Oral Care as Prevention for Nonventilator Hospital-Acquired Pneumonia: A Four-Unit
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
ORIGINAL RESEARCH
Oral Care as Prevention
for Nonventilator
Hospital-Acquired
Pneumonia: A Four-Unit
Cluster Randomized Study
Findings suggest that daily oral care can play a crucial role.
H
ospital-acquired pneumonia (HAP) is now ity.8, 13, 14 Moreover, within 48 hours of hospitaliza-
the most common type of hospital-acquired tion, changes occur in the oral microbiota that are
infection in the United States, accounting associated with more virulent pneumonia-caus-
for 26% of all such infections, according to the ing organisms.15, 16 Respiratory pathogens such as
most recent point prevalence survey conducted Staphylococcus aureus, Klebsiella pneumoniae,
by the Centers for Disease Control and Preven- Enterobacter cloacae, and Pseudomonas aerugi-
tion (CDC).1 It is also the most common hospital- nosa colonize the dental plaque and can be aspi-
acquired infection in Europe.2, 3 Of the HAP cases rated, introducing these organisms into the lungs,
in the CDC survey, fully 65% were found to be even in healthy adults.17-19 Studies indicate that
nonventilator hospital-acquired pneumonia (NV- patients are up to six times more likely to develop
HAP). HAP if the mouth is persistently colonized by
NV-HAP presents a serious and largely prevent- such pathogens.15, 20 Several studies have shown
able threat to patient safety. Compared with all that improved cleaning of the oral biofilm pro-
other hospital-acquired infections except ventilator- vides primary source control of HAP pathogens
associated pneumonia, NV-HAP is associated with and reduces HAP incidence.5, 14, 21
increased morbidity and mortality, longer hospital Given the relatively high risk of NV-HAP, it’s
stays, increased ICU utilization, and markedly imperative that we gain a better understanding of
higher costs.4-7 One study found that, after control- effective means of prevention. An emerging body
ling for multiple comorbidities and other factors, of literature addresses the role of oral care in pre-
patients with NV-HAP were at much higher risk for venting NV-HAP.4, 21-26 An associated reduction in
death during hospitalization than those without antibiotic use has also been noted.27 Because oral
NV-HAP (15.5% versus 1.6%).7 microbiota is arguably the most modifiable risk
Pathogenesis. Pneumonia occurs when factor for NV-HAP,21, 22 primary source control was
microbes move from proximal sites such as the the underlying strategy used in this study.
oral cavity into the lungs and incite an inflam- Study aim. The primary aim of this study was
matory response.8-10 Researchers have found an to determine the effectiveness of a universal, stan-
important relationship between the oral micro- dardized oral care protocol in preventing NV-HAP
biota and HAP.10-12 For example, bacteria found in the acute care setting, specifically, four units at
in the bronchi of patients with HAP have been an 800-bed tertiary medical center. We hypothe-
matched with specific flora found in the oral cav- sized that there would be a significant reduction in
24 AJN ▼ June 2021 ▼ Vol. 121, No. 6 ajnonline.comBy Karen K. Giuliano, PhD, RN, FAAN, Daleen Penoyer, PhD, RN, CCRP, FCNS, FCCM,
Aurea Middleton, RN, and Dian Baker, PhD, RN, APRN-BC, PNP
ABSTRACT
Background: Nonventilator hospital-acquired pneumonia (NV-HAP) presents a serious and largely
preventable threat to patient safety in U.S. hospitals. There is an emerging body of evidence on the effec-
tiveness of oral care in preventing NV-HAP.
Purpose: The primary aim of this study was to determine the effectiveness of a universal, standardized
oral care protocol in preventing NV-HAP in the acute care setting. The primary outcome measure was NV-
HAP incidence per 1,000 patient-days.
Methods: This 12-month study was conducted on four units at an 800-bed tertiary medical center.
Patients on one medical and one surgical unit were randomly assigned to receive enhanced oral care
(intervention units); patients on another medical and another surgical unit received usual oral care (control
units).
Results: Total enrollment was 8,709. For the medical control versus intervention units, oral care fre-
quency increased from a mean of 0.95 to 2.25 times per day, and there was a significant 85% reduction in
the NV-HAP incidence rate. The odds of developing NV-HAP were 7.1 times higher on the medical control
versus intervention units, a significant finding. For the surgical control versus intervention units, oral
care frequency increased from a mean of 1.18 to 2.02 times per day, with a 56% reduction in the NV-HAP
incidence rate. The odds of developing NV-HAP were 1.6 times higher on the surgical control versus inter-
vention units, although this result did not reach significance.
Conclusions: These findings add to the growing body of evidence that daily oral care as a means of
primary source control may have a role in NV-HAP prevention. The implementation of effective strategies
to ensure that such care is consistently provided warrants further study. It’s not yet known what degree
and frequency of oral care are required to effect favorable changes in the oral microbiome during acute
care hospitalization.
