Now and Future: GERD and Nocturnal Acid Reflux Treatments - Aaron M. Clark Amenity Health, Inc.
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
Now and Future: GERD
and Nocturnal Acid
Reflux Treatments
Aaron M. Clark
Amenity Health, Inc.EXECUTIVE SUMMARY
With at least 10% of the US population suffering from gastroesophageal reflux disease (GERD)
and the majority (89%) of this population also suffering from nocturnal acid reflux, the treatment
of GERD and nocturnal acid reflux has become a major topic of discussion for the medical
community at large.
The dangers posed specifically by nocturnal acid reflux are particularly significant as prolonged
esophageal acid exposure has been linked to leading to serious health complications, such as erosive
esophagitis, peptic stricture, esophageal ulcerations, Barrett’s esophagus, and adenocarcinoma
of the esophagus. Additionally, patients who suffer from nocturnal acid reflux experience a
diminished health-related quality of life as sleep deprivation takes its toll health-wise and on
productivity in the workplace.
The current treatment options for GERD and nocturnal acid reflux include lifestyle changes,
medications, and surgery. While lifestyle changes are recommended, Proton Pump Inhibitor (PPI)
medications, have become the mainstay of treatment. However, this class of medication has been
linked by the FDA with serious health risks. Surgical procedures are often ineffective at providing
desired symptom relief and come with negative side effects.
Amenity Health developed the Medcline reflux relief system to address this need for nocturnal
TM
acid reflux patients. Validated by a clinical study at the Medical University of South Carolina,
sleeping on Medcline has been proven to decrease patient esophageal acid exposure without the
TM
side effects posed by PPIs and surgery.
2Now and Future: GERD and Nocturnal Acid Reflux Treatments
SYMPTOMS OF GERD AND Sleep deprivation causes difficulties in concentration; vision
NOCTURNAL ACID REFLUX disturbances; slower reaction times; lower capabilities and
efficiency of task performance; increased number of errors;
At least 10% of Americans have been diagnosed with gastro- and slurred speech. Longer–term health consequences
esophageal reflux disease (GERD)1. While the most common include increased sensitivity to pain; changes in the immune
complaints from those suffering from GERD are of heartburn response and hormonal secretion patterns; increased risk of
and acid reflux, there are many less obvious symptoms such obesity; diabetes; and increases in cardiovascular disease12. The
as dysphagia (difficulty swallowing), chronic cough, asthma, treatment of GERD itself and the secondary consequences of
hoarseness, laryngitis, chronic sinusitis, headaches, and dental nighttime symptoms as related to sleep deprivation result in a
erosions2. Symptoms are produced by the abnormal reflux of marked economic burden on the healthcare system13.
gastric contents (stomach acid) from the stomach back up into
the esophagus3.
The majority of GERD sufferers also experience nocturnal
• 30 million in US suffer from GERD
acid reflux. In fact, in a survey of 11,685 survey respondents • 88.9% experience nighttime symptoms
with GERD, 88.9% experienced nighttime symptoms, 68.3%
experienced sleep difficulties, 49.1% experienced difficulty • $75 billion in lost productivity each year
initiating sleep, and 58.2% experienced difficulty maintaining
sleep4. Symptoms specific to nocturnal acid reflux, include
nighttime awakenings caused by coughing or choking,
regurgitation of fluid or food, and an acidic/bitter taste. Lost Productive Time
There are also significant indirect costs to nocturnal acid reflux
DANGERS SPECIFIC TO NOCTURNAL ACID and GERD in terms of lost productive time. A 2005 study
REFLUX found a 10% reduction in productivity caused by nighttime
symptoms and the resultant sleep deprivation. When
Increased Esophageal Exposure extrapolated based on 2005 salary data, the study found that
During sleep, the body’s natural defense mechanisms against based on the estimated 14.5 million people of working age
refluxed stomach contents, including saliva production and with GERD in the US, this 10% reduction in productivity
swallowing, are greatly reduced5. Also, during the night, costs US employers up to $75 billion/year14.
though reflux episodes tend to be less frequent than during
the day, nighttime episodes are longer in duration6. Both of
these factors lead to increased nighttime acid exposure making TREATMENT OPTIONS
nocturnal acid reflux, in fact, more serious than daytime acid
reflux7. Currently within the medical community, there are three main
treatment protocols for nocturnal acid reflux and GERD.
