National Survey of Noncommunicable Diseases in Seychelles 2013 2014 (Seychelles Heart Study IV): main findings - WHO FCTC
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

National Survey of Noncommunicable Diseases in
Seychelles 2013‐2014 (Seychelles Heart Study IV):
main findings
This report focuses on selected main findings from the 2013 National NCD Survey and these findings are compared,
whenever possible, with results from previous national NCD surveys in 1989, 1994 and 2004.
A technical report presenting crude results for all the variables assessed in the 2013 NCD survey entitled “National
Survey of Noncommunicable Diseases in Seychelles 2013‐2014 (Seychelles Heart Study IV): Methods and Overall
Findings” was produced by the Public Health Authority, Ministry of Health, Seychelles (2nd version, 10 November
2014). These findings were discussed in two half‐day meetings in the presence of Minister of Health, officials and
interested persons on 31 October & 4 November 2014.
Detailed analysis of specific issues and related recommendations will be available in separate reports.
Public Health Authority
24 February 2015 (version 2)
1
National Survey of Noncommunicable Diseases in Seychelles 2013‐2014
(Seychelles Heart Study IV): main findings
Pascal Bovet, Bharathi Viswanathan, Meggy Louange & Jude Gedeon, on behalf of the Survey Team
Unit of Prevention and Control of Cardiovascular Diseases (UPCCD)
Public Health Authority
Ministry of Health
Victoria
Republic of Seychelles
Survey team
Pascal Bovet, MD, NCD consultant, Ministry of Health, Seychelles & associate professor, Institute of Social and
Preventive Medicine, University of Lausanne, Switzerland
Bharathi Viswanathan, RN, program manager, UPCCD
Barbara Fock Tave, RN, UPCCD
Juddy Labiche, RN, UPCCD
Gaynor Mangroo, health promotion officer, UPCCD
Romena Maria, RN, UPCCD
Vanessa Lafortune, UPCCD
Gina Michel, RN, program manager, Cancer and Other NCDs Unit
Daniel Belmont and colleagues, Public Health Laboratory
Maygane Jean and colleagues, Clinical Laboratory, Seychelles Hospital
Meggy Louange, MD, Director General, NCD Section, MOH
Jude Gedeon, MD, Public Health Commissioner, Public Health Authority, MOH
Funding
Ministry of Health, Republic of Seychelles (staff, laboratory and partial direct funding)
World Health Organization (core methodology of survey [STEPS] and partial direct funding)
University Institute of Social and Preventive Medicine, Lausanne, Switzerland (technical support and partial
direct funding)
Seychelles Trading Company (STC), Seychelles (unconditional vouchers to all participants)
Seychelles Petroleum (SEYPEC), Seychelles (unconditional partial funding)
2
Acknowledgements
Grateful thanks are expressed to the following institutions and persons who have been instrumental in the organization of the survey:
Public Health Authority, Ministry of Health, Seychelles, particularly Mitcy Larue (minister), Jude Gedeon (public health
commissioner), Shoba Hajarnis (director general), and Meggy Louange (director of the NCD section)
All the staff members of the Unit of Prevention and Control of Cardiovascular Disease (UPCCD), Public Health Department,
including Bharathi Viswanathan (program manager); Barbara Fock Tave; Juddy Labiche; Gaynor Mangroo; Vanessa Lafortune;
Romena Marie and Maria Omath; and Gina Michel (program manager) from Unit of Other NCDs
Clinical laboratory, Seychelles Hospital, particularly Prosper Kinabo (director), Maygane Jean (senior technician) and colleagues
Public Health Laboratory, Ministry of Health Seychelles, particularly Philip Palmyre (director), Daniel Belmont (senior technician)
and colleagues
Praslin Hospital, particularly Dina Hibonne (coordinator) and Logan Hospital, particularly Pamela Dubignon (coordinator)
National Bureau of Statistics (NBS), particularly Laura Ahtime (CEO) and Helena Deletourdis (principal statistician)
Ministry of Administration and Community Services (MACS), particularly Denis Rose (principal secretary), Dan Frichot (director
general), and all the district administrators and their staff
Seychelles Broadcasting Company (SBC), particularly Antoine Onesime (CEO), Cindy Wirtz (sales manager) and the journalists
involved in several programs on TV and radio on the survey
World Health Organization, particularly Cornelia Atsyor (local liaison officer) and the WHO AFRO office
Institute of Social and Preventive Medicine, University Hospital Center, Lausanne, Switzerland, particularly Fred Paccaud
(director), Brigitte Santos Eggimann (advisor on questionnaire sections related to frailty and aging) and Samuel Hirsiger for
contribution to preliminary analysis of the overall results
Seychelles Trading Company (STC), particularly Patrick Vel (CEO up to 2013) and Veronique Laporte (CEO 2014), for providing a
large non conditional grant (vouchers to all participants)
Seychelles Petroleum (SEYPEC), particularly Conrad Benoiton (CEO) and Sarah Romain (commercial manager) for providing a large
non conditional grant
OMRON Healthcare Europe, The Netherlands, particularly Dounia Benjelloun (Sales Manager Africa) for supplying free or charge
equipment to perform ECG and bioimpedance
Bayer Consumer Care AG, Switzerland, particularly Konstantin Tselikas (country manager NaOC) for providing discounted prices on
diagnostic equipment for diabetes, including A1c
Minister of health, high officials and survey team at the opening ceremony of the Seychelles
NCD Survey (Seychelles Heart Study IV) on 23 September 2013
3 Table of contents Summary and recommendations .............................................................................................................................4 Context of NCDs globally and in Seychelles .............................................................................................................6 Objectives of the 2013 survey ..................................................................................................................................7 Methods and participants for the 2013 survey ........................................................................................................7 Population and mortality, Seychelles, 1989‐2013.........................................................................................................8 Participation to Seychelles NCD surveys ..................................................................................................................9 Body mass index (BMI) .............................................................................................................................................9 Tobacco use ........................................................................................................................................................... 11 Alcohol use ............................................................................................................................................................ 13 Dietary habits ........................................................................................................................................................ 16 Physical activity (PA) .............................................................................................................................................. 18 High blood pressure (HBP) .................................................................................................................................... 19 Blood cholesterol................................................................................................................................................... 22 Diabetes ................................................................................................................................................................. 24 Trends in risk factors between 1989 and 2013 ..................................................................................................... 26 Socio demographic variables (2013 Survey).......................................................................................................... 27 Perceived health status ......................................................................................................................................... 28 Utilization of health care services ......................................................................................................................... 28 Screening of selected cancers ............................................................................................................................... 30 Communication, mass media, and exposure to health programs ........................................................................ 31 Appendix 1. Tabulation of selected findings by sex and survey year .................................................................... 33 Appendix 2. Questionnaire in English.................................................................................................................... 38 Appendix 3. Data entry form for measurements .................................................................................................. 52

4
Summary and recommendations selected days in study centers located in Mahé, Praslin, and La
Digue. All the eligible participants who did not attend were
This report provides information on selected summary results of actively traced using (telephone, local administration,
the National Survey of Noncommunicable Diseases in Seychelles announcements on radio, etc) and invited to attend the survey.
in 2013‐2014 (Seychelles Heart Study IV). The survey is also Since participants were randomly selected from the general adult
referred shortly as the “2013 Survey” in this report. Overall crude population, findings of the survey can be inferred to the general
results were reported in a comprehensive report in November adult population of Seychelles.