Keywords: hospital-acquired infection, nonventilator hospital-acquired pneumonia, oral care,
pneumonia
NV-HAP incidence on the intervention units com- had 26 beds for postoperative cardiac surgery
pared with the control units. Frequency of oral care patients; the surgical control unit had 32 beds for
in compliance with the new oral care protocol was postoperative vascular surgery patients. Nurse-to-
used to assess fidelity to the intervention. The pri- patient ratios were 1:4 on the medical units and
mary outcome measure was NV-HAP incidence 1:3 on the surgical units. Nursing assistant-to-
per 1,000 patient-days. Our secondary aim was patient ratios were 1:9 on the medical units and
to learn more about NV-HAP outcomes and add 1:7 on the surgical units. Other nursing care
this to the emerging literature.4, 6, 28 To that end, we actions that might influence NV-HAP rates, such
also collected data on NV-HAP–associated events, as head of bed elevation and early mobilization,
including the development of postadmission sepsis, were not changed and were similar between the
unplanned ICU transfer, 30-day readmission, and control and intervention units.
mortality. Sample. To determine the necessary sample
size, a power analysis was conducted via
METHODS G*Power 3.1.9.4 freeware.29 Using data from
Study design and setting. The study was previous research on NV-HAP incidence and pre-
designed as a single-site cluster randomized trial. implementation data, we performed the analysis
It involved a total of four clinical units: one medi- with a target set at 50% reduction in the NV-HAP
cal and one surgical unit were randomized to an incidence rate from 1.8 per 1,000 patient-days
enhanced oral care protocol; these were matched (control) to 0.9 per 1,000 patient-days (interven-
to one medical and one surgical unit randomized tion). Results indicated that 2,580 patients per
to usual care. The study units were selected based group—a total of 10,320 patients—were needed
on similar patient admission diagnoses and inci- to power the study, per the typical settings of α
dence of NV-HAP as evaluated over the preceding = 0.05 and power = 0.8 (α represents the proba-
12 months. Unit randomization was done by sim- bility of finding significance where there is none;
ple, blind drawing from a container. The medical power represents true significance).29
intervention and control units had 49 and 38 Approval for the study was obtained from the
beds, respectively. The surgical intervention unit organization’s institutional review board prior
ajn@wolterskluwer.com AJN ▼ June 2021 ▼ Vol. 121, No. 6 25to data collection. Signed consent was waived The kits used in the study were provided by
because the intervention presented minimal risk to Medline Industries (Northfield, IL). They were
participants. chosen because they were the only kits available
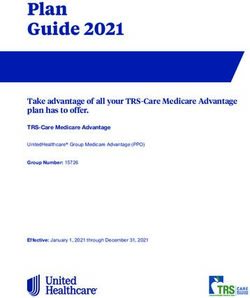
The intervention consisted of the implemen- that contained all the products in the protocol.
tation of a standardized oral care protocol (see (Organizations can also follow the protocol’s rec-
Figure 1) and targeted education. The protocol, ommendations by assembling kits using individual
which was first developed for an earlier study,30 products from a variety of manufacturers.) Unit-
was adapted by two of us (DB and KKG) for this level team members (nurses and nursing assistants)
study. It was approved by the American Dental were instructed to perform daily oral assessments to
Association (ADA) Board of Trustees in 2017. ensure that patients had the correct supplies based
Before implementation, all nurses and nursing on their status, which could change. They were
assistants on the intervention units received edu- asked to document both these assessments and oral
cation on the protocol. In individual and group care in the electronic health record (EHR).
sessions, the investigators covered topics that On the control units, all unit-level team mem-
included the importance of oral care, methods of bers received refresher training on the hospital’s
delivery, and assessment of patient needs. Dem- usual oral care protocol and required documenta-
onstrations of new oral care techniques and prod- tion. No special oral care supplies were provided,
ucts used in the study were given, and regularly but team members were reminded to document all
scheduled coaching as well as reinforcement when oral care performed. In keeping with usual care,
needed were offered throughout the study period. patients were not reminded to brush their teeth or
Patients and family members on the interven- educated on the importance of doing so. Assistance
tion units were educated through flyers, signage, with oral care was provided as needed. No attempt
teaching that emphasized the importance of oral was made to inform team members on the control
care, and demonstrations of oral care techniques units of the procedures and materials used on the
and products. intervention units.
Determining NV-HAP incidence. All 8,713
patients discharged from the four study units during
the study period (a number that includes all those
who died) were screened for inclusion. Those who
weren’t at least 18 years of age were excluded.
