MEMBER STATES INFORMATION SESSION ON INFECTION PREVENTION AND CONTROL ( IPC) - 7 March 2022 - WHO | World Health Organization
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
MEMBER STATES
INFORMATION SESSION ON
INFECTION PREVENTION AND
CONTROL (IPC)
7 March 2022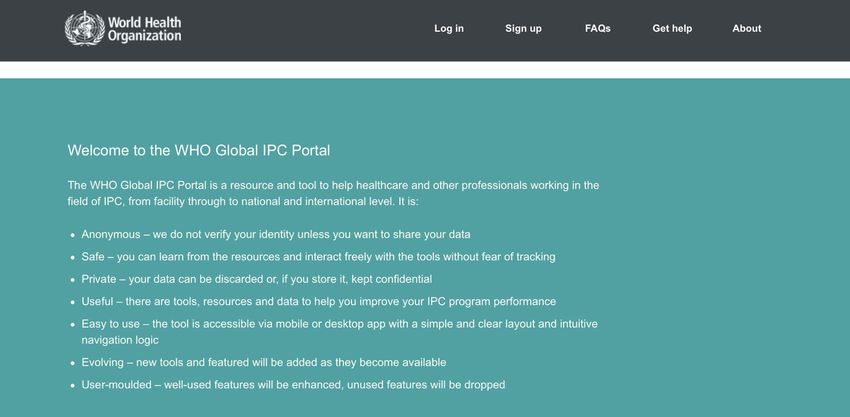
Agenda
Chair: Dr Rudi Eggers, Director, Integrated Health Services (IHS) department, UHC/LC division
Time Agenda item Speaker
(CET)
15.30 Welcome remarks Dr Zsuzsanna Jakab, Deputy Director-General and ExD a.i., UHC/LC division
15.35 Overview of the IPC situation Dr Rudi Eggers, Director, IHS department, UHC/LC division
worldwide: highlights of
achievements and gaps
15:45 Impact of IPC – Dr Benedetta Allegranzi, IPC Technical Lead, IHS department, UHC/LC division
WHO areas of work and critical Dr Silvia Bertagnolio, Unit Head, Surveillance, Prevention and Control department, AMR
guidance on IPC division
Dr April Baller, IPC Focal Point, Country Readiness Strengthening department, WHE division
16.00 Country capacity building Dr Maha Talaat, IPC focal point, Eastern Mediterranean Regional Office, on behalf of all
supported by regional offices regional offices
16.10 Priorities and strategic Dr Zsuzsanna Jakab, Deputy Director-General and ExD a.i., UHC/LC division
directions for IPC
16.20. Discussion All participants
16.55 Closing remarks TBD
17.00 Session closure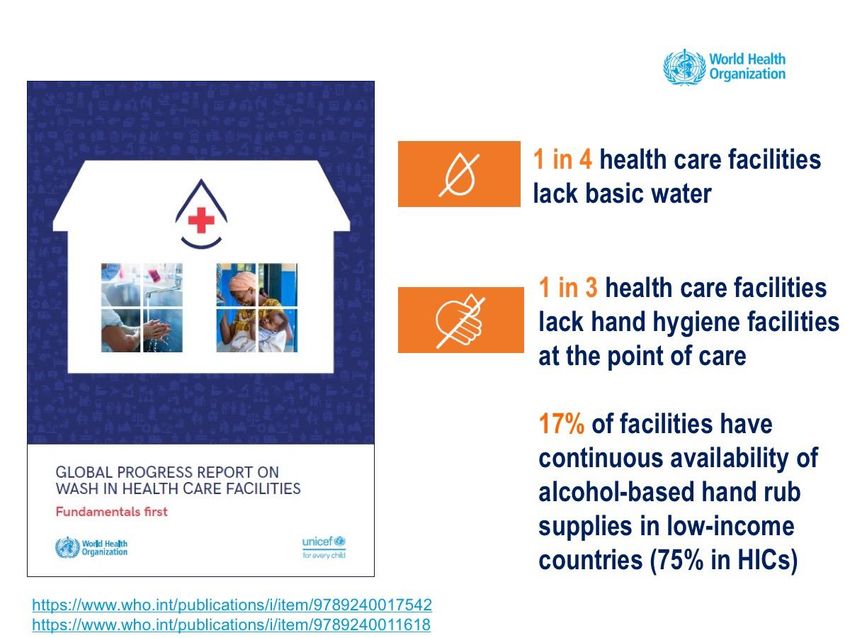
Member States Information Session on
Infection Prevention and Control
OVERVIEW OF THE IPC
SITUATION WORLDWIDE:
HIGHLIGHTS OF ACHIEVEMENTS
AND GAPS
Dr Rudi Eggers
Director, Integrated Health Systems department
UHC/LC WHO HQ
7 March 2022
Health care-associated infection (HAI)
also referred to as “nosocomial” or “hospital-acquired infection”
An infection acquired by a patient
during the process of care (including preventive, diagnostic and treatment services)
in a hospital or other health-care facility,
which was not present or incubating at the time of admission;
HAIs can also appear after discharge.
