Meeting of the Perinatal Health Committee - December 7, 2020 - North Carolina ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Meeting of the Perinatal Health Committee December 7, 2020

Welcome and roll call attendance Approval of minutes from meeting on 10/26/2020 Unapproved minutes were sent to committee, are linked to on agenda, and are available on the CFTF website at: https://www.ncleg.gov/DocumentSites/Committees/NCCFTF/Perinatal%20Health/2020- 2021/agenda,%20minutes,%20and%20roster/PH%20minutes%2010-26-2020.pdf

Child Fatality Task Force
Recommendations to Strengthen the
NC Child Fatality Prevention System
(2019/2020 carry-over item)
Kella Hatcher, JD
Executive Director
NC Child Fatality Task Force
Initial 2017 discussions led to two-day Child Fatality
Prevention System Summit April 2018: gathering of
over 200 people
Post-Summit work involved research on other states’
CFP systems, consultation with national experts,
stakeholder discussions
Journey of
CFTF recommendations addressing CFP System
CFP strengthening adopted in the Child Welfare Reform
Plan from the Center for Support of Families
Strengthening CFTF recommendations were addressed in 2019
Work Appropriations Act which did not become law (HB 825
was included in HB 966)
NCDHHS has continued work to move
recommendations forward because they are aligned
with DHHS priorities and were part of Child Welfare
Reform Plan; this work has included convening of
stakeholder group by NCIOM
MAIN COMPONENTS OF CURRENT NC CFP SYSTEM:
FOUR TYPES OF REVIEW TEAMS PLUS TASK FORCE
These three
components Two State Child
addressed in
Types of Uses local team Fatality
Article 14 of Review
Juvenile Code Local members
Review Team
Teams
This component
State Child addressed in G.S.
Fatality §143B-150.20
Prevention
Team NC Child
Each type of team Fatality One case may be
handles data,
information, and
Task reviewed by
reporting Force three different
differently; minimal types of teams
Policy only; no
data is collected
case reviews
Current System * Structure *This graphic was created in 2018 and this ED position is now at DHHS

Current System Process

2019/2020 CFP Strengthening Recommendations

I. Implement centralized state-level staff with whole-system support in one
location; OCME child fatality staff remains in OCME; form new Fatality
Review and Data Group to be information liaison
Centralizes
leadership;
streamlines state-
level support
functions Team approach
New FRD group
increases efficiency,
ensures connection
capacity,
of information
standardizes tools
among local teams,
and resources for all
OCME, and CFTF
teams
Connects
system
components
9
II. Implement a centralized electronic data and information system that
includes North Carolina joining 45 other states to participate in the
National Child Death Review Case Reporting System
Ensures Ensures
meaningful data appropriate
analysis and data protection
reports and sharing
Expands,
Ensures data modernizes, and
entry and standardizes
reporting by all Maximizes data capture,
teams usefulness of analysis, and
information reporting
learned from
reviews
10III. Reduce the volume of team reviews by changing the types of deaths
required to be reviewed by fatality review teams to be according to
certain categories most likely to yield prevention opportunities
• Undetermined causes
• Unintentional injury
• Violence Capacity to More motivated
• Motor vehicle incidents strengthen and engaged
• Child abuse or neglect/CPS infant reviews team members
involvement
• Sudden unexpected infant death
Optimization of
• Suicide
efforts &
• Deaths not expected in the next
resources to
6 months
yield prevention
• [Potential for additional special
criteria for infant deaths; other opportunities
deaths; FIMR]
11IV. Reduce the number and types of teams performing fatality reviews by combining the functions
of the four current types of teams into one with different procedures and required participants for different
types of reviews and giving teams the option to choose whether to be single or multi-county teams
DHHS should study Recognizes
and determine an Preserves critical strength of
effective functions & diverse local team Recognizes that
framework for contributions by combining some
meeting federal multidisciplinary county teams may
requirements for
teams and state- optimize efforts.
Citizen Review
Panels and for
level staff.
reviewing active
DSS cases.
Streamlines, Eliminates There is a more
standardizes and duplication to
effective way to
improves review optimize
overall efforts have Citizen
processes and Review Panels
& resources
procedures
12V. Formalize the 3 CFTF Committees with certain required members;
expand CFTF reports to address whole CFP System and to be distributed to
additional state leaders.
