Performance of GeneXpert MTB/RIF for Diagnosing Tuberculosis Among Symptomatic Household Contacts of Index Patients in South Africa
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Open Forum Infectious Diseases
MAJOR ARTICLE
Performance of GeneXpert MTB/RIF for Diagnosing
Tuberculosis Among Symptomatic Household Contacts of
Index Patients in South Africa
Kavindhran Velen,1, Laura J. Podewils,2 N. Sarita Shah,3 James J. Lewis,4,5 Tiro Dinake,1 Gavin J. Churchyard,1,6 Mary Reichler,7 and
Salome Charalambous1,6
1
The Aurum Institute, Johannesburg, South Africa, 2Denver Public Health, Denver, Colorado, USA, 3Emory University Rollins School of Public Health, Atlanta, Georgia, USA, 4MRC Tropical
Epidemiology Group, London School of Hygiene and Tropical Medicine, London, United Kingdom, 5Y Lab, the Public Services Innovation Lab for Wales, School of Social Sciences, Cardiff University,
Cardiff, United Kingdom, 6The School of Public Health, University of Witwatersrand, Johannesburg, South Africa, 7Atlanta, Georgia, USA
Downloaded from https://academic.oup.com/ofid/article/8/4/ofab025/6104320 by guest on 08 August 2021
Background. We describe the performance of GeneXpert MTB/RIF (Xpert) for diagnosing tuberculosis (TB) among sympto-
matic household contacts (HHCs) of rifampicin-resistant and drug-sensitive index cases.
Methods. We conducted a cross-sectional study among HHCs of recently diagnosed (in diagnosing TB compared with mycobacterial culture [16]. health facility for further TB investigation and preventative A 2015 systematic review of Xpert for diagnosing pulmonary therapy. TB in children found that Xpert offers better sensitivity com- Each sputum specimen was decontaminated using NaOH- pared with smear microscopy; however, its sensitivity remains NALC-sodium citrate solution to a final (NaOH) of 1%. After suboptimum compared with mycobacterial culture [17]. In ad- centrifugation, the pellet was suspended in approximately dition, in the Gambia, among symptomatic household contacts 1.5–2 mL phosphate buffer pH 6.8. The sediment was split to (HHCs)
HHC was determined by combining the self-reported status tests. One hundred seventeen (18.9%) contacts self-reported
with additional testing results obtained through testing that was being HIV positive, and 291 (47.0%) contacts had an unknown
conducted within the households. or negative HIV status at enrollment; of these, 45 (15.5%) were
tested for HIV, and 9 of these were HIV positive. The overall
Patient Consent Statement HIV prevalence was 20.4%.
All study participants provided written consent, and the study
was approved by the ethics committees of the University of Comparison of Diagnostic Performance
the Witwatersrand Human Research Ethics Committee, US Mycobacterial Growth Indicator Tube Culture and Smear
Centers for Disease Control and Prevention, and the research Microscopy Testing
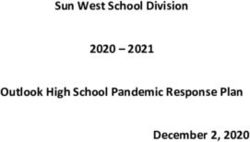
committee of the North West Province, South Africa. Figure 1 shows the results of Xpert and MGIT tests for the 289
specimens. The MGIT testing identified 33 (11.4%) patients
as positive for MTB, 8 (2.8%) were non-TB mycobacteria, 18
RESULTS
(6.2%) were contaminated, and 230 (79.6%) were negative for
Index Patient Characteristics any growth. The median TTCP among culture-positive con-
Downloaded from https://academic.oup.com/ofid/article/8/4/ofab025/6104320 by guest on 08 August 2021
From August 2013 to July 2015, we enrolled 216 index TB cases: tacts was 12 days (IQR, 9–22) with a range of 2–37 days (Figure
73 with RR-TB and 145 with DS-TB (Table 1). The median age 2). Among samples that were both MGIT culture- and Xpert-
was 36 years (interquartile range [IQR], 33–41) for RR-TB pa- positive, the median TTCP was 6 days (IQR, 5–10), whereas
tients and 37 years (IQR, 35–40) for DS-TB patients. The me- among samples that were MGIT culture-positive and Xpert
dian number of HHCs per index patient was 3 (IQR, 1–4) for negative, the median TTCP was 18 days (IQR, 10–26).
