Microbiome and Dysbiosis: where are we?
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
5/19/2021
Microbiome and Dysbiosis:
where are we?
Jan S. Suchodolski, DrMedVet, PhD, DACVM, AGAF
Professor & Associate Director Research
Head of Microbiome Sciences, Gastrointestinal Laboratory
Department of Small Animal Clinical Sciences
Texas A&M University, College Station, TX, USA
PREIDIS AND VERSALOVIC, GASTROENTEROLOGY 2009;136:2015–2031
1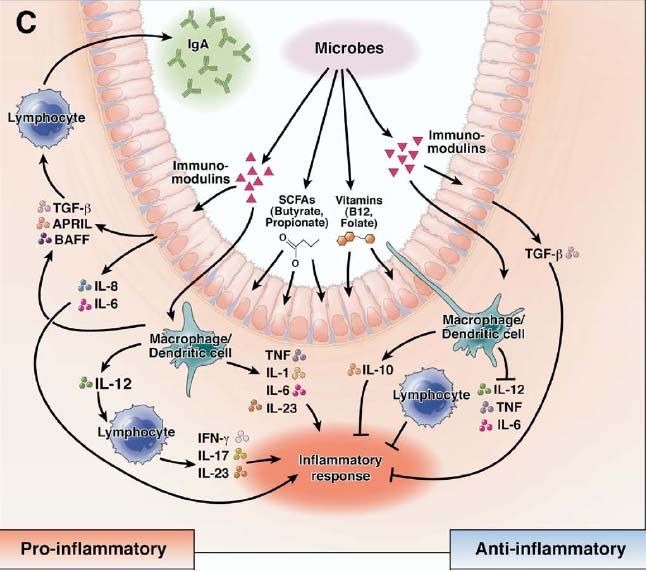
5/19/2021
TOBIE
5 year old Dachshund
chronic diarrhea > 2 year duration
mixed origin
soft/watery, occasionally tenesmus
diarrhea sometimes 2‐3x per day
fed commercial kibble diet
HISTORY
history of parvovirosis as puppy
several unsuccessful treatment attempts over last year
short‐term improvement on home‐made diet (duck)
deworming (fenbendazole)
since 3 months intermittently on metronidazole
15 mg/kg PO q12 hours
partial improvement when on, relapses when stopped
2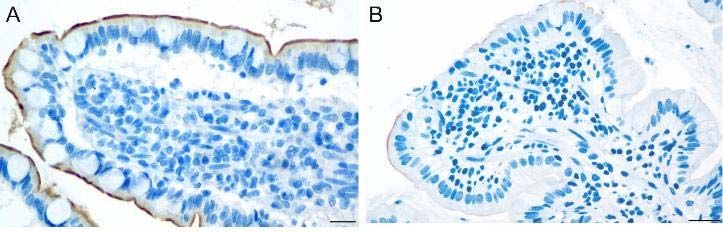
5/19/2021
PHYSICAL/LABORATORY RESULTS
physical exam unremarkable
weight 4.7 kg, BCS 3/9
CBC, serum chemistry profile
no abnormalities
GI PANEL
Test Unit Reference interval
cPLI 133 µg/L < 200 µg/dl
cTLI 20 µg/L 5.7 – 45.2
Cobalamin 301 ng/L 251 ‐ 908
Folate 21.4 ng/L 7.7 – 24.4
Cobalamin low normal – may indicate malabsorption
associated with chronic enteropathy
3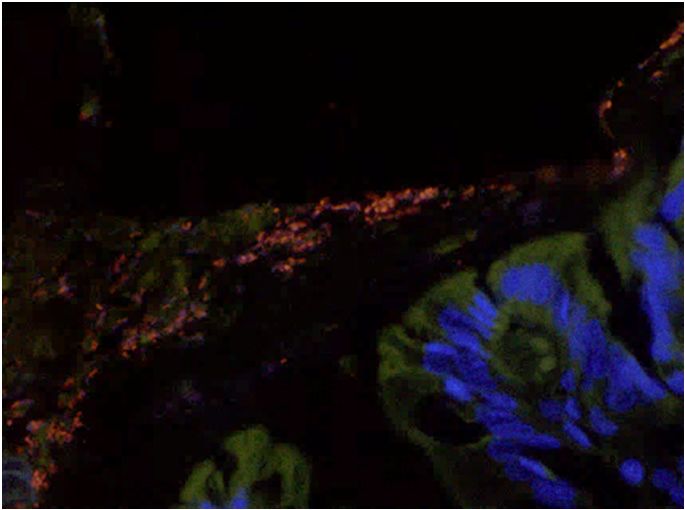
5/19/2021
FECAL EXAMINATION
Fecal flotation for parasites
Previous PCR enteropathogen panel – positive for Clostridium difficile
Fecal Dysbiosis Index
Test Result Reference interval
Dysbiosis Index 4.2 = dysbiosis
5/19/2021
WHAT SHOULD WE TREAT?