HAIs may also be acquired by health workers during health care delivery,
and by visitors.
Modified from: Report on the burden of endemic health care-associated infection worldwide. Geneva: World Health Organization; 2011. https://apps.who.int/iris/handle/10665/80135
4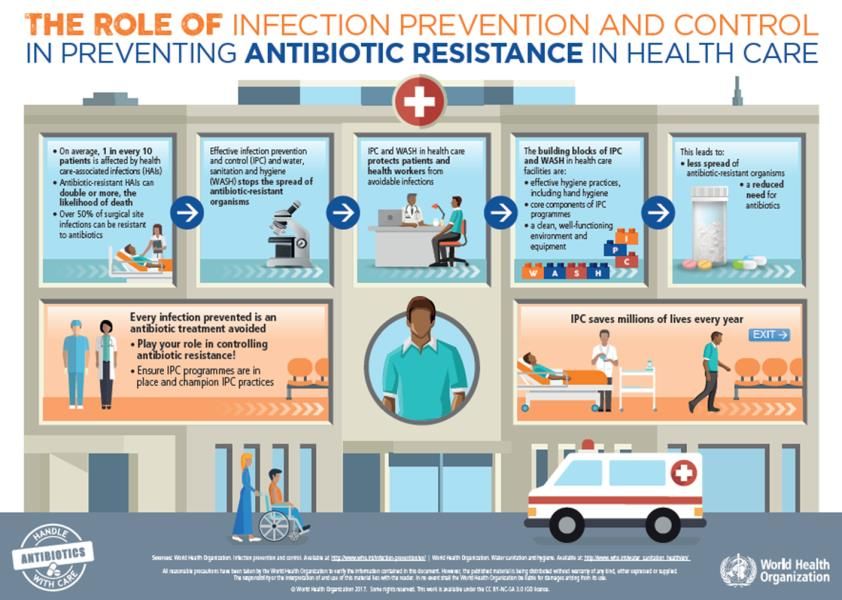
Global burden of HAIs (1)
Globally, hundreds of millions of people every year are affected
by health care-associated infections (HAIs), many of which are
completely avoidable
No country or health system, even the most developed or sophisticated,
can claim to be free of HAIs
• out of every 100 patients, 7 in high- and 15 in low-/middle-income
countries (LMIC) will acquire at least one HAI, in acute care hospitals
• 1 in every 10 affected patients dies of HAI
• 8.9 million HAIs occur every year in acute and long-term care facilities in EU/EEA
Sources:
• Report on the burden of endemic health care-associated infection worldwide. Geneva: World Health Organization; 2011. https://apps.who.int/iris/handle/10665/80135
• Allegranzi B, et al. Burden of endemic health-care-associated infection in developing countries: systematic review and meta-analysis. Lancet 2011;377(9761):228-41.