NV-HAP prevention is of Cases of pneumonia were then identified using the
International Classification of Diseases, Tenth Revi-
paramount importance to sion (ICD-10) codes, as documented in the hospi-
tal’s electronic data warehouse. Patients without
such codes were excluded, as were those who had
patient safety. been hospitalized less than 48 hours, received a
pneumonia diagnosis within 48 hours of admission,
been extubated within 48 hours of pneumonia diag-
nosis, or been present on a study unit less than 48
hours before such diagnosis. From the remaining
The intervention was designed to align with the cases, NV-HAP was confirmed using the CDC’s cri-
ADA-approved protocol’s recommendations. It teria for pneumonia (which involve radiologic
made use of a kit that included a high-quality soft- determination, cultures when available, and symp-
bristle toothbrush, plaque-removing toothpaste, a tom assessment).31
nonalcohol-based mouthwash, and lip and mouth Data collection. After staff education on the new
moisturizers applied as needed. Target frequency of oral care protocol was completed, there was a
oral care was set at four times a day.30 The fre- 30-day run-in period (September 1 through Septem-
quency and timing were similar whether the patient ber 30, 2018) to monitor compliance and provide
was on a regular meal schedule or not. Suction additional training as needed. Data collection took
toothbrush kits were used with patients who were place over a 12-month period, from October 1,
at risk for aspiration or unable to perform their 2018, through September 30, 2019.
own oral care. Patients with dentures were given For all patients in the study, frequency of oral
special kits that included a high-quality soft-bristle care was recorded by nurses and nursing assistants
toothbrush, denture adhesive cream, and a denture in the EHR. Because the EHR did not permit docu-
cup and sanitizing tablets for nightly cleaning. mentation at the level of detail needed to track the
Every kit came with standard directions for use and new oral care protocol, randomized audits were
additional patient education materials developed conducted weekly via direct patient interviews on
for the study. all study units. These took place in real time with
26 AJN ▼ June 2021 ▼ Vol. 121, No. 6 ajnonline.comFigure 1. The Standardized Oral Care Protocol
• Complete oral care assessment includes a swallow assessment • Document oral care in the patient record.
first. Determine if a bite block is required and if additional • Disposable oral swabs do not replace tooth brushing. They are for
swallow assessment is required. comfort care, one-time use only; do not leave oral swabs soaking in
• Always use Personal Protective Equipment (PPE) when assisting a cup for reuse later.
patients with mouth care and wash your hands before and after • Maintain adequate oral hydration when possible to maximize
the procedure per policy. salivary flow.
EQUIPMENT PROCEDURE
Self-care and • Soft toothbrush, ADA approved 1. Set patient up at sink or in bed with all equipment.
staff-assist. • Toothpaste and mouth rinse, ADA approved 2. Instruct patient to brush teeth for 1-2 minutes.
Able to expectorate • Mouth moisturizer prn or mouthwash 3. Use mouth rinse twice a day, swish for 20 to 30 seconds.
(spit) • Dental floss or interdental cleansers (optional) 4. If patient is able and supply is available, use floss or
• Lip balm (optional) interdental cleansers.
5. May moisturize interior of mouth and lips using an oral
FREQUENCY swab prn.
6. Discard disposable equipment/swab in appropriate
• After each meal and before bedtime. receptacle.
• If patient is NPO, oral care should be done 2-4 times daily.
EQUIPMENT PROCEDURE
• Suction toothbrush with oral cleaning solution packet 1. Moisten suction or regular toothbrush as noted.
Dependent for (as appropriate and available) 2. Assist the patient to brush all surfaces of the
oral care. • Soft toothbrush moistened with clean tap water or teeth until clean (1-2 minutes).
Not able to alcohol-free mouthwash 3. Suction debris from mouth.
expectorate (spit). • Mouth moisturizer prn 4. Apply mouth moisturizer using an oral swab, to
At risk for • Dental floss or interdental cleansers (optional) the interior of the oral cavity and apply lip balm.
aspiration. • Lip balm (optional) 5. Discard disposable equipment in appropriate
receptacle.
FREQUENCY
• After each meal and before bedtime.
• If patient is NPO, oral care should be done 2-4 times daily.
EQUIPMENT PROCEDURE
Dependent on • Suction toothbrush/ oral swab 1. Provide suction prn to remove oropharyngeal secretions that can
• Oral cleansing solution migrate down the tube and settle on top of the cuff.
oral care.
• Mouth moisturizer 2. Obtain suction toothbrush/oral swab and moisten with
Patient on a
• May consider chlorhexidine oral rinse oral cleansing solution.
ventilator.
per hospital policy — current studies are 3. Connection suction toothbrush to continuous suctions.
unclear as to benefit and harm 4. If chlorhexidine is used, remove the debris and cleanse the gums,
tongue, and inside of cheeks with the solution-saturated oral swab.
FREQUENCY 5. Suction debris from mouth
6. Apply moisturizer using oral swab to the interior of the oral cavity
• Every four hours and pm to remove oral and lips.
debris. 7. Discard disposable equipment/swab in appropriate receptacle.
EQUIPMENT PROCEDURE
Denture care or • Denture cup, labeled 1. After removing dentures, place in a labeled denture cup.
patients with • Denture brush is preferred when 2. Brush the palate, buccal surfaces, gums, and tongue with the toothbrush
available, otherwise soft toothbrush or swab.
no teeth.