2014. Further detailed analyses and recommendations on
particular topics will be performed separately. The survey included a questionnaire and clinical and biological
tests including anthropometrics, bioimpedance, blood pressure,
The survey 2013 Survey addressed the following objectives: blood tests, urine tests, one lead ECG, bone ultrasound, and
selected functional tests to assess frailty.
Primary objectives
Main findings and global recommendations
a) Distribution of the main modifiable risk factors of
noncommunicable diseases (NCD), particularly blood Pending further analysis, and based on preliminary analysis
pressure, adiposity markers, diabetes and blood lipids reported in this report and the overall report produced in
b) Distribution of health behaviors related to NCDs, particularly November, the following general findings can be formulated:
tobacco use, alcohol drinking, and physical activity
c) Rates of awareness, treatment and control of hypertension, a) The prevalence of tobacco use decreased between 1989‐and
diabetes and dyslipidemia 2013, reflecting strong tobacco control programs and policy
d) Comparison of findings in survey in 2013‐2014 with results in in the interval. Data also show that the general public largely
previous surveys in 1989, 1994, 2004 supports the tobacco control legislation implemented a few
e) Dietary patterns years ago in Seychelles.
f) Knowledge, attitudes and practices related to NCDs and NCD Tobacco control needs to be strengthened including strict
risk factors enforcement of current legislation and need to address new
Secondary objectives issues, e.g. electronic cigarettes, shisha, measures targeting
smoking among youth, etc.
g) Assessment of indicators of quality of health (e.g. SF‐12)
h) Assessment of psychological stress and relation with NCD b) Blood pressure (BP) tended to decrease over time, consistent
i) Assessment of indicators of frailty (e.g. handgrip strength with improved awareness, treatment and control rates
test, chair strand test, questions on functional limitations) between 1989 and 2013. Favorable trends likely reflect socio‐
j) Assessment of knowledge and level of agreement with economic development, increasingly diverse nutrition, and
current policies on tobacco control improved medical care. However, the level of control of BP
k) Use of public and private health care services, particularly for among persons with HBP and knowledge on hypertension is
NCDs far from optimal.
l) Exposure to advice on health behaviors given by health There is a need to improve health care for patient with HBP,
professionals at health care level including updated guidelines for detection and treatment of
m) Burden of chronic diseases not related to the main NCDs (e.g. hypertension, training of health professionals, extended use
musculoskeletal, mental health, etc) of home BP monitoring, etc. There is also a need to improve
n) Screening of selected cancers population‐based interventions, including awareness
o) Assessment of the kidney function in the population campaigns (“know your number”, “reduce your salt”, etc) and
p) Frequency of heart arrhythmias (one‐lead ECG) and heart structural measures in all sectors to improve choices for
murmurs (auscultation) healthy products and regular physical activity (e.g. reduction
q) Assessment of bone mineral density (ultrasound of of salt in locally made or imported manufactured foods).
calcaneus)
r) Exposure of the population to the mass media, particularly in c) The prevalence of overweight/obesity and diabetes has
relation to health programs, and use by the population of markedly increased between 1989 and 2013, consistent with
new communication technologies worldwide upward trends and increasingly globalized food
s) Assessment of social variables and their association with the markets. The survey provides information on dietary patterns
variables measured in the survey in the population, which is useful to guide individual‐based
t) More generally, the survey provides broad information and population‐based interventions.
(medical, social, environment, etc) that can be useful for
Need to develop structural interventions in all sectors to
tailoring NCD prevention and control programs.
improve the availability of, and access to, healthy foods for all
Overall methods of the survey people and in different settings (schools, workplaces, etc),
including adequate food labeling, ban on advertising of
The survey was performed in a sex and age stratified random unhealthy foods in mass media, subsidies/taxes on
sample of all adults aged 25‐64 years of Seychelles between healthy/unhealthy foods, food labeling, etc. Interventions in
October and December 2013 on Mahé and during 2 weeks in all sectors are also needed to promote physical activity in
February 2014 in the islands of Praslin and La Digue. These three different settings. Health education programs are helpful to
islands account for >98% of the total population of Seychelles. raise awareness on healthy lifestyles and should target all
The eligible sample was extracted from the population registry. population sub‐groups. The school setting is particularly
The survey was attended by 1240 adults, with a participation rate important to empower healthy choices at a young age and
of 73%. Participants were invited to attend the survey on specific measures include water fountains in all schools,
5
healthy food menus in canteens, compulsory 2 or 3 hours of Global targets for NCD prevention and control
physical activity per week, etc.
All WHO member states, including the Seychelles, agreed at the
d) Knowledge on NCDs is fairly good in the population, reflecting World Health Assembly in 2014 on 9 targets to be achieved by
the impact of continued health education programs in the 2025 (compared to baseline in 2010):.
mass media in Seychelles and through other avenues over the 1) 25% reduction of NCD
past 2‐3 decades. Yet several areas of knowledge about NCDs 2) 10% reduction in alcohol use
should be improved. The survey also provides information on 3) 10% reduction in prevalence of insufficient physical activity
how people are exposed to different mass media in 4) 30% reduction in mean population salt intake
Seychelles and how people use electronic communication 5) 30% reduction in the prevalence of tobacco use
devices: this provides useful information on how these mass 6) 25% reduction in the prevalence of raised blood pressure
media and new technologies could be used to strengthen 7) 0% increase in obesity and diabetes
new NCD awareness campaigns. 8) At least 50% of eligible people receiving drug therapy and
counseling to prevent heart attack and stroke (this includes
Need to brainstorm ways to enhance health education
hypertension and diabetes treatment)
programs, including through targeted use of mass media and
9) At least 80% availability of the affordable technologies and
new communication technologies.
essential medicines, including generics, required to treat major
e) Many people report less than optimal exposure to advice on NCDs on both public and private facilities
healthy lifestyle and nutrition by health professionals at the
Next national NCD surveys & WHO Global Status Reports
level of health care.