both RR-TB and DS-TB patients. Smear microscopy was performed on 289 samples, but 271
were included in the analysis; 5 were smear-positive and 266
Household Contact Characteristics were smear negative. Sensitivity of smear microscopy for detec-
There were 619 HHCs included from the 216 index patients. tion of MTB, using MGIT culture as reference standard, was 3
Median age was 22 years (IQR, 9–40) (Table 2) and females of 33 (9.0%; 95% CI, 1.9–24.3) versus Xpert sensitivity of 21.2%
comprised 60.6% of enrolled HHCs. Previous history of TB overall (P < .001) (Table 3).
was reported among 42 (6.8%) HHCs. There were 336 (54.3%)
HHCs who presented with at least 1 TB symptom; a cough ≥24
hours was the most common symptom, which was reported by Table 2. Characteristics of HHCs and Culture-Positive TB Cases
98.5% of symptomatic contacts. A sputum sample was collected
All HHCs Culture-Positive TB
from 297 (88.4%) symptomatic contacts representing 47.8% of Characteristic (N = 619) Cases (N = 33)
all HHCs; 289 (97.3%) had complete results for all 3 diagnostic Gender, n (%)
Male 244 (39.4) 16 (48.5)
Table 1. Characteristics of Index RR-TB and DS-TB Patients Female 375 (60.6) 17 (51.5)
Age, n (%)
Characteristic MDR-TB (n = 73) DS-TB (n = 145)Xpert Testing evidence for a difference by HIV status in Xpert PPV (66.7% in
Xpert testing identified 16 (5.5%) patients as positive for MTB. The HIV-positive vs 60.0% in HIV-negative; P = 1.0). Xpert spec-
Xpert quantitation results for the 16 sputa in which MTB was de- ificity was 98.9% for HIV-negative vs 96.1% for HIV-positive
tected were “high” for 4 (25.0%), “medium” for 1 (6.3%), “low” for (P = .9) or NPV (90.2% for HIV-negative vs 89.3% for HIV-
6 (37.5%), and “very low” for 5 (31.2%). The mean CT value among positive; P = 1.0).
Xpert-positive contacts was 24.2 (95% CI, 20.8–27.8), the median Among specimens with MTB detected by Xpert, rifampicin
was 24.9 (IQR, 17.3–30.6), and the range was 13.5–33.1. Four of resistance was detected in 2 of 16 (12.5%). The 2 specimens
the 16 Xpert-positive patients tested negative on MGIT culture; 2 that were rifampicin resistant on Xpert were contaminated on
were smear-positive (1+) and 2 were smear-negative. MGIT culture; therefore, phenotypic drug-susceptibility testing
Xpert performance characteristics, stratified by smear and could not be performed.
HIV status, using MGIT culture as the reference standard are Among the 42 TB cases identified through either MGIT cul-
shown in Table 3. Overall, 271 (93.8%) sputa had an interpret- ture, Xpert, or smear microscopy, 81% (34 of 42) were started on
able result for MGIT and Xpert; we excluded 18 specimens from TB treatment; this was reported through patient record review
Downloaded from https://academic.oup.com/ofid/article/8/4/ofab025/6104320 by guest on 08 August 2021
this analysis that were contaminated in MGIT (5 Xpert-positive at the referring health facility. Among TB cases diagnosed on
and 13 Xpert-negative). Xpert sensitivity was 21.2% (95% CI, culture (n = 33), 26 (79%) were successfully started on TB treat-
9.0–38.9), specificity was 98.3% (95% CI, 95.6–99.5), PPV was ment, whereas among TB cases diagnosed on Xpert (n = 16), 12
63.6% (95% CI, 30.8–89.1), and NPV was 90.0 (95% CI, 85.7– (75%) were successfully started on TB treatment.