• ADA approved denture cleanser (for soaking) 3. Patient can swish and spit mouthwash, or use oral swab to apply moisturizer.
Before the patient goes
to sleep, remove and • 2 oral swabs 4. Line the sink with paper towel and add water to cushion the dentures in
clean dentures and place • Denture adhesive (optional) case you drop them. Carefully brush dentures with warm tap water.
them in a denture • Mouth rinse Do not use toothpaste as this may scratch the surface of the dentures.
cleansing solution • Mouth moisturizer prn or mouthwash 5. Clean and dry equipment and return to patient’s bedside table.
once daily. 6. Assist patient in inserting dentures into mouth.
FREQUENCY 7. If patient needs denture adhesive to hold firmly in place, follow
manufacture directions.
• Dentures are removed for cleaning at
8. Soak dentures in a denture cleanser in the denture cup at bedtime.
bedtime. Remove dentures when sleeping
ADA = American Dental Association; NPO = nil per os, or nothing by mouth.
Note: This is the hospital-wide protocol used at the study site. For the purposes of this study, the orange section on care for ventilated patients was not relevant.
Image courtesy of the authors.
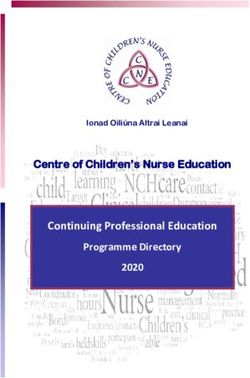
ajn@wolterskluwer.com AJN ▼ June 2021 ▼ Vol. 121, No. 6 27an average of 63% of patients on a unit, depend- group (10 patients). See Figure 2 for a flow dia-
ing on census. An investigator (AM) asked patients gram describing our process for obtaining this
and family members about their experience in the final patient sample.
last 24 hours: the number of times they’d com- Regarding age, there were small but significant
pleted oral care, the level of assistance needed, and differences between both the medical and surgical
whether they’d used their own oral care products or control versus the intervention groups. Patients
those provided by the hospital. in the medical and surgical control groups had
Data analysis. All data were entered into an a mean age of 60.9 and 62.6 years, respectively.
Excel spreadsheet and were audited for accuracy by Those in the medical and surgical intervention
two clinical research coordinators (AM and another groups had a mean age of 62 and 64.9 years,
coordinator at the hospital) and by the research respectively. Regarding length of stay, there was
team. Data were then imported into IBM SPSS, ver- a significant difference between the surgical con-
sion 26, for analyses. The NV-HAP incidence rate trol group (mean, 5.3 days) and the surgical inter-
per 1,000 patient-days on the intervention units was vention group (mean, 7.4 days). Regarding race,
compared with that on the control units. A χ2 anal- there were no significant differences between the
ysis was used to determine the relationship between medical control and intervention units. On the
units, and the Wald test for logistic regression was surgical units, there were significantly more white
calculated to obtain the odds ratio and confidence patients on the intervention unit (64.5%) than on
intervals between groups. Means comparisons of the control unit (50.1%) and significantly more
continuous variables (age, length of stay) across the Asian patients on the control unit (27.1%) than
control and intervention groups were done using on the intervention unit (12.2%). Demographic
the independent samples t test. The Mann-Whit- data for the full sample are provided in Table 1.
ney U test was used to test for group differences of Deidentified demographic and general out-
categorical variables (gender, race). The Cramér V comes data were retrieved for the 39 identified
effect size was calculated to assess the strength of NV-HAP patients. Demographic data included
association between categorical variables. Monthly age, gender, length of stay, and hospital day of
tracking of NV-HAP cases, compliance with oral NV-HAP onset. Outcomes data included sepsis
care practice standards, and pneumonia readmis- diagnosis postadmission, unplanned ICU transfer,
sion rates on all study units were summarized using 30-day readmission, and mortality. For details, see
descriptive statistics to compare the control and Table 2.
interventional units. For all analyses, statistical Primary outcome. To determine the effective-
significance was set at P ≤ 0.05. ness of a universal, standardized oral care proto-
col in preventing the development of NV-HAP, we
looked at the incidence rate of NV-HAP per 1,000
patient-days. Logistic regression revealed a signifi-
Improved oral care was cant difference between the medical control and
intervention groups. Patients on the medical con-
trol unit were 7.1 times more likely to develop
associated with NV-HAP NV-HAP than those on the medical intervention
unit. The Cramér V effect size was 0.52, indica-
reductions. tive of a moderate association between being on a
control unit and developing NV-HAP. But the dif-
ference between the surgical control and interven-
tion groups did not reach significance. For all
units, the NV-HAP incidence rate per 1,000
RESULTS patient-days and the percentage by which this
Sample. Of the 8,713 patients initially screened, decreased are shown in Table 3.
four were excluded because they were under 18 The initial power analysis indicated a requisite
years of age, leaving a total of 8,709 patients. Dis- sample size of 2,580 patients per group, for a total
tribution across the study units was as follows: of 10,320 patients. While none of the four groups
medical control, 2,075 patients; surgical con- reached a sample size of 2,580, post hoc power
trol, 2,088 patients; medical intervention, 2,709 analyses of the medical control versus the medical
patients; surgical intervention, 1,837 patients. All intervention units revealed a moderate Cramér V
8,709 patients were evaluated for the presence of effect size of 0.54 and an actual power of 0.99.