Nocturnal acid reflux has been found to be an underlying risk Treatment aims to relieve symptoms, improve patient health-
factor for developing more serious health complications, such related quality of life, and reduce the potential for developing
as erosive esophagitis, peptic stricture, esophageal ulcerations, serious complications from chronic damage to the esophagus.
Barrett’s esophagus, and adenocarcinoma of the esophagus8. Current treatments include one or more of the following: (a)
In fact, while the risk of esophageal adenocarcinoma lifestyle changes, including changes to diet, weight loss, and
increases eightfold for those suffering with daytime acid sleep positioning; (b) medications, including antacids, H2
reflux symptoms, the risk increases to 11-fold for those with blockers, PPIs; and/or (c) surgical procedures.
nighttime symptoms9. Esophageal adenocarcinoma is actually
the fastest growing cancer in terms of incidence in the United Lifestyle Changes
States10.
Diet and Weight Loss
Diminished Health-Related Quality of Life When diagnosing GERD, many doctors will first look at
Beyond esophageal damage, nighttime symptoms are very a patient’s diet to determine if there are any changes that
disruptive to sleep, often leading to sleep deprivation. Over can be made to decrease symptoms. It has been found that
time, sleep deprivation takes its toll resulting in a substantially meals that are smaller and lower in fat tend to create less acid
diminished health-related quality of life as compared to those exposure than meals that are larger and higher in fat15. It is
without nighttime symptoms11 . often recommended that patients avoid coffee, tea, carbonated
3beverages, alcohol, citrus fruits, tomatoes, chocolate, mint or Many studies have found that GERD patients are more
peppermint, fatty or spicy foods, onions, and garlic. Because likely to reflux when lying flat on the right side and that
individuals react so differently to food, patients are often asked acid clearance time is slower when lying on the right side
to pay attention to the foods that seem to trigger symptoms so episodes last longer19. These findings suggest that GERD
and avoid them as much as possible. Weight loss is also patients should be advised to sleep on their left side to
recommended as extra pressure around the abdomen increases decrease reflux episodes and the duration of those episodes.
acid reflux. Additionally, right-side episodes tend to be more distressing
and destructive as they are predominately liquid in nature20.
Sleep Positioning
During sleep the body naturally produces less saliva and
swallowing decreases resulting in increased acid clearance time Medications
in the esophagus5. Increased acid clearance time means that
refluxed stomach acid lingers in the esophagus potentially In addition to OTC antacids, there are two classes of
causing serious erosion and long-term damage. Additionally, medications generally used to treat GERD, both of which act
when laying flat on the back at night (supine position) gravity to suppress gastric acid secretion - Proton Pump Inhibitors
cannot help clear acid back to the stomach. Doctors often (PPIs) and Histamine 2 Receptor Antagonist (H2 blockers).
recommend sleeping at an incline to help with acid clearance Brand names for PPIs include Prilosec®(omeprazole),
time. Traditionally, there are two methods to sleep in an Prevacid® (lansoprazole), AcipHex® (rabeprazole), Protonix®
inclined position – head of bed elevation (HOB) or sleeping (pantoprazole), Nexium® (esomeprazole); Zegarid®
on a bed wedge. (omeprazole). Brand names for H2 blockers include Tagamet®
(cimetidine), Pepcid® (famotidine), Axid® (nizatidine), and
HOB is typically achieved by putting blocks or risers under Zantac® (ranitidine). Which medication, or combination
the bed frame so that the entire head of the bed is elevated. of medication used, varies based on severity and individual
Studies have shown a reduction in nocturnal acid exposure, response to each class of medication.
acid clearance time, and symptom improvement16. Though
potentially effective, many who try HOB complain that sliding Antacids
down throughout the night is a consistent issue and/or their OTC antacids, such as Tums® or Rolaids®, act to neutralize
sleep-mate is disturbed17. acid in the esophagus but do not significantly alter overall
gastric pH levels21. Additionally, while antacids can provide
Another traditional method of achieving elevated sleep immediate symptom relief, they do not prevent subsequent
positioning is utilizing a bed wedge. Studies have shown that heartburn episodes and often offer short-lived relief.