93.4). Xpert sensitivity was higher for smear-positive specimens
than for smear-negative specimens; 100% (3 of 3) for smear-
positive vs 12.9% (4 of 30) for smear-negatives, P = .06. DISCUSSION
Xpert sensitivity was higher for patients who were HIV- In evaluating Xpert diagnostic performance among HHCs, we
positive than for HIV-negative patients, although not statisti- found that it performed poorly in comparison to mycobacterial
cally significant: 40.0% (4 of 10) for HIV-positive vs 13.0% (3 of culture, diagnosing only 21.2% of all culture-confirmed cases,
23) for HIV-negatives, P = .21. Similarly, there was no statistical although still better than smear microscopy. Xpert diagnostic
HH contacts consented
(N = 619)
HH contacts considered symptomatic
(≥1 symptom)
(N = 336)
Sputum speciments obtained
(N = 297)
MGIT:
sample rejected
(N = 8)
Speciment tested by MGIT, smear
microscopy, and xpert
(N = 289)
MGIT: MGIT: MGIT: MGIT:
MTB present MTB absent NTM contaminated
(N = 33) (N = 230) (N = 8) (N = 18)
Xpert: Xpert:
MTB present MTB absent Xpert:
(N = 7) (N = 26) MTB absent
(N = 8)
Xpert: Xpert: Xpert: Xpert:
MTB present MTB absent MTB present MTB absent
(N = 4) (N = 226) (N = 5) (N = 13)
Figure 1. Flow diagram of Xpert MTB/RIF and mycobacterial growth indicator tube (MGIT) culture testing results. HH, household; MTB, Mycobacterium tuberculosis.
4 • ofid • Velen et alCulture-positive TB cases
Negative (N = 209)
90.2 (85.3–94.0)
98.9 (96.2–99.9)
60.0 (14.7–94.7)
13.0 (2.8–33.6)
40
184/204
184/186
Time-to-culture-positivity (days)
35
3/23
3/5
30
25
HIV Status
20
15
Performance Characteristics of the Xpert MTB/RIF Test Overall, and Stratified by Smear Microscopy Status and HIV Status, Using MGIT Culture as the Reference Standard
10
89.3 (78.1–96.0)
66.7 (22.3–95.7)
96.1 (86.7–99.5)
5
Positive (N = 62)
40.0 (7.5–70.1)
0
50/56
50/52
4/10
4/6
Positive Negative
Xpert MTB/RIF result
Abbreviations: CI, confidence interval; HIV, human immunodeficiency virus; MGIT, mycobacterial growth indicator tube; NPV, negative predictive value; PPV, positive predictive value; TB, tuberculosis.
Downloaded from https://academic.oup.com/ofid/article/8/4/ofab025/6104320 by guest on 08 August 2021
Figure 2. Distribution of time to culture positivity for each of the 33 culture-
positive tuberculosis cases.
Sensitivity of smear microscopy for detection of MTB, using MGIT culture as reference standard, was 3 of 33 (9.0%, [95% CI, 1.9–24.3] vs Xpert sensitivity of 21.2% overall (P < .001).
Negative (N = 266)
performance was possibly influenced by low bacillary burden,
90.0 (85.7–93.4)
66.7 (22.2–95.7)
99.1 (97.0–99.9)
13.3 (3.8–30.7)
an expected consequence of active case finding that has impor-
234/260
234/236
4/30
4/6
tant programmatic implications for TB elimination efforts. Our
study, conducted among HHCs of RR-TB and DS-TB index
patients, found a high microbiologically confirmed TB yield
Smear status
of 6.8% when testing a single spot sputum using either culture
or Xpert.