NV-HAP using the criteria described above. At However, such analyses of the surgical control ver-
the end of data collection, nearly three times as sus the surgical intervention units revealed a much
many NV-HAP cases had been identified in the smaller Cramér V effect size of 0.02 and a lower
control group (29 patients) as in the intervention power of 0.61.
28 AJN ▼ June 2021 ▼ Vol. 121, No. 6 ajnonline.comFigure 2. CONSORT Flow Diagram: Initial Screening to Final Identified NV-HAP Cases
Patients screened
(n = 8,709)
Intervention Control
(n = 4,546) (n = 4,163)
Excluded (n = 4,127) Excluded (n = 3,735)
• No ICD-10 PNA code • No ICD-10 PNA code
Had ICD-10 PNA code Had ICD-10 PNA code
(n = 419) (n = 428)
Excluded (n = 367) Excluded (n = 368)
• < 48 hrs LOS (n = 24) • < 48 hrs LOS (n = 31)
• PNA on admission (n = 327) • PNA on admission (n = 325)
• < 48 hrs postextubation (n = 16) • < 48 hrs postextubation (n = 12)
Included (n = 52) Included (n = 60)
Excluded (n = 29) Excluded (n = 20)
• < 48 hrs before PNA diagnosis • < 48 hrs before PNA diagnosis
PNA diagnosis on PNA diagnosis on
study unit (n = 23) study unit (n = 40)
Met CDC criteria (n = 10) Met CDC criteria (n = 29)
Surgical Medical Surgical Medical
(n = 7) (n = 3) (n = 13) (n = 16)
CDC = Centers for Disease Control and Prevention; CONSORT = Consolidated Standards of Reporting Trials; ICD-10 = International Classification of
Diseases, Tenth Revision; LOS = length of stay; PNA = pneumonia.
ajn@wolterskluwer.com AJN ▼ June 2021 ▼ Vol. 121, No. 6 29Table 1. Patient Demographics (N = 8,709) by Unit
Medical Surgical
Control Intervention Control Intervention
Variable (n = 2,075) (n = 2,709) P (n = 2,088) (n = 1,837) P
Age, mean (SD), years 60.9 (17.6) 62 (17.7) 0.03 62.6 (16.3) 64.9 (13) < 0.001
LOS, mean (SD), days 5.5 (6.7) 5.4 (6.5) 0.43 5.3 (5.5) 7.4 (6.9) < 0.001
Gender, No. (%)
Female 983 (47.4) 1,357 (50.1) 0.74 965 (46.2) 682 (37.1) 0.46
Male 1,092 (52.6) 1,352 (49.9) 1,123 (53.8) 1,155 (62.9)
Race, No. (%) a
White 969 (46.7) 1,237 (45.7) 0.28 1,047 (50.1) 1,185 (64.5) < 0.001
Asian 18 (0.9) 37 (1.4) 21 (1) 19 (1)
Black or African 668 (32.2) 854 (31.5) 565 (27.1) 224 (12.2)
American
Other 410 (19.8) 567 (20.9) 438 (21) 403 (21.9)
LOS = length of stay.
a
Percentages are based on total number per unit. Some data were missing; thus, not all columns sum to 100%.
Table 2. Demographic and Outcomes Data for NV-HAP Patients (n = 39)
Medical Surgical
Control Intervention Control Intervention
Variable (n =16) (n = 3) (n = 13) (n = 7)
Age, years
Mean (SD) 61.8 (13.3) 64 (5) 65.5 (20) 70.4 (12.5)
Median 63.5 64 67 73
Gender, No. (%)
Female 9 (56.2) 2 (66.7) 6 (46.2) 2 (28.6)
Male 7 (43.8) 1 (33.3) 7 (53.8) 5 (71.4)
LOS, days
Mean (SD) 17.1 (11.5) 16.7 (17.6) 11.6 (5) 24.2 (13.9)
Median 14.8 7.7 11 25
Hospital day of
NV-HAP onset
Mean (SD) 8 (6) 5 (1) 6 (2) 11 (5)
Median 6 5 5 12
Outcomes for All NV-HAP Cases, No. (%)
Sepsis Diagnosis Unplanned ICU 30-Day
Postadmission Transfer Readmission Mortality
Yes 8 (20.5) 10 (25.6) 5 (12.8) 2 (5.1)
No 31 (79.5) 29 (74.4) 34 (87.2) 37 (94.9)
LOS = length of stay; NV-HAP = nonventilator hospital-acquired pneumonia.