• Suetens et al. Prevalence of healthcare-associated infections, estimated incidence and composite antimicrobial resistance index in acute care hospitals and long-term care facilities: results from two European point
prevalence surveys, 2016 to 2017. Euro Surveill. 2018;23(46):pii=1800516. https://doi.org/10.2807/1560-7917.ES.2018.23.46.1800516
Global burden of HAIs (2)
Intensive care:
• High-income countries (HICs): up to 30% of patients affected by at least one HAI in intensive care units
• Lower/middle income countries (LMICs): incidence is at least 2─3 times higher.
• 1 in 4 cases (23.6%) of all hospital-treated sepsis cases are health care-associated
• 48.7% of sepsis with organ dysfunction treated in adult ICUs are hospital-acquired
• Mortality among patients affected by health care-associated sepsis was 24.4%, with an increase to
52.3% among patients treated in ICU
Neonatal care:
• Neonatal infection rates in LMICs are 3-20 times higher than in HICs
• Incidence of health care-associated sepsis in neonates is 7.5 times higher than in adults
• In hospital-born infants, HAIs account for estimated 4%- 56% of all deaths in neonatal period
Surgical care:
• Most frequent type of HAI in low- and middle-income countries (LMICs), 2nd & 3rd in Europe and the USA
• Most frequent complication of surgery in Africa
• WHO Report on the burden of endemic health care-associated infection worldwide, 2011. https://apps.who.int/iris/handle/10665/80135
• Markart R, et al. Intensive Care Med 2020, https://doi.org/10.1007/s00134-020-06106-2
• WHO Global Report on the Epidemiology and Burden of Sepsis, 2020. https://www.who.int/servicedeliverysafety/areas/sepsis/en/
• WHO Global guidelines for the prevention of surgical site infection, 2018. https://apps.who.int/iris/handle/10665/277399
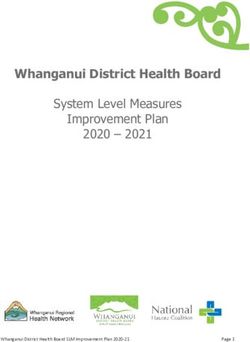
Comparing the burden of HAIs
with other infectious diseases in EU/EEA (2011-12)
HAIs
account for twice the burden
of 32 other infectious diseases
75% of DALYs attributable to AMR
in Europe is a result of HAIs
Mortality among patients infected
with MRSA is the double of those
infected with MSSA
DALYs: disability-adjusted life years, i.e. years of life lost to due to Mortality in patients infected with
premature mortality and years lived with a disability due to HAIs pathogens resistant to
carbapenems is about
Source: Cassini A, et al. PLoS Med *Cassini
Source: 2016;13(10):e1002150
A, et al. PLoS Med 2016;13(10):e1002150 (18 October 2016) .
** Cassini A, et al. PLoS Med (submitted). 3-times higher
COVID-19 Health worker cases & deaths
RISK FACTORS (Chou R et al, living review, https://pubmed.ncbi.nlm.nih.gov/32369541/
• High-risk exposures (e.g. involvement in intubations, more direct or intense patient contact,
or contact with bodily secretions)
• Not wearing masks or respirators appropriately
• Black and Asian race and Hispanic ethnicity relative to White race
• Contact with an infected household member or in a private setting
Interim findings of WHO case control study in 97 health facilities in 19 countries
Risk factors for COVID-19 in HCWs
➢ Prolonged close contact (>15min within 1 meter)
➢ Inconsistently wearing a respirator or a surgical mask or both compared to
consistently wearing a respirator during aerosol-generating procedures