Tuberculosis yield identified among HHCs in our study is
60.0 (14.7–94.7)
consistent with other studies conducted in South Africa [11, 12],
Positive (N = 5)b
but double the 3.1% estimate from a meta-analysis conducted
100.0
0/0
0.0
3/5
3/3
0/2
0.0
by Fox et al [24] in 2013. In addition, we demonstrated a higher
microbiologically confirmed yield than a recent multicountry
study conducted among contacts of multidrug-resistant TB
index patients that reported a TB yield of 2% among bacteri-
ologically confirmed cases [25]. The high yield highlights the
importance of active case-finding strategies such as HHCT.
Overall (N = 271)a
90.0 (85.7–93.4)
63.6 (30.8–89.1)
98.3 (95.8–99.5)
21.2 (9.0–38.9)
These findings also emphasize the need for scaling-up TB pre- 234/260
234/238
ventive therapies to such high-risk groups, a strategy that has
7/33
7/11
Excluded from the analysis were 18 specimens that were contaminated in MGIT culture.
been shown to be highly effective among contacts exposed to
infectious TB cases [26].
Our findings on Xpert performance contrast with a recent
study conducted by Lebina et al [27] among HHCs, which
found no significant difference in diagnostic yield between
Xpert and culture. It is possible that differences in our study
% (95% CI)
% (95% CI)
% (95% CI)
% (95% CI)
sample preparation and testing, ie, both culture and Xpert tests
were conducted from 1 sample in our study, which differed
N/N
N/N
N/N
N/N
from the Lebina et al [27] study, which used 2 separate samples
for comparison, might explain the contrasting results. The sen-
sitivity of Xpert varies in different settings, ranging from 58% to
100% [28]; however, there are few estimates of its performance
Performance characteristic
Xpert MTB/RIF specificity
Xpert MTB/RIF sensitivity
for HHCT. One study from Tanzania reported a sensitivity of
100% among 5 culture-positive contacts, whereas another from
Xpert MTB/RIF NPV
Xpert MTB/RIF PPV
the Gambia among 14 culture-positive childrenthe limited evidence of Xpert performance in real-world con- shortcomings for diagnosing TB. In particular, Xpert requires lim-
ditions and our contrasting findings, national TB programs ited laboratory infrastructure and human resources, has a quicker
should consider selection of TB testing strategies based on their turnaround for results, and minimizes the possibility of sample
own operational research. contamination, all of which are limitations associated with culture
The poor sensitivity of Xpert from our study and previous testing. Thus, microbiological testing among contacts may require
studies [18, 19] have been explained by lower sputum bacillary a solution that balances the need for quicker results, minimal labo-
burden present during early development of TB disease, dem- ratory infrastructure, and costs but limits missed diagnoses. An al-
onstrated among HHCs or children [29]. A study that diag- gorithm that combines Xpert and culture testing may be possible,
nosed TB in childrenof the smear-negative culture-positive TB cases. The poor 13. Reid MJ, Shah NS. Approaches to tuberculosis screening and diagnosis in people
with HIV in resource-limited settings. Lancet Infect Dis 2009; 9:173–84.
performance of Xpert for diagnosing TB among symptomatic 14. Boehme CC, Nabeta P, Hillemann D, et al. Rapid molecular detection of tubercu-
HHCs suggests that consideration to a more sensitive test such losis and rifampin resistance. N Engl J Med 2010; 363:1005–15.
15. National Department of Health. National Tuberculosis Management Guidelines
a Xpert Ultra, in combination with mycobacterial culture, may 2014. In: Health, ed. South Africa: South African National Department of Health;
be needed to optimize contact investigation. 2014.
16. Dorman SE, Schumacher SG, Alland D, et al.; study team. Xpert MTB/RIF Ultra
for detection of Mycobacterium tuberculosis and rifampicin resistance: a prospec-
Acknowledgments tive multicentre diagnostic accuracy study. Lancet Infect Dis 2018; 18:76–84.
We thank the study participants and the research team for their contribu- 17. Detjen AK, DiNardo AR, Leyden J, et al. Xpert MTB/RIF assay for the diagnosis
of pulmonary tuberculosis in children: a systematic review and meta-analysis.
tions; in particular, Beauty Morake, Martha Seme, Hellen Mooketsi, Victor
Lancet Respir Med 2015; 3:451–61.