while sleeping on a wedge does produce a decrease in distal
esophageal acid exposure, it does not decrease the number Histamine 2 Receptor Antagonist (H2 blockers)
of reflux episodes throughout the night17. Critics of this Histamine 2 Receptor Antagonist (H2 blockers) block the
technique site that wedges elevate only the head, rather than action of histamine on acid producing cells, thus reducing
the entire upper torso of the body, so it does not give any stomach acid production. H2 blockers have been found to
advantage of gravity in clearing reflux and further may cause provide long-term symptom control in about 50% of GERD
neck pain18. As with HOB, patients also have a tendency to patients, especially those with mild-to-moderate symptoms
slide down the wedge throughout the night. and also promote esophageal healing in 44–58% of treated
patients22. H2 blockers are often prescribed to patients who
continue to be symptomatic on standard or double-dose
PPIs23. Also, over-the-counter H2 blockers are often used
as an on-demand solution because of their rapid effect on
symptoms1.
Head of Bed Elevation (HOB) Bed Wedge
Though H2 blockers can provide symptom relief, tachyphylaxis
develops quickly, meaning that patients build up a resistance
In looking at both traditional methods, HOB and the use of
over time so doses have to continue to increase. Patient’s built–
a bed wedge have been shown to provide similar, but limited,
up resistance to H2 blockers limits their regular use in clinical
levels of relief17.
practice24.
4Now and Future: GERD and Nocturnal Acid Reflux Treatments
Proton Pump Inhibitors (PPIs) This ineffectiveness has also been found specifically in
Proton pump inhibitors reduce the production of acid by nocturnal acid reflux patients as well. A survey of over 600
blocking the enzyme in the wall of the stomach that produces GERD patients on PPIs found that the majority of patients
acid. In 2009, more than 119 million PPI prescriptions were continued to experience heartburn, with 83% experiencing
written in the US. $13.5 billion is spent on PPIs in the US nocturnal symptoms and 32% reporting severe or very severe
annually, making them the second biggest-selling drug class nocturnal symptoms35. It has also been found that even when
after cholesterol lowering agents25. doses of PPIs are increased, patients continue to experience
less than satisfactory symptomatic response36.
PPIs came onto the market in the 80s and quickly have
become the treatment of choice for GERD and nocturnal The estimated cost per person, per year of patients on a once-
Acid Reflux due to their profound and consistent inhibitory a-day PPI is $2,000 to $4,500 for brand name prescription
effect on acid secretion1. Though PPIs do provide symptom PPIs37.
relief, they do not provide a long-term cure for GERD.
Additionally, recent population-based studies, along with
multiple FDA safety announcements, have suggested that Surgical Treatments for GERD
long-term PPI use may pose significant health risks to
patients. For patients who are unresponsive to lifestyle changes and
drug therapy, surgery is often explored. While other medical
As a result of the risks posed by long-term exposure to PPIs, procedures have been developed, such as Transoral Incisionless
there is growing interest by patients and physicians alike to Fundoplication (TIF), Radio-Frequency Ablation, and
discover non-PPI-related therapeutic strategies for GERD1. Stretta® therapy, the most common surgery performed is
called Nissen Fundoplication.
Treating GERD with PPIs is also problematic in that up to
40% of those on a daily PPI are refractory, meaning they still Nissen Fundoplication
experience symptoms34. During this laparoscopic procedure, the surgeon wraps the
top part of the patient’s stomach around the lower part of
the esophagus attempting to tighten the lower esophagus to
prevent acid from refluxing from the stomach back into the
Serious Health Complications with esophagus. The tightening of the lower esophagus, creating
Long-term PPI Use what is often referred to as a “one way valve,” often leads to
unintended consequences. In fact, after the procedure, 60% of
• Increased risk of contracting Clostridium Difficile, a patients developed new symptoms, such as dysphagia, choking,
serious and potentially deadly bacterial infection26.
epigastric pain, gas/bloating, inability to belch, nausea, and/or
• Increased risk of hip, wrist, and spine fractures with
diarrhea38.
high doses or long-term use of prescription PPIs27.