a) continue metronidazole (to eliminate C. difficile)
b) change to another antibiotic (eg, tylosin)
c) dietary change to novel or hydrolyzed protein diet
d) probiotics to balance microbiota dysbiosis
e) fecal microbiota transplant (FMT) to improve dysbiosis
Microbiota in GI health and disease
Intestinal microbiota Intestinal microbiota
in health in CE
5
5/19/2021
Microbiota in GI health and disease
Intestinal microbiota Intestinal microbiota
in health in chronic enteropathy
Dog with antibiotic responsive
Healthy dog enteropathy
6
5/19/2021
abnormal metabolite ratios lead to abnormal bile acid conversion
activation of virulence factors leads to overgrowth with
Salmonella, E. coli C. difficile, C. perfringens, E. coli
Dysbiosis
inflammation, maldigestion, malabsorption
ASSESSMENT AND CLINICAL INTERPRETATION
OF THE MICROBIOME
difficult – there is no one single test that allows proper
assessment of microbiota and function
7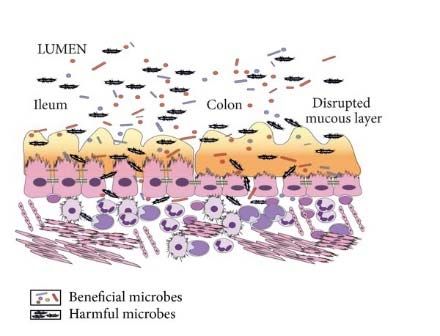
5/19/2021
Conclusion: Culture has no use
in assessment of dysbiosis
only small percentage of bacteria can be cultivated using routine
methods
only useful for detection of specific pathogens
Salmonella, Campylobacter jejuni
antibiotic susceptibility testing
Healthy dogs have a highly individual microbiota
100% Enterobacteriaceae
Succinivibrionaceae
Helicobacteraceae
Campylobacteraceae
80% Alcaligenaceae
Coriobacteriaceae
Bifidobacteriaceae
Turicibacteraceae
Streptococcaceae
60% Enterococcaceae
Bacillaceae
Fusobacteriaceae
Erysipelotrichaceae
Ruminococcaceae
40% Veillonellaceae
Peptostreptococcaceae
Peptococcaceae
Clostridiales;f__
Clostridiales;Other
20%
Clostridiaceae
Lachnospiraceae
[Paraprevotellaceae]
Prevotellaceae
0% Porphyromonadaceae
Bacteroidaceae
8
5/19/2021
Change in dysbiosis Properties
beneficial
Faecalibacterium ↓ anti‐inflammatory
Turicibacter ↓ short‐chain fatty acids
Blautia ↓ short‐chain fatty acids
Fusobacterium ↓ short‐chain fatty acids
Clostridium hiranonis ↓ bile acid converter
harmful
Streptococcus ↑ overgrowth in maldigestion
E. coli ↑ pro‐inflammatory
Dysbiosis Index Sensitivity CI (95%) Specificity CI (95%)
2 0.63 0.53‐0.72 1 0.96‐1.00
0 0.74 0.65‐0.82 0.95 0.89‐0.98
‐1 0.82 0.73‐0.88 0.91 0.84‐0.96
‐2 0.86 0.78‐0.92 0.83 0.74‐0.90
9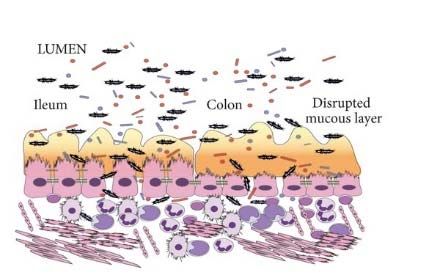
5/19/2021
The higher DI the less diverse the microbiome
‐low microbial diversity may be negative predictor for treatment outcome
r= ‐0.707
p5/19/2021
open access
Different types of dysbiosis
increase in total bacterial load in small intestine
‐ increased microbial metabolites causing diarrhea
‐ increased inflammatory response
increased mucosa‐adherent bacteria
‐ increased inflammatory response
115/19/2021
Different types of dysbiosis
abnormal substrate in lumen (eg, undigested nutrients, drugs)
‐ increase in microbial derived metabolites causing diarrhea
loss of beneficial bacteria (ie, C. hiranonis)
‐ no secondary bile acids
‐ overgrowth of pathogens
‐ lack of anti‐inflammatory properties of secondary bile acids
Different treatments address different mechanisms
dietary
change
probiotics prebiotics
microbiome
dysbiosis
FMT antibiotics
125/19/2021
Type of
Likely mechanism Potential disadvantage
treatment
• improved digestibility leads to
less dietary substrate available
for bacterial growth
Dietary change • none when no food sensitivity
• hypoallergenic – reduces
inflammation and secondary
dysbiosis
Type of
Likely mechanism Potential disadvantage