Broader report
provides better and
deeper information to
Ensures broad advance prevention
opportunities. More state
and consistent
member leaders will be
informed about
participation prevention
in committee opportunities.
work.
Maintains CFTF
strengths &
formalizes long
standing
effective system
13Funding recommendations (2020) • Support for maintaining current state funding supporting Child Fatality Prevention System work, and for additional recurring funding to support this work pursuant to DHHS determinations to be made related to the most appropriate placement and staffing configuration for this central office as well as funding needs of local health departments to support CFP system work. • Pursuant to DHHS determinations to be made related to launching a Fetal and Infant Mortality Review Program to inform state-level action related to the prevention of child deaths, support funding to enable implementation of the evidence-informed practice of Fetal and Infant Mortality Reviews as a pilot.
Why Is This Important?
Why Now?• Local Social • Health Care
Services Provider
• Local Health • Emergency
Department medical or Local teams consist of
• Law Enforcement firefighter community leaders;
• District Attorney • District Court teams are rich in
Judge
• Local Community expertise & ripe for
Action Agency • County Medical
Examiner collaboration needed
• Local School to strengthen health
Superintendent • Local childcare
• County board of
facility or Head and safety in their
Start
social services communities.
• Parent of child
• Mental Health who died
• Guardian ad LitemUltimate Goal: Prevent Child Deaths & Maltreatment; Support Child Safety & Wellbeing • OPTIMIZE LOCAL TEAM EFFORTS: CFP State Office structure, and eliminating duplication supports local teams to optimize work and facilitate local prevention efforts to save lives at a time when the demands on team members in their communities may be greater than ever. • DATA TO UNDERSTAND TRENDS: A sophisticated data system that collects richer layers of data makes reviews more valuable and easier for understanding and reacting to what’s happening at the state and local level at a time when society is experiencing new and major changes. • ADDRESSING INFANT MORTALITY: System strengthening involves more best practice attention to infant deaths at a time when North Carolina’s infant mortality rate has been among the worst dozen in the nation, disparities persist, and infant deaths make up two- thirds of all child deaths. • ENSURING USE OF INFORMATION LEARNED: Ensuring that information/recommendations from reviews reaches appropriate agencies and leaders is critical to making reviews effective. • MORE STATE-LEVEL PREVENTION WORK: CFP State Office provides a structure for facilitating or implementing various prevention initiatives, including efforts to seek grant opportunities.
Prior CFTF CFP System strengthening recommendations and proposed legislation involved DHHS developing a plan for system restructuring
Child Fatality Prevention
System
Walker Wilson
Assistant Secretary of Policy
Karen Wade
Policy Advisor
NC Department of Health and Human Services
December 7, 2020
19Overview of Progress on Recommendations
• NCDHHS leadership established workgroup to
discuss goals and structure of a new office.
− Identifying the type of team needed in the office to
implement this important work.
• Interviews with other states and national subject
matter experts on best practices.
• NCIOM convened multiple meetings with
stakeholders across the state. The group’s input is
helping inform:
− How to reduce the number and types of teams
− The types of deaths required to be reviewed
− Connecting to the national data systemKey Principles
• The need for specialized staff in a centralized state
office.
− Staff to provide training and technical assistance to county
teams and identifying statewide trends.
• Importance of maintaining the structure of fatality
reviews conducted on the local level.
− County or multi-county teams conduct reviews, with the state
office providing guidance and a global view on fatality trends
across NC.
• Joining the National Child Death Review Case
Reporting System and the 45 other states who are
already participating.
− Centralized office will lead implementation by establishing
policies and procedures.Key Principles
• Making the 9 recommended categories of death
be required for review by the local teams:
− Undetermined causes, unintentional injury, violence,
motor vehicle incidents, child abuse or neglect/child
protective services involvement, sudden infant death,
suicide and deaths not expected in the next six months.
• Establishing a separate system for Citizen
Review Panels.
− Focused on examining the policies, procedures and practices of state
and local child protection agencies.SUMMARY OF CFP SYSTEM RECOMMENDATIONS
I. Implement centralized state-level staff with whole- IV. Reduce the number and types of teams performing
system support in one location; OCME child fatality staff fatality reviews by combining the functions of the four
remains in OCME; form new Fatality Review and Data current types of teams into one with different
Group to be information liaison. procedures and required participants for different types
of reviews and giving teams the option to choose
II. Implement a centralized electronic data and whether to be single or multi-county teams. DHHS
information system that includes North Carolina should study and determine an effective framework for
participating in the National Child Death Review Case meeting federal requirements for Citizen Review Panels
Reporting System. and for reviewing active DSS cases.