Modimokwane, and Peter Mfuloane. 18. Togun TO, Egere U, Sillah AK, et al. Contribution of Xpert(R) MTB/RIF to the
Disclaimer. The findings and conclusions in this manuscript are those diagnosis of pulmonary tuberculosis among TB-exposed children in The Gambia.
of the authors and do not necessarily represent the official position of the Int J Tuberc Lung Dis 2015; 19:1091–7, i-ii.
Centers for Disease Control and Prevention or the US Department of 19. Ntinginya EN, Squire SB, Millington KA, et al. Performance of the Xpert(R)
Health and Human Services. MTB/RIF assay in an active case-finding strategy: a pilot study from Tanzania. Int
Financial support. This work was funded by the US Centers for Disease J Tuberc Lung Dis 2012; 16:1468–70.
Downloaded from https://academic.oup.com/ofid/article/8/4/ofab025/6104320 by guest on 08 August 2021
Control and Prevention (Grant TBNX-14-61028-1; in part to K. V. and 20. World Health Organization. Automated real-time nucleic acid amplification tech-
S. C.). J. J. L. was funded in part by a grant jointly funded by the UK Medical nology for rapid and simultaneous detection of tuberculosis and rifampicin resist-
ance: Xpert MTB/RIF assay for the diagnosis of pulmonary and extra-pulmonary
Research Council (MRC) and the UK Department for International
TB in adults and children. World Health Organization; 2013.
Development (DFID) (MR/K012126/1) under the MRC/DFID Concordat 21. Massyn N, Peer N, English R, et al. District Health Barometer 2015/16. Durban:
agreement and is also part of the EDCTP2 programme supported by the Health Systems Trust; 2016.
European Union. 22. Dorman SE, Chihota VN, Lewis JJ, et al. Performance characteristics of the Cepheid
Potential conflicts of interest. All authors: No reported conflicts of in- Xpert MTB/RIF test in a tuberculosis prevalence survey. PLoS One 2012; 7:e43307.
terest. All authors have submitted the ICMJE Form for Disclosure of 23. Hanrahan CF, Theron G, Bassett J, et al. Xpert MTB/RIF as a measure of sputum
Potential Conflicts of Interest. bacillary burden. Variation by HIV status and immunosuppression. Am J Respir
Crit Care Med 2014; 189:1426–34.
24. Fox GJ, Barry SE, Britton WJ, Marks GB. Contact investigation for tuberculosis: a
References systematic review and meta-analysis. Eur Respir J 2013; 41:140–56.
1. World Health Organization. Global Tuberculosis Report 2019. Geneva: World 25. Gupta A, Swindells S, Kim S, et al. Feasibility of identifying household contacts of
Health Organization; 2019. rifampin-and multidrug-resistant tuberculosis cases at high risk of progression to
2. Ayles H, Muyoyeta M, Du Toit E, et al.; ZAMSTAR team. Effect of house- tuberculosis disease. Clin Infect Dis 2020; 70:425–35.
hold and community interventions on the burden of tuberculosis in 26. Reichler MR, Khan A, Sterling TR, et al.; Tuberculosis Epidemiologic Studies
southern Africa: the ZAMSTAR community-randomised trial. Lancet 2013; Consortium Task Order 2 Team. Risk factors for tuberculosis and effect of pre-
382:1183–94. ventive therapy among close contacts of persons with infectious tuberculosis. Clin
3. Fox GJ, Nhung NV, Sy DN, et al. Household-contact investigation for detection of Infect Dis 2020; 70:1562–72.
tuberculosis in Vietnam. N Engl J Med 2018; 378:221–9. 27. Lebina L, Fuller N, Osoba T, et al. The use of Xpert MTB/Rif for active case
4. Shah NS, Yuen CM, Heo M, et al. Yield of contact investigations in households finding among TB contacts in North West Province, South Africa. Tuberc Res
of patients with drug-resistant tuberculosis: systematic review and meta-analysis. Treat 2016; 2016:4282313.
