Nuevas dianas terapéuticas del Cáncer de Mama - Joaquín Gavilá Gregori Servicio de Oncología Médica
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Nuevas dianas terapéuticas
del Cáncer de Mama
Joaquín Gavilá Gregori
Servicio de Oncología Médica
06 de mayo de 2021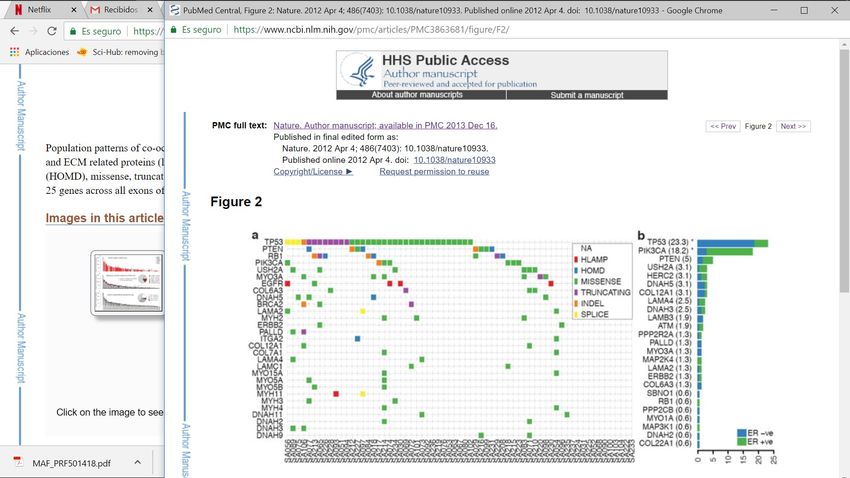
La complejidad del Cáncer de Mama
CM a día de hoy Tumor y Microambiente
HER2 +3 HER2 ISH+
Tumor
Infiltrating
mRNA microRNA Protein
Lymphocytes
ER-positive ER-negative (TILs)
Courtesy of Dr. Pedro Fernández DNA Copy Number DNA Methylation DNA Mutations
TCGA Nature 2012
Cortesía de A. Prat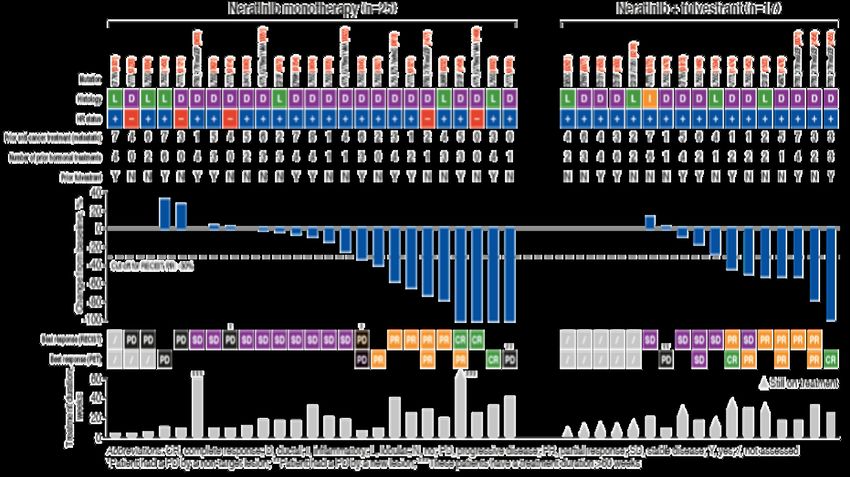
Medicina de Precisión: Marcadores de estratificación
Biomarker+
100% response/benefit
e r
ar k
io m
b
e al
Id
St r Biomarker+
a
bio tifica
ma tion
rke 44% response/benefit
r
25%
response/benefit