III. Reduce the volume of team reviews by changing the V. Formalize the 3 CFTF Committees with certain
types of deaths required to be reviewed by fatality required members; expand CFTF reports to address
review teams to be according to certain categories most whole CFP System and to be distributed to additional
likely to yield prevention opportunities. state leaders.
Funding: maintain current CFP funding and appropriate additional funds pursuant to DHHS determinations related
to state office, local teams, and FIMR pilot
Today’s agenda also contains 2020 recommendations
23Committee discussion and determination addressing carry-over Child Fatality Prevention System strengthening recommendations for 2021
Kin Care/ Safe Days and
Paid Family & Medical Leave:
Concrete Supports that Improve Child Health and
Decrease Infant Mortality
Presentation to the NC Child Fatality Task Force, Perinatal Health Committee
by Beth Messersmith, MomsRising, December 7, 2020• 65% of North Carolina children live in households where all
Parents & available parents are currently working.
North
• Two-thirds of mothers with children under age six are in the US
Carolina’s labor force, and three-quarters of mothers with children under 18
Workforce are in the labor force.
• In North Carolina, about 44% of mothers are the sole or primary
breadwinner for their families, earning at least half of their total
household income, and an additional 21% of mothers are married
mothers whose wages comprise at least 25% of total household
earnings.
• Each year about 1.6% of North Carolina’s labor force gives birth.
Source: Status of Women in NC: Employment and Earnings; US Bureau of Labor Statistics, “Breadwinning Mothers Continue to be the US Norm’”, and “Pregnant Workers Make Up a Small Share of the Workforce and Be be Readily Accommodated: A State-by-State Analysis”The Role of Social Determinants of Health
Paid Sick Days and Paid Family and Medical Leave:
How They are Different and Why We Need Both
Paid Sick Days Paid Family & Medical Leave
• To stay home and recover from a short-term • To address a serious personal health condition, like
illness, like the common cold cancer, that requires longer-term care or treatment
• Access preventative care • Care for a family member with a serious health
• Care for a sick child or family member condition
• Attend school meetings related to a child’s health • Care for a newborn, newly adopted child, or newly-
condition or disability placed foster child
• Allow survivors of domestic violence, stalking, or • Care for a family member injured in military service
sexual assault (or their close family member) to or to deal with exigencies of military deployment
use paid sick time to recover or seek assistance • The length is adequate to cover the full range of
related to an incident personal medical and family caregiving needs
established in the Family and Medical Leave Act
*Note-Kin Care/ Safe Days as described in proposal before CFTF expands who paid (FMLA)
or unpaid, job-protected sick days can be used to care for and the purposes for
which they can be usedWhy do these matter? ● Brain Science: early experiences have long term impacts ● Key to fostering protective factors (concrete supports, knowledge of parenting & child development, strengthening resilience, social connections, social and emotional competence) ● Research proven to improve child well-being and outcomes
Impact on Business
Businesses are already impacted by employees’ caregiving needs
In NC, women’s workforce participation declined from 2002 to
2016, from 59.9 percent to 57.3 percent.
28 percent of women and 15 percent of men work part time in NC,
with 26 percent of PT workers citing family obligations and
childcare problems as the reason they don’t work FT.
75 percent of mothers and 50 percent of fathers have passed up
work opportunities, switched jobs, or quit to care for their
children.
Nearly 40 percent of parents say they’ve left a job because it lacked
flexibility
These trends can also negatively affect career attainment of
parents with young children, especially mothers.