➢ Not always appropriately performing hand hygiene during prolonged patient contact
Global number of deaths among HWs
with COVID-19 (Jan 2020-May 2021)
115,500 (80,000-180,000)
The impact of COVID-19 on health and care workers: a closer look at deaths. Geneva:
World Health Organization; 2021. https://apps.who.int/iris/handle/10665/345300
Global pulse survey on continuity of essential health services during the COVID-19 pandemic Source: Round 3 Global pulse survey on continuity of essential health services, Nov-Dec 2021 (reflecting situation during previous 6 months)
Infection prevention and control (IPC)
is an evidence-based approach and practical
solution designed to
prevent harm to patients and health workers
at every single health care encounter
across the whole health system
by stopping the spread of infection and antimicrobial
resistance (AMR)
http://www.who.int/infection-prevention/en/https://amrcountryprogress.org/ 2020-21
• 33%: no national IPC programme (A) or not implemented (B) (LICs 8.3 times more likely)
• 35%: IPC programmes properly implemented in healthcare facilities nationwide (D) and monitored (E)
• 32%: IPC programme implemented in selected health-care facilities (C)2021 WHO global survey on IPC
minimum requirements at the
national level – preliminary results
Lower- Upper-
Total Low High
Indicator % % middle % middle % %
N income income
income income
Total countries participating
65 - 9 - 14 - 24 - 18 -
(interim analysis)
Met 100% of national IPC programme
2 3% 0 0% 0 0% 0 0% 2 11%
minimum requirements
Met 75% of national IPC programme
32 49% 6 67% 6 43% 11 46% 9 50%
minimum requirements
Met 50% of national IPC programme
52 80% 7 78% 11 79% 17 71% 17 94%
minimum requirements
WHO confidential unpublished data
In 2020, 44% of countries indicated lack of IPC supplies and best practices as a major reason for essential health
services disruption (e.g., interruption of routine vaccination programmes) in the context of the COVID-19 pandemic
WHO. Pulse survey on continuity of essential health services during the COVID-19 pandemic: interim report, 27 August 2020 ( https://apps.who.int/iris/handle/10665/334048?locale-attribute=fr&)2019 WHO global survey on IPC in health
care facilities: 4440 facilities, 81 countries
Overall implementation of IPC
➢advanced: 50.7%
➢Intermediate or basic: 47.3%
➢Inadequate: 2%
• Only 16% of HCFs met ALL WHO IPC minimum requirements (MR),
➢ 0% in LICs
➢ 27% of primary & 11% of secondary/tertiary HCFs in HICs
• 69% met 75% of IPC MR
• 93% met 50% of IPC MR
Souce: Tomczyk S, et al. The Lancet Infectious Diseases 2022
https://doi.org/10.1016/S1473-3099(21)00809-42020 1.8 billion people are using health care facilities that lack basic water services 800 million people are using facilities with no toilets
2021 global survey on IPC minimum
requirements at the national level –
comparison with 2018 in 35 countries
• Same proportion of countries having a national IPC programme: 62.9% in 2018 and
2021
• Significant increases of key indicators, i.e. proportion of countries:
o that appointed a trained IPC focal point (25.7% vs 68.6%, p=0.004).
o having a dedicated budget (22.9% vs 48.6%, p=0.05)
o having an in-service IPC curriculum (60% vs 85.7%, p=0.04). But in 2021 only 36.9% of
countries are able to provide training materials and support for these training activities.