The WHO 2014 Global Status Report on NCDs provides
Need to brainstorm efficient and innovative mechanisms to population levels of selected indicators related to the 9 targets in
provide health education at the level of health care services 2010 and 2014 for all countries, based on actual data or
(to target patients) and through other channels (to target the estimated using statistical models. For Seychelles, levels of risk
general public). factors of NCDs appearing in the WHO Global Status Report 2014
f) The survey provides information on frequency of screening on NCDs come from the 2013 survey.
for several priority cancers. Within the WHO Global Monitoring Framework and the WHO
Need to brainstorm the design, implementation and Global Plan of Action for the Prevention and Control of NCDs
monitoring of screening programs for priority cancers in endorsed by all countries in 2013 and 2014, all countries are
Seychelles. expected to report population levels of these 25 NCD indicators
and updated national data will be published in updated versions
g) Several characteristics related to NCDs (health behaviors, risk of the Global Status Report on NCDs in 2020 and 2025. This
factors, knowledge, exposure to information, use of health implies that each country should perform national surveys of
care services, etc) were less favorable among lower socio‐ NCD risk factors, similar to the 2013 Survey. On these premises, a
economic groups. next survey in Seychelles could be organized in 2018‐2019 and, in
Need to brainstorm these results and consider social factors all cases, in 2023‐2024 in order to assess achievement of the 9
when designing interventions to address the prevention and priority targets.
control of NCDs.
The following data collected in the 2013 Survey will be examined
in separate report: quality of life; stress and NCDs; frailty & aging;
kidney function; heart arrhythmias & murmurs; bone mass
density; A1c vs. blood glucose for the diagnosis of diabetes, etc.
Of note, the WHO 2014 NCD Status Report (available on www‐
who.int) provides lists of most cost‐effective population wide and
high risk interventions to reduce the burden of NCDs.
6
Context of NCDs globally and in Seychelles past 2‐3 decades in the Seychelles to address NCDs, particularly
strong tobacco control measures (e.g. comprehensive tobacco
Global burden of NCDs control legislation in 2009), improved nutrition (i.e. increasingly
diverse food available) and free health care allowing all high risk
Cardiovascular diseases (CVD) and other main noncommunicable
persons to receive treatment.
diseases (NCD) such as cancer, diabetes, and obstructive
pulmonary disease account for more than 70% of all premature However, Seychelles experiences a rapid demographic transition
deaths in most middle income countries, including in Seychelles. so that the total number of NCD patients (which tend to occur at
The burden of NCD is largely attributable to 4 “physiological” middle or older age) will rise over time, even if interventions to
main risk factors (body mass index, blood pressure, blood lipids prevent and control NCDs are successful.
and diabetes) which are themselves largely determined by 4
major modifiable risk behaviors (smoking, insufficient physical NCD risk factors in previous surveys in Seychelles
activity, unhealthy diet, and excess alcohol intake). The key information needed to guide interventions for NCD
Main risk factors of NCDs prevention and control is the current levels of risk factors in the
population. Population‐based surveys require that participants
The focus on 4 main modifiable behaviors to reduce the NCD are randomly selected from the general population. Previous
burden is encapsulated in the so called “4*4 strategy”, advocated population‐based surveys of NCD risk factors were conducted in
in the Political Declaration on NCD Prevention and Control 1989, 1994 and 2004. Results of these surveys have been widely
adopted [1] and in the WHO 2013‐2020 Global Plan of Action for reported in overall reports [7‐9] and through more than 50
the Prevention and Control of NCDs adopted by all member publications that have focused on special NCD issues [10‐15]. The
states in May 2013 [2]. From a clinical perspective (i.e. the health existence of data from 4 national surveys between 1989 and
care response) the emphasis is on the main physiological risk 2013 is unique and no country in the African region has
factors (blood pressure, blood lipids, and blood glucose performed more than2 NCD surveys recently, except Mauritius.
impairment), which are amenable to screening and control
through cost effective treatment. Results from the past surveys (i.e. 1989, 1994, and 2004) have
shown divergent trends of NCD risk factors over time: downward
WHO targets to reduce the burden of NCDs trend for smoking (good news), unchanged or decreasing trends
for high blood pressure and high blood cholesterol (good news)
The “Global Action Plan for the Prevention and Control of NCDs,
but largely upward trends for diabetes and obesity (bad news)
2013‐2020 (3) adopted by all WHO member states in May 2013
[13,14,15]. Findings of these previous surveys have been
[3] defines 9 voluntary national targets to be achieved by 2025
instrumental to guide prevention and control programs in
and 25 indicators to monitor progress towards meeting these
Seychelles since the early 1990s.
targets.
The NCD survey in 2013‐2014 was therefore timely to update the
The 9 targets to be achieved by 2025, compared to baseline in
situation of NCD risk factors which was last surveyed in 2004.
2010, are:
Information in 2013‐2014 will be important to guide and adjust
1) 25% reduction of NCD
clinical and public health responses to address NCDs, including
2) 10% reduction in alcohol use
useful information to guide the Seychelles NCD strategy.
3) 10% reduction in prevalence of insufficient physical activity
4) 30% reduction in mean population salt intake References
5) 30% reduction in the prevalence of tobacco use 1) UN General Assembly. Political declaration of the high‐level meeting
6) 25% reduction in the prevalence of raised blood pressure of the General Assembly on the prevention and control of non‐
7) 0% increase in obesity and diabetes communicable diseases. A/66/L.1. 16 September 2011.
th
8) At least 50% of eligible people receiving drug therapy and 2) 65 World Health Assembly closes with new global health
measures.www.who.int/mediacentre/news/releases/2012/wha65_cl
counseling to prevent heart attack and stroke
oses_20120526/en/index.html
9) At least 80% availability of the affordable technologies and 3) Global Action Plan for the Prevention and Control of NCDs, 2013‐2020,
essential medicines, including generics, required to treat major WHO, Geneva, 2013, www.who.int/nmh/events/ncd_action_plan/en/
NCDs on both public and private facilities 4) World Health Organization. Global status report on
noncommunicable diseases 2014. WHO, Geneva, 2015
All WHO Member States have committed to report national www.who.int/nmh/publications/ncd_report2014/en
levels of NCD risk factors on a regular basis. A first report (WHO 5) Annual Health Statistical Report. Ministry of Health, 2013.