Source: NC Council for Women and Youth Involvement and Institute for Women’s Policy Research (2018) “Status of Women in NC: Employment and Earnings.”; “North Carolina Employers Agree: Family-Friendly Practices Are Good for Business,” Family Forward NC.
https://files.familyforwardnc.com/wp-content/uploads/2018/04/Family-Forward-Research-Report_Online_091218.pdf; “Research and Analysis: Family Friendly Policies and Practice,” Family Forward NC. https://files.familyforwardnc.com/wp-
content/uploads/2018/04/F_NCECF_Family_Friendly_Policies_Presentation_020218.pdfBenefits to business of being
family-friendly
• NC employees think employers who are family-
friendly have a competitive advantage, according to
a study of 300 NC employers and 300 employees
• 73 percent of NC employees say they would be more
committed to their employers if they had more
family-friendly practices
• 94 percent say family-friendly policies help
businesses attract and retain talent
• Employers agree—71 percent think family-friendly
policies have a positive impact on their organization
and those who’ve incorporated them see the positive
benefits firsthand.
Source: “North Carolina Employers Agree: Family-Friendly Practices Are Good for Business,” Family Forward NC. https://files.familyforwardnc.com/wp-content/uploads/2018/04/Family-Forward-Research-Report_Online_091218.pdf; “Research
and Analysis: Family Friendly Policies and Practice,” Family Forward NC. https://files.familyforwardnc.com/wp-content/uploads/2018/04/F_NCECF_Family_Friendly_Policies_Presentation_020218.pdfSick Days, Kin Care, & Safe Days
In NC, 1.6 million workers– 38 percent of our state’s workforce have 0 paid sick days.
For a typical family without paid sick days, on average, 3.3
days of pay lost due to illness are equivalent to the
family’s entire monthly health care budget, and 2.7 days Source: Institute for Women’s Policy Research & National Partnership for Women & Families. (2015, May). Workers’
Access to Paid Sick Days in the States. Table 2. Retrieved 8 July 2015, from http://www.nationalpartnership.org/research-
library/work-family/psd/workers-access-to-paid-sick-days-in-the-states.pdf; Green, Andrew, Filion, Kai, and Gould, Elise.
are equivalent to its entire monthly grocery budget. (2011) “The Need for Paid Sick Days: The Lack of a Federal Policy Further Erodes Family Economic Security.” Economic
Policy Institute. https://www.epi.org/publication/the_need_for_paid_sick_days/Who has access to paid sick days?
● Nationwide, more than 34 million workers can’t earn paid
sick days.
● Millions more can’t earn paid sick time they can use to care
for a sick child or family member or take them to access
preventative care.
● Nearly ¼ of US adults (23 percent) have lost a job or been
threatened with job loss for taking time off due to illness
or to care for a sick child or relative.
● One-quarter to one-half of domestic violence survivors
report losing a job in part due to the violence.
Source: U.S. Bureau of Labor Statistics. (2018, July 20). National Compensation Survey: Employee Benefits in the United States, March 2018. (Table 5). Retrieved 4 October 2018, from https://www.bls.gov/news.release/pdf/ebs2.pdf; Smith, T. W., & Kim, J. (2010, June). Paid Sick Days:
Attitudes and Experiences. National Opinion Research Center at the University of Chicago for the Public Welfare Foundation Publication. Retrieved 4 October 2018, from http://www.nationalpartnership.org/research-library/work-family/psd/paid-sick-days-attitudes-and-
experiences.pdf; U.S. General Accounting Office, Health, Education, and Human Services Division. (1998, November). Domestic Violence Prevalence and Implications for Employment among Welfare Recipients (GAO/HEHS-99-12). Retrieved 4 October 2018, from
http://www.gao.gov/archive/1999/he99012.pdfThe problems are even more profound for low wage
workers:
Nationally, only 57 percent of the lowest paid private
sector employees had the ability to earn paid sick days.
In NC, 68 percent of those in the lowest earnings
bracket did not have access to any paid sick days.
Workers in frequently low-paying jobs, such as food
prep, personal home care, and childcare are among
the least likely to have access and most likely to be
unable to afford an unpaid day away from work.
Disparities in access to paid sick days
disproportionately expose Black and Latinx workers
to increased risk of illness and increase racial health
disparities.
Nearly half (48 percent) of Latinx workers and more
than one-third (36 percent) of Black workers report Disparities in access
having no paid time away from work.
