutical companies have shown • The European Advanced Translational
their commitment to developing Research Infrastructure in Medicine
personalised treatments by
collaborating with companies in their
industry.
• Procter & Gamble and Inverness Medical Personalised Medicine in Action: Hospital Spotlight
Innovations, a diagnostics company,
• T
he Herlev Hospital/Copenhagen University Hospital is collaborating with
created a $325 million joint venture to
other universities in Denmark, the European Union and the United States for
create diagnostics products.14
research purposes and treatment of patients, as well as with the National
• Merck and AstraZeneca collaborated to
Laboratory for Sustainable Energy and many biotech and pharmaceutical
combine two experimental cancer drugs,
companies.
one from each company, to create a
cocktail that could provide better results • T
he Kuopio University Hospital in Finland is collaborating with several
than each alone.15 institutions for research purposes, including the National Institutes of Health
of the US Department of Health and Human Services, the University of
Non-traditional healthcare companies Southern California and the University of Ann Arbor in the United States, and
are working together to increase the University of Gothenburg in Sweden.
innovation in technology that will • T
he University Hospital of Dijon, France, is collaborating with several
monitor the individual’s health. organisations, including other university hospitals, scientific groups and
• Intel and General Electric formed an biotech companies. In particular, the University Hospital of Dijon collaborates
alliance to market home-based health. with the Cancer Centre Georges François Leclerc, which develops its own
The primary objectives were to enable research programs, some of which are common within the University
remote monitoring of patients and lower Hospital of Dijon, INSERM research centre and the biotech company
healthcare costs by reducing the number Oncodesign.
of necessary hospital visits.16 • T
he Medical Health Science Center University of Debrecen, Hungary, is
collaborating with orphan drug companies, such as Genzyme, a laboratory
Multicentre networks of clinical testing research on Fabry disease.
research in Europe.
• The
University Medical Centre Ljubljana, Slovenia, is collaborating with other
• The European Clinical Research
universities, companies providing consumables, government and health
Infrastructures Network (ECRIN) is
insurance companies.
based on the connection of coordinating
13 Universityof Minnesota, Mayo Clinic sign research pact with Karolinska. Available at http://www.ahc.umn.edu/media/releases/umayokaro/index.htm.
14 “P&G partners with Inverness in diagnostics venture” Mass High Tech, 18 May 2007. Available at http://www.masshightech.com/stories/2007/05/14/daily43-PG-
partners-with-Inverness-in-diagnostics-venture.html.
15 Ron Winslow, “AstraZeneca, Merck to Test Cancer Drugs in ‘Cocktail’”, Wall Street Journal, 2 June 2009. Available at http://online.wsj.com/article/
SB124380640803770139.html.
16 Gran Gross, “Intel, GE partner on home health tech”, NetworkWorld, 2 April 2009. Available at http://www.networkworld.com/news/2009/040209-intel-ge-partner-
on-home.html.
17 PwC, “The new science of personalized medicine: Translating the promise into practice”, 2009.
14 Personalised Medicine in European Hospitals4. Conclusions
on which treatment(s) should be used
when reading genetic data. This
includes making better use of modern
imaging technologies as well as the
more effective use of decision support
tools. While many new potential
biomarkers are being discovered, the
Although a great deal of progress has rate at which these are being qualified
been made in genomic and proteomic and validated is slow.
research and the field of molecular • Universal standards for managing
genomics, many challenges remain. genomic information in electronic
medical records will be necessary to
The learning curve poses new implement this technology and ensure
challenges for doctors and clinical data is collected and
scientists interpreted in a standardised
• Recognising which genes or biological manner.20
mechanisms signify that a patient is
predisposed to certain diseases and The least evident challenge is
how this in turn translates into often the hardest to overcome
knowledge that can be used for • Consumer behaviour, an obstacle that
prevention and treatment strategies may not be apparent, will be key when
poses a large learning curve that implementing personalised medicine
scientists and doctors will have to and creating a culture that can adapt
overcome.18 to these changes.21
•H ow we manage our personal health
• Diseases need to be reclassified to and lifestyle are not only difficult
reflect new knowledge about human habits to modify but also play a key
biology. Many clinical entities role in our susceptibility to disease
currently described as single diseases and disease management. Swinging
may in fact be more than one disease, the pendulum from treatment to
requiring different treatment prevention and from illness to
approaches.19 wellness will be essential to
implement a consumer-focused
Implementation of effective culture.
technologies is no easy task •P atients need to be educated and
• Key challenges remain in determining physicians need to be instructed in the
the appropriate type and new technologies and methods that
sophistication of technology needed allow for a more personalised
for doctors to make effective decisions diagnosis of diseases and treatments.