Cortesía del Dr. Aleix Prat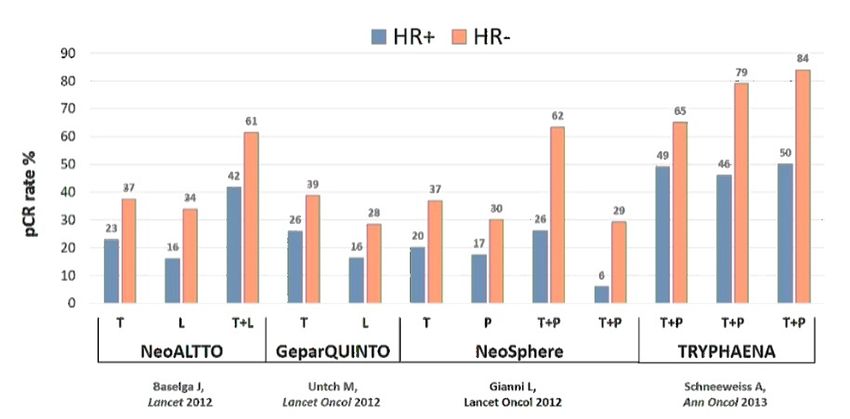
Medicina de Precisión: Marcadores de estratificación
Biomarker+
100% response/benefit
r ker
io ma
alb
Id e
St r Biomarker+
atif
bio icati
m a on
r
#1 ker 44% response/benefit
Biomarker+
St r
a
bio tifica
25% ma tion
rke
100%
response/benefit #2 r response/benefit
Cortesía del Dr. Aleix Prat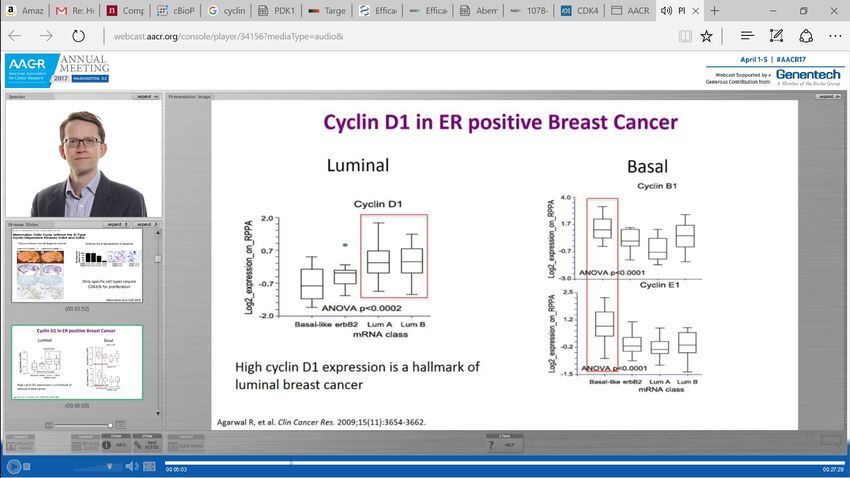
Enfermedad Triple Negativa ¿un verdadero desafío?
CM Triple negativo… ¿un verdadero desafío?
Imágenes Cortesía de Dr. Francisco Gozlabo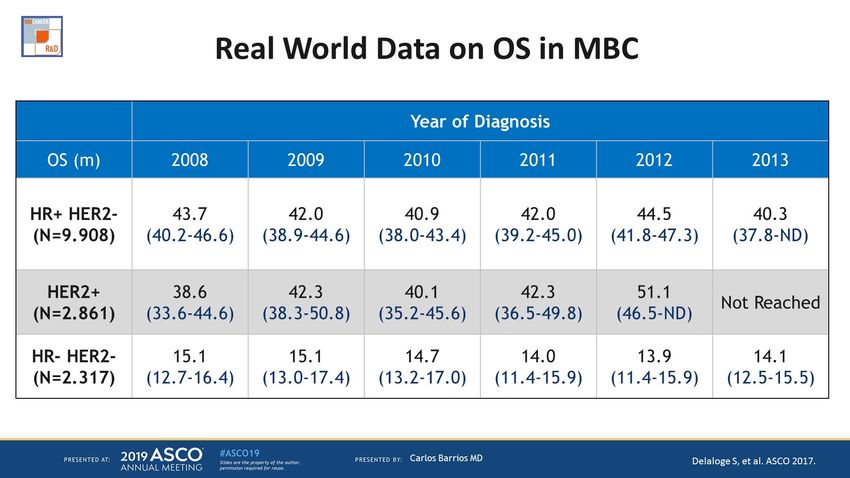
CM Triple negativo… un verdadero desafío
NO HEMOS SIDO CAPACES DE CAMBIAR SU HISTORIA
Es más agresivo que otros subtipos de CM
- Recidivas precoces (años 1-3 tras el diagnóstico)
- Frecuente diseminación visceral
Dent R et al. Clin Cancer Res 2007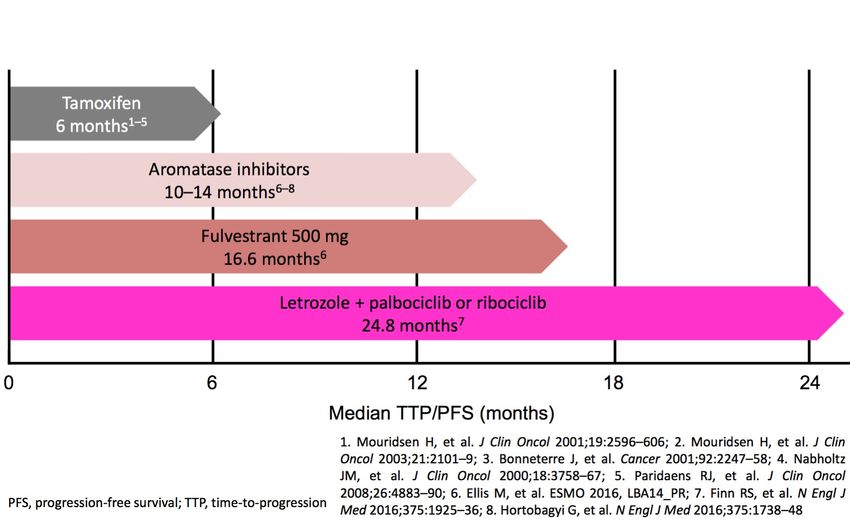