treatment
• improved digestibility leads to
Dietary change less dietary substrate available • none when no food sensitivity
for bacterial growth
• minor effect on total microbiota
• can improve barrier function
Probiotics • unclear which patient would
• immunomodulatory
benefit from which strain
135/19/2021
Type of
Likely mechanism Potential disadvantage
treatment
• improved digestibility leads to
Dietary change less dietary substrate available • none when no food sensitivity
for bacterial growth
• minor effect on total microbiota
• can improve barrier function
Probiotics • unclear which patient would
• immunomodulatory
benefit from which strain
• increase in beneficial bacteria • can initially cause flatulence
Prebiotics/fibers
• bind bacterial metabolites • individual patient response
Type of
Likely mechanism Potential disadvantage
treatment
• negative changes in microbiota
• reduction in total and mucosa‐
• when stopped re‐growth of
Antibiotics adherent bacteria
bacteria
• less toxic bacterial metabolites
• antimicrobial resistance
145/19/2021
Type of
Likely mechanism Potential disadvantage
treatment
• negative changes in microbiota
• reduction in total and mucosa‐
• when stopped re‐growth of
Antibiotics adherent bacteria
bacteria
• less toxic bacterial metabolites
• antimicrobial resistance
• minor effect on mucosa‐
Fecal microbiota • alters luminal microbiota and adherent bacteria
transplantation metabolites • recurrence of dysbiosis when
(FMT) • reduction of enteropathogens intestinal inflammation still
present
SMALL INTESTINAL DYSBIOSIS
clinical syndrome caused by an abnormal accumulation of
bacteria in the small intestine
increased number of bacteria
abnormal bacterial species
other terminology
small intestinal bacterial overgrowth (SIBO)
antibiotic responsive diarrhea (ARD)
155/19/2021
CAUSES OF DYSBIOSIS
Exocrine
Pancreatic
Insufficiency Defective
Gastric Acid
Intestinal Output
inflammation
Unabsorbed
Nutrients Abnormal Motility
Obstruction
Healthy dog Dog with enteropathy
165/19/2021
DIAGNOSIS FOR SMALL INTESTINAL DYSBIOSIS
serum folate can be increased
serum cobalamin can be decreased
empirical response to antibiotics
Not Specific
CHRONIC ENTEROPATHY
umbrella term that encompasses different chronic GI disorders, with etiology
unknown
food‐responsive enteropathy (FRE) is most common,
50‐70% of patients respond to novel or hydrolyzed protein diet
antibiotic‐responsive enteropathy (ARE)
11‐15% ‐ tylosin or metronidazole
steroid‐responsive enteropathy (SRE) Dandrieux J et al, Australian Vet J 2019
Allenspach K et al, Vet Rec 2016
20‐25% require immunosuppression Volkmann M et al, J Vet Intern Med 2017
175/19/2021
FOOD‐RESPONSIVE ENTEROPATHY (FRE)
chronic enteropathies are frequently responsive to diet changes (50‐70% of
patients)
structured work up for patients with chronic GI signs mandatory
diet trials represent important FIRST step
hydrolyzed or novel protein diets
strict owner compliance important – no treats etc
improvement in 10‐14 days
TOBY DIAGNOSED WITH FOOD‐RESPONSIVE ENTEROPATHY
commercial hydrolyzed protein diet
proteins5/19/2021
Cobalamin – is bound to intrinsic factor (from pancreas)
and absorbed in ileum
• Decreased serum cobalamin
• decreased absorption due
to inflammation in ileum
• dysbiosis can cause
decreased serum cobalamin
concentrations
Suchodolski et al., Clinical Techniques Small Animal Practice 2003
Folate – is absorbed in the proximal small intestine