30 AJN ▼ June 2021 ▼ Vol. 121, No. 6 ajnonline.comTable 3. NV-HAP Rates and χ2 Results by Group
NV-HAP
Incidence Rate per
Treatment Group No Yes Total 1,000 Patient-Days
Medical Control, No. (%) 2,059 (99.2) 16 (0.8) 2,075 1.40
Medical Intervention, No. (%) 2,706 (99.9) 3 (0.1)a 2,709 0.21
Total 4,765 19 4,784 −85 (% difference)
Surgical Control, No. (%) 2,075 (99.4) 13 (0.6) 2,088 1.17
Surgical Intervention, No. (%) 1,830 (99.6) 7 (0.4)b 1,837 0.51
Total 3,905 20 3,925 −56 (% difference)
CI = confidence interval; NV-HAP = nonventilator hospital-acquired pneumonia; OR = odds ratio.
a
OR for medical control vs. medical intervention units (OR: 7.1; 95% CI, 2.01-24.1, P = 0.002).
b
OR for surgical control vs. surgical intervention units (OR: 1.6; 95% CI, 0.65-4.1, P = 0.29).
Table 4. Oral Care Frequency and Type Provided
Frequency of Daily Oral Care per Month
Medical Units Surgical Units
Control, range (mean) 0.86 –1.03 (0.95) 0.9 –1.4 (1.18)
Intervention, range (mean) 1.28 – 2.9 (2.25) 1.19 – 2.3 (2.02)
% Difference +135 a
+70 a
Type of Oral Care Provided, % of Patients
Required some Required total assistance and
Independent assistance use of suction toothbrush
Medical intervention 40 39 20
Medical control 39 40 22
Surgical intervention 55 37 7
Surgical control 63 30 6
a
P ≤ 0.05.
While our goal of achieving an oral care fre- daily oral care frequency improved significantly on
quency of four times daily wasn’t met on any of the intervention units, reaching up to 2.9 times per
the study units, the frequency was significantly day on the medical intervention unit. Although this
higher on both the intervention units compared didn’t meet the target level, improved oral care was
with the control units. On the medical units, the associated with NV-HAP reductions of 85% on the
intervention unit increased the daily oral care medical intervention unit and 56% on the surgical
frequency by 135% compared with the control intervention unit. This finding supports previous
unit. On the surgical units, the intervention unit research that showed a positive relationship
increased the frequency by 70% compared with between increased frequency of daily oral care and
the control unit. For more details on oral care NV-HAP incidence reduction.23
frequency and types of oral care provided, see Studies of implementation science can involve
Table 4. a variety of contextual factors that aren’t specif-
ically related to the intervention itself, including
DISCUSSION nursing culture and leadership, workload, admin-
This study tested the impact of enhanced oral care istrative responsiveness and support, and level of
on NV-HAP prevention in patients on medical and resistance to change.32-34 We found this to be so in
surgical units. Over the course of the study, the our study. The medical intervention unit embraced
ajn@wolterskluwer.com AJN ▼ June 2021 ▼ Vol. 121, No. 6 31the oral care intervention and provided more fre- vention efforts can be substantial.21 But this requires
quent oral care (135% more than control) com- a sizable initial investment in such products, which
pared with the surgical intervention unit (70% will present a roadblock for many hospitals. In
more than control)—even though the medical unit short, changing the clinical mindset will take time,
had less staffing. Also, more patients on the med- sustained effort, ongoing involvement of nurses and
ical than the surgical intervention unit were iden- nursing assistants, interdisciplinary collaboration,
tified as partially or entirely dependent on assis- and buy-in from nursing and hospital leadership.
tance for oral care (59% versus 44%). There was Although we collected demographic data on
a general expectation that patients could perform age, gender, and race, the small number of NV-
oral self-care in the first days after cardiovascu- HAP cases did not permit analyses to assess these
lar surgery, and this may have accounted for the data in relation to findings. The influence of age,
lower frequency of oral care on the surgical inter- gender, and race on NV-HAP incidence represents
vention unit compared with the medical interven- an area for further study. The additional data we
tion unit. The surgical intervention unit also had a collected on the development of postadmission
significantly higher mean length of stay and mean sepsis, unplanned ICU transfer, 30-day readmis-
patient age compared with the surgical control sion, and mortality can help to inform future
unit; both variables are known risk factors for research on morbidity and mortality associated
hospital-acquired infection. with NV-HAP.
Findings suggest that primary source control through improved
oral care may be important for NV-HAP prevention.