CM Triple negativo… un verdadero desafío
POR SU HETEROGENEIDAD
Bianchini. G, et al. Nat Rev Clin Oncol 2016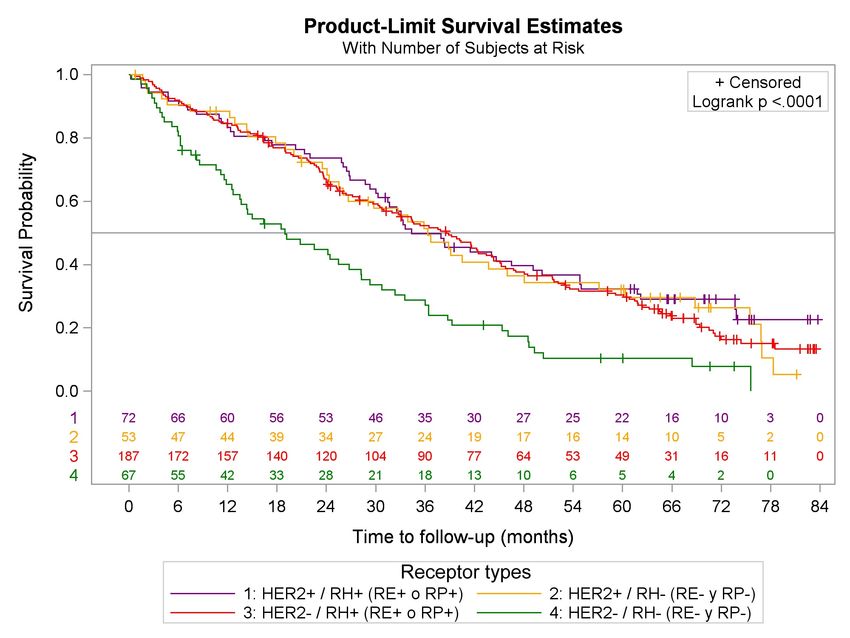
CM Triple negativo… un verdadero desafío
POR SU HETEROGENEIDAD
Bianchini. G, et al. Nat Rev Clin Oncol 2016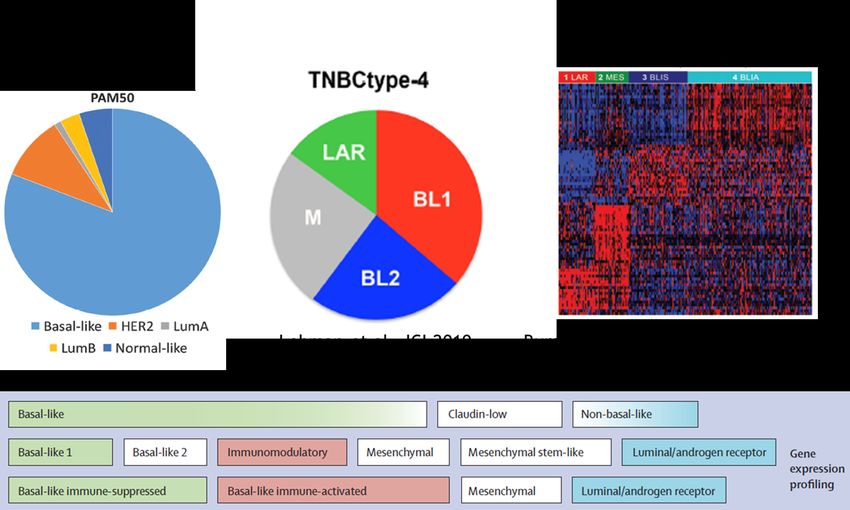
CM Triple negativo… un verdadero desafío
POR AUSENCIA DE DIANA TERAPEUTICA
Cáncer de Mama Triple Negativo
Diversas mutaciones activadoras, “not druggables”
Shah G, et al. Nature 2012Mayo 2021
Cáncer de Mama Triple Negativo
QuimioterapiaCM Metastásico Triple negativo…
Supervivencia similar al Cáncer de Pulmón
Overall Survival curves for the four tumour subtypes
HER2-/HR+ Median OS:
38.6 months
TN Median OS:
19.0 months
Garcia J et al. SABCS 2016¿Podremos estratificar el Cáncer de Mama Triple Negativo?