o promoting multimodal strategies for IPC interventions (54.3% vs 88.6%, p=0.006)
WHO confidential unpublished dataKey messages
• Patients affected by HAI and sepsis have prolonged hospital stay, excess mortality,
complications and long-term disabilities
• HAIs also add a significant burden to health systems, including increased workloads and costs
• HAI morbidity and mortality due to HAIs is 2-20 times higher in low- and middle-income countries
• Health care facilities can be amplifiers of outbreaks, involving both patients & health workers
• Antibiotic-resistant microorganisms are responsible for most of HAIs
• There is strong evidence on effectiveness and cost-effectiveness of IPC interventions
• While national IPC programmes may exist, they are often poorly funded & implemented (even in
high-income countries), with much lower implementation in low- and middle-income countries
• In 2021, some significant progress has been made on a number of IPC indicators but shocking
gaps still exist and sustainability should be ensuredMember States Information Session on
Infection Prevention and Control
IMPACT OF IPC -
WHO AREAS OF WORK AND
CRITICAL GUIDANCE
Dr Benedetta Allegranzi, IHS department, UHC/LC, WHO HQ
Dr Silvia Bertagnolio, SPC department, AMR, WHO HQ
Dr April Baller, CRS department, WHE, WHO HQ
7 March 2022IPC work at WHO
Global IPC Network
HQ IPC IPC GUIDELINES &
Task Force DEVELOPMENT
RESEARCH
GROUPS
HQ Sepsis
Coordination
GroupIPC decreases risk of SARS-CoV-2 infection among health workers Decreased risk significantly associated with: ➢training in IPC* ➢adequacy and appropriate use of PPE** ➢hand hygiene** ➢universal masking in health care facilities* *Chou R et al, living review, https://pubmed.ncbi.nlm.nih.gov/32369541/ **Chou R et al & WHO multi-center case-control study
IPC is cost-effective in response to outbreaks
OECD/WHO Joint Project on the COVID-19 pandemic
• Cost-effectiveness model used with data
regarding the first 180 days of the pandemic
• Combining increased access to PPE
with IPC training yields the greatest
global health and economic gains
➢ >50% of new infections among HCWs
in South-East Asia, Europe and the Americas,
and approximately one third of new infections
in other regions, could have been averted
➢ $7.2 billion USD net savings globally
➢ Hand hygiene also cost-effective in most
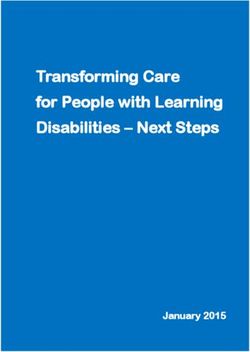
regionsEvidence about IPC impact on infections and
AMR as patient outcomes
35-70%
HAI • Implementing IPC programmes and interventions
reduction
• Single-bed rooms
• ABHR at the point
of care
50%
HAI • Improving hand hygiene compliance
reduction
• Multiple AMR
56% patterns in health
MRSA • In England according to a national target over 4 years care
reduction
44% • In African countries, implementing a prevention
SSI programme combined with safety climate
reduction improvementIPC is cost-saving: proper IPC saves lives and
allows facilities to MAKE money
• HAI extra costs: US $1,000-12,000, depending on the country
• US $7.2-14.9 billion spent on HAIs in the USA, in 2016
When IPC and hand hygiene are implemented in
combination with antibiotic stewardship programmes
Ensure the WHO core components for effective IPC
are in place!!
• OECD (2018), Stemming the Superbug Tide: Just a Few Dollars More. Available at oe.cd/amr-2018
• Forrester J, et al. J Pat Saf 2021; doi: 10.1097/PTS.0000000000000845
https://www.who.int/teams/integrated-health-services/infection-prevention-control/ipc-and-antimicrobial-resistanceWHO core components for
The guideline recommendations
effective IPC programmes
• http://www.who.int/infection-prevention/publications/ipc-components-guidelines/en/
• Zingg W et al. TLID 2015
• Storr J et al. ARIC 2017
• Price L et al. TLID 2017WHO IPC global guidelines https://www.who.int/teams/integrated-health-services/infection-prevention-control
Translating guidelines to action
Implementation manuals and resources
IPC national & facility level assessment tools
http://www.who.int/infection-prevention/tools/core-components/en/