Global Status Report on NCDs was published in 2011 (WHO 6) Stringhini S, Sinon F, Didon J, Gedeon J, Paccaud F, Bovet P. Declining
Global Status Report on NCDs 2014) and an updated report was stroke and myocardial infarction mortality between 1989 and 2010 in
published in 2015 (WHO Global Status Report on NCDs 2014) a country of the African region. Stroke 2012; 43: 2283‐88.
[16]. Updated versions of this report will be published by WHO in 7) Bovet P, Rosalie D, Shamlaye C, Darioli R, Paccaud F. The Seychelles
2021 and in 2025. This implies that a next survey in Seychelles Cardiovascular Diseases Survey 1989: methods and results. Sozial &
Praeventivmedizin 1991;36 (Suppl 1):S1‐89.
should possibly take place before 2019 or and/or before 2024.
8). Bovet P, Perret F, Shamlaye C, Darioli R, Paccaud F. The Seychelles
Overall trends of NCDs in Seychelles Heart Study II. Methods and selected basic findings. Seychelles
Medical & Dental Journal 1997;5:8‐24.
Vital statistics in Seychelles show that CVD and cancer account
for the largest share of premature mortality and morbidity in
Seychelles [5]. The good news is that the age‐standardized rates
of CVD are decreasing in Seychelles [6], consistent with trends in
high income countries. This favorable downward trend in is likely
related to the many programs and policies implemented over the
7
Objectives of the 2013 survey from the general adult population, findings can be inferred to the
general adult population of Seychelles.
The 2013 survey addressed the following objectives:
Instruments used in the survey to collect data
Primary objectives
The survey included a questionnaire and several examinations
a) Distribution of the main modifiable risk factors of including anthropometrics, bioimpedance, blood pressure, blood
noncommunicable diseases (NCD), particularly blood tests, urine tests, one lead ECG, bone ultrasound, and selected
pressure, adiposity markers, diabetes and blood lipids functional tests.
b) Distribution of health behaviors related to NCDs, particularly
tobacco use, alcohol drinking, and physical activity Detailed information on methods are described in the report
c) Rates of awareness, treatment and control of hypertension, entitled “National Survey of Noncommunicable Diseases in
diabetes and dyslipidemia Seychelles 2013‐2014 (Seychelles Heart Study IV): Methods and
d) Comparison of findings in the survey in 2013‐2014 with Overall Findings, Public Health Authority, Ministry of Health,
nd
results in previous surveys in 1989, 1994, 2004 Seychelles, 2 version, 10 November 2014”).
e) Dietary patterns Further analyses will be performed to allow detailed description
f) Knowledge, attitudes and practices related to NCDs and NCD of the findings and to formulate specific recommendations in
risk factors different health areas.
Secondary objectives Approval of the survey
g) Assessment of indicators of quality of health (e.g. SF‐12) The protocol of the survey was approved by the Health
h) Assessment of psychological stress and relation with NCD Research and Ethics Committee.
i) Assessment of several indicators of frailty (e.g. handgrip The objectives of the survey were guided by the
strength test, chair strand test, functional limitations) recommendations of the WHO Global Monitoring to
j) Assessment of knowledge and level of agreement with countries to regularly conduct population surveys on the 25
current policies on tobacco control priority NCD markers.
k) Use of public and private health care services, particularly for A large part of the survey followed standard methods for
NCDs NCDs advocated by WHO (i.e. STEPS).
l) Exposure to advice on health behaviors given by health
professionals at health care level Consent form
m) Burden of chronic diseases not related to the main NCDs (e.g.
Upon arrival to the study center, the aim and procedures of
musculoskeletal, mental health, etc)
the survey was explained to each participant separately and
n) Screening of selected cancers
each participant was invited to sign an informed consent
o) Assessment of the kidney function
form.
p) Frequency of heart arrhythmias (one‐lead ECG) and heart
Participants were asked to separately sign a consent form for:
murmurs (auscultation)
1) consent to participate in the survey along modalities stated
q) Assessment of bone mineral density (ultrasound of
in the invitation letter (no participant declined); 2) consent
calcaneus)
for blood to be used for genetic tests, and 3) consent to be
r) Exposure of the population to mass media, particularly in
possibly contacted in the future for possible follow up related
relation to health programs, and use by the population of
to any possible follow up of the survey.
new communication technologies
All participants retained the right to decline any question or
s) Assessment of a number of social variables and their
any test.
association with the variables measured in the survey
t) More generally, the survey provides broad information The original paper consent forms will be kept for 5 years in a
(medical, social, environment, etc) that can be useful for locked room and a scanned copy of all consent forms will be
tailoring NCD prevention and control programs. kept for at least 10 years.
Communication of results to the participants
Methods and participants for the 2013 survey Before being discharged from study centers, participants
received information on their own results, with relevant
Selection of participants advice, from the medical doctor of the survey.
The survey was performed in a sex and age stratified random Participants with a newly found abnormal medical condition
sample of all adults aged 25‐64 years of Seychelles between received a referral form signed by the doctor of the survey (a
October and December 2013 on Mahé and during 2 weeks in copy of which is kept at UPCCD) and were advised to go to a
February 2014 in the islands of Praslin and La Digue. These three health center or to a specialist clinic to confirm or manage
islands account for >98% of the total population of Seychelles. the condition.
The eligible sample was extracted from the population registry. Participants who presented a serious medical condition were
sent to the casualty for further diagnosis or care.
The survey was attended by 1240 adults, with a participation rate A letter with selected results was sent to each participant
of 73%. Participants were invited to attend the survey on shortly after the visit to the survey center.
selected days in study centers located in Mahé, Praslin, and La
Digue. Non participants were actively traced (telephone, local
administration, announcements on radio, etc) and invited to
attend the survey. Since participants were randomly selected
8
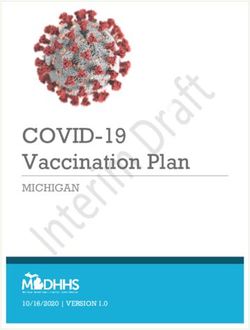
Population and mortality, Seychelles, 1989‐2013 health care occurring in the interval. Decreased age‐specific
mortality is consistent with substantially increased life
These data are compiled from Seychelles vital statistics of the expectancy in Seychelles over the past 25 years.
Ministry of health and from the National Bureau of Statistics.