Source: Institute for Women’s Policy Research & National Partnership for Women & Families. (2019, February). Access to Paid Sick Time in NC.; Xia, J., Hayes, J., Gault, B., & Nguyen, H. (2016, February 17). Paid Sick Days Access and Usage Rates Vary by Race/Ethnicity, Occupation,
and Earnings. Institute for Women’s Policy Research Publication. Retrieved 4 October 2018, from https://iwpr.org/publications/paid-sick-days-access-and-usage-rates-vary-by-raceethnicity-occupation-and- earnings/; Kumar, S., Crouse Quinn, S., Kim, K. H., Daniel, L. H., &
Freimuth, V. S. (2012, January). The Impact of Workplace Policies and Other Social Factors on Self-Reported Influenza-Like Illness Incidence During the 2009 H1N1 Pandemic. American Journal of Public Health, 102(1), 134-140. doi: 10.2105/AJPH.2011.300482
4 U.S. Bureau of Labor Statistics. (2019, August 29). Access to and Use of Leave Summary (Table 1). Retrieved 7 October 2020, from U.S. Bureau of Labor Statistics website: https://www.bls.gov/news.release/leave.t01.htmSick days, Kin Care, & Safe Days • Sick Days-Time earned off from work, whether paid or job-protected unpaid, for an employee to use to recover from a short-term illness or injury. Sometimes can be expanded to include sickness / well-being needs of employees’ family, to access preventative care, or for other well-being related needs • Kin Care-Explicitly says that whatever kind of sick leave an employee earns it can be used to care for a family member. May also expand to include accessing preventative care or other needs • Safe Days-Explicitly says that whatever kind of sick leave an employee earns it can be used to deal with the physical, emotional, or legal impacts of domestic violence, sexual assault, or stalking or to seek safety.
Health and Safety Benefits to
Children
• Paid sick leave is a primary factor in a parent’s decision to stay home
when their child is sick.
• Lack of access to affordable childcare for sick children means without
access to paid sick days or sick days that can be used for family
members, sick children are often left home alone sick or sent to
school or childcare sick.
• Allowing parents to stay home prevents spread of illness.
• Allows parents to address children’s health needs such as managing
health complications or disabilities, well-child visits, vaccinations.
• 9,490 NC children affected by domestic violence and 3,040 by sexual
assault each year. Parents need time off to address the physical,
mental, and legal impacts of these incidents.
Source: S. Jody Heymann, Alison Earle, and Brian Egleston, “Parental Availability for the Care of Sick Children,” Pediatrics vol. 98 no. 2 (August 1996): 226-230.; S. Jody Heymann, Forgotten Families: Ending the Growing Crisis Confronting Children and Working Parents in the Global
Economy (Oxford University Press, 2006).; Isabelle Diehl, “The prevalence of colds in nursery school children and non-nursery school children,” Journal of Pediatrics vol. 34 no. 1 (January 1949): 52-61.; Lennart Hesselvik, “Respiratory infections among children in day nurseries,” Acta
Paediatricia Scandinavica no. 37 sup. S74 (May 1949): 1-103.; Hamman, Mary Kathryn. 2011. “Making Time for Well-Baby Care: The Role of Maternal Employment.” Maternal and Child Health Journal 15 (7): 1029–36.; DeRigne, LeaAnne, Patricia Stoddard-Dare, and Linda Quinn. 2016.
"Workers without paid sick leave less likely to take time off for illness or injury compared to those with paid sick leave." Health Affairs 35(3): 520-527; Hamman, Mary Kathryn. 2011. “Making Time for Well-Baby Care: The Role of Maternal Employment.” Maternal and Child Health Journal 15
(7): 1029–36.; DeRigne, LeaAnne, Patricia Stoddard-Dare, and Linda Quinn. 2016. "Workers without paid sick leave less likely to take time off for illness or injury compared to those with paid sick leave." Health Affairs 35(3): 520-527; 2018 Data from NC Coalition Against Domestic Violence.COVID and Sick Days: Families First Coronavirus Response Act Families First Coronavirus Response Act (FFCRA) passed April 1, 2020 provides emergency paid sick leave and emergency paid family leave: -covered employee can take 2 weeks (or up to 80 hours) of paid sick time if the employee is unable to work (or unable to telework) due to a need for leave because they are subject to a quarantine order, have been advised by a medical professional to self-quarantine, are experiencing COVID-19 symptoms and are seeking a medical diagnosis, are caring for an individual subject to a quarantine or self-isolation notice, are caring for a child whose school or place of care is closed (or child care provider is unavailable) for reasons related to COVID-19 -A covered employee can take up to 10 weeks of emergency, expanded paid family leave (in addition to the 2 weeks of sick leave for a total of 12 weeks), only if it is to care for a child whose school or place of care is closed or childcare provider is unavailable for reasons related to COVID-19. -exemptions exclude employers with more than 500 employees as well as many employees at small businesses along with health care workers, emergency responders, and most federal employees. -excludes more than 106 million workers nationally and excludes more than 3.1 million NC workers, well more than half of our state’s workforce -sunsets December 31, 2020
According to a recent study from researchers at Cornell University
Role of paid and the Swiss Economic Institute, states with new access to
emergency paid leave during the pandemic have seen 400 fewer
sick days in cases per day, further underscoring that paid leave is one of the best
tools for slowing the spread of the virus and combating the
pandemic.