https://www.who.int/teams/integrated-health-services/infection-prevention-control/core-componentsNew WHO IPC monitoring portal
Please contact your national IPC focal point
https://ipcportal.who.int/
and encourage your country’s participation!IPC and WASH https://washinhcf.org/
IPC & quality of care, patient safety
and primary care
https://www.who.int/teams/integrated-health-services/quality-health-services
https://www.who.int/teams/integrated-health-services/patient-safety
https://www.who.int/teams/integrated-health-services/infection-prevention-controlIPC & maternal, newborn, child adolescent health
and ageing care
• IPC training package for maternal & neonatal care
• Interprofessional Midwifery Education Toolkit
• WHO IPC recommendations for small and sick newborns
• IPC guidance for long term care facilities in the context of
COVID-19
• https://www.who.int/teams/maternal-
newborn-child-adolescent-health-and-
ageing/covid-19
• https://www.who.int/teams/sexual-
and-reproductive-health-and-
research-(srh)/overviewIPC and antimicrobial resistance (AMR)
• Implementation of Objective 3 of the Global Action Plan on AMR
• Indicator 3.d.2 for AMR: reducing the percentage of bloodstream
infections due to selected antimicrobial-resistant organisms
• Tripartite AMR Country Self-Assessment Survey (TrACSS)
• Global Antimicrobial Resistance and Use Surveillance System
• IPC competencies and curriculum
• IPC integration with antimicrobial stewardship
• Training package: leadership skills to implement multisectoral AMR NAPs
• OpenWHO course: Reducing antimicrobial resistance of treatable
sexually transmitted infections in antenatal care
https://www.who.int/teams/integrated-health-services/infection-prevention-control/ipc-and-
antimicrobial-resistance
https://www.who.int/teams/surveillance-prevention-control-AMRGlobal AMR research agenda Priority questions (including IPC) to curb AMR ➢ 4 cross-cutting domains o Descriptive of AMR burden and drivers o Delivery of existing interventions with better quality o Development of improved interventions (reduce costs, optimize impact and feasibility) o Discovery and demonstration of new tools and interventions ➢ A ranking methodology developed by WHO (CHNRI) ➢ In collaboration with WHO technical teams ➢ Based on scoring from large global panel of experts ➢ Ensuring research triggers effective and actionable interventions
IPC during COVID-19 pandemic: Thematic areas of work https://www.who.int/publications/m/item/covid-19-research-and-innovation---powering-the-world-s-pandemic-response-now-and-in-the-future
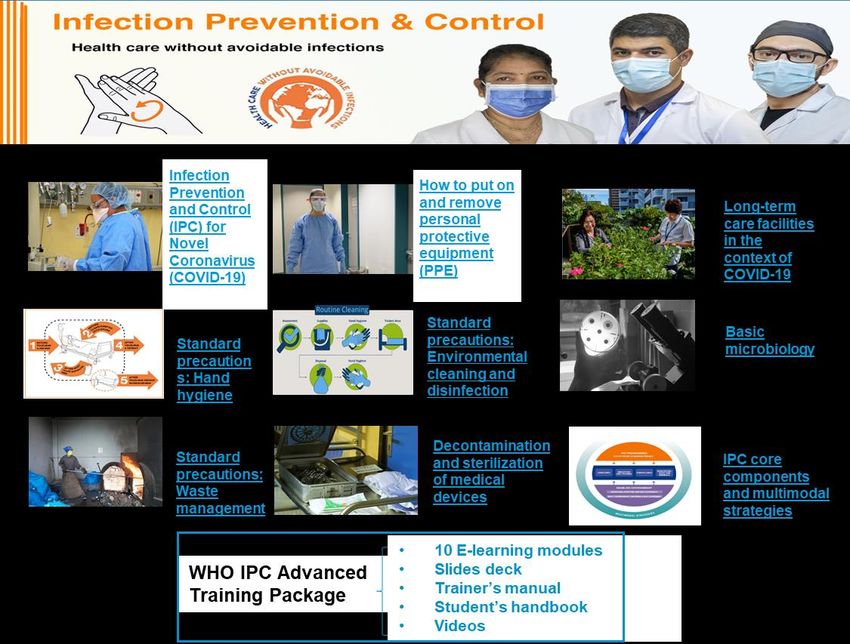
WHO IPC Basic, Advanced and COVID-19 Training
5 COVID-19 courses
• 1,317,000 enrollments
• 74% completion rate
11 basic IPC courses
• 629,000 enrollments
• 64% completion rate
https://openwho.org/COVID-19 Operational readiness and Country support in
Fragile, Conflict, Vulnerable (FCV) States
Northern
Ethiopia(Tigray):
Country support PPE supplies
through technical WASH and IPC
specialists
missions
Scaling Up IPC Capacity In Cox’s Bazar In Response To
Yemen COVID-19 response
Covid-19 Pandemic Furthers Streamlining Of Best
Practices In General Health Facilities
Checklist for health facility level IPC in
the event of a surge of COVID-19
HEALTH
EMERGENCIES
programmeOther outbreak responses: Ebola and Marburg Virus Disease and
IPC Technical Guidance development
2014 2016 2018
• Technical support to the field teams in Guinea, DRC, Ivory Coast May 2021- April July-
• IPC EVD training package updates and adaptation of 2022 September2022
packages for Marburg Virus Disease
Phase 1: Health facility setting Phase 3: Special populations
• IPC/WASH preparedness and readiness webinars in French and
English for surrounding countries:
Côte d’Ivoire, Guinée Bissau, Liberia, Mali, Sierra Leone and Senegal >200
participants over 2 days April July 2022
Phase 2: Community setting
HEALTH
EMERGENCIES
programmeFramework and Toolkit for IPC Outbreak Preparedness,
Readiness and Response
To provide national and subnational authorities with:
HEALTH
EMERGENCIES
programmeTHANK YOU and to
WHO IPC colleagues!
