NATIONAL COVID-19 DEPLOYMENT AND VACCINATION PLAN - SURINAME 2021
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

NATIONAL
COVID-19
DEPLOYMENT AND
VACCINATION PLAN
SURINAME 2021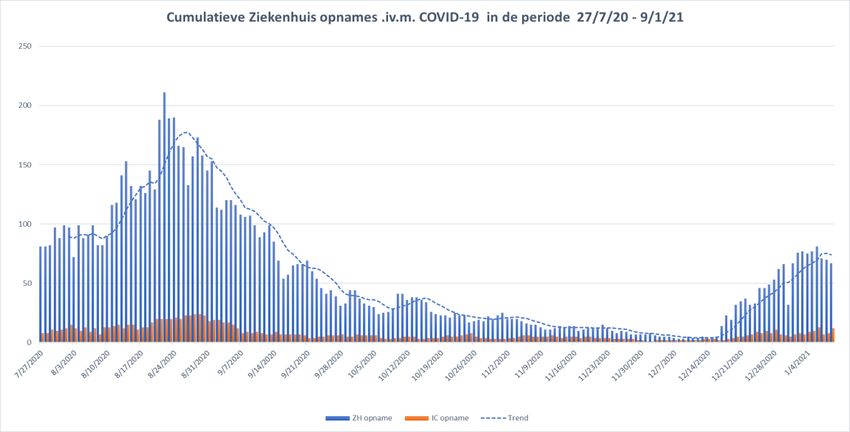
Endorsement
COVID-19 started at the end of 2019 in Wuhan, Hubei Province in China. Due to the rapid
spread to several countries with, increasing reports of morbidity and mortality, the World
Health Organization (WHO) declared the disease a Public Health Emergency of International
Concern on January 30, 2020, and a global pandemic on March 11, 2020.
Suriname detected its first case of the disease on Friday, March 13, 2020. Since December
2020, the country is experiencing the second wave of the disease, and the increasing cases
and deaths are of concern to the country. In the absence of definitive therapeutic options for
the management and control of this disease, vaccination as a primary prevention measure is
a good option for the control of the disease in terms of saving lives through reduction of
severe disease and deaths.
The COVAX Facility is a mechanism for the equitable access to various vaccine options, and
Suriname has signed onto this facility to receive allocation of vaccine doses which have
received approval from the WHO and other Stringent Regulatory Authorities.
In order to protect the population against the disease, the Government of Suriname has
appointed the “Technical Advisory Commission Immunization Policy COVID-19” for the
general management and monitoring of the COVID-19 situation in Suriname, and a
“Vaccination Committee” to develop a vaccination plan and to guide the implementation of
this plan.
Relevant Ministries of the Government of Suriname, and relevant public and private
institutions have been involved in the planning of the campaign, and will continue their
support to the further implementation of this plan. Specific measures with regard to funding
of the campaign, as well as facilitating the approval of the vaccine for use by the Registration
Commission, tax exemptions, customs clearance, safe arrival, receipt, and storage of the
vaccine and ancillary needs, have been taken.
The vaccination campaign will start soon after the arrival of the first batch of vaccines, that
will cover up to 3% of the population, beginning with the first priority group of frontline
healthcare workers.
Suriname is open to consider at due time the availability of other vaccines that may be
beneficial in terms of cost, dosing schedule, cold chain storage requirements and other
factors. The vaccination plan has been developed to consider all possible options.
The Ministry of Health is thankful for the efforts made, and those that will continue to be
made by all stakeholders and partners towards a successful fight against this disease.
A. Ramadhin, MD
Minister of Health
Republic of Suriname
1Table of contents
Contents
Endorsement .............................................................................................................................. 1
Table of contents ........................................................................................................................ 2
Executive summary .................................................................................................................... 3
1. Introduction ........................................................................................................................ 7
2. Regulatory preparedness................................................................................................... 11
3. Planning and coordination of the vaccine introduction .................................................... 13
4. Resources and funding...................................................................................................... 15
5. Target populations and vaccination strategies .................................................................. 17
6. Supply chain management and health care waste management ....................................... 36
7. Human resource management and training ...................................................................... 39
8. Vaccine acceptance and uptake ........................................................................................ 42
9. Vaccine safety monitoring and management of AEFI and injection safety ..................... 44
10. Immunization monitoring system ................................................................................... 45
11. Disease surveillance ....................................................................................................... 46
12. Evaluation of introduction of COVID-19 vaccines ....................................................... 46
Annex 1: Detailed budget for the COVID-19 Vaccination Campaign ................................. 48
Annex 2: ESAVI................................................................................................................... 53
Annex 3: Terms of Reference for the National Coordination Team .................................... 58
Annex 4: Implementation Plan ............................................................................................. 61
2Executive summary
Since December 2019, there have been more than 101 million cases of COVID-19
worldwide, including more than 1.2 million deaths. In order to control the pandemic, in
addition to preventive hygiene measures, effective vaccines are needed to protect against
COVID-19, especially in the pursuit of a situation without restrictions on international travel
and trade including lockdowns, quarantine and isolation.
A global effort to develop vaccines has been underway since the start of COVID-19. Several
vaccine candidates are in various stages of development and to date, some of these have
already received Emergency Use Listing by the WHO. Others are expected to receive similar
approval for emergency use in the very near future.
Suriname has committed itself to the COVAX Facility, the vaccine arm of the Access to
COVID-19 Tools Accelerator (ACT) which aims to facilitate equitable access to 2 billion
doses of vaccines for countries by the end of 2021.Through this agreement, Suriname
already has the guarantee of receiving vaccines to be able to vaccinate 20% of its
population.
This plan carefully develops the important processes and procedures required for vaccine
regulatory approval, arrival, storage, distribution, administration, registration, logistics,
surveillance, reporting, safety monitoring and evaluation. This documentation is necessary in
preparation for a responsible and successful course of the national COVID-19 vaccination
campaign. The plan follows the “WHO Guidance on Developing a National Deployment and
Vaccination plan for COVID-19 vaccines” and contains the following main components, with
an estimated budget of USD 16,047,881 for the vaccination of the identified priority groups.
Component
1. Introduction
2. Regulatory preparedness
3. Planning and coordination of the vaccine introduction
4. Resources and funding
5. Target populations and vaccination strategies
6. Supply chain management and health care waste management
7. Human resources management and training
8. Vaccine acceptance and uptake
9. Vaccine safety monitoring and management of AEFI’s and
injection safety
10. Immunization monitoring system
11. Disease Surveillance
12. Evaluation of introduction of COVID-19 vaccines
The National COVID-19 Deployment and Vaccination Plan is an important and necessary
condition to receive the COVID-19 vaccine. The Technical Advisory Commission
Immunization Policy COVID-19 is a multidisciplinary group of national experts responsible
for providing independent, evidence-based advice to policy makers and program managers
on policy issues related to immunization and vaccines. The committee is able to review the
international and regional policy guidelines of the WHO’s Strategic Advisory Group of
Experts on Immunization (SAGE) and the PAHO Regional Technical Advisory Group on
Immunization (RITAG), taking into account the national context, national priorities and
disease epidemiology. The committee will regularly review, revise and update its
recommendations to national policymakers, as new evidence becomes available.