18 PwC, “The new science of personalized medicine: Translating the promise into practice”, 2009.
19 European Perspectives in Personalised Medicine, May 2011. European Commission.
20 PwC, “The new science of personalized medicine: Translating the promise into practice”, 2009.
21 PwC, “The new science of personalized medicine: Translating the promise into practice”, 2009.
Personalised Medicine in European Hospitals 15These challenges will need to be • Provide new health and wellness
addressed at European, national, products and services to the
regional and local levels. community.
• Work with patients to educate them
With any challenge, however, comes about the need to proactively manage
opportunity. The shifting healthcare their own health and commit to
paradigm provides hospitals and wellness programs and the benefits
healthcare systems around the world that some programs have derived from
with an opportunity to adapt to the putting them into practice.
changing needs of the patient, treat the • Look to other industries to understand
disease sooner and create cost-cutting how to market directly to patients and
measures by instituting alternate forms deliver excellent customer-centric
of medicine or treatment. Key services.
recommendations are evident as the • Collaborate in research projects to
health industry considers how to boost personalised medicine research
respond to the emerging personalised productivity and effectiveness as well
medicine market and explore as ensure that proper policy
sustainable business models. recommendations are developed to
accelerate and support this emerging
Recommendations for providers/ market.
provider systems are as follows: • Encourage collaboration between
• Learn genomics and proteomics to personalised medicine experts and
develop effective prevention and doctors with expertise in the field in
treatment plans. the development of new care models.
16 Personalised Medicine in European Hospitals• Implement interoperable electronic hospitals and providers to respond to the
health records to enable the sharing of changing market. Personalised medicine
genomic, proteomic, and other health can be set up and implemented into a
data related to personalised medicine hospital model in a variety of ways, as
among research and healthcare discussed in the interviews with several
organisations. European hospitals in Part II of this
document. As demonstrated through the
It is clear that key challenges exist as the preceding “Hospital Spotlights”, many
pressure to be personalised continues to European hospitals have already begun
mount. As evidenced through the above to define what personalised medicine
recommendations, hospitals and means to their hospital and have
providers have a clear opportunity to developed their approach to
adapt to the new healthcare paradigm implementation.
and provide services that are targeted to
the individual patient. It is important to
recognise, however, that different
hospitals operate and require different
hospital models. Just as doctors will no
longer be able to apply the same forms of
treatment to a group of patients, not all
hospitals will be able to apply the same
approach to addressing the challenges
brought on by personalised medicine.
Fortunately, there are many ways for
Personalised Medicine in European Hospitals 17Part II. Hospitals in focus List of Participating Hospitals Herlev Hospital / Copenhagen University Hospital at Herlev, Denmark Kuopio University Hospital, Finland University Hospital of Dijon, France Medical and Health Science Center University of Debrecen, Hungary University Medical Centre Ljubljana (UMCL), Slovenia Hospital Clinic de Barcelona, Spain 18 Personalised Medicine in European Hospitals
Copenhagen, Denmark.
Herlev Hospital/
Copenhagen
University
Hospital at Herlev
Denmark
Herlev Hospital (HEH) has for treatment with trastuzumab. Clinical Biochemistry, Pathology,
several years focused on research for Several units at HEH provide Radiology and Clinical Physiology.
better personalised medicine and technical and logistical support to HEH has several PET/CT, CT, MRI
has included new biomarkers in research in personalised medicine. and ultrasound scanners used in
routine clinical practice, e.g. analysis These units help to improve the projects related to personalised
of KRAS mutation status in patients effectiveness of the logistics medicine, e.g. early evaluation of
with colorectal cancer before processes and research activities in treatment response to new biologics
treatment with cetuximab and the field of oncology, hematology, for cancer patients.
analysis of HER2 protein expression medicine, surgery and gynecology.
in patients with breast cancer before The units include Departments of
Type of Hospital Public/Academic
425,000 (700,000 in
Reference Population
certain specialities)
Nº Beds 624
Nº Employees 4,141
Nº Physicians 768
Nº Inpatient
131,123
Admissions
Nº Day-Hospital
426,379
Admissions
Nº Surgery
20,400
Procedures
Hospital Annual
3,008 mil DKR
Revenues
Interview with Julia S. Johansen,
Professor, Senior Consultant, DMSc, Herlev Hospital
Hospitals in focus 19Interview with Julia S. Johansen
What do you believe to be the key trends related to the What are the top five value propositions that
implementation of personalised medicine within the personalised medicine may provide?
hospital environment?