Post hoc power analyses showed that the surgical Limitations. Although units were selected as
units were underpowered to answer the research matched pairs for their similarity in diagnoses and
question, and the effect size was very small. Even required care levels, we could not check for cluster
with 12 months of data collection, we were unable control effects on any of the units. The ideal frequency
to achieve the full sample of patients. of oral care for NV-HAP prevention is unknown. In
Despite the use of multiple means of education, this study, accuracy in tracking such frequency was a
coaching at the point of care, readily available sup- challenge, as nursing staff didn’t always fully docu-
plies, and ongoing reports during weekly huddles, ment each oral care event and may have recorded self-
oral care frequency remained lower than our target care that didn’t actually occur. Moreover, because oral
level. This is consistent with the findings of other care was performed by both patients and staff, we
researchers exploring the impact of oral care on could not control for its quality. Hospitals are
NV-HAP rates and the challenges of improving dynamic institutions and it’s not always possible to
such care.21, 23, 35, 36 understand all the potential influencers on interven-
As oral care is solely a nursing intervention— tions and controls. Therefore, it’s possible that other
and one critical to patient safety—nurses are hospital initiatives directly or indirectly affected the
well positioned to have a strong impact in this oral care intervention and NV-HAP outcomes. Lastly,
area. Nursing assistants are also vital to oral care this study was conducted in a single hospital and find-
improvement, as they often provide much of this ings should be interpreted in that context.
basic care. In order to realize the importance of
the nursing role in NV-HAP prevention, we must CONCLUSIONS
change the mindset of nurses and other health care Critically ill hospitalized patients are at high risk
providers from seeing oral care as a comfort mea- for NV-HAP and the associated increased morbid-
sure to recognizing oral care as a therapeutic inter- ity and mortality. NV-HAP prevention is of par-
vention and oral care products as therapeutic amount importance to patient safety. Our study
devices. From an organizational perspective, there findings suggest that primary source control
is evidence that the return on investment in higher- through improved oral care may be important for
quality oral care products for use in NV-HAP pre- NV-HAP prevention. Developing and implementing
32 AJN ▼ June 2021 ▼ Vol. 121, No. 6 ajnonline.comunit undergoing mechanical ventilation. Clin Infect Dis
effective strategies that foster frequent, consistent 2008;47(12):1562-70.
oral care for all inpatients warrants further study. 14. Perry SE, et al. The association between oral bacteria, the
Moreover, it’s not yet known what degree and fre- cough reflex and pneumonia in patients with acute stroke
quency of oral care is necessary to favorably influ- and suspected dysphagia. J Oral Rehabil 2020;47(3):386-94.
15. Abele-Horn M, et al. Decrease in nosocomial pneumonia in
ence changes in the oral microbiome during acute ventilated patients by selective oropharyngeal decontamina-
care hospitalization. Questions regarding ideal oral tion (SOD). Intensive Care Med 1997;23(2):187-95.
care frequency, best practices, and consistent imple- 16. Kitsios GD, et al. Dysbiosis in the intensive care unit:
mentation would best be addressed through large microbiome science coming to the bedside. J Crit Care
2017;38:84-91.
randomized controlled trials. ▼ 17. Didilescu AC, et al. Respiratory pathogens in dental plaque
of hospitalized patients with chronic lung diseases. Clin Oral
Karen K. Giuliano is an associate professor at the College of Investig 2005;9(3):141-7.
Nursing and the Institute for Applied Life Sciences, University of 18. Gleeson K, et al. Quantitative aspiration during sleep in nor-
Massachusetts Amherst. Daleen Penoyer is the director of the Center mal subjects. Chest 1997;111(5):1266-72.
for Nursing Research and Advanced Nursing Practice, Orlando
19. Huxley EJ, et al. Pharyngeal aspiration in normal adults
Health, Orlando, FL. Aurea Middleton is the research coordina- and patients with depressed consciousness. Am J Med
tor for Orlando Health’s Center for Nursing Research. Dian Baker 1978;64(4):564-8.
is a professor at the School of Nursing, California State University,
20. Ewan VC, et al. Dental and microbiological risk factors
Sacramento. Financial support for this study was provided by Med-
for hospital-acquired pneumonia in non-ventilated older
line Industries (which supplied the kits used) and Orlando Health. patients. PLoS One 2015;10(4):e0123622.
Baker and Giuliano have also created a CE program on NV-HAP
sponsored by Medline. An intervention toolkit is available from the 21. Quinn B, et al. Basic nursing care to prevent nonven-
tilator hospital-acquired pneumonia. J Nurs Scholarsh
authors. The authors acknowledge Joohyun Chung for her guidance
2014;46(1):11-9.
and review of the statistical approach and analyses. Contact author:
Karen K. Giuliano, kkgiuliano96@gmail.com. The authors have dis- 22. Cassidy MR, et al. The I COUGH multidisciplinary periop-
closed no other potential conflicts of interest, financial or otherwise. erative pulmonary care program: one decade of experience.
Jt Comm J Qual Patient Saf 2020;46(5):241-9.