3The Government of Suriname is committed to follow international actions and procedures to
save lives, and mitigate the effects of the COVID-19 pandemic, by implementing all relevant
actions, including vaccination of its population, in order of priority groups that have been
identified by the Technical Advisory Commission Immunization Policy COVID-19. Supporting
sub-committees and teams have been identified to support the work of this Technical
Advisory Commission:
- The National Coordination team to present this Plan and lead the campaign
activities, with support of sub groups for:
• Personnel: mobilization, training, evaluation.
• Finances: Funding, budget management, coordination of payments to service
providers and personnel.
• Information/Education: Development and dissemination of informational
material and messaging to generate demand.
• Logistics and Transportation: Vaccine clearance, mobilization of
transportation, distribution schedules.
• Supply chain management: Forecasting procurement, stock management,
materials for the teams and vaccination sites.
• Secretarial support: keeping notes of meetings, consolidation of reports by
supervisors, consolidation of administrative information, and supervision of
the end report.
• Partnerships: Coordination of contact with external organizations, mobilization
of private sector, donations and sponsoring.
- The Implementation Team, with the rayon (district area) coordinators of the Medical
Mission Primary Health Care Suriname (MM), the Regional Health Services (RGD),
the Bureau of Public Health (BOG) and the hospitals, for operations management
including monitoring and supervision.
- The Central Administrative Team at the BOG.
- The Vaccination Teams at the health facilities managed by the MM, the RGD, and
other public and private health facilities.
For the National Immunization Program (NIP) of Suriname, the “Bedrijf Geneesmiddelen
Voorziening Suriname (BGVS)” (State Drug Supply Company) is responsible for all actions
towards preliminary administrative matters, payment of fees and taxes, customs clearance
and transportation of the vaccines received through the PAHO Revolving Fund for Access to
Vaccines, following rules of cold chain, from point of arrival to point of storage.
Within this authority, the BGVS will do the same for the vaccines and dry store items that will
be received for the COVID-19 vaccination campaign.
The received vaccines will be stored in the facilities of the Wanica Streekziekenhuis that
complies with cold chain regulations, and has sufficient Ultra Cold Chain (UCC) and regular
storage capacities for the expected number of vaccines. The Wanica Streekziekenhuis also
has secured space and facilities available for administrative matters of the distribution of
vaccines and supply items that need to be kept in stock for the vaccination campaign.
4The distribution of the vaccines will follow the guidelines and procedures as outlined in this
plan of action. In summary:
Day of arrival of vaccines Arrival and storage of the vaccines at the Wanica
Streekziekenhuis, under responsibility of the National
Immunization Program.
Two to three days leading The National Coordinating Team will provide an overview of
to vaccination the scheduled dates and vaccination sites, and the needed
quantities of the vaccines and ancillary items. The
vaccination sites will have received prior approval by the
National Coordinating Team to receive, store, and further
distribute these to the outreach sites under their
responsibility. Vaccination sites will be inspected to ensure
that the site complies with the protocols for COVID-19
vaccination.
Day before Vaccination/ The Supply Chain Manager of the National Coordinating
Day of vaccination Team will distribute the requested quantities of vaccines to
the vaccination sites, taking into account the rules with
regard to cold chain management.
After vaccination All unopened vials, reconstituted vials with unused doses,
and empty vials from the vaccine sites will be returned to the
Supply Chain Manager of the National Coordinating Team,
taking into account the rules of vaccine safety, the open vial
policy and waste management. This can also be used as a
double check for the registration of the administered
vaccines.
Suriname has subscribed to the COVAX Facility as a self-financing member for an initial
coverage of 20% of the population. The vaccines will be delivered in tranches and
proportional to the population.
• The first tranche expected in the second half of 2021 is to cover vaccination of
healthcare and social workers which is estimated at 3% of the population.
• The second tranche is to cover vaccination of high-risk adults (elderly 60 years and over,
and adults with underlying conditions) estimated at 17% of the population.
• The third tranche will cover vaccination for other priority groups.
To cover more than 20% of the population will depend on the disease context in the country,
participants’ vulnerability and the COVID-19 threat. Subsequent doses will become available
in the course of this year and 2022. The regimen for the expected vaccine depends on the
vaccines to be received, in general 2 doses per person. During the process, the country
might decide to access other vaccines to cover a larger proportion of the population, as they
become available. If so, then this plan and budget, and the implementation details will be
adapted accordingly.
The target estimated date for the first administration of the vaccine in the country is 7 (seven)
days after arrival, provided that all other needed items, such as appropriate syringes,
needles, diluents (if needed), and the logistics are in place.
Table 1 provides an overview of the target groups in order of priority, as identified by the
National Coordination Team, and the doses that will be needed to vaccinate these risk
groups in two rounds, including a wastage rate of 10%.
5Table 1: Priority groups and vaccine doses needed for 2 doses regimen
Priority Population Persons Doses needed
Group 1 Healthcare workers, first line 1,497 2,994
Group 2 Healthcare workers, second line 3,794 7,588
Group 3 Military, police, penitentiary officers, Government Officials 3,500 7,000
Group 4 Populations in elderly homes, including dialysis patients 2,900 5,800
Group 5 Elderly sixty years and over, national level 90,170 180,340
Group 6 Adult population, based on medical grounds/risk factor 30,000 60,000
(Diabetes Mellitus, High Blood Pressure, Sickle Cell
Anemia, Cardio vascular Diseases, COPD, Oncologic
Diseases, Indigenous population. (40 – 59 years)
Group 7 Adult population, based on medical grounds/risk factor 11,000 22,000
(Diabetes Mellitus, High Blood Pressure, Sickle Cell
Anemia, Cardio vascular Diseases, COPD, Oncologic
Diseases, Indigenous population, ….) (18 – 39 years)
Group 8 Other risk groups 1,100 2,200
Group 9 Healthy population (18 - 59 years) (estimated) 265,779 531,558
Total 409,740 819,480
Wastage rate 10% 81,948
Grand total 901,428
The leading week will also be needed for preliminary activities, before the actual date of
commencement of vaccination.
The first batch of vaccines to be received will be administered to the health workers,
identified as the first priority group. These health workers will preferably receive their
vaccination in the institutions where they are employed.
The procurement of the vaccine and the vaccination against Covid-19 will be done within a
national strategy, with joint funding from the Government and the private sector. A national
fund will be set up, whereby fundraising will be done with the joint effort of the Government,
the business community, and other stakeholders. To this end, consultation has already been
held with various stakeholders, investors, insurance companies, gold mining companies and
the business community. The Government has accepted the willingness of these partners to
support local fundraising.