Data on health outcomes in relation to CVD shown in this page Figure 3. Total numbers of cardiovascular disease, cancer and
help put results of the 2013 and other surveys in context. other broad causes of deaths between 1989 and 2013
800
Figure 1. Population of Seychelles between 1989 and 2013 669
651
700
100'000 543 559
7.0k
6 .5k 7.8% 600
7.8%
272 Other
Deaths per year
5 .1k 276
80'000 4.2k 7.0%
500
6.4% 233 235 Cancer
400
Population (k)
60'000 35k 49k CVD other
32k 49% 65+ 118
25k 55% 300 115
37% 43% 80 96 Stroke
25‐64
40'000 200 121 139 MI
96 102
9
Participation to Seychelles NCD surveys are less older than young people in the population, the sampling
strategy was designed to include similar numbers of participants
Table 1. Participation to the 2013 NCD Survey by age and sex in each of four 10‐year age categories (i.e. random sex and age
stratified sample from the total population aged 25‐64 years).
25‐34 35‐44 45‐54 55‐64 Tota l The sample sizes in each of the four surveys are sufficiently large
Men to provide sufficient statistical power to assess the main
El i gi bl e 196 202 217 215 830 objectives of the surveys, i.e. the prevalence of risk factors and
Pa rti ci pa nts 111 109 150 161 531 their trends over time.
Participation (%) 56.6 54 69.1 74.9 64
Of note, similar methods were used in all four surveys in relation
Women
to the sampling strategy (sex and age stratified random samples
El i gi bl e 204 216 222 230 872 of the total population aged 25‐64), questionnaires used (a
Pa rti ci pa nts 162 168 183 196 709 majority of questions were identical in each survey) and methods
Participation (%) 79.4 77.8 82.4 85.2 81.3 used to assess risk factors (blood pressure, BMI, etc). This allows
Tota l both inferring results to the general population of Seychelles and
El i gi bl e 400 418 439 445 1702 directly comparing results across different survey.
Pa rti ci pa nts 273 277 333 357 1240
Participation (%) 68.3 66.3 75.9 80.2 72.9
Participation in the 2013 survey was lower among men (64.0%)
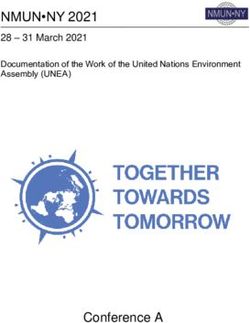
Body mass index (BMI)
than among women (81.3%) and lower among young men than Figure 1. Mean BMI by sex, age and survey year, age 25‐64
older male participants (55.6% among men aged 25‐34 and 54%
among men aged 25‐44). These findings are frequently 32
Men Women
encountered in surveys in all countries. 30
With regards to non participation, we were able to compare
Body mass index (kg/m2)
28
education status among eligible participants who did not 1989
participate and eligible participants who participated in the 2013 26 1994
Survey, as Information on education was available in the sample 2004
of eligible participants provided by National Bureau of Statistics. 24
2013
Education was not different in participants and non‐participants,
22
which gives reasonable assurance that participants and non‐
participants did not differ substantially in terms of socio‐ 20
economic status.
Table 2. Participants in surveys in 1989, 1994, 2004 and 2013.
Mean BMI is higher in women than men, in young than older
25‐34 35‐44 45‐54 55‐64 Tota l
persons, particularly in women. Mean BMI increased markedly
Men
between 1989 and 2013 in all sex and age categories. The
El i gi bl e 196 202 217 215 830 increase of mean BMI between 1989 and 2013 is particularly
Pa rti ci pa nts 111 109 150 161 531 striking in young women aged 25‐34.
Participation (%) 56.6 54 69.1 74.9 64
Figure 2. Age‐standardized prevalence of overweight and obesity
Women
by sex and survey year, age 25‐64
El i gi bl e 204 216 222 230 872
Pa rti ci pa nts 162 168 183 196 709 100
Prevalence of overweight & obesity (%)
Participation (%) 79.4 77.8 82.4 85.2 81.3 Men Women
Tota l 80
El i gi bl e 400 418 439 445 1702
60
Pa rti ci pa nts 273 277 333 357 1240 39 Obese
35
Participation (%) 68.3 66.3 75.9 80.2 72.9 15 22 28 Overweight
40 23
8
The four surveys included similar total numbers of participants,
4
i.e. 1081 in 1989, 1067 in 1994, 1255 in 2004 and 1240 in 2013. 20 36 35
30 32 33 33
Participation rates in the surveys in 1989, 1994 and 2004 24 28
exceeded 80% and participation in 2013 was 73%. These 0
participation rates are excellent for such exanimation surveys, 1989 1994 2004 2013 1989 1994 2004 2013
and allow generalizing findings to the entire population of
Seychelles. Participation to examination surveys, for which Between 1989 and 2013, the prevalence of combined overweight
2
participants have to come to designated study centers, is often (i.e. slight excess of weight, BMI: 25‐29 kg/m ) and obesity
2
lower than 50% in high income countries. (marked excess of weight, BMI ≥30 kg/m ) doubled in men (from
28% to 57%) and also markedly increased in women (from 51% to
To maximize the statistical power of estimates of the variables 72%).
assessed in the survey in all age categories considering that there10
Figure 3. Total numbers of overweight and obese persons by sex aged 26‐64 in 2013). This predicts high numbers of persons with
and survey year, age 25‐64 complications in near, middle and long terms.
30'000 Figure 6. Mean BM by sex, socio‐economic status and survey
Men Women year, age 25‐64
25'000
32
8'070
20'000 Men Women
Mean body mass index (kg/m2)
8'673 30
6'662
15'000 Obese
7'466
28
Overweight
4'195 Non manual
10'000
17'822
4'757 26
14'015 2'828 13'664
Manual
5'000 2'932 10'569
8'546 Unskilled
6'107 24
5'453
3'496
0
22
1989 1994 2004 2013 1989 1994 2004 2013
20
Because of the increasing and aging population between 1989 1989 1994 2004 2013 1989 1994 2004 2013
and 2013, the increasing prevalence of overweight and obesity
over time results in increasing numbers of overweight and obese There is a strong sex‐specific social patterning of body weight in
persons in the population (48’830 aged 25‐64 in 2013). all surveys. BMI is higher among women of low than higher SES
Figure 4. Age‐standardized prevalence of categories of BMI, age while BMI is markedly higher in men of higher than lower SES.