Cejalvo JM and Pascual T,et al. Cancer Treatment Rev 2018¿Podremos estratificar el Cáncer de Mama Triple Negativo?
¿Cúantos CM TN tienen mutación en BRCA ½?
The majority of TNBC are BRCA1m and HR+ tumours are BRCA2m 1,2
TNBC patients1
~17%
have BRCA mutations
HR+ patients3
~6%
have BRCA mutations
BRCAm=BRCA mutation; TNBC=triple negative breast cancer; HR+=hormone receptor positive; ER+=oestrogen receptor positive
1. Engel C et al. BMC Cáncer 2018;18:265. 2. Aleskandarany M, et al. Breast Cancer Res Treat. 2015;150:81-90. 3. O’Shaughnessy et al. Breast Cancer Research 2020 22:114iPARP en CMM: Aprobación EMA y FDA
OlympiAD: progression free survival
EMBRACA: progression free survival
PFS = 8,6 vs 5,6 ms
PFS = 7 vs 4,21 ms
1. Litton et al N Eng J Med 2018;379:753-63; 2 Robson et al. N Engl J Med. 2017; 377:523-533;¿Inmunoterapia en CM Triple Negativo?
El CMTN es un candidato a la terapia Inmune
•Sin terapias dirigidas y Resistencia rápida a la QT
•Alta carga mutacional frente a otros subtipos
•Presencia de tumor- infiltrating lymphocytes (TILs) y correlación con
respuesta a QT y en otros tumores
•Mayor expresión de PD-L1
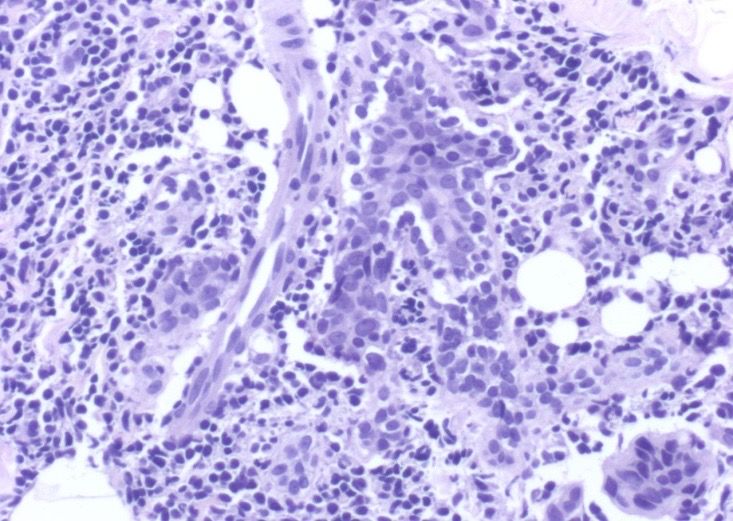
Alexandrov et al. Nature. 2013.Infiltrado Linfocitario en CM
La evaluación morfológica mediante hematoxilina-eosina en secciones tumorales
de los linfocitos infiltrantes de tumor (TIL) en el cáncer de mama está ganando
impulso como biomarcador inmunológico de gran relevancia clínica.
Intratumoral TIL:
direct contact to tumor cells.
Stromal TIL:
between the tumor cells.
LPBC (lymphocyte-predominant
breast cancer):
«more lymphocytes than tumor
cells» (≥60% TIL/≥50% TIL).
La metodología prevista es suficientemente detallada como
TLS (tertiary lymphoid structures): para ofrecer un punto de partida pragmático aplicado de
follicular aggregates outside of the manera uniforme y mejorar la consistencia y reproducibilidad
tumor. en la medición de TIL para futuros estudios.