The estimated budget for the campaign is summarized as follows:
Table 2: Estimated budget by category
Category Budget
Political priority and legal framework (USD) 50,000
Planning and coordination 68,000
Biologicals (vaccines) and supplies 11,433,913
Cold chain 72,600
Training 27,000
Social mobilization 333,150
Operating costs 2,017,530
Supervision and monitoring 145,000
Epidemiological surveillance (including AEFI 195,140
management)
Information systems 186,650
Research 12,000
Evaluation 48,000
TOTAL 14,588,983
Miscellaneous 10% 1,458,898
Grand total 16,047,881
61. Introduction
COUNTRY BACKGROUND
The Republic of Suriname, bordered by French Guyana in the east, Brazil in the south,
Guyana in the west and the Atlantic Ocean in the north, is located on the northeast coast of
South America. The country has a total area of 163,820 km2 and consists of narrow coastal
plain with swamps, hills and tropical rainforest.
The country is divided into ten administrative districts that are subdivided into 62 regions.
The coastal area comprises 2 urban districts and 6 rural districts, and the interior has 2
districts. The 2 urban districts, the capital city
Paramaribo and Wanica, cover 0.5 % of the
landmass and contain 70% of the total
population.
The vital statistics profile by the Algemeen
Bureau voor de Statistiek (General Bureau of
Statistics) shows a mid-year population in
2018 of 590,100.
The number of registered live births is about
10,000 to give a crude birth rate of 20 per
100,000 and a total fertility rate of 2.5.
Mortality has remained relatively stable at
around a crude death rate of 6.5 to 7 per
100,000. Life expectancy at birth for males is
69.34 years and for females, 75.01 years.
Demographic Characteristics of the population
The Suriname population has many ethnic backgrounds composed of
- Hindustanis (27.4%)
- Creoles (17.7%)
- Maroons (14.7%)
- Indonesians (14.6%)
- Mixed (12.5%)
- Amerindians (3.7%)
- Chinese (1.8%)
- Others (7%)
Sranan Tongo is the ‘’native language”, the main and unofficial language of the population.
The official language is Dutch, and English is widely spoken.
Health Care Delivery System
The Ministry of Health (MOH) is responsible for the health sector and health system
management, specifically the availability, accessibility and affordability of health care. The
main responsibilities of the MOH are planning, policy development, inspection, coordination,
monitoring and evaluation and setting of standards in the health system. The core-
institutions of the Ministry of Health are the MOH Central Office, the Inspectorates (Medical,
Nursing and Pharmaceutical) and the Bureau of Public Health (BOG).
7Primary Health Care and Prevention
The Ministry of Health is responsible for coordinating the national health care system. The
Bureau of Public Health coordinates preventive health care, supervises and executes
programs that provide information on the distribution of diseases. The Epidemiology Unit
operates a surveillance system on communicable diseases in close cooperation with the
Regional Health Services and the Medical Mission. This system relies on weekly reports
from 31 sentinel stations. At the operational level, the government health care providers
include the government subsidized primary health care organizations such as the Regional
Health Services, covering the population living in the coastal area, and the Medical Mission,
covering the population living in the interior. Primary health care is also provided by the large
group of private General Practitioners, especially in the urban districts of Paramaribo and
Wanica.
Regional Health Services
The Regional Health Services (RGD) has 46 clinics in 8 districts in the coastal area and
provides primary health care services and selective prevention activities to mainly the poor
and near poor. Approximately 150,000 poor and near poor who are registered with the
Ministry of Social Affairs, are covered by a basic package of health services, organized by
the State Health Insurance Fund (SZF). The other clients (estimated 250,000) insured by
the State Health Insurance Fund (government employees, retired civil servants and their
dependents), can also use the services of the RGD, especially in the coastal districts.
Medical Mission Primary Health Care
The Medical Mission Primary Health Care Suriname (MM) is responsible for the primary
health care and selective prevention activities in the interior. This NGO operates 52 clinics in
the interior, with a coordinating center located in Paramaribo, and is subsidized by the
Government. They cover about 60,000 people living in the large interior. Their target group is
mainly Indigenous and tribal people living in close proximity of the rivers and dispersed in the
high lands of south Suriname.
Secondary and Tertiary Health Care
The Ministry of Health operates two general and one psychiatric hospital in Paramaribo, and
three district hospitals in the western coastal district of Nickerie, in the eastern district of
Marowijne, and in the coastal district of Wanica. One of the general hospitals in Paramaribo
is also specialized in Maternal and Child Care. There are also 2 private hospitals in
Paramaribo, the Diakonessenhuis (DH) and the St. Vincentius Ziekenhuis (SVZ). These
eight hospitals have a total of 1500 hospital beds, 3.0 beds/1000 inhabitants. The average
bed occupancy rate is approximately 85%. The average length of stay is 7.9 days.
There are 40 dedicated ICU beds available in 4 of the hospitals.
The first case of COVID-19 was confirmed in Suriname on 13 March 2020. The cases that
followed were quickly traced and isolated, and their contacts were placed in controlled
quarantine. Measures were also announced, air traffic was stopped, and Suriname was
placed in a 'bubble'. Since the start of the epidemic, the government has applied two
important measures to curb the epidemic, namely isolating infected individuals and placing
their close contacts in home quarantine. General measures included wearing mouth-nose
masks in public places, keeping physical distance, prohibiting public transportation and
limiting the number of persons who are allowed to gather in one place.
In the month of December 2020, the 2nd wave of COVID- 19 cases began in Suriname. The
reproduction rate (R) quickly climbed to 3.3. Strict measures were promulgated to bring this
back down, due to a strict enforcement policy from the government. The reproduction rate
went down, but the many cases that were already present in society resulted in many
patients. In the second week of January 2021, 91 people with COVID-19 had been admitted
to hospital, 10 of whom were in intensive care, and in addition, 299 people with COVID-19
8were in isolation. The reproduction rate in the second week of January 2021 was still above
one (1), which means that the number of COVID-19 cases will continue to increase.
With the second wave that started in the first week of December 2020 there was a fairly
sharp increase in the number of hospital admissions from the third week of December 2020
onwards.
Up to 11 January 2021, a total of 138 people has died from COVID-19, with 21 people dying
during the second wave that started in December 2020. The picture in these deceased has
not changed from the 1st wave of the epidemic in terms of risk factors; the case fatality rate
(CFR) till early December was ~2.2%. For the new wave, counting from mid-December, the
CFR is ~ 2.0%.
The average age of the admitted patients was 69 years and 80% was 60 years and older.
The youngest person was 45 years old. More than 80% of these individuals suffered from
underlying conditions. More than half had both diabetes and hypertension in their history.
Among these individuals, more than half had already suffered complications from these
chronic diseases such as stroke and chronic kidney failure. There were 4 patients on dialysis
included in this group. A number of people that were admitted due to poor clinical condition,
died shortly after admission.