25‐64 Figure 7. Perceived ideal body shape by sex, BMI and SES
Men Women 5.0
0.3 0.0 0.9 1.5
100
Perceived ideal body shape (scale 1‐9)
0 1 1.8
4 7
2 4 6
4.0
5
4.5 6.7 Men Women
12 11 4.5
16 10
24 15
Age standardized prevalence (%)
80 18
30 20 ≥40
22 4.0
36 35‐39
35 28
60 30‐34
32 3.5 Manual
33 25‐29
33 Non manual
40 66
18.5‐24 3.0
5711
Figure 9. Men taking currently concrete measures to control their Tobacco use
body weight by age and SES indicators, (green: yes; red: some effort; Figure 1. Age standardized prevalence of occasional and daily
blue: no)
smokers by sex, age and survey year, age 25‐64
60
Men Women
3.2
50
Prevalence of smoking (%)
40 4.6
7.7
30 5.9 Occasional
50.3 Current
20 36.5
30.8 28.3 0.8
1.3
10
2.6
9.8 2.0
6.8 5.1
3.9
0
Substantial proportions of men, with a marked difference 1989 1994 2004 2013 1989 1994 2004 2013
according to higher vs. lower SES; take measures to control
weight in the total population. The prevalence of daily smokers is much higher in men than
women. The prevalence decreased between 1989 and 2013 in all
Comments age categories in men. The prevalence tended to increase in
BMI (i.e. body weight) largely increased over time in Seychelles in women between 2004 and 2014.
all sex, age and SES categories. High BMI is associated with many Figure 4. Age‐standardized number of cigarettes smoked per day
detrimental heath conditions, including diabetes, high blood among daily smokers, by sex and survey year, age 25‐64
pressure, dyslipidemia, osteoarticular problems, etc. It is the
main cause of the increasing prevalence of diabetes in the 14
population (“diabesity”).
Number of cigarettes smoked per day
12
The 2013 Survey identified marked differences in men vs women, 10
among daily smoker
and differ SES categories, in relation prevalence of obesity and in
associated factors, such as perception of ideal body weight, and 8 Men
attitudes (efforts to lose weight). These variables will be analyzed 6 12.7 12.3 Women
in further detail as they bear important significance in terms of 10.4
4 8.1
cultural, social incentives/disincentives for people to gain or lose 6.7
7.3 7.2 6.8
weight. 2
The WHO member states, including Seychelles, have agreed in 0
2014 on the target of 0% increase of the prevalence of obesity 1989 1994 2004 2013
and diabetes between 2010 and 2025.
The number of cigarettes smoked by daily smokers, which was
Interventions to reduce body weight at the individual level often much higher in men than women in the past, has decreased in
have little efficacy, except for bariatric surgery. Therefore, weight male smokers, but not in female smokers.
control interventions should address the societal causes of the
obesogenic environment and involve population‐based Figure 3. Prevalence of smoking by sex, socio‐economic status,
interventions in all sectors (education, agriculture, finance, and survey year, age 25‐64
transports, nutrition, food industry:) to enable people to chose
100
healthier diets through awareness campaigns, food labeling, Men Women
tax/subsided on healthy/unhealthy foods; ban on advertising of
80
unhealthy foods, healthy food in canteens of schools/workplaces,
Prevalence of smoking (%)
etc, and in population‐based strategies to engage people to have
more physical activity in their daily lives (e.g. bus/cycling lanes, 60
Laborer
safe sidewalks, public transports, disincentives to use private Manual
cars, etc). 40
Non manual
The WHO 2014 NCD Status Report lists cost‐effective
20
interventions in many sectors to help reduce weight and promote
physical activity in the population.
0
1989 1994 2004 2013 1989 1994 2004 2013
The prevalence of smoking was higher in all surveys in lower vs.
higher SES groups, particularly in men.12
Figure 4. Numbers of regular and occasional smokers by sex and Figure 7. Did anyone smoke in your home when you were
survey year, age 25‐64 present in the past 7 days? (yes: red)
10000
Men Women
8000
1369
1657
468
771
6000
Occasional
Current
4000
6545 6830
5887 6313
2000
97 212 617
428
1070 930 796 1206
0
1989 1994 2004 2013 1989 1994 2004 2013
Nearly 20% of all adults report are exposed to smoke at home,
Even if the prevalence of smoking has markedly decreased in
slightly less often in higher than lower SES households.
men and not markedly increased in women, the total numbers of
smokers has increased over time because of the largely Figure 8. Do you agree with the ban on smoking in enclosed
increasing population between 1989 and 2013. public places, including work places and restaurants? (blue: fully
agree)
Figure 5. Use of pipe, cigars, cigarillos, hand rolled cigarettes and
shisha (n=17) among 354 ever smokers (yes: red)
The prohibition on smoking in enclosed places by law is very
largely supported, including by a large majority of smokers.
The use of tobacco products other than cigarettes is very
uncommon. In addition, most users of other products also smoke Figure 9. Did anyone smoke in enclosed areas in your workplace
cigarettes (data not shown here). when you were present in the past 7 dayss, by sex, age and SES
categories (red: yes)
Figure 6. Proportion of daily smokers who tried to quit in past 12
months in 2013, by sex, age and SES categories (yes: red)
Around 10% of participants report exposure to indoor smoke in
A large proportion of smokers wish to quit. This proportion is the workplace, which suggests the need to improve enforcement
higher among higher than lower SES, consistent with high of the legislation.
prevalence of smokers among low than higher SES. Of note,
attempt to quit are often not successful because of the addictive
nature of nicotine, which emphasizes the need to focus on
measures to prevent smoking uptake at the first place.13
Figure 10. Received advice on smoking cessation from a health areas that need be improved so that the prevalence of smoking
officer in past 12 months, among 127 smokers who visited a keeps decreasing in Seychelles and the target of a 30% decrease
doctor in past 12 months (yes: blue) between 2010 and 2025 can be achieved.
As the first country to have ratified the Framework Convention
for Tobacco Control in the African region, Seychelles should aim
at implementing best practices in tobacco control in the region.
Alcohol use
Figure 1. Mean daily intake of ethanol by sex, age and survey
year, age 25‐64
100
90 Men Women
Ethanol per day on average (ml)
80
70
Only a third of smokers receive advice to quit smoking during
60 25‐34
medical visits. This advice should be repeated at all visits as
50 35‐44
studies show that advice to quit smoking by doctors is cost
40 45‐54
effective.