23. McNally E, et al. Oral care clinical trial to reduce non-
REFERENCES intensive care unit, hospital-acquired pneumonia: lessons for
1. Magill SS, et al. Changes in prevalence of health care- future research. J Healthc Qual 2019;41(1):1-9.
associated infections in U.S. hospitals. N Engl J Med 24. Munro S, Baker D. Reducing missed oral care opportunities
2018;379(18):1732-44. to prevent non-ventilator associated hospital acquired pneu-
2. Cassini A, et al. Burden of six healthcare-associated monia at the Department of Veterans Affairs. Appl Nurs Res
infections on European population health: estimating 2018;44:48-53.
incidence-based disability-adjusted life years through a 25. Munro S, et al. Implementation and dissemination of a
population prevalence-based modelling study. PLoS Med Department of Veterans Affairs oral care initiative to prevent
2016;13(10):e1002150. hospital-acquired pneumonia among nonventilated patients.
3. Suetens C, et al. Prevalence of healthcare-associated infec- Nurs Adm Q 2018;42(4):363-72.
tions, estimated incidence and composite antimicrobial 26. Pássaro L, et al. Prevention of hospital-acquired pneumo-
resistance index in acute care hospitals and long-term care nia in non-ventilated adult patients: a narrative review.
facilities: results from two European point prevalence sur- Antimicrob Resist Infect Control 2016;5:43.
veys, 2016 to 2017. Euro Surveill 2018;23(46).
27. Lacerna CC, et al. A successful program preventing non-
4. Baker D, Quinn B. Hospital acquired pneumonia prevention ventilator hospital-acquired pneumonia in a large hospital
initiative-2: incidence of nonventilator hospital-acquired system. Infect Control Hosp Epidemiol 2020;41(5):547-52.
pneumonia in the United States. Am J Infect Control
28. Giuliano KK, Baker D. Sepsis in the context of nonventilator
2018;46(1):2-7.
hospital-acquired pneumonia. Am J Crit Care 2020;29(1):
5. Baker D, et al. Sustaining quality improvement: long-term 9-14.
reduction of nonventilator hospital-acquired pneumonia. J
29. Sun S, et al. A comprehensive review of effect size reporting
Nurs Care Qual 2019;34(3):223-9.
and interpreting practices in academic journals in education
6. Giuliano KK, et al. The epidemiology of nonventilator hos- and psychology. J Educ Psychol 2010;102(4):989-1004.
pital-acquired pneumonia in the United States. Am J Infect 30. Quinn B, Baker DL. Comprehensive oral care helps prevent
Control 2018;46(3):322-7. hospital-acquired nonventilator pneumonia. Am Nurse
7. Micek ST, et al. A case-control study assessing the impact of Today 2015;10(3):18-23.
nonventilated hospital-acquired pneumonia on patient out- 31. Tablan OC, et al. Guidelines for preventing health-care–
comes. Chest 2016;150(5):1008-14. associated pneumonia, 2003: recommendations of CDC
8. Gomes-Filho IS, et al. Respiratory disease and the role of and the Healthcare Infection Control Practices Advisory
oral bacteria. J Oral Microbiol 2010;2. Committee. MMWR Recomm Rep 2004;53(RR-3):1-36.
9. Scannapieco FA. The oral microbiome: its role in health 32. Boehm LM, et al. Implementation science training and
and in oral and systemic infections. Clin Microbiol Newsl resources for nurses and nurse scientists. J Nurs Scholarsh
2013;35(20):163-9. 2020;52(1):47-54.
10. Scannapieco FA, Shay K. Oral health disparities in older 33. Powell BJ, et al. Methods to improve the selection and tai-
adults: oral bacteria, inflammation, and aspiration pneumo- loring of implementation strategies. J Behav Health Serv Res
nia. Dent Clin North Am 2014;58(4):771-82. 2017;44(2):177-94.
11. Di Pasquale M, et al. Non-intensive care unit acquired 34. Shoemaker SJ. Transforming into a patient-centered medi-
pneumonia: a new clinical entity? Int J Mol Sci 2016; cal home: understanding facilitators, barriers and context
17(3):287. from a synthesis of implementation studies. Implement Sci
12. Sopena N, et al. Risk factors for hospital-acquired pneumo- 2015;10(Suppl 1):A68.
nia outside the intensive care unit: a case-control study. Am 35. Ferguson C, et al. Exploring nursing and allied health per-
J Infect Control 2014;42(1):38-42. spectives of quality oral care after stroke: a qualitative study.
13. Heo SM, et al. Genetic relationships between respiratory Eur J Cardiovasc Nurs 2020;19(6):505-12.
pathogens isolated from dental plaque and bronchoal- 36. Warren C, et al. A nurse-driven oral care protocol to reduce
veolar lavage fluid from patients in the intensive care hospital-acquired pneumonia. Am J Nurs 2019;119(2):44-51.
ajn@wolterskluwer.com AJN ▼ June 2021 ▼ Vol. 121, No. 6 33You can also read