Alessandro Cassini April Baller
Nita Bellare Mandy Deeves
Claire Kilpatrick Hannah Hamilton
Aimee Ramos Lauretha Madumere
Paul Rogers Patrick Mirindi
Julie Storr Madison Moon
Ermira Tartari Pierre Yves Oger
Joao Toledo Maria Clara Padoveze
Anthony Twyman Leandro Pecchia https://www.who.int/teams/integrated-
Paul Schumacher health-services/infection-prevention-control
Sara Tomczyk
Vicky Willet
IPC regional focal points: G. Avortri, AP Coutinho Rehse, L. Cihambanya, P.
Kariyo, M. Letaief, B. Ndoye, N. Prasopa-Plaizier, A. Shah Singh, H. Sobel,
M. Talaat Ismail, B. ZayedMember States Information Session on
Infection Prevention and Control
COUNTRY CAPACITY BUILDING
SUPPORTED BY
REGIONAL OFFICES
Dr Maha Talaat, IPC focal point, Eastern
Mediterranean Regional Office
7 March 2022A stepwise approach for
implementation
https://www.who.int/publications/i/item/9789241516945Supporting countries with a tailored, stepwise
implementation approach
Implementation cycle Multidisciplinary
team
https://www.who.int/teams/integrated-health-services/infection-prevention-control/core-componentsAssessments in a spirit of
improvement
• Regular assessments of IPC programmes are essential for
continuous quality improvement.
• Assessment helps to identify existing strengths and take
stock of achievements made so far to convince decision-
makers that success and progress is possible.
• Assessment also helps to identify gaps and create a sense
of urgency for the changes needed to improve IPC
• Data are of value, ONLY if they are used for action, i.e. to
elaborate and implement targeted and feasible
improvement plans and to track progressMember States Information Session on
Infection Prevention and Control
PRIORITIES AND STRATEGIC
DIRECTIONS FOR IPC
Dr Zsuzsanna Jakab, Deputy Director-
General and ExD a.i., UHC/LC division
7 March 2022IPC is a tried-and-true approach that is
effective and cost-saving
5 reasons to invest in IPC
1 2 3 4 5
Ensures quality of Directly improves Reduces health Consists of proven Is scalable and
care and patient and key health outcomes care costs and out- strategies supported by adaptable to the
health workers’ and saves lives implementation aids
safety of-pocket expenses local contextCritical priorities for IPC in national and international
health agendas (1)
1. Functional IPC • Dedicated budget
programmes • Trained IPC professionals
2. IPC minimum • At national and facility levels in all countries
requirements • Demonstrated by M&E of key IPC and WASH indicators
3. Decisive and visible • At the highest levels
political commitment and • Allocation of national and local health budgets
leadership engagement • Establishing targets for IPC investment
• To enforce IPC requirements and policies through accreditation
4. Regulations and legal and accountability systems
framework • Reporting of key IPC performance indicators and targets
Source: EB150 ReportCritical priorities for IPC in national and international
health agendas (2)
5. Integration and
• Specific IPC programme that horizontally integrates/aligns with
alignment with other existing ones
programmes
6. Embedding IPC within • Tools and SOPs to support IPC understood and practiced at
the patient pathway and the point of care in all clinical areas
clinical care • Workflow, human factors, ergonomics to be considered
• Implementation of accredited IPC curricula (pre- & postgraduate,
7. IPC training and in-service)
education at all levels • Based on the WHO IPC core competencies
IPC professionals:
8. Human resources and • with a recognized career pathway