• Decreased folate cobalamin
• decreased absorption due
to due to inflammation in
jejunum
• Increased serum folate
• due to increased bacterial
folate synthesis in jejunum
Suchodolski et al., Clinical Techniques Small Animal Practice 2003
195/19/2021
COBALAMIN (VITAMIN B12)
important for various metabolic pathways
many animals with CE are deficient in B12
studies have shown that low cobalamin is associated with poorer outcome
therefore, cobalamin supplementation is needed
start supplementing when cobalamin is already in low normal range
COBALAMIN (VITAMIN B12)
oral (PO) daily cobalamin supplementation
cyanocobalamin 1 mg/tablet
dogs < 10 kg: ¼ tablet/day
dogs 10‐20 kg: ½ tablet/day
dogs ≥ 20 kg: 1 tablet/day
cats: ¼ tablet/day
parenteral (PE)
cats: 250 µg
dogs 20kg: 1000 µg
cobalamin injection/week during 6 weeks and a final injection 4 weeks
later
205/19/2021
COBALAMIN (VITAMIN B12)
most animals need indefinite treatment (serum concentrations will fall
without supplementation in most patients)
folate/ folic acid: daily oral 200 µg for cats and smaller dogs (5/19/2021
Microbiota in GI health and disease
Intestinal microbiota Intestinal microbiota
in health in chronic enteropathy
30 of 71 owners (42%) of CPV dogs reported chronic
gastrointestinal problems compared to only 8 of 67 owners of
control dogs (12%)
chronic GI signs in 87% dogs of the CPV group began during the
first year of life
19/30 dogs responded to diet change alone (food‐responsive)
225/19/2021
BLUE – 10 MONTH OLD FEMALE GOLDEN RETRIEVER
every 6‐8 weeks episodes of watery diarrhea
received metronidazole at 4 months of age
testing because of repeated episodes of diarrhea
fecal parasites negative
enteropathogen panel ‐ increase in C. perfringens toxin A
fecal dysbiosis index – all bacteria normal
CAUSES ‐ ACUTE UNCOMPLICATED DIARRHEA
very rarely bacterial infections
eg, Campylobacter jejuni
and even then in most cases self‐limiting
Clostridial overgrowth often consequence of underlying microbiota changes
and unlikely causative
netF toxin associated with acute hemorrhagic diarrhea, but often also self‐limiting
Ziese et al, PLOS One 2018
parasites
motility changes (stress) and dietary causes
undigested food can cause bacterial proliferation
235/19/2021
TREATMENT ‐ ACUTE UNCOMPLICATED DIARRHEA
most cases are self limiting within 2‐4 days
discuss with owner expectations and treatment options
risk and benefits of therapy
gastrointestinal diet for 7 days
highly digestible, low to moderate fat, preferably wet
antiemetic if needed – maropitant (1 mg/kg SQ)
probiotic for 14‐21 days
kaolin‐pectin q8 hours for the first 2‐3 days may help improving fecal quality
SUMMARY
commensal microbiota and their metabolites modulate host health
important to keep microbiota healthy
dysbiosis is early marker of underlying GI disease
treatment of dysbiosis depends on underlying disease
diets, probiotics, prebiotics have little side effects
diet should always be first step
antibiotics useful in some patients, but high relapse rates
245/19/2021
CASE REPORT
“Zorro”, 8 year old Rottweiler with CE
was stable on prednisolone for 4 years
6 months ago, developed calcinosis cutis
prednisolone stopped – dog developed watery diarrhea
no success with treatment with cyclosporine, azathioprine,
metronidazole, and fecal microbiota transplant
still watery diarrhea, weight loss of 3 kgs over 3 months
CASE REPORT
dog received cholestyramine (QuestranTM)