• Possible connection to low serum magnesium levels
Additionally problematic is that fact that follow up studies
if taken for prolonged periods of time (in most
cases, longer than one year). In approximately one- have found that 40% of Nissen Fundoplication patients had
fourth of the cases reviewed, supplementation did symptoms return, had esophagitis come back, needed medicine
not improve low serum magnesium levels after the for recurrent symptoms, and/or needed another operation after
PPI had to be discontinued28.
seven years39.
• Possible cause of cardiovascular disease, which may
also increase the likelihood of a heart attack29.
The estimated cost of a Nissen Fundoplication procedure is
• Increased risk for vitamin B12 deficiency, which can $18,000.
cause tiredness, weakness, constipation, and a loss
of appetite, and more seriously, balance problems,
memory difficulties, and nerve problems30. LINX® Reflux Management System
• Increased risk of developing community-acquired
Another surgical option for patients who are unresponsive
pneumonia31. to lifestyle changes and medications is the LINX® Reflux
• Increased risk of acquiring microscopic colitis32 Management System. The LINX® device (which consists of a
leading to chronic diarrhea. series of titanium beads, each with a magnetic core, connected
• Increased incidence of small intestinal bacterial together with titanium wires to form a ring shape) is surgically
overgrowth (SIBO)33. implanted around the lower end of the esophagus. The device
opens as food is digested down into the stomach, then tightens
up so that stomach contents cannot reflux back up into the
esophagus.
5The most common patient complaint following the LINX® 4%
procedure include difficulty swallowing (76 events in 68
patients). The second most common complaint is pain (25
events in 24 patients)40. Additionally, patients who have the
LINX® device must not be exposed to, or undergo, Magnetic 3%
Resonance Imaging (MRI) as this could cause serious injury to
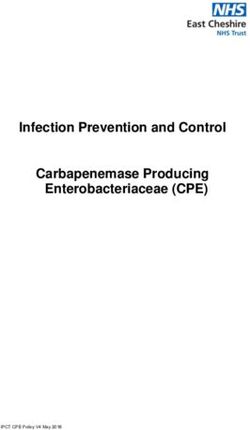
Percent Time pH < 4.0
the patient, as well as damage to the device.
The average LINX® surgical procedure is $15,000 - $20,000. 2%
1%
AMENITY HEALTH OFFERS MEDCLINE™
TO TREAT NOCTURNAL ACID REFLUX
Medical research suggests that developing new therapeutic 0
strategies for GERD, in lieu of indefinite or high-dose PPI Medcline™ Sleep Bed Wedge
treatments or invasive surgical procedures, should be a high Assist Device
priority for pharmaceutical and medical device companies1. Figure 2: Medcline™ shows significantly less esophageal acid exposure
Amenity Health developed Medcline™ to address this need. compared to a traditional bed wedge.
Medcline™ is the much needed treatment alternative for and cleared for patient use. Medcline™ also meets the IRS
nocturnal acid reflux. The Medcline™ reflux relief system (see Guidelines to be classified as an FSA/HSA-approved medical
Figure 1) leverages proven techniques for nighttime symptom expenditure. Patients can purchase Medcline™ directly from
relief and protection against the serious health complications Amenity Health.
associated with long-term esophageal acid exposure. Its
patented Cradle-Loc™ design places patients in an ideal
sleeping position with their entire torso elevated and gently Looking Ahead
holds them on their left side for maximum results. Medcline™ is currently being utilized in a clinical study with
Cleveland Clinic. This study aims to quantify health-related
quality of life improvements when sleeping on Medcline™, as
well as accessing patients’ ability to decrease medication usage
over time.
15-20˚
In addition to patients with a GERD or nocturnal acid reflux
diagnosis, Amenity Health is continually researching new
applications for Medcline™, including thoracic patients for
Figure 1: Medcline™ is comprised of an ergonomic incline base and lung transplants and idiopathic pulmonary fibrosis (IPF);
companion body pillow. scleroderma patients; non-tuberculosis mycobacteria patients;
Under the direction of Donald O. Castell, MD, the Medical esophagectomy recovery patients; and silent reflux patients.