Feasibility/ Ease of Time Horizon
Danish patients and healthy subjects are willing to participate Value Proposition
Implementation1
in translational studies concerning improved personalised Better clinical response 1 10 years
medicine. The infrastructure and logistics are established for Better survival 1 15 years
translational research at HEH. We mainly need further Reduce treatment failures 1 10 years
support for hospital staff, researchers and operational costs Reduce side effects 1 10 years
for analysis studies in translational research. Decrease cost 1 10 years
1
Each proposal is rated within a scale 1: high complexity and 5: low complexity
How should the health system in your country lay the
groundwork for the next steps in personalised What are the main barriers for the implementation of
medicine? personalised medicine within the hospital
Increase the amount of funding for specific studies related to environment?
translational medicine with a main focus on better Lack of research funding for better personalised medicine.
personalised medicine.
Description of personalised medicine approach in your hospital:
Core Activity
Diagnostics and Many departments at HEH have a high focus on better diagnostics and therapeutics, e.g. cancer patients are
Therapeutics discussed at multidisciplinary team conferences (surgeons, oncologist, pathologists and radiologists).
Personalised Medical Care
EMR/Clinical
Conducted between departments and at multidisciplinary team conferences.
Decision Support
Disease management is used in several departments, such as oncology, haematology, intensive care, surgery
Disease Management
and medicine, paediatrics, and gynaecology. Personalised medical care is used in disease management.
Telemedicine/Remote
Multidisciplinary teleconferences with other hospitals.
Patient Monitoring
HEH participates in many research projects related to better personalised medicine that is funded by public
and private agencies.
The Copenhagen General Population Study is located at the Department of Clinical Biochemistry. This is
a blood biobank and research study which will follow about 100,000 volunteers, aged 20 years to 100 years,
from the Copenhagen area in Denmark. Today more than 60,000 volunteers are included. Initial enrolment
Research/Expansion
is taking place at HEH, and the participants are followed yearly in the Danish Health registries thereafter.
of Science-Base
The secretarial office of the Danish CancerBiobank is located at the Molecular Unit, Department of Pathology,
HEH. The objective of this biobank nationally is to collect blood and tissues optimal for translational research
from patients with primary cancer in order to, for example, improve personalised medicine. The project started
in January 2010, which included biological material from 5,281 patients in its first year. There is a connection
with the Danish nationwide clinical databases and other national registries.
The Experimental Cancer Therapy Unit, Department of Oncology at HEH has been involved in clinical
trials for more than 25 years. The department has broad experience with cytostatic drugs, biological and
anti-hormonal agents, dendritic cells, and intrahepatic chemotherapy. The Experimental Cancer Therapy
Unit was founded in 2004. Its core competency focuses on the planning, preparation and conduct of phase I
clinical trials in cancer patients as well as early phase II trials.
• The unit offers complete project and clinical trial management systems.
Others
• The unit operates with ICH GCP and standards of the pharmaceutical industry, including standard
operating procedures (SOP’s) covering all aspect of clinical trials.
• The unit complies with all current legal requirements and the EU Directive on Clinical Trials (Directive
2001/20/EC & Directive 2005/28/EF).
• The unit has experience in design and administration of databases and the development of computerised
trial management software.
20 Personalised Medicine in European HospitalsInterview with Julia S. Johansen
•T he unit has experience in incorporation of health economics and quality-of-life measures.
•T he unit has a network of leading scientists and oncologists and collaborates with other phase I units in
Denmark and Europe.
A dedicated team, including research nurses, oncologists, and statisticians staffs the unit. The staff members
have a comprehensive experience in developing, planning, implementing and running a clinical trial, as well
Others
as conducting data management and statistical analysis. The staff members are trained in handling blood
samples for pharmacokinetics, pharmadynamics and translational research. Additionally, tissue sampling
may be added to the unit through the collaboration with the Department of Diagnostic Radiology and
various surgical departments. Furthermore, the unit has access to MRI, CT and PET-scans, and a variety of
other interventional diagnostic radiology and clinical physiological assessments.