30 55‐64
Comments 20
10
The age‐adjusted prevalence of smoking decreased over time as
0
well as the number of cigarettes smoked per day in male
1989 1994 2004 2013 1989 1994 2004 2013
smokers. This decrease is one factor that underlies the marked
decrease in the age‐adjusted mortality rates of cardiovascular Volume of drinking (ml ethanol per day and per capita on average
diseases and lung cancer between 1989 and 2013. Decreasing = alcohol intake per capita) is much lower among women than
prevalence of smoking (men) likely reflects the high profile men and has decreased markedly over time in men. Consumption
tobacco control program in Seychelles since the late 1980s, which was not assessed in 1994 for persons drinking alcohol less than
includes continued awareness programs, fairly high tax on weekly but this has little impact on mean drinking volume.
tobacco products (>65% of total cost of cigarette packet in 2014),
and impact of comprehensive legislation on tobacco control in The decrease in mean alcohol intake per capita over time in men
2009 (i.e. total ban on smoking in enclosed public places an is likely largely driven by the marked decreased consumption of
selected open public spaces, total ban on tobacco advertising, homebrews over time, which accounted for as much as 50% of
promotion and sponsorship, etc). the total ethanol intake in 1989 (mainly among men) but is only
minimal in 2013. The decrease is also driven by the decrease over
However, the total numbers of smokers in the population is still time of heavy drinkers (>75 ml/day), which also used to be
both high and increasing over time, which emphasizes the need strongly associated with homebrew drinking.
to further strengthen tobacco control program as a main public
health priority. Figure 2. Mean alcohol intake by sex, socio‐economic status and
survey year, age 25‐64
This emphasizes that interventions to reduce tobacco use should
be strengthened. This includes ensuring complete enforcement 120
of the ban on smoking in public places with regular monitoring by Men Women
inspectors and spot fining smokers and managers when smokers 100
Mean ethanol per day (ml)
smoke in non authorized areas, as prescribed by the law; swift
80
implementation of rotating health warnings on tobacco packets
as requested by the law and the FCTC; further tax increases at Laborer
60
regular intervals at greater pace than inflation, so that the ratio Skilled manual
of tax/total cost is larger than 75%); and continued health 40
Non manual
education programs in all settings.
20
It is also necessary that a cessation smoking program is provided
by health services to help smokers who wish to quit, including
0
free provision of nicotine replacement medications. 1989 1994 2004 2013 1989 1994 2004 2013
The WHO member states, inclusive Seychelles, have agreed on a
Ethanol intake differed largely by socio‐economic status (SES) in
30% relative reduction in the prevalence of smoking between
men, with much higher intake of alcohol in low than higher SES
2010 and 2025. The WHO 2014 NCD Status Report provides a list
men. However, the difference decreased markedly over time,
of cost‐effective interventions for tobacco control.
likely driven by the marked decrease in homebrew drinking. It
All tobacco control interventions and policies implemented in was mostly person of lower SES who used to drink inexpensive
Seychelles are reported in the Reporting Instrument submitted homebrews, and drank it in large amounts, in past surveys (as
every 2 years to the Conference of Parties to the Framework found in past surveys). Homebrew drinking has virtually
Convention of Tobacco Control. It is necessary to address all disappeared in recent years and consumption now almost14
entirely relies on commercial beverages, highly taxed. High price and moderate drinkers, and the increasing population between
of alcohol beverages is an effective measure against heavy 1989 and 2013, result in largely increasing numbers of light and
drinking and one could even expect a reversal of the social moderate drinkers over time, both male and female.
gradient in heavy drinking (as already apparently seen, at a small
scale, with higher alcohol intake in women of higher vs. lower
SES. Figure 5. Number of drinks on a typical week day by sex, age and
socio economic indicators (orange: 3; grey: 4; red:5+)
Figure 3. Age‐standardized prevalence of categories of drinkers,
age 25‐64 (1‐29 ml/day = 1‐2 drinks per day on average; 30‐75 ml/day =
3‐ 5 drinks; ≥75 ml/day >5drinks)
100
Men Women
80
Prevalence of drinkers (%)
11
60 34 >75 ml/d
14
30‐75 ml/d
28
1‐29 ml/d
40 22 1
6
24
22
3
5
20 17
1
34 3 35
19 22 20
11 14
2
1
0 3
1989 1994 2004 2013 1989 1994 2004 2013 Figure 6. Number of drinks on a typical Friday (orange: 3; grey: 4;
red: 5‐10: blue grey: 11‐20)
The prevalence of heavy drinkers (≥5 drinks per day on average),
which was high in men in early surveys (1989, 1004) has
decreased over time but is still substantial (nearly 11% of men in
2013). However, the prevalence of both moderate drinkers (1‐2
drinks per day) and marked drinkers (3‐5 drinks per day) has
increased over time in both men and women.
Of note, alcohol intake was not assessed in 1994 for persons
drinking less than once weekly and the prevalence of category 1‐
25 ml/day is underestimated in 1994. This has impact on
estimation of the frequency of light drinkers but only little impact
on the estimation of on total alcohol consumption.
Figure 4. Total number of drinkers of light, moderate, marked
and heavy amounts of alcohol by sex and survey year, age 25‐64
30'000
Figure 7. Number of drinks on a typical Saturday, (orange: 3; grey:
Men Women
237 4; red: 5‐10: blue grey: 11‐20)
25'000
1422
2698
132
20'000 645
2814 247 8496 >75 ml/d
6735 2894
220 30‐74 ml/d
15'000 3532 4916 433
497 1‐29 ml/d
2671 361
4403 4605 8294
10'000 1967 2316 0 ml/d
16713
2967 14461 14259
5'000 2389 8460 8506
8046
6381
3380
0
1989 1994 2004 2013 1989 1994 2004 2013
Note: 1‐29 ml/d = 1‐2 drinks/d; 30‐75 ml/d =3‐5 drinks/d; >75
ml/d, >5 drinks/d. Alcohol consumption was not assessed in 1994
for persons drinking alcohol less often than once weekly, hence
the frequency of drinking 1‐25 ml/day is under‐estimated and the
category of 0 ml/day is overestimated in 1994.