2 grams BID – improvement of watery diarrhea
dose increased to 3 grams morning + 2 grams evening
complete resolution of diarrhea with 10 days
dog vomited 3x in a week (side effect of cholestyramine)
dose reduced to 2 grams BID – diarrhea returned
dose again increased to 3 + 2 grams – complete resolution of diarrhea
dog stable for 3 months, gained 3 kg
255/19/2021
BILE ACID DIARRHEA (BAD)
under recognized in humans (limited diagnostic testing)
approx. 30% of patients with IBS
40% of patients with Crohn’s Disease
1% of total population
type 1: bile acid malabsorption, secondary to ileal resection or
inflammation
type 2: idiopathic bile acid malabsorption, primary bile acid
diarrhea
type 3: secondary to various GI diseases including small
intestinal dysbiosis
ASBT bile acid transporter in the ileum ‐ 90% of bile acid reabsorption
ASBT expression is reduced in ileum in dogs with chronic enteropathy
(CE) – may lead to increase in bile acids, leading to diarrhea
healthy chronic enteropathy (CE)
Giaretta P et al, JVIM 2019
265/19/2021
TREATMENT OF BILE ACID MALABSORPTION
cholestyramine (bile acid sequestrants)
2-4 grams/dog q12h
can be increased if no response and no side effects
corticosteroids
induce expression of bile acid transporters in ileum
helps with reabsorption of bile acids
should empirically try cholestyramine in dogs that have partial response to
corticosteroids
or respond well to corticosteroids but not other immunosuppressive drugs
when dogs don’t tolerate steroids
CASE – BOXER DOG
clinical signs of colitis
large bowel diarrhea, 5-8 per day
tenesmus, hematochezia, mucus in stool
therapeutic trial without success
different diets, antibiotics (tylosin, metronidazole)
infectious reason excluded (Salmonella, Campylobacter)
275/19/2021
CASE – BOXER DOG
because dog was losing weight, endoscopy was initiated
colonoscopy revealed inflamed mucosa with ulceration
histology revealed granulomatous colitis
Periodic acid–Schiff (PAS) positive macrophages
highly suspicious of
granulomatous colitis of
Boxer dogs
GRANULOMATOUS COLITIS OF BOXER DOGS
also known as Histiocytic Ulcerative Colitis
clinical signs are severe large bowel diarrhea, weight loss,
hypoalbuminemia
Boxer dogs are most commonly affected
Mastiff, Doberman Pinscher, and French Bulldogs are sporadically
affected
genetic susceptibility to dysfunctional bacterial clearance
285/19/2021
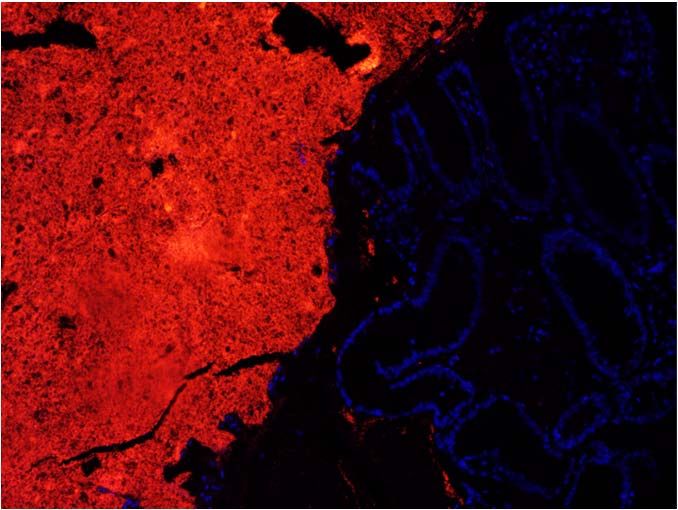
DIAGNOSIS BY VISUALIZING TRANSLOCATED BACTERIA BY
FLUORESCENCE IN SITU HYBRIDIZATION (FISH)
1. normal mucosa 2. granulomatous colitis in Boxer
dogs
Courtesy of Dr. Kenneth Simpson, Cornell University
THERAPY OF GRANULOMATOUS COLITIS
antibiotics for 6 weeks to clear invasive bacteria (E. coli)
antibiotic of choice was enrofloxacin
however, many resistant E. coli strains reported (up to 70%)
ideally, a bacterial culture of the biopsies for E. coli antibiotic
sensitivity is needed
good prognosis if response to antibiotics observed
295/19/2021
SUMMARY
chronic enteropathies are common in dogs and cats
no ideal diagnostic modality
empirical therapy needed
diet is the first line treatment in stable patients
antibiotics should be cautiously used in regular CE cases
dogs respond initially, but often relapse due to underlying disease
antibiotics are needed in cases of granulomatous colitis
QUESTIONS?
jsuchodolski@cvm.tamu.edu
https://tx.ag/DysbiosisGI
30You can also read

















