Nutrition & Wellness
Nutrition/Organic Several departments have focused on nutrition and physical activity to improve wellness and treatment of
Care patients.
Complementary &
N/A
Alternative Medicine
Others N/A
Other Related Products and Services
Stem Cells N/A
The Clinical Research Unit, Department of Oncology, HEH has been involved in clinical trials for more than
25 years. The department has broad experience with cytostatic drugs, biological and anti-hormonal agents,
dendritic cells, and intrahepatic chemotherapy.
Clinical Research Unit was founded in 1992. The main objective of the unit is to conduct high-quality
research to achieve patient benefits. Its core competencies focus on the planning, preparation and
performance of phase I–III clinical trials in cancer patients.
•T he unit offers complete project and clinical trial management systems.
•T he unit operates with ICH GCP and standards of the pharmaceutical industry, including standard
operating procedures covering all aspect of clinical trials.
•T he unit complies with all current legal requirements and the EU Directive on Clinical Trials (Directive
2001/20/EC & Directive 2005/28/EF).
•T he unit has experience in the design and administration of databases and the development of
computerised trial management software.
•T he unit has experience in incorporation of health economics and quality-of-life measures.
Others •T he unit has expertise and computing facilities required to coordinate multicentre clinical trials.
•T he unit organises educational activities, including training courses and workshops.
•T he unit has a network of leading scientists and oncologists, including collaboration with other phase I
units in Denmark and Europe.
The unit collaborates closely with the Experimental Cancer Therapy Unit, a dedicated unit for
experimental cancer therapy and phase I trials. Furthermore, the unit has easy access to a basic science
laboratory and all facilities of a large centre.
A dedicated team, including research nurses, oncologists and statisticians staff the unit. The staff members
have comprehensive experience in developing, planning, implementing and running a clinical trial, as well
as conducting data management and statistical analysis. The staff members are trained to handle blood
samples for pharmacokinetics, pharmadynamics and translational research. Additionally, tissue sampling
may be added to the unit through the collaboration with the Department of Diagnostic Radiology and
various surgical departments. Lastly, the unit has access to MRI, CT and PET-scans, and a variety of other
interventional diagnostic radiology and clinical physiological assessments.
Hospitals in focus 21Interview with Julia S. Johansen
Where does your hospital stand on the Which service lines, including clinical services as well
implementation level of each activity? as non-clinical services, related to personalised
medicine are more developed in your hospital?
Diagnostics and
Therapeutics
• Clinical chemistry: e.g. SNPs, genes, mRNA, microRNA,
5
protein biomarkers
4
• Pathology: e.g. SNPs, genes, mRNA, microRNA, protein
Nutrition / Organic EMR / Clinical
Care Decision Support
biomarkers
3
• Radiology: CT, MRI, ultrasound
2
• Clinical Physiology: PET/CT
1
0 Policies and programs play an important role as an
Other: The Disease accelerator and regulator. What are the key
Experimental Management personalised medicine enablers in your hospital
environment?
Herlev Hospital has for several years focused on research for
Research /
Telemedicine / better personalised medicine and has rapidly incorporated
Expansion of
Remote Patient
Science-Base
Monitoring
new biomarkers in routine clinical practice, e.g. analysis of
KRAS and BRAF mutation status in patients with colorectal
(0: Not applicable; 5: High development).
cancer and melanoma before treatment with biologics and
analysis of HER2 protein and FISH expression in patients with
Do you have relationships or affiliations with other breast cancer before treatment with trastuzumab.
sector organisations as it relates to personalised
medicine (such as universities, IT companies, HEH participates in many research projects related to better
government, biotech, etc.)? How do these personalised medicine funded by the Hospital, and also by,
relationships work? e.g. the Danish government, the Danish Cancer Society, the
HEH is collaborating with several institutions for research Danish Heart Association, the Danish Rheumatism
purposes and treatment of patients. These institutions Association, Biotech Companies like Novo Nordisk, Roche,
include: Merck/Serono, Novartis and private foundations.