Graph: Cumulative Hospital admissions COVID-19, 27 July 2020 – 9 January 2021
In this second wave of COVID-19, the spread occurred much faster in a shorter time than
during the first wave. Partly, this is because people wait too long to seek testing, and
therefore stay longer in their infectious and clinical period before seeking care. Isolating
infected people is less effective. It is therefore important to start testing as soon as possible,
preferably on the day of onset of symptoms. It has not yet been established if the fast spread
could be the result of a more infectious virus strain.
The most affected age groups of the confirmed cases remain primarily the productive age
groups of 30 – 39 years, followed by 20 - 29 years, 40 - 49 years and 50 - 59 years. These
age groups account for 79.7% of all cases. There is a slight rise of infections among the age
groups between 20 - 49 years, since the second wave commenced.
9Lessons learned from Influenza A-H1N1 and other relevant activities
The country has had previous experience regarding vaccination in response to a pandemic
and will benefit from the lessons learned during that campaign. The Influenza A-H1N1
vaccination campaign in 2010 had targeted 23,000 recipients in specific risk groups. Only
20.2 % of these target groups were vaccinated, as follows:
Health workers and other essential workers: 29.8%,
Chronic diseases: 14.6%,
Pregnant women: 6.4%,
Healthy population 5 -19 years: 9.6%.
The low intake may have been the result of a mix of factors related to readiness of the
health institutions and the acceptance of the target population, as well as negative
campaigning against the vaccination.
In planning towards the COVID-19 vaccination campaign, which is also receiving negative
publicity, it is therefore important to focus, with regard to the current pandemic, on (mass)
communication to all categories of targeted recipients, including health workers, the elderly,
community leaders, community workers, social workers, religion leaders, the options
available to fight the situation, and advocacy towards vaccination.
The communication has started as early as possible, with a targeted risk-based approach.
Towards this end, the Ministry of Health has in production some public service
announcements that appear on social media, social networks, radio and television
channels. The messages are being communicated in the two main languages, Sranan
Tongo and Dutch. Towards the implementation of the campaign, the messages will be
expanded to include the ethnic languages widely spoken in the several ethnic groups in the
country.
102. Regulatory preparedness
Most regulatory functions of a National Regulatory System or Authority (NRA) recommended
by the WHO are limited or non-existent in Suriname, i.e., market surveillance (MS),
pharmacovigilance (PV), Quality Control (QC) and Information (Figure 1). The functioning of
the Registration and Pharmaceutical Inspection (PI) is limited due to lack of capacity and
resources.
Figure 1
In January 2021, a new Medicine Registration Committee (RC) was installed, based on a
Resolution of the President of Suriname. The new committee is in the process of reviewing
the current arrangements for registration of health products. The MOH has plans to
strengthen the existing PI and to include a Sub-Directorate for Pharmacy which is to carry
out most other NRA functions.
In Suriname, vaccines are exclusively being procured by the National Immunization
Programme (NIP) of the Ministry of Health (MOH) through PAHO’s Revolving Fund for
Access to Vaccines (PAHO-RF), almost since its launch in 1977. The parastatal Medicine
Supply Company Suriname (Bedrijf Geneesmiddelen Voorziening Suriname, BGVS) is
charged with immediate clearance on arrival and transport of the vaccines to the storage
facilities of the NIP. This system has functioned well over the years and challenges are
limited to issues with storage capacity, late payments, or errors in forecasting and planning.
Formally, medicines, including vaccines, have to be registered before they are allowed to be
imported and used in te country (Medicine Registration Law 1973). For the import of
medicine, the Pharmaceutical Inspection (PI) issues a Certificate of Registration to an
authorized importer as a ‘no objection for importation’ to the licensing body, the Ministry of
Economic Affairs, Entrepreneurship and Technological Innovation, Department of Import,
Export and Foreign Exchange Control. The PI further physically checks import samples to
ensure that imported medicines are the same as what is stated in the import permits.
11However, vaccines supplied through the PAHO-RF have never been registered. For each
procurement, waivers (exemption of registration) are granted by the Pharmaceutical
Inspection acting for the Director of the MOH, relying on PAHO-RF’s system for quality
assurance for vaccines including pre-qualification by WHO. This procedure may be used as
long as vaccines have received approval from WHO and are obtained through the PAHO-
RF, which is the expectation for vaccines to be obtained through the COVAX Facility.
Alternatively, when other mechanisms are being considered for procurement of COVID-19
vaccines, the country will rely on technical guidance for assessments of these products by
qualified organizations, like WHO, PAHO and the Caribbean Registration System (CRS)
which rely on the WHO Prequalification Programme’s product approval or approval by
Stringent Regulatory Authorities (SRA) acknowledged by the WHO.
Pharmacovigilance and Information
1. The PV and Information functions will be executed as much as possible based on the
recommendations of global, regional and subregional bodies (WHO, PAHO and CRS);
and,
2. should be done together with the entities undertaking ESAVI & AEFI management.
3. Local pharmacists with expertise on PV and Information functions will be recruited.
In summary:
● COVID-19 vaccines may be imported using the current regulatory arrangements
similar to vaccines supplied through PAHO-RF
○ if obtained through the COVAX Facility.
○ if assessments by qualified organizations are available
○ if, in the long-term, registration of vaccines by the RC is realized.
● In-country regulatory arrangements for MS, PV and QC are to be organized based on
the existing international technical guidelines, making use of locally available
expertise.
The Ministry of Health has received approval of the Ministry of Finance, for tax exemptions
regarding this shipment and future shipments of COVID-19 vaccines for this campaign.
No such challenges should be expected in the distribution to and storage of the vaccines at
local storage points prior to vaccination, since these storage and vaccination sites already
are equipped with the proper means to secure the cold chain process.
The central storage facility at the Wanica Ziekenhuis is one of the facilities in the country
that has UCC storage capacities, and therefore will be in charge of the storage and
distribution of the vaccines. They have already taken proper actions towards safe handling
during this process. A distribution plan is in the making, and will be implemented as soon as
the exact dates of the vaccination campaign have been decided. The transportation of the
vaccines to the districts and the hinterland will need specific attention with regard to keeping
of the cold chain.
The existing national regulatory processes and procedures for the import of vaccines for the
national vaccination program will be in force, in order to expedite vaccine availability in the
country. The formal procedures for the import of the COVID-19 vaccines are to be finalized
by the Ministry of Health.
123. Planning and coordination of the vaccine introduction
Following is the organizational chart in place for the coordination mechanism at national and
local level.