Although the prevalence of heavy drinkers (>5 drinks per day on
average) has decreased over time, the total number of heavy
drinkers remains high with nearly 3000 male heavy drinkers in
2013. The cumulating effect of the increasing prevalence of light15
Figure 8. Number of drinks on a typical Sunday (orange: 3; grey: 4; Figure 10. Number of days drinking more than 4 (women) or 5 (men)
red: 5‐10: blue grey: 11‐20) drinks per month (orange: 5‐10; grey: 11‐15; red: 16+)
Around 20% of all adults drink vey high amounts of alcohol on
Few adults drink on workdays but high proportions drink on more than 5 days per month and around 10% of all adults drink
Fridays and Sundays with even higher proportions drinking on excessive alcohol amounts of alcohol on more than 10 days per
Saturdays. This suggests binge drinking patterns in many month. Binge drinking is more frequent in male vs. female and in
drinkers. persons of lower vs. higher SES. There was little difference
between young and older persons. Overall, these figures show
Figure 9. Proportion of persons drinking homebrews (kalou, baka,
high frequency of binge drinking, with many men and women
lapire) among 665 current drinkers (yes: blue)
drinking in excess on many days per month.
Comments
Ethanol consumption per capita decreased over the past 25
years, largely driven by both a marked decrease of heavy drinking
among men and a largely decreasing consumption of homebrews
between 1989 and 2013.
However, while the prevalence of heavy drinking (>5 drinks per
day on average) has decreased, the frequency of light and
moderate drinking has increased among both men and women.
Because the population has largely increased, the total numbers
of heavy drinkers in the population (mainly men) remains high,
and the numbers of drinkers of 1‐2 and 3‐5 drinks per day on
Homebrew drinking was very low in 2013, and was higher in male average have largely increased. This implies large and further
vs. female, older vs. young, and lower vs. higher SES persons. increasing numbers of health, social and other alcohol‐related
Figure 10. Number of drinks (any type) in a single day on special problems, e.g. larger numbers of drunk drivers on the roads.
occasions (green: 6‐10, orange: 11‐15; grey: 16‐20; red: 21+) A further important problem is that alcohol is often consumed
along a binge drinking pattern (i.e. high intake on few occasions).
Binge drinking (as compared to regular low intake) is associated
with many health and social problems (heart attack, drunk
driving, violence, etc).
Findings in the different surveys between 1989 and 2013 confirm
that alcohol misuse remains a main public health issue in
Seychelles and requires a strengthened public health response,
e.g. frequent random alcohol checks of all drivers in sensitive
points (discotheques, social gatherings at night, etc), high taxes
on alcohol beverages on a basis of alcohol content of beverages,
severe penalties for drunk driving, ban on advertisements of
alcohol beverages in public mass media, awareness campaigns,
etc).
Around 20% of all adults report drinking >10 drinks on single
special occasions. This proportion is higher in male vs. female, The WHO member states, inclusive Seychelles, have agreed on a
young vs. old, and lower vs. higher SES persons. Binge drinking 10% relative reduction of the prevalence of harmful use of
(irregular drinking with high amounts on drinking sessions) has alcohol between 2010 and 2025. The WHO 2014 NCD Status
numerous health and social detrimental outcomes. Report provides a list of cost‐effective interventions in multiple
sectors to reduce alcohol misuse in the population.16
Dietary habits The proportion of people drinking full cream milk is high and
does not differ according to SES categories. Awareness
Figure 1. Patterns of dietary habits, based on food frequency campaigns should encourage people drinking semi‐skimmed milk.
questionnaire, age 25‐64
Figure 4. Number of spoons of sugar added in tea or coffee, (blue
daily 5-6 d/wk 3-4d/wk 1-2 d/wk17
Figure 7. Do you use olive oil when cooking or to add in salad, Taking vitamin supplements has been associated with adverse
(blue: never; red: rarely, green 1‐2 times/wk, orange: ≥2 times/wk) health effects in many studies.
Figure 10. Do you read labels on food packages to help you
decide, e.g. to look for salt, sugar or fat content (blue: never; green:
sometimes; red: rarely; orange: often)
The consumption of olive oil (a healthy oil rich in mono‐
unsaturated fatty acids) is unexpectedly high in the population
and likely a new trend, likely reflecting health consciousness,
impact of health education programs, and recent decrease in the
price of olive oils. Consumption of olive oil is markedly higher in Few people read food labels, and many of those who read labels
higher v. lower SES persons, possibly reflecting both a cost issue said they read mostly expiry dates. There is a need for health
and better health awareness. education programs to raise this issue, as well as policy measures
to regulate the content and format of food labels so most people
Figure 8. How Important to you is lowering the salt content in can understand them and help them chose healthy products.
your diet (blue: not; red: a bit important; green: very important)
Comments
Fish, unpolished rice and sugared tea continue to be the staple
diet in Seychelles. Of note, these items do not include a number
of nutrients so the trends towards a more diverse diet are
welcome to provide healthy micronutrients and vitamins.
A few other items are consumed frequently in 2013, e.g. bread,
vegetables, fruit, lentils, breakfast cereals, milk, and cheese.
Intakes of meat, processed meat, potatoes, potato chips, and
pasta are still low (although likely largely increased compared to
past years). Consumption of poultry is more frequent. Intake of
salted and sweet snacks is substantial.
The data do not provide information on portion sizes. Therefore
The proportion of people reporting paying attention to salt
high frequency of eating an item per week (e.g. “vegetables”)
reduction (a main measure for reducing blood pressure) is high in
does not necessarily mean that a product is consumed in large
the population, likely reflecting ongoing awareness campaigns on
amounts. For example, a large proportion of people report eating
this issue. This proportion of persons trying to reduce salt intake
salad on most days of the week, but the amount of salad actually
is higher among female vs. male, older vs. young, and higher vs.
found in plates in Seychelles (in grams) is often very low.
lower SES persons.
Overall, a more varied diet, as found in the 2013 survey, has
Figure 9. Took vitamins during last 4 weeks (red: yes)
advantages in providing a broader range of nutrients and
vitamins (e.g. bread, cheese, milk, breakfast cereals,) which are
not present in rice and fish. However, the current diet also
includes substantial intake of nutrient poor and energy rich food
items (e.g. large amounts of sugar added in tea/coffee, soft
drinks, juices in packets, salted and sweet snacks, processed
meat, etc). These nutrients contribute large amounts of sugar,
salt, saturated fats or trans fats, which are main causes of
cardiovascular disease. Sugared drinks have little nutritional
value and contribute large energy intake and, therefore, fuel the
raising prevalence of obesity.
There is a need to sustain health education campaigns on healthy
nutrition, e.g. emphasizing on five portions of vegetables and
(fresh) fruit a day, need to prefer water (including tap water),
The proportion of adults taking vitamins is high, possibly
semi‐skimmed milk and fresh fruit juices to soft drinks of packets
reflecting health concerns. Yet, there is no medical reason for
of fruit juices.
healthy people having a proper diet to take vitamin supplements.You can also read