• Other University Hospital in Denmark
• Other universities in Denmark, the European Union, and the The “Copenhagen General Population Study” is located at the
United States Department of Clinical Biochemistry, HEH. This is a blood
• T he Danish Technical University biobank and research study which will follow 100,000
• R ISØ, National Laboratory for Sustainable Energy volunteers, aged 20 years to 100 years, from the Copenhagen
• Many biotech and pharmaceutical companies area in Denmark. Today more than 60,000 volunteers are
included. Initial enrolment is taking place at HEH, and the
Have you built a research centre that encompasses participants are followed yearly in the Danish Health
personalised medicine? registries thereafter. Some of the expenses (e.g. salaries to
The Clinical Research Unit, Department of Oncology, has a technicians and doctors, biomarker analysis) for this unique
close collaboration with the Experimental Cancer Therapy biobank are paid by HEH.
Unit, a dedicated unit for experimental cancer therapy and
phase I trials. Furthermore, the unit has easy access to a basic The secretarial office of the “Danish CancerBiobank” is
science laboratory and all facilities of a large centre. located at the Molecular Unit, Department of Pathology, HEH.
The objective of this biobank is to nationally collect blood and
The units have access to MRI, CT and PET-scans, and a variety tissues optimal for translational research from patients with
of other interventional diagnostic radiology and clinical primary cancer in order to, for example, improve personalised
physiological assessments. medicine. The project started in January 2010, and during the
first year, biological material from 5,281 patients was
Current status report on the integration of included. There is a connection with the Danish nationwide
personalised medicine into actual clinical practice clinical databases and other national registries. Some of the
within your hospital: expenses (e.g. salaries to technicians and doctors) for this
Several tests for personalised medicine are used in daily unique biobank are paid by HEH.
clinical practice (e.g. KRAS mutations, HER2 expression,
molecular profiling in haematological disease). Several units at HEH provide technical and logistic support to
research in personalised medicine and help to improve the
22 Personalised Medicine in European HospitalsInterview with Julia S. Johansen
effectiveness of logistics processes and research activities in
the field of oncology, haematology, internal medicine, surgery
and gynaecology. The units include Departments of Clinical
Biochemistry, Pathology, Radiology and Clinical Physiology.
HEH has several PET/CT, CT, MRI and ultrasound scanners
used in projects related to personalised medicine, e.g. early
evaluation of treatment response to new biologics for cancer
patients. Technicians at the Department of Clinical
Biochemistry take many project-related blood samples from
healthy subjects and patients included in different projects,
without cost, at the same time as routine blood samples are
collected. This is also a benefit for the patients (they will not
have to give blood twice) with various types of diseases
included in different clinical studies (including biomarkers
studies of treatment response to, for example, biological
treatment of patients with cancer and inflammatory diseases).
What are the operational challenges you have
experienced in your hospital as it relates to
integrating personalised medicine?
Dimension Challenges
Architecture and Equipment Too little space
Services Offered –
Clinical Activity –
Organisational Structure –
IT Bad/slow in many areas
Financial Limited financial support
Research & Development –
Academic/Teaching activity –
How does personalised medicine impact on quality
measures in your hospital?
• Better survival
• Fewer side effects
• Shorter hospitalization With any new technology or new initiative, there is an
• Cost adoption curve before the initial investment pays off.
• Patients are more satisfied Where do you stand with personalised medicine on
that curve?
Can you describe the basic infrastructure New technologies of initiatives for personalised medicine are
(technologies and tools) for the application of typically adopted as soon as they are introduced.
personalised medicine that exists in your hospital
today? Did personalised medicine impact the roles and
Several units at HEH provide technical and logistical support responsibilities of your healthcare providers?
to research in personalised medicine. These units help to Yes, very much. In recent years, the cost of new medicine, i.e.
improve the effectiveness of the logistics processes and biologics like adalimumab and infliximab (for patients with
research activities in the field of oncology, haematology, rheumatoid arthritis); trastuzumab (for patients with breast
medicine, surgery and gynaecology. The units include the cancer); rituximab (for patients with lymphoma) and
Departments of Clinical Biochemistry, Pathology, Radiology bevacizumab, cetuximab and panitumumab (for patients with
and Clinical Physiology. HEH has several PET/CT, CT, MRI colorectal cancer) have increased dramatically during the last
and ultrasound scanners used in projects related to five to ten years. Unfortunately, less than 30% of the patients
personalised medicine. Early evaluation of treatment response will benefit from the treatment since it is very expensive and
to new biologics for cancer patients is one example. has severe side effects. The healthcare providers know very
Hospitals in focus 23You can also read