University of South Carolina conducted a study to validate
the effectiveness of Medcline™. The study compared
Medcline™ to a traditional bed wedge and found that when
users slept on their left side, Medcline™ provides41:
• 87% reduction in esophageal acid exposure time
(see Figure 2)
• 38% reduction in nighttime acid reflux episodes
• 2x more comfort than a wedge
Medcline™ is a Class I Medical Device listed with the FDA
6Now and Future: GERD and Nocturnal Acid Reflux Treatments
References
1 Hershcovici,Tiberiu, Fass, Ronnie. Gastro-oesophageal reflux disease, 25 Heidelbaugh JJ, Goldberg KL, Inadomi JM. Overutilization of proton
beyond proton pump inhibitor therapy. Drugs 2011; 71 (18): 2381-2389. pump inhibitors: a review of cost-effectiveness and risk[corrected] Am J
2 Storr M, Meining A, Allescher HD. Pathophysiology and pharmacological Gastroenterol. 2009;104 (Suppl 2):S27–S32.
treatment of gastroesophageal reflux disease. Dig Dis Sci 2000; 18: 26 Dial S, Alrasadi K,Manoukian C, et al. Risk of Clostridium difficile
93–102. diarrhea among hospital inpatients prescribed proton pump inhibitors:
3 DeVault, Kenneth R., Castell, Donald O. Updated guidelines for the cohort and case-control studies. CMAJ 2004 Jul 6; 171 (1): 33-8. AND
diagnosis and treatment of gastroesophageal reflux disease. American 2.8.2012 FDA Safety Announcement.
Journal of Gastroenterology. 2005;100:190–200. 27 Yang YX, Metz DC. Safety of proton pump inhibitor exposure.
4 Mody, R., et al., Clinical Gastroenterol and Hepatol 2009;7:953-959. Gastroenterology 2010 Oct; 139 (4): 1115-27 (and) 3.23.2011 FDA
5 Fass, Ronnie. PPI bashing’ drives use of alternatives. gastoendnews.com, Safety Announcement.
Sept. 2011. 28 3.2.2011 FDA Safety Announcement.
6 Orr, WC, Johnson LF, Robinson MG. Effect of sleep on swallowing, 29 Study conducted by researchers at Texas Methodist Hospital Research
esophageal peristalsis, and acid clearance. Gastroenterology 1984; 86: Institute, Stanford University, and MRC Clinical Sciences Center,
814-819. Imperial College, London, UK, August 2013.
7 Orr , William C., Management of nighttime gastroesophageal reflux disease, 30 Study conducted by researchers at Kaiser Permanente, December 2013.
Gastroenterology & Hepatology. 2007 August; 3(8): 605–606. 31 Laheij RJ, Sturkenboom MC, Hassing RJ, et al. Risk of community-
8 Lagergren, J, Bergstrom R, Lindgren A, et al. Sympomatic gastroesophageal acquired pneumonia and use of gastric acid suppressive drugs. JAMA 2004
reflux as a risk factor for esophageal adenocarcinoma. N Engl J Med 1999; Oct 27; 292 (16): 1955-60.
340: 825-831. 32 Keszthelyi D, Jansen SV, Schouten GA, et al. Proton pump inhibitor use
9 Lagergren J, Bergstrom R, Lindgren A, Nyren O. Symptomatic GER is associated with an increased risk for microscopic colitis: a case-control
as a risk factor for esophageal adenocarcinoma. N Engl J Med 1999; study. Aliment Pharmacol Therapy. 2010 Nov; 32 (9): 1124-8.
340:825–831. 33 Lombardo L, FotiM, Ruggia O, et al. Increased incidence of small
10 Ashburn, Ted T, Gupta Meera S. The GERD market. Drug Discovery Vol . intestinal bacterial overgrowth during proton pump inhibitor therapy.
5. April 2006. 277-278. Clinical Gastroenterology & Hepatology 2010 Jun; 8 (6): 504-8.
11 Farup, Kleinman, Sloan S, et al. The impact of nocturnal symptoms 34 Dickman, Ram, et al. Comparison of clinical characteristics of patients
associated with gastroesophageal reflux disease on health-related quality of with gastroesophageal reflux disease who failed proton pump inhibitor
life. Arch Internal Med 2001; 161: 1448-1456. therapy versus those who fully responded. J Neurogastroenterol Motil, Vol.