COVID-19 Organizational structure and partners involved
National National COVID-19
Central Coordination:
Director of Health and Technical Advice
Registration Direcor BOG Commission
Commission Vaccination Policy
COVID-19
Working Group
Working group Working Group
Cold Chain/
Prioritairy Groups Logistcs
Supply Chain
Proces
Management Management Monitoring
Planning & Monitoring
cold chain, Training and publc and
budget vaccinne
supply chain supervision communicati Evaluation
management safety
logistiek on
Coordination
Regionaal Coordination Coordination Coordination
East Par'bo, Wanica, West Sipaliwini
Para
• RGD •RGD •RGD •RGD
• MMPHC •MMPHC •MMPHC •MMPHC
•Ziekenhuis •Hospitals •MMC
Marwina
Local
Coordination Implementation
vaccination sites vaccination
The Technical Advisory Commission Immunization Policy COVID-19 consists of the following
authorities:
1. The Deputy Director of Health
2. Infectiologist - clinical expert in infectious diseases.
3. Epidemiologist/researcher of the Public Health discipline of the Faculty of Medical
Sciences
4. Registration committee - Expert regulation medicines and vaccine safety
5. Microbiologist
6. Manager of the National Immunization Program
7. Manager of the Epidemiology Unit of the Bureau of Public Health
13The Commission is a multidisciplinary group of national experts responsible for providing
independent, evidence-based advice to policy makers and program managers on policy
issues related to immunization and vaccines.
The Commission is competent and able to review and contextualize the international and
regional policy guidelines of the WHO Strategic Advisory Group of Experts on Immunization
(SAGE) and the PAHO Regional Technical Advisory Group on Immunization (RITAG), taking
into account the national context, national priorities and disease epidemiology. The
commission will need to regularly review, revise and update its recommendations to national
policy makers as new evidence becomes available.
Responsibilities of the commission, especially in response to the current COVID-19
pandemic, include:
• Review of recommendations from SAGE, the RITAG regarding COVID-19 vaccine
use in the response.
• Periodic review of the national/regional epidemiology and sero-epidemiology of
COVID-19, including laboratory confirmed cases, hospitalization and deaths
associated with COVID-19, and natural immunity data within selected population
groups.
• Advise the Ministry of Health on priority groups and vaccination strategies based on
scientific information and available international and regional guidelines.
• Updating the advice and, in particular, providing vaccine specific recommendations
based on new information/updates on:
o The characteristics of COVID-19 vaccines under development, including efficacy
and effectiveness
o The vaccine safety related to different age and risk groups, effect of the vaccine
on infection and transmission of infection, available vaccine supply and
predictions of vaccine production.
o COVID-19 vaccine specific recommendations from SAGE and RITAG.
• Advising the Ministry of Health on the best communication approaches regarding the
introduction of COVID-19 vaccines, taking into account the characteristics of the
vaccine and the dynamics of public acceptance.
• Reviewing and advising on cases of serious vaccine adverse events (AEFI’s and
Adverse Events of Special Interest (AESI) identified by the passive and active
vaccine safety surveillance conducted and examined by the National Immunization
Program.
• Advising on communication approaches to communities on vaccine safety and
vaccine side effects for which no clear answers are yet available.
• Reviewing and making recommendations on the development of the National
COVID-19 Vaccination Plan.
In preparation for the vaccination campaign, the country has adopted and adapted as
needed, the existing national governance mechanism which are in force for the regular
immunization program in the country. The Technical Advisory Commission Vaccination
Policy COVID-19 is the national coordinating commission, with representation of relevant
institutions, as described above.
The NITAG has been dormant for quite a while, needing renewal of its representation and its
mandate. There is also no active Inter-agency Coordinating Committee. However, past
members of both these committees are involved in the National Coordination Team for the
campaign. Technical guidance has also been sought from international organizations e.g.
PAHO and UNICEF.
The vaccines to be used for the vaccination campaign will be selected upon criteria adopted
by the Ministry of Health and upon approval from the Registration Committee.
144. Resources and funding
Financing COVID-19 vaccination
The procurement of the vaccine and funding of the vaccination program for Covid-19 will be
done within the framework of a national strategy using Government financing and
partnerships with the private sector. A national fund is being established, involving
fundraising with the joint effort of the Government, the business community and other
stakeholders. This decision regarding the fund resulted from a meeting between the
President, the Minister of Health, and the Minister of Foreign Affairs, International Business
and International Cooperation. Consultations were held with various stakeholders, investors,
insurance companies, gold mining companies and the business community. They will
collaborate in local fundraising, which is accepted by the government.
The fundraising will take place through a national fundraising campaign and the fund will be
jointly managed by the business community and the government, resulting in transparency.
Other resources have been made available through the regular budget of the Ministry of
Health, the Ministry of Finance, and other related Ministries, related to this matter.
Budgeting and funding COVID-19 vaccination campaign preparations and implementation
Table 3 summarizes the category of activities and the costs estimated for the implementation
of the Plan. The budget is estimated on best practices and experiences. The detailed budget
for phase 1 is provided in annex 1.
The budgets for the other groups in remaining 3 phases follow the same template, however,
these budgets were adapted to the specific circumstances for these remaining groups, and
taking into account that certain items were already covered in the first phase. It is noted that
this budget will be adapted accordingly, based on the cost of the vaccine to be used in the
first phase and the subsequent phases.
Table 3: Summary of campaign budget (USD)
Summary all 4 phases Phase 1 Phase 2 Phase 3 Phase 4 Total
Political priority and legal framework 20,000 10,000 10,000 10,000 50,000
Planning and coordination 17,000 17,000 17,000 17,000 68,000
Biologicals and supplies 326,315 2,516,216 1,174,832 7,416,550 11,433,913
Cold chain 72,600 - - - 72,600
Training 27,000 - - - 27,000
Social mobilization 89,300 67,950 87,950 87,950 333,150
Operating costs 315,226 616,726 315,226 770,352 2,017,530
Supervision and monitoring 25,000 40,000 25,000 55,000 145,000
Epidemiological surveillance and laboratory 56,250 38,790 28,100 72,000 195,140
Information systems 98,850 29,100 29,350 29,350 186,650
Research 3,000 3,000 3,000 3,000 12,000
Evaluation 12,000 12,000 12,000 12,000 48,000
Total 1,062,541 3,350,782 1,702,458 8,473,202 14,588,983
Miscellaneous 10% 106,254 335,078 170,246 847,320 1,458,898
Grand Total 1,168,795 3,685,860 1,872,704 9,320,522 16,047,881
15Table 3a: Summary by phase
Group Description Phases Target Budget
Group 1 Healthcare workers, first line Phase 1 11,691 1,168,795
Group 2 Healthcare workers, second line
Group 3 Military, police, penitentiary officers,
Government Officials
Group 4 Populations in elderly homes, including dialysis
patents
Group 5 Population sixty years and over, national level Phase 2 90,170 3,685,860
Group 6 Population, based on medical grounds/risk Phase 3 42,497 1,872,704
factors (40 – 59 years)
Group 7 Population, based on medical grounds/risk
factors, (18 – 39 years)
Group 8 Other risk groups
Group 9 Healthy population (18 -59 years) (estimated) Phase 4 265,779 9,320,522
Grand Total 409,740 16,047,881
Partners and Financing
• Ministry of Health through its institutions: BOG, MM, RGD and others.