slowing Unsurprising given that previous research had already shown that
COVID-19 increasing sick leave coverage causally reduces the spread of the flu.
Focusing on “normal” times and economic conditions, research has
spread shown that employees who lack paid sick leave are more likely to
go to work sick, have financial hardships, skip preventive health
care, and spread contagious diseases.
Economic models suggest that “contagious presenteeism”
behavior—working sick with a contagious disease—decreases when
employees gain access to paid sick leave, as they are more likely to
stay home.
In total, as of February 2020, 12 states and the District of Columbia
had implemented state-level sick pay mandates, whereas 39 did not.
Flaws with the approach: exemptions, sunset, doesn’t address
repeated or time-lagging family exposures.
Source: See endnote.Request to the Child Fatality Task
Force
• Proposing the Task Force endorse passage of a kin care
and safe days bill that would guarantee all NC workers the
right to use their sick days (whether paid or job-protected
unpaid) to care for a sick loved one, seek preventative
care, or deal with the physical, mental, or legal impacts of
domestic violence, sexual assault, or stalking.
• Other states, including Georgia, have passed some
variation of these.
• On October 23, 2019, Gov. Cooper signed an Executive
Directive allowing sick leave to be used as safe days for
state employees under his purview
Source: Georgia Family Care Act, SB 242. http://www.legis.ga.gov/Legislation/en-US/display/2015_16/45011; NC Executive Action on Safe Days, October 2019.Let’s not return to normal: It’s time to achieve racial health equity in birth outcomes Keisha L. Bentley-Edwards, PhD Duke University Samuel Dubois Cook Center on Social Equity General Internal Medicine Division
Commonality
What is Normal?
Socio-
historical Statistics
ContextWhat is normal, ultimately determines what
is…
Acceptable Actionable Valid
42What’s commonly accepted
as normal…
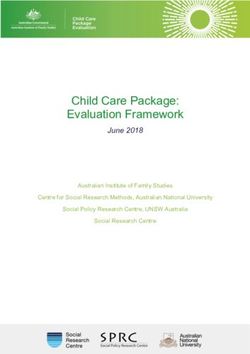
Perinatal Health DisparitiesInfant Mortality Rates (per 1,000)
6.2
OTHER
7.6
NATIVE AMERICAN OR ALASKAN NATIVE
7.6
13.4
BLACK (NH)
Infant Mortality
10.8
6
HISPANIC OR LATINO
Rates
5
ASIAN
4.1
5
WHITE (NH)
5.1
7.2
TOTAL
6
0 2 4 6 8 10 12 14 16
NC Infant Mortality Rates National Infant Mortality
2013, US Rates; 2016 NC RatesBeing Black is Not a Risk Factor If we understand that race is a social construct, then we can point to social contexts, and uneven risks within social contexts as causes for health disparities. Scott, Robbins & Bentley-Edwards, 4 2021 5
African Americans are over-represented in service
jobs such as:
• Public service
• Food service
• Manufacturing
• Food processing
• postal service
• package delivery
• Custodial
• healthcare support, and
Presenteeism • gig economy (e.g., ride-share and grocery delivery) jobs
(Bureau of Labor Statistics, 2018)
Jobs dominated by women are over-represented in
Presenteeism: (education, care & welfare sectors)
• Nursing
• midwifery professionals
• nursing home aides
• school teachers
• preschool/primary
(Aronsson, G., Gustafsson, K., & Dallner,educationalists.