12 Orzal-Gryglewska, Jolanta, Consequences of sleep deprivation. 17 No. 4 October, 2011.
International Journal of Occupational Medicine and Environmental 35 Chey WD , Mody RR , Wu EQ et al. Treatment patterns and symptom
Health 2010; 23(1):95–114. control in patients with GERD: US community-based survey . Curr Med
13 Sandler RS, Everhart JE, Donowitz M, et al. The burden of selected Res Opin 2009 ; 25:1869–78.
digestive diseases in the United States. Gastroenterology 2002 May; 122 36 Fass R, Murthy U, Hayden CW, et al. Omeprazole 40 mg once a day is
(5): 1500-11. equally effective as lansoprazole 30 mg twice a day in symptom control of
14 Wahlqvist, P, Reilly ,MC, Barkun, A. Systematic review: the impact patients with gastro-oesophageal reflux disease (GERD) who are resistant
of gastro-oesophageal reflux disease on work productivity, Aliment to conventional-dose lansoprazole therapy-a prospective, randomized,
Pharmacology & Therapeutics 24, 259–272. multi-centre study. Aliment Pharmacol Therapy 2000;14:1595-1603.
15 Iwakiri et al., Dig Dis Sci 1996; 41:926. 37 Monthly cost reflects nationwide retail average prices for March 2010,
16 Khan, Bashir A. et al. Journal of Gastroenterology and Hepatology, rounded to the nearest dollar. Information derived by Consumer
Accepted article. Reports Best Buy Drugs from data provided by WoltersKluwer Health,
17 Hamilton, John W, et al. Sleeping on a wedge diminishes exposure of the Pharmaceutical Audit Suite®. Average monthly cost is based on
esophagus to refluxed acid. Digestive Diseases and Sciences, Vol. 33, No. 5 recommended dosage of one pill daily. May, 2010.
(May 1988), pp. 518-522. 38 Humphries, L.A., et al., Surg Endosc 2013;27:1537-1545.
18 Pope CE: Gastro esophageal reflux disease: Pathophysiology, diagnosis, 39 Lundell, L. et al. (2007). Seven Year Follow-Up of a Randomized Clinical
management. Philadelphia, WB Saunders 1983, 449-490. Trial Comparing Proton-Pump Inhibition with Surgical Therapy for
19 Khoury, Ramez M. Influence of spontaneous sleep positions on nighttime Reflux Oesohpagitis. British Journal of Surgery, 94(2):198-203.
recumbent reflux in patients with Gastroesophageal Reflux Disease. The 40 LINX™ Reflux Management System - P100049. http://www.
American Journal of Gastroenterology. Vol. 94, No. 8, 1999. fda.gov/MedicalDevices/ProductsandMedicalProcedures/
20 Shay SS, Conwell DL, Mehindru V, et al. The effect of posture on DeviceApprovalsandClearances/Recently-ApprovedDevices/ucm300790.
gastroesphageal reflux event frequency and composition during fasting. htm.
Am J Gastroenterology. 1996; 91: 54-60. 41 Person, EB, Rife CC, Castell DO, et al. A novel sleep-assist device
21 McRorie JW Jr, Gibb RD, Miner PB Jr. Journal of American Assoc Nurse prevents gastroesophageal reflux: A randomized controlled trial. Am J
Practice. 2014 May 13. doi: 10.1002/2327-6924.12133. Gastroenterology 2013; 108:S1-S36.
22 Galmiche JP, Letessier E, Scarpignato C. Treatment of gastro-oesophageal
reflux disease in adults. Br Med J 1998; 316:1720–1723.
23 Peghini PL, Katz PO, Castell, DO. Ranitidine controls nocturnal gastric
acid breakthrough on omeprazole: a controlled study in normal subjects.
Gastroenterology 1998; 115 (6): 1335-9.
24 Fackler WK, Ours TM, Vaezi MF, et al. Long-term effect of H2RA
therapy on nocturnal gastric acid breakthrough. Gastroenterology 2002;
122 (3): 625-32.
78830 Rehco Rd. Suite E, San Diego, CA 92121
800.610.1607 | support@amenityhealth.com | www.amenityhealth.com
Copyright © 2014 Amenity Health, Inc. All rights reserved. Medcline™, and its affiliate brand names, is protected by US Patent No.8661586. #1127v1You can also read