Salgado et al. Ann Oncol. 2014; Dieci et al. Sem in Cancer Biol. 2018.TIL distribución según los diferentes tipos de CM
• For an effective immune response, activated effector T cells
must traffic to the tumour site and infiltrate the tumour1
• Primary TNBC tumours show increased levels of tumour-
infiltrating T cells compared with luminal subtypes2–4
• T cell infiltration in TNBC is associated with improved
prognosis for patients
• For each 10% increase in the level of stromal tumour-
infiltrating T cells:
Denkert et al. SABCS. 2016.TIL capacidad predictiva y pronóstica
La presencia de TIL alto se asocia a mejor pronóstico
Loi S, et al. J Clin Oncol. 2013. Loi S et al. Ann Oncol 2014TIL capacidad pronóstica en CM TN
• For an effective immune response, activated effector T cells
must traffic to the tumour site and infiltrate the tumour1
• Primary TNBC tumours show increased levels of tumour-
infiltrating T cells compared with luminal subtypes2–4
• T cell infiltration in TNBC is associated with improved prognosis
for patients
• For each 10% increase in the level of stromal tumour-
infiltrating T cells:
Park et al. ESMO. 2019.Impassion 130: Anti-PDL1 en CMM
Atezolizumab
+ nab-paclitaxel
• Metastatic or inoperable locally advanced
TNBC
• No prior therapy for advanced TNBC
R RECIST v1.1
– Prior (neo)adjuvant chemo allowed if Double blind; no crossover permitted
1:1
TFI ≥ 12 months PD or toxicity
• ECOG PS 0-1
Placebo
Stratification factors:
• Prior taxane use (yes vs no)
+ nab-paclitaxel
• Liver metastases (yes vs no)
• PD-L1 status on IC (positive [≥ 1%] vs negative [< 1%])
◆ Co-primary endpoints were PFS and OS in the ITT and PD-L1+ populations
Schmid P, ESMO 2018.Impassion 130: Beneficio en SG población PDL1+
100
Median OS, mo
90 Population HR (95% CI)
A + nab-P P + nab-P
80 25.0 18.0
PD-L1 IC+ a 0.71 (0.54, 0.93)
70 PD-L1 IC− 19.7 19.6 0.97 (0.78, 1.20)
60
OS (%)
50
40
30
20
A + nab-P (PD-L1+ n = 185)
10 P + nab-P (PD-L1+ n = 184)
A + nab-P (PD-L1− n = 266) 18.0 mo 25.0 mo
0 P + nab-P (PD-L1− n = 267) (13.6, 20.1) (19.6, 30.7)
3 6 9 18 21 24 27 30
0 12 15 33 36 39 42
Time (months)
Schmid P, ESMO 2018.Enfermedad HER2 positiva
Cambio en la historia natura del CMM HER2 positivo
Delalogue et al. ASCO. 2018.Trastuzumab (Herceptin)
Enfermedad HER2: Cambio en su historia natural
• Hasta la llegada de Trastuzumab SG en CM HER2+ era similar a CM TN
(SG=20 meses).
• Trastuzumab aumentó la SG a 31 meses.
• Con la llegada de nuevos agentes: Pertuzumab, TDM1, Lapatinib
• La SG prácticamente se ha duplicado.
Slamon D. NEJM 2001. Baselga J NEJM 2012. Swain S. NEJM 2015. Verma S NEJM 2014. Krop I. Lancet Oncol 2014. Giordano JCO 2014HER2 se une a with HER3 y activa el
crecimiento celular
HER2 HER3
Ligand-activated
HER2:HER3 dimer
P
P
P P
Phosphorylation of the HER3 intracellular domain by HER2
initiates a signalling cascade
Baselga, Swain. Nat Rev Cancer 2009;9:463–475; Yarden, Sliwkowski. Nat Rev Mol Cell Biol 2001;2:127–137;
Graus-Porta et al. EMBO J 1997;1647–1655; Tzahar et al. Mol Cell Biol 1996;16:5276–5287;
Lee-Hoeflich et al. Cancer Res 2008;68:5878–5887.Pertuzumab impide la unión de las proteínas HER2-HER3
HER2 HER3
Pertuzumab
Dimerisation
domain
1. Agus et al. Cancer Cell 2002;2:127–137; 2. Baselga. Cancer Cell 2002;2:93–95;
3. Citri et al. Exp Cell Res 2003;284:54–65. 4. Franklin et al. Cancer Cell 2004;5:317–328;
5. Hughes et al. Mol Cancer Ther 2009;8:1885–1892Trastuzumab y Pertuzumab actúan de modo diferente pero
complementario
Pertuzumab
Trastuzumab HER2
HER3
Dimerisation
domain
Subdomain IV
• Trastuzumab does not inhibit ligand- • Pertuzumab inhibits ligand-activated