M, 2000)Relationship between systemic inequalities &
infant mortality
• B/W disparities
• For every 1% increase in
unemployment disparities, resulted in
5% increase in Black infant mortality
Systemic (Wallace, Crear-Perry, Richardson, Tarver, & Theall, 2017)
Inequalities
• 76% of Black Mothers work, yet consistently earn
less than White male and female counterparts
• 18% of mothers with small children are low-wage
workers
https://www.americanprogress.org/issues/women/news/2018/11/02/460353/eff
orts-combat-pregnancy-discrimination/Key Policy Recommendations
Paid Perinatal Practitioner Fund Enforce
Family Care Training Programs Discrimination
Leave & Service Laws
48Thank You
Keisha.Bentley.Edwards@duke.edu
www.DrBentleyEdwards.com
@Keisha_BentleyPaid Family and Medical Leave
Only 17% of American workers - and 5% of low wage workers - have
access to paid leave. In NC, only 12% have access to paid leave.
Fewer than 40% of employees have access to personal medical leave
through their employer.
Source: National Partnership for Women & Families. (2018). Paid Leave. Retrieved from: http://www.nationalpartnership.org/our- work/workplace/paid-leave.html; Gassman-Pines, Anna and Elizabeth Ananat, 2019. “Paid Family Leave in North Carolina: An Analyis of Costs and
Benefits.” Duke Center for Child and Family Policy. Retrieved 6 August 2019 from: https://duke.app.box.com/s/9wti16byhdyyz6k99ri2yib3ttlprgl8Disparities in Access
Only 25% of Latino workers and 43% of Black workers reported having any access to paid or partially paid
leave compared with 50% of white workers. This has serious implications for racial health disparities,
particularly as they relate to infant mortality, premature birth, and low birth weight.
Source: The Council of Economic Advisors (2014) The Economics of Paid and Unpaid Leave. https://obamawhitehouse.archives.gov/sites/default/files/docs/leave_report_final.pdfImproved outcomes for children
● Provides critical time for bonding; building nurturing,
responsive relationships; and learning how to parent
● Increases accessing of adequate prenatal care
● Decreases infant mortality and premature birth
● Decreases child abuse
● Decreases maternal postpartum depression
● Increases the ability to secure safe, high-quality childcare
● Increases the likelihood of well-child checks and
vaccinations
● Increases breastfeeding initiation and duration
● Allows for early detection of developmental delays
● Increases positive father involvement
● Decreases intimate partner violence
● Decreases re-hospitalization for both mothers and infants,
● Good for businesses and the overall economy [47]
Source: See endnote.Paid Family & Medical
Leave: What’s at Stake
• 1 in 4 mothers go back to work within 2 weeks of
birth unable to establish breastfeeding, continue
bonding, and heal from birth.
• Most licensed childcares cannot take babies younger
than 6 weeks and NC’s shortage of licensed childcare
options and long childcare subsidy waiting lists can
put infants in very vulnerable situations in their first
6 weeks.
• Lack of paid family leave further widens the pay gap
and can drive families into poverty, creating stress.
Paid family leave provides economic security.
Source: US Bureau of Labor Statistics. Retrieved August 7, 2016 from :http://www.bls.gov/ncs/ebs/benefits/2015/ownership/civilian/table32a.pdf;Lerner,
Sharon Lerner. “The Real War on Families,” In These Times, August 18, 2015. Retrieved August 7, 2016 from: http://inthesetimes.com/article/18151/the-
real-war-on-families; Jessen-Howard, S., Malik, R., Workman, S., & Hamm, K. (2018). Understanding Infant and Toddler Child Care Deserts. Center for
American ProgressHow does paid leave decrease child maltreatment? Increases protective factors by providing concrete support Prevents Adverse Childhood Experiences by strengthening economic support for family Increases economic stability & family income Increases maternal employment Improves caregivers’ ability to meet children’s basic needs.
How does paid leave decrease
child maltreatment?
Centers for Disease Control recommends paid leave as a
strategy for reducing child maltreatment [49]
2015 Study in the State of California found:
Significant decrease in abusive head trauma admissions
for children under age 2 when their parents had paid
family leave, compared to seven states that did not have
paid family leave policies [50]
Source: Klevens, J., Luo, F., Xu, L., & Latzman, N. E. (2016). Paid Family Leave’s Impact on Hospital Admissions for Pediatric Abusive Head Trauma. Injury Prevention.; Berger, L. M., Hill, J., & Waldfogel, J. (2005