• Ministry of Regional Development: Meetings with District Commissioners, District
Council, Resort Council, local transportation (hinterland).
• Ministry of Education: Schools, additional vaccination sites, …
• Medical Faculty of the ADEK University of Suriname (MWI): Support staff,
vaccinators.
• Public and Private Hospitals, Nursing schools: Support staff, vaccinators.
• Ministry of Public Works: Logistics.
• Ministry of Defense: Logistics, Security.
• Ministry of Justice and Police: Security.
• Private sector, Service Clubs: Sponsoring of human and financial resources,
logistics, public announcements, food, refreshments, advertisements, document
duplication, data input, computer hardware, internet facilities.
• International Agencies.
165. Target populations and vaccination strategies
The following groups have been identified by the National Coordination Team, to be
included in the vaccination campaign. Vaccination will be free of charge and will be
accepted on a voluntary basis (out of free will). Table 4 summarizes the target groups in
order of priority.
Table 4. Summary total persons by priority group, to be vaccinated in one round
Priority Population Persons
Group 1 Healthcare workers, first line 1,497
Group 2 Healthcare workers, second line 3,794
Group 3 Military, police, penitentiary officers, Government Officials 3,500
Group 4 Populations in elderly homes, including dialysis patents 2, 900
Group 5 Population sixty years and over, national level 90,170
Group 6 Population, based on medical grounds/risk factor (Diabetes Mellitus, 30,000
High Blood Pressure, Sickle Cell Anemia, Cardio vascular Diseases,
COPD, Oncologic Diseases, Indigenous, ….) (40 – 59 years)
Group 7 Population, based on medical grounds/risk factor (Diabetes Mellitus, 11,000
High Blood Pressure, Sickle Cell Anemia, Cardio vascular Diseases,
COPD, Oncologic Diseases, Indigenous, ….) (18 – 39 years)
Group 8 Other risk groups 1,100
Group 9 Healthy population (18 -59 years.) (estimated) 265,779
Total 409,740
The following tables details on where the priority groups will be vaccinated, the estimated
teams to be deployed and the basic inventory needed by a team.
For the calculation of number of teams, the following assumptions/criteria are used:
- It will take 5 minutes to register, including questioning on contraindications, of one
person in an outside facility.
- In one hour, 1 vaccinator can vaccinate 15 persons, personal break time included.
- One vaccination session will start at 8.00 am and end at 4:00 pm, in total 8 hours,
minus 1 hour break time, a day. Facilities will be open until the last person has been
vaccinated. So, overtime and consumption for the team have been included in the
budget.
- Accordingly, one team can vaccinate 3 x 15 x 7 = 315 persons in a one-day session.
- Some clinics with small populations can be joined together, taking into account the
geographic possibilities.
- Since there is no system of postcodes or other criteria to daily organize the flow to
the facility, it might happen that all those needing the vaccination, will show up on
one day, if not well informed or organized properly. In order to address this issue, it
would be practical and cost saving to do a district in 1 day, by the available teams in
that district area, assisted by additional teams from other districts, or the RGD, or
volunteers, provided that there is sufficient transportation organized.
- For the city and other communities, it can be decided to do a vaccination day with so
many teams simultaneously, as practically organizable. Given this reasoning, it is
advisable thus that the vaccination is organized by district.
- It must be noted that smooth flow of vaccine recipients through the phases of
registration, vaccination and observation post-vaccination, will need adaptation to the
situation during the activities. A practical issue would be that, if for example 15
17persons receive the vaccination in one hour, these 15 persons will have to spend the
required 15 – 30 minutes in the observation area. A continuous flow of the recipients
in the observation area will pose practical issues with regard to accommodation of all,
at once and to ensure adherence to the COVID-19 public health measures.
- The same process will be repeated for the second dose to be given 3 - 4weeks later,
depending on the vaccine being used.
The following table gives a breakdown of what would be the basic inventory for 1 vaccination
team. More than 1 team may be deployed to one site, in order to facility smooth operation.
Table 5: Breakdown of the basic inventory needed for a team
Item Unit price Needed Total
Vaccine carrier 40 1 40
Thermos box (where needed) 0
Ice packs, at least 4 per carrier 10 1 10
Laser thermometer 75 1 75
Cotton rolls 5 1 5
Disinfectants 2 10 20
Hand sanitizers 2 10 20
Paper towels, toilet paper 5 2 10
Band aids (box of 100) 1 5 5
Vaccination cards, at least 500 per session 0.1 500 50
Stamp and stamp pad 25 1 25
PPE Equipment (masks only) 1 100 100
Disposable gloves 2 15 30
Safety boxes 10 5 50
Waste bags 5 10 50
Manuals, intake forms, ESAVI surveillance,
10 1 10
writing materials,
Total 500
The following tables give an overview of vaccination sites where the priority groups will be
vaccinated. More than 1 team may be deployed to one site, in order to facility smooth
operation.
Table 5a. Group 1: Health Care workers, first line
Basic
Hospitals/Health Centers
To Vaccinate Teams Days Inventory
Militair Hospitaal
Academisch Ziekenhuis Paramaribo 422 2 1 1,000
Diaconessenhuis 200 1 1 500
Lands Hospitaal 115 1 1 500
St. Vincentius Ziekenhuis (RKZ) 188 1 1 500
Wanica Ziekenhuis 138 1 1 500
Mungra Medisch Centrum Nickerie 44 1 1 500
RGD 65 1 1 500
Medische Zending 100 1 1 500
PCS 25 1 1 500
Others (MOH team, Swab teams, and others) 200 1 1 500
Total 1,497 11 10 5,500
18Table 5b. Group 2: Health care workers, second line.
Hospitals/Health Centers To Vaccinate Teams Days Cost
Militair Hospitaal 1,200 4 2,000
Academisch Ziekenhuis Paramaribo 630 2 1,000
Diaconessenhuis 340 1 500
Lands Hospitaal 276 1 500
St. Vincentius Ziekenhuis (RKZ) 375 1 500
Wanica Ziekenhuis 120 1 500
Mungra Medisch Centrum Nickerie 200 1 500
RGD 590 1 500
Medische Zending 63 1 500
PCS
Total 3,794 13 1 6,500
Table 5c. Group 3: Military, police, penitentiary officers, Government Officials
Hospitals/Health Centers To Vaccinate Teams Days Cost
Militair Hospitaal 2,000 5 1 2,500
Academisch Ziekenhuis Paramaribo 1
Diaconessenhuis
Lands Hospitaal
St. Vincentius Ziekenhuis (RKZ)
Wanica Ziekenhuis 1,000 3 1 1,500
Mungra Medisch Centrum Nickerie 500 2 1 1,000
Other vaccination sites, public and private
Total 3,500 10 4 5,000
Table 5d. Group 4: Populations in elderly homes, including dialysis patents
Target: 2,050 and 850 persons respectively.