career pathway for IPC • empowered with a clear mandate and authority
• accountable for implementation and reporting impact
Source: EB150 ReportCritical priorities for IPC in national and international
health agendas (3)
• Connected with existing platforms (e.g. GLASS)
9. Surveillance of HAIs • Existing standardized surveillance protocols (e.g. ECDC
and AMR in health care PPS)
• Data must be used locally for action
• Using standard M&E approaches
• Regular assessments and feedback to health workers
10. Monitoring IPC
• Data must be used locally for action
programmes • WHO Global IPC Portal is a protected and confidential
solution
• Tailored & consistent communications
11. IPC and • Authoritative source, based on science
communications • Multiple target audiences
Source: EB150 ReportIPC part of other health priorities & resolutions
2021: WHA resolution 74.7 on
2020: WHA resolution IPC as part of preparedness
73.8 on IPC as part of and response
strengthening IHR
2019: WHA resolution
72.6 on IPC as part of 2020: WHA resolution 73.1 on
patient safety IPC as part of the COVID-19
response
2015: WHA resolution 2019: WHA resolution
72.6 on IPC as crucial 72.7 on IPC as part of
part of quality of care WASH
2017: WHA resolution
1995: WHA
70.7 on IPC as part of
resolution 48.7 on
prevention of sepsis
IPC as part of IHR
2015: WHA resolution
58.27 on IPC as 3rd
objective of GAP AMRElevating the importance of IPC
WHO advocacy
&
IPC on EB150 MS information EB150
MS highlights of EB report
agenda session 1 discussions
IPC
at WHA/EB 2021Thanking all Member States (MS)
intervening at EB150
• Interventions were made by the following MS; France for the EU, Colombia, Malaysia, Singapore, Tajikistan, Denmark,
UK, Republic of Korea, Japan, Kenya, USA, Canada, Thailand, Spain, China and Brazil, Guinea Bissau on behalf of the
African region, Oman, Philippines, Singapore, Syria on behalf of the Easter Mediterranean region and Timor Leste
• MS consistently highlighted the importance of IPC in addressing:
o the widespread concern about the silent burden of AMR and health care-associated infections (HAI) but also its
o infectious hazard health emergency preparedness and response
o health worker and patient safety
o provision of high-quality and safe health care through
o health systems strengthening with a primary health care approach.
• MS fully recognized the gaps in IPC programmes highlighted by the pandemic
• MS highlighted that the COVID-19 pandemic response also presents a unique opportunity to
o strengthen IPC programmes at all levels
o save lives and money
o help restore communities’ trust in health care
• Guinea Bissau on behalf of the African region, Oman, Philippines, Singapore, Syria on behalf of the Easter
Mediterranean region and Timor Leste called for WHO to develop a global IPC strategy
51Ideal next steps for IPC
WHA IPC global
IPC global
MS resolution IPC global strategy
EB strategy
information requesting strategy adoption by
discussions decision by
session 2 IPC global development EB and WHA
WHA
strategy 2023Conclusions: Preventing HAI and AMR is Now! • Harm acquired where healthcare is provided should no longer be accepted. • Several countries have been able to introduce IPC standards despite limited resources and constrained situations. • A global strategy would support a wider implementation of the WHO core components for IPC and WASH. • This will save patient and health worker lives and health care costs.
Thank you for your attention https://www.who.int/teams/integrated-health- services/infection-prevention-control
You can also read