Clin Infect Dis 2014; 58:381–91. 28. Steingart KR, Schiller I, Horne DJ, et al. Xpert(R) MTB/RIF assay for pulmonary
5. World Health Organization. Systematic Screening for Active Tuberculosis: tuberculosis and rifampicin resistance in adults. Cochrane Database Syst Rev
Principles and Recommendations. Geneva: World Health Organization; 2013. 2014; 1:CD009593.
6. World Health Organization. Recommendations for Investigating Contacts of 29. Detjen AK, DiNardo AR, Leyden J, et al. Xpert MTB/RIF assay for the diagnosis
Persons With Infectious Tuberculosis in Low- and Middle-Income Countries. of pulmonary tuberculosis in children: a systematic review and meta-analysis.
Geneva: World Health Organization; 2012. Lancet Respir Med 2015; 3:451–61.
7. Corbett EL, Bandason T, Duong T, et al. Comparison of two active case-finding 30. Zar HJ, Workman L, Isaacs W, et al. Rapid diagnosis of pulmonary tuberculosis in
strategies for community-based diagnosis of symptomatic smear-positive tuber- African children in a primary care setting by use of Xpert MTB/RIF on respira-
culosis and control of infectious tuberculosis in Harare, Zimbabwe (DETECTB): tory specimens: a prospective study. Lancet Glob Health 2013; 1:e97–104.
a cluster-randomised trial. Lancet 2010; 376:1244–53. 31. Theron G, Peter J, Calligaro G, et al. Determinants of PCR performance (Xpert
8. Hinderaker SG, Rusen ID, Chiang CY, et al. The FIDELIS initiative: innovative MTB/RIF), including bacterial load and inhibition, for TB diagnosis using speci-
strategies for increased case finding. Int J Tuberc Lung Dis 2011; 15:71–6. mens from different body compartments. Sci Rep 2014; 4:5658.
9. Zachariah R, Spielmann MP, Harries AD, et al. Passive versus active tuberculosis 32. Pinyopornpanish K, Chaiwarith R, Pantip C, et al. Comparison of Xpert MTB/
case finding and isoniazid preventive therapy among household contacts in a RIF assay and the conventional sputum microscopy in detecting mycobacterium
rural district of Malawi. Int J Tuberc Lung Dis 2003; 7:1033–9. tuberculosis in Northern Thailand. Tuberc Res Treat 2015; 2015:571782.
10. Jackson-Sillah D, Hill PC, Fox A, et al. Screening for tuberculosis among 2381 33. Theron G, Venter R, Smith L, et al. False-positive Xpert MTB/RIF results in re-
household contacts of sputum-smear-positive cases in The Gambia. Trans R Soc tested patients with previous tuberculosis: frequency, profile, and prospective
Trop Med Hyg 2007; 101:594–601. clinical outcomes. J Clin Microbiol 2018; 56:e01696-17.
11. Thind D, Charalambous S, Tongman A, et al. An evaluation of ‘Ribolola’: a house- 34. Rachow A, Zumla A, Heinrich N, et al. Rapid and accurate detection of
hold tuberculosis contact tracing programme in North West Province, South Mycobacterium tuberculosis in sputum samples by Cepheid Xpert MTB/RIF
Africa. Int J Tuberc Lung Dis 2012; 16:1643–8. assay–a clinical validation study. PLoS One 2011; 6:e20458.
12. Shapiro AE, Variava E, Rakgokong MH, et al. Community-based targeted case 35. Firnhaber C, Kendall MA, Wu X, et al. Evaluation of Xpert MTB/RIF to identify
finding for tuberculosis and HIV in household contacts of patients with tubercu- pulmonary tuberculosis in tuberculosis suspects from low and higher prevalence
losis in South Africa. Am J Respir Crit Care Med 2012; 185:1110–6. settings compared to acid fast smear and culture. Clin Infect Dis 2016; 62:1081-8.
GeneXpert Performance in TB Contacts • ofid • 7You can also read