Hospitals/Health Centers To Vaccinate Teams Days Cost
Militair Hospitaal for the Dialysis patients 850 4 1 2,000
Academisch Ziekenhuis Paramaribo
Diaconessenhuis
Lands Hospitaal
St. Vincentius Ziekenhuis (RKZ)
Wanica Ziekenhuis
Mungra Medisch Centrum Nickerie
Other vaccination sites, public and private 2,050 10 1 5,000
Total 2,900 14 1 7,000
19Table 5e. Target group 5: Population 60 years and older, national level
District Resorts Communities Target
Brokopondo 6 7 1,171
Commewijne 6 37 5,163
Coronie 3 4 574
Marowijne 6 29 2,843
Nickerie 5 22 6,060
Para 5 45 3,458
Paramaribo 12 114 45,148
Saramacca 6 36 2,784
Sipaliwini 6 41 4,811
Wanica 7 135 18,158
Total 62 470 90,170
Vaccine and related costs for the population 60 years and older
This list is based on two sources:
1. The Central Bureau for Public Affairs (Centraal Bureau voor Burgerzaken) (CBB) with
an overview of all persons over 60 years, as registered in the respective districts,
resorts (district areas), and communities.
2. The Medical Mission Primary Health Care, with all their clients registered in the
respective districts and resorts.
For further elaboration of this risk group, both sources have been used. For the population of
the Medical Mission, their sources have been used, while for the remaining RGD resorts, the
CBB data have been used. The total number of persons over 60 years as provided by the
CBB, have not been altered for the general analysis.
Teams and sessions for the implementation of the campaign, of the population over
60years old
According to CBB data, the total population in this age group is 90,170 living in 10 districts,
in 62 resorts, and 470 communities. Most of these communities have health facilities
operated by the Regional Health Services (RGD) in the coastal area, and the Medical
Mission in the hinterland. (The hospitals and private facilities are excluded here).
The facilities in the coastal area are in general geographically easily accessible, while only a
part of those in the hinterland can be reached by road. Most of the communities/villages in
the hinterland can only be reached over water or by air.
In planning the logistics of the campaign, transportation over water and air constitute a
significant part of the costs. Transportation over road from village to village was taken into
account, when planning the number of teams needed per district.
The basis of the planning for human resources, is that a fixed/mobile/outreach team will
consist of:
3 vaccinators, 1 administrative support, 1 driver and 1 “gatekeeper”.
The administrative support and the “gatekeeper” can be recruited from the local facilities, or
other support services available there.
The teams operating in Paramaribo and parts of some districts can move easily from facility
to facility, by road transportation.
20Table 5e-1: Number of vaccination sessions needed per district, resort and population
in the service area of the Medical Mission.
Note: The information in this table for the MM is derived, based on the information from the
table by CBB. The CBB table is left in its original format, minus the sessions in the MM area,
to indicate the (total) population size in all districts.
RESSORT CLINIC SESSIONS TOTAL
BROKOPONDO BROWNSWEG 1
2
NW. KOFFIEKAMP 1
KLAASKREEK 1
2
Nw. LOMBE (boat) 1
Brownsweg
MARCHALLKREEK 1 1
PHEDRA 1 1
POWAKKA 1
2
REDI DOTI 1
BROKOPONDO 1 1
ASIGRON 1 1
Brokopondo
BALINGSOELA 1 1
LEBIDOTI 1 1
Bovenlandse Bovenlandse SIPALIWINI (air) 1
Indianen en Indianen 2
ALALAPAROE (air) 1
West
PALUMEU (air) 1
Suriname 2
PELELE TEPOE (air) 1
PULEOWIME (air) 1
2
KAWEMHAKAN (air) 1
COEROENI (air) 1
KWAMALASAMUTU (air) 1 3
AMOTOPO (Air) 1
1 1
WEST SURINAME WITAGRON
Boven DEBIKE DEBIKE 1
Suriname HEKOENOENOE 1 3
KAMBALOA 1
PIKIEN SLEE 1 1
DJOEMOE DJOEMOE (air) 1
2
KAJANA (air) 1
SEMOISIE (boat) 1 1
POKIGRON 1
2
LADOANI DOEWATRA 1
GOEJABA (boat) 1
2
LADOANI (boat) 1
SOEKOENALE (boat) 1 1
JAW-JAW 1 1
BIGI POIKA 1 1
21PIKIN SARON 1 1
MIDDEN MIDDEN KWAKOEGRON 1 1
SURINAME SURINAME POESOEGROENOE (by air) 1 1
NJ JACOB KONDRE (by air) 1 1
DRIETABIKI (air) 1 1
DRIETABBETJE GODORO (air) 1 1
KARMEL (air) 1 1
AGAIGONI (boat) 1 1
APOEMA (boat) 1 1
OOST COTTICA (boat) 1 1
SURINAME GAKABA (boat) 1 1
STOELMANSEILAND GONINI (boat) 1 1
LANGATABIKI (boat) 1 1
LAWATABIKI (boat) 1 1
NASON (boat) 1 1
STOELMANSEILAND (air) 1 1
Total sessions 52 52
Table 5e-2. Number of vaccination sessions needed per district, resort and
population, using CBB data
DISTRIKT RESSORT POPULATION Sessions needed, based Total
on target population size sessions
and geographic needed
accessibility
Brokopondo Brownsweg 340
Centrum 282 Included in
Klaaskreek 227 the previous
Kwakoegron & Klaaskreek table of the
125 MM
& Marshallkreek
Sarakreek 197
Commewijne Alkmaar 915 2
Bakie & Margaretha 189 1
Meerzorg 1835 5 12
Nieuw Amsterdam 1167 2
Tamanredjo 1057 2
Coronie Johanna Maria & Totness &
574 2 2
Welgelegen
Marowijne Albina 1038 2
Galibi 143 1
Moengo 1246 3 8
Moengo Tapoe 137 1
Patamacca & Wanhati 279 1
Nickerie Groot Henar 419 1
Nieuw Nickerie 2391 6 13
Oostelijke Polders 1006 2
22Wageningen 592 1
Westelijke Polders 1652 3
Para Bigi Poika 75
Carolina 77 Included in
the previous
Noord 1118
table of the
Oost 1195 MM
Zuid 993
Paramaribo Beekhuizen 2911 6
Blauwgrond 7113 13
Centrum 5342 13
Flora 3713 9
Latour 3807 9
Livorno 1299 3
104
Munder 3045 9
Pontbuiten 2573 6
Rainville 5340 13
Tammenga 2750 6
Weg Naar Zee 3043 7
Welgelegen 4212 10
Saramacca Calcutta 242 1
Groningen 520 2
Jarikaba 822 2
8
Kampong Baroe 407 1
Tijgerkreek 534 1
Wayamboweg 259 1
Sipaliwini Boven Coppename 78
Boven Saramacca 109 Included in
Boven Suriname 2279 the previous
Coeroenie 185 table of the
Kabalebo 297 MM
Tapanahony 1863
Wanica De Nieuwe Grond 4080 10
Domburg 1234 4
Houttuin 2300 5
Koewarasan 3046 7 47
Kwatta 2349 6
Lelydorp 3456 10
Saramacca Polder 1693 5
TOTAL 90170 194 194
Thus, the total number of sessions for the 60+ group on national level is (52 + 194) x 2 = 492
sessions for both vaccination rounds.