activated HER2 dimerisation HER2 dimerisation
• Trastuzumab prevents HER2 activation by • Pertuzumab flags cells for destruction
by the immune system
extracellular domain shedding
• Pertuzumab suppresses multiple HER signalling
• Trastuzumab inhibits ligand-independent pathways, leading to a more comprehensive
HER2 signalling and flags cells for blockade of HER2-driven signalling
destruction by the immune system
Cho et al. Nature 2003;421:756–760; Fendly et al. Cancer Res 1990;50:1550–1558; Franklin et al. Cancer Cell 2004;5:317–328;
Nahta et al. Cancer Res 2004;64:2343–2346; Scheuer et al. Cancer Res 2009;69:9330–9336Secuencia actual del tratamiento CMM HER2 positivo
Swain S. NEJM 2015. Verma S NEJM 2014. Kropp I Lancet Oncol 2014. Giordano JCO 2014TDM-1= Caballo de Troya
T-DM1 se introduce en la célula y la destruye
T-DM1 binds to the HER2
protein on cancer cells
Receptor-T-DM1 complex is
Potent antimicrotubule
internalised into HER2-
agent is released once
positive cancer cell inside the HER2-positive
tumour cell
MOA = mode of actionNuevos Fármacos en Enfermedad HER2
Trastuzumab-Deruxtecan: nuevo anticuerpo conjugado
Trastuzumab deruxtecan is an ADC composed of 3 components: 1 Payload MOA:
topoisomerase I inhibitor
• A humanized anti-HER2 IgG1 mAb with the same
amino acid sequence as trastuzumab, covalently linked to 2 High potency of payload
• A topoisomerase I inhibitor payload, an exatecan derivative, via
• A tetrapeptide-based cleavable linker 3 High drug to antibody ratio ≈ 8
Humanized anti-HER2 Deruxtecan1,2
4 Payload with short systemic half-life
IgG1 mAb1-3
5 Stable linker-payload
Tetrapeptide-Based Cleavable Linker
6 Tumor-selective cleavable linker
Topoisomerase I Inhibitor payload
(DXd) 7 Membrane-permeable payload
The clinical relevance of these features is under investigation.
ADC, antibody-drug conjugate; MOA, mechanism of action.
1. Nakada T, et al. Chem Pharm Bull (Tokyo). 2019;67(3):173-185. 2. Ogitani Y, et al. Clin Cancer Res. 2016;22(20):5097-5108. 3. Trail PA, et al. Pharmacol Ther. 2018;181:126-142. 4. Ogitani Y, et al. Cancer Sci. 2016;107(7):1039-
1046.Trastuzumab-Deruxtecan: tasa de respuestas
40
n=168
Best % Change From Baseline in the Sum
of Diameters of Measurable Tumors
20
0
-20
-40
-60
-80
Confirmed ORR: 60.9%a
-100
(95% CI, 53.4%–68.0%)
11 CRs
The line at 20% indicates progressive disease; the line at −30% indicates partial response.
a
Includes all patients who received T-DXd 5.4 mg/kg (intent-to-treat analysis; N=184).
Krop I al, SABCS 2019 & NEJM 2019Trastuzumab-Deruxtecan: PFS
Modi S, et al. SABCS 2020¿Un nuevo subtipo de Cáncer de Mama?
… HER2 LOWDefinición Clínica HER2-Low
P Tarantino et al; JCO 2020¿Es frecuente el subtipo HER2-Low?
P Tarantino et al; JCO 2020Trastuzumab-Deruxtecan: tasa de respuestas en enfermedad HER2 Low
The confirmed ORR by independent central review was 20/54, 37.0% (95% CI, 24.3% to 51.3%)
S Modi et al. JCO 2020Medicina de Precisión: Marcadores de estratificación
Biomarker+
100% response/benefit
r ker
io ma
alb
Id e
St r Biomarker+
atif
bio icati
m a on
r
#1 ker 44% response/benefit
Biomarker+
St r
a
bio tifica
25% ma tion
rke
100%
response/benefit #2 r response/benefit
Cortesía del Dr. Aleix PratMedicina de Precisión: Marcadores de estratificación
The 3-year rate of
survival free from
invasive disease was
98.7% (95% CI, 97.6-99.8)
Stage I + HER2+ disease
Tolaney SM et al.NEJM 2015 and ASCO 2017Búsqueda de Biomarcadores en tumores HER2+
Expresión de RH se asocia a menor tasa de RCp
Baselga j et al. Lancet 2012; 379(9816):3633-40.
Uncht M et al. Lancet Oncol 2012; 13 (2):135-44.
Gianni L et al. Lancet Oncol 2016;17 (6):791-800.
Schneeweiss A et al. Ann Oncol 2013;24(9): 2278-84.Búsqueda de Biomarcadores en tumores HER2+
Expresión de RH se asocia a menor tasa de RCp
All samples HR+ samples HR-neg samples
N=151 N=77 N=74
2% 1.3% 2.7%
5.9%
14.6% 12.2%
28.6%
10.6%
66.9% 49.3% 85.1%
20.8%
Prat A, et al. SABCS 2016PATRICIA - SOLTI 1303
Fase II de la combinación de palbociclib y trastuzumab, con o sin letrozol, en
pacientes postmenopáusicas con cáncer de mama localmente avanzado o
metastásico HER2+ previamente tratado
PRIMARY
ENDPOINT
PFS at 6 months
PI: Eva CiruelosPATRICIA - SOLTI 1303
Fase II de la combinación de palbociclib y trastuzumab, con o sin letrozol, en
pacientes postmenopáusicas con cáncer de mama localmente avanzado o
metastásico HER2+ previamente tratado
Progression-free survival (PFS) Luminal
versus others
Hazard ratio, 0.4468
(95% CI; 0.196-1.016)
p=0.054
12.4
months
4.1 months
PI: Eva CiruelosPATRICIA 2
PRIMARY
ENDPOINT
PFS
PI: Eva CiruelosCáncer de Mama Luminal ¿Es importante la resistencia Hormonal?
50
Pan H, et al. N Eng J Med 2017¿Hemos cambiado la Historia Natural del CMM Luminal?
51
Delalogue S, et al. ASCO 2017.Enfermedad Luminal…¿Mal Pronóstico?
Median Overall p-
N: 2.102 patients N HR
Survival 95%CI value
ER[+] AI-SENS 869 33.2 (31.1 to 38.8) 1
ER[+] AI-RESIST 648 21.7 (20.4 to 23.9) 1.7 .0001
TNBC 585 18.3 (12.3 to 19.7) 2.1
52
Llombart-Cussac A, et al. The Breast 2014.Mecanismos de Resistencia Hormonal
• Adaptación de vías alternativas de transducción de señales
•
• Pérdida del RE (silenciamiento epigenético)
• Mutaciones / translocaciones del RE
• Alteración de los co-reguladores a nivel del complejo
transcripcional del RE
53
Clarke R, et al. Mol Cell Endocrinol 2015.Mecanismos de Resistencia Hormonal
ESR1
Mutations
AF2
Primary Secondary
Resistance Resistance
AF1
HER2
Activation
PI3K
Activation
Zilli M, et al. Biochim Biophys Acta 2009.Sobreexpresión de HER2: Resistencia Hormonal
55
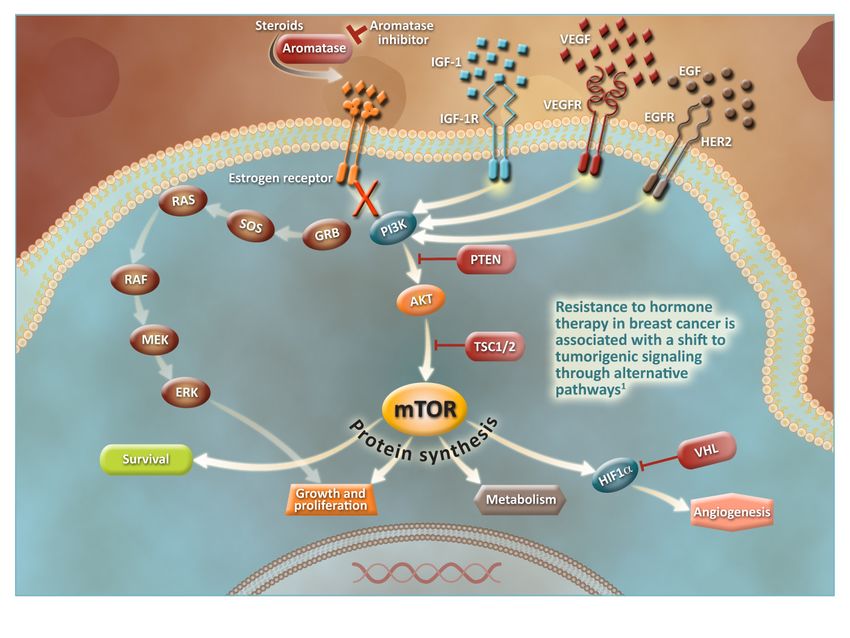
Jonhston S, et al. JCO 2009.Vía PI3K / Akt / mTOR
56
Moy B, Clin Cancer Res 2006.Prevalencia de mutaciones de PI3KCa en CMM
5
7
Albanell J, et al. ESMO 2019Estudio SOLAR 1: Alpelisib aprobado para CMM RH+ PI3KCa mutado
Juric D, et al. ESMO 2018Papel de CDK4/6 en el cáncer de mama RH+
Growth Factor
Estrogen E2
Receptors
Receptor
G0
Cyclin B-CDK1
PI3K/AKT/mTOR
G2
M + or
RAS/RAF/MAPK
+
Cyclin D-CDK4
Cyclin D-CDK6
G1
R point
RB E2F
S P
RB
P P
P
Cyclin E-CDK2
Cyclin A-CDK2 E2F S-Phase Transcription Program
59Ciclina D1: Hallmark en el cáncer de mama RH+
Agarwal R. Clin Cancer Res 2009Inhibidores de CDK 4/6 de 3ª generación: Abema, palbo y Ribociclib
Kisqali es un inhibidor de
CDK4/6
Transcripción
genética
Lange CA et al. Endocr Relat Cancer. 2011 Jul 4;18(4):C19-24.
61 Figura adaptada de: Lange CA et al. Endocr Relat Cancer. 2011 Jul 4;18(4):C19-24.Hito Oncológico: CMM RH+ Inhibidores de CDK 4/6 ofrecen PFS 24-25 m en 1ª línea
La complejidad del Cáncer de Mama
CM a día de hoy Tumor y Microambiente
HER2 +3 HER2 ISH+
Tumor
Infiltrating
mRNA microRNA Protein
Lymphocytes
ER-positive ER-negative (TILs)
Courtesy of Dr. Pedro Fernández DNA Copy Number DNA Methylation DNA Mutations
TCGA Nature 2012
Cortesía de A. PratSubtipos intrínsecos capacidad pronóstica en 1ª línea
Estudio fase III EGF30008
Estudio Retrospectivo No Planificado. CMM RE +. N=644 HER2-
PFS OS
1.0 Luminal A 1.0 Luminal A
Progression-free survival proportion
Luminal B Luminal B
0.8 Basal-like 0.8 Basal-like
Overall survival proportion
HER2-enriched HER2-enriched
0.6 0.6
0.4 0.4
0.2 0.2
P-valueLa complejidad del Cáncer de Mama
CM a día de hoy Tumor y Microambiente
HER2 +3 HER2 ISH+
Tumor
Infiltrating
mRNA microRNA Protein
Lymphocytes
ER-positive ER-negative (TILs)
Courtesy of Dr. Pedro Fernández DNA Copy Number DNA Methylation DNA Mutations
TCGA Nature 2012
Cortesía de A. PratFive recurrent genomic alterations
correlated with drug efficacy
Genomic alteration Incidence Drug / Efficacy
BRCA2 (germline) mutation 3% Carboplatin, PARP inhibitors
AKT1 mutation 4-5% AZD5363 (3 PR /18 pts)
ERBB2 mutation 2% Neratinib
PIK3CA mutation 25-45% α-specific inhibitors (taselisib, alpelisib), ORR
25% with ET
ESR1 mutations 10-30% ORR in ESR1 mutants (GDC-0810, RAD
FGFR1 amplification 10-15% No efficacy with specific inhibitors
Responses with pan-TKIs (toxicity!)
CCND1 amplification 10-15% No predictive value for palbociclib
Other >30% PTEN, NOTCH, FBXW7, EGFR, NF1, MYC
Adapted from F. André, personal communicationNeratinib is active in ER+/HER2- MBC
with activating ERBB2 mutations
ORR 33.3% ORR 58.3%
mPFS 3.5m mPFS 3.7m
Hyman D et al. SABCS 2016La complejidad del Cáncer de Mama
CM a día de hoy Tumor y Microambiente
HER2 +3 HER2 ISH+
Tumor
Infiltrating
mRNA microRNA Protein
Lymphocytes
ER-positive ER-negative (TILs)
Courtesy of Dr. Pedro Fernández DNA Copy Number DNA Methylation DNA Mutations
TCGA Nature 2012
Cortesía de A. PratTumor Infiltrating Lymphocytes (TILs) in Breast Cancer
N=2,009 N=1,079 N=297 N=256
Loi S, et al. J Clin Oncol. 2013;31(7):860-7ULTIMATE TRIAL DESIGN
Patients with CD8+ T Patients treated End of
cell infliltration ≤ 10% as per participation in
at the 3 weeks biopsy Investigator the study
NCT02997995; PI: Fabrice ANDRERealidad actual del CMM luminal
Selección de la Primera línea del CMM ¿Qué hacemos a la PE del INH CDK4/6?
• Tratamiento elección • Tratamiento de elección
• HT+ Inh ciclinas • HT+Everolimus
• HT • HT+inhPI3K?
• QT • QT
• IPARP?
• Toma de decisiones • Toma de decisiones
• Parámetros clínicos • Biomarcadores?
• Perfil de paciente¿Cómo será el más allá tras iCDK4/6?
Luminal A/B (80%) HER2 enriquecido (20%)
PI3K wild type (60%) PI3K mutado (40%)
FGFR1 (20%) HT+Alpelisib HT+Neratinib/Ribo
SERD+Lucitanib
Ciclina E (50%) HT+Alpelisib+
SERD+inhCDK2 inhCDK4/6
SERD+Venetoclast HT+CapivasertibYou can also read