23Transportation costs will be added depending on the geographical area of the site.
Table 5e-3: Roundtrip transportation cost Medical Mission
TRANSPORTATION COSTS MEDICAL MISSION – 1 round (USD)
Poesoegroenoe and Nw Jacob kondre (air) 1,353
Kwakoegron/ Witagron / Pikin Saron (road) 440
Bigi Poika and Pikin Saron (road) 220
Sipaliwini/ Alalaparoe (air) 2,428
Pelele Tepoe/ Palumeu (air) 2,150
Puleowime/ Kawemhakan (air) 1,620
Coeroeni/ Amotopo/ Kwamalasamutu (air) 2,324
Kajana/ Djoemoe (air) 1,526
Djoemoe/ Semoisie (boat) 100
Debike/Hekoenoenoe/ Kambaloa/ Pikin Slee (boat) 250
Ladoani/ Goejaba (boat) 178
Pokigron/ Duatra (road) 430
Brownsweg/ nw. Koffiekamp (road) 240
Klaaskreek/ nw. Lombe (road/boat) 176
Marchallkreek/ Phedra (road) 155
Powakka/ Redi Doti (road) 154
Brokopondo/ Balingsoela (road) 200
Brokopondo/ Asigron (road) 30
Brokopondo/ Lebi Doti (road/boat) 300
Stoelmanseiland/ Gonini/ Agaigoni (air/boat) 1,783
Drietabbetje (flight)/Stoelmanseiland (drop vaccines)/
Cottica /Lawatabiki 2,156
TOTAL USD 18,213
24Based on these criteria, the following overview is presented in table 5e-4.
Table 5e-4: Costs for reaching out to vaccination sites (USD) for the 60+ target group
Overtime/
District Population Sessions Inventory Transport
Consumption
Brokopondo 12 6,000 1,800
1,171
Bovenlandse Indianen 9 4,500 1,350
West Suriname 1 500 150
18,213
Boven Suriname 12 6,000 1,800
Midden Suriname 6 3,000 900
Oost Suriname 12 6,000 1,800
Commewijne 5,163 12 6,000 300 1,800
Coronie 574 2 1,000 500 300
Marowijne 2,843 8 4,000 500 1,200
Nickerie 6,060 13 6,500 700 1,950
Included in specification
Para 3,458
by MM
Paramaribo 45,148 104 52,000 200 15,600
Saramacca 2,784 8 4,000 200 1,200
Included in specification
Sipaliwini 4,811
by MM
Wanica 18,158 47 23,500 500 7,050
Total 90,170 123,000 29,583 36,900
Vaccine and related costs for the 60+ population
The components in the following table have been included in the detailed budget and this will
be programmed separately. Fine tuning will be needed, once the prices for the ancillary
items have been determined.
Table 5e-5: Vaccine doses needed (including 10% wastage rate) per district for the
population of 60 years and older
Population Vaccine Syringes/ If reconstitution needed
District doses needles Diluent vials Syringes 5ml Needles
Brokopondo 1,171 incl.20%
2,576 2,576 10515
ml reconstitution
515 reconstitution
515
Commewijne 5,163 waste
11,359 11,359 2,272 2,272 2,272
Coronie 574 1,263 1,263 253 253 253
Marowijne 2,843 6,255 6,255 1,251 1,251 1,251
Nickerie 6,060 13,332 13,332 2,666 2,666 2,666
Para 3,458 7,608 7,608 1,522 1,522 1,522
Paramaribo 45,148 99,326 99,326 19,865 19,865 19,865
Saramacca 2,784 6,125 6,125 1,225 1,225 1,225
Sipaliwini 4,811 10,584 10,584 2,117 2,117 2,117
Wanica 18,158 39,948 39,948 7,990 7,990 7,990
Total 90,170 198,374 198,374 39,675 39,675 39,675
25Table 5e-6: Vaccine and syringes/needles cost for a vaccine that costs 10.50 USD per
dose (example)
District Population Vaccine Syringes/ Vaccines Syringes/ Total USD
Brokopondo 1,171 doses 2,576 needles
2,576 32,460 Needles
185 32,646
Commewijne 5,163 incl.20%
11,359 11,359 143,118 818 143,936
Coronie 574 waste 1,263 1,263 15,911 91 16,002
Marowijne 2,843 6,255 6,255 78,808 450 79,258
Nickerie 6,060 13,332 13,332 167,983 960 168,943
Para 3,458 7,608 7,608 95,856 548 96,404
Paramaribo 45,148 99,326 99,326 1,251,503 7,151 1,258,654
Saramacca 2,784 6,125 6,125 77,172 441 77,613
Sipaliwini 4,811 10,584 10,584 133,361 762 134,123
Wanica 18,158 39,948 39,948 503,340 2,876 506,216
Total 90,170 198,374 198,374 2,499,512 14,283 2,513,795
Table 5f. Group 6: Population, based on medical grounds/risk factor (Diabetes
Mellitus, High Blood Pressure, Sickle Cell Anemia, Cardio vascular Diseases, COPD,
Oncologic Diseases, Indigenous) (40 – 59 years)
Target: 30,000 persons
The details with regard to where these persons are located, where they will be vaccinated,
and what will be the cost for this group, will be confirmed when full information about this
group becomes be available.
Hospitals/Health Centers To Vaccinate Teams Days Cost
A designated location or tent on the grounds of the
hospital or near the hospital, where the patient can
go after visiting the specialist 10,000 10 10 5000
Outreach (mobile) clinics for surrounding
villages/polders. 5,000 5 10 2500
Designated outpatient clinics (separate location in
the clinic, or a tent on site). 5,000 5 10 2500
Temporary clinics or mobile outreach teams 5,000 5 10 2500
Other vaccination sites, public and private 5,000 5 10 2500
Total 30,000 30 15,000
Table 5g. Group 7: Population, based on medical grounds/risk factor (Diabetes
Mellitus, High Blood Pressure, Sickle Cell Anemia, Cardio vascular Diseases, COPD,
Oncologic Diseases, Indigenous) (18 – 39 years)
Target: 11,000 persons
The details with regard to where these persons are located, where they will be vaccinated,
and what will be the cost for this group, will be determined when full information about this
group will be available.
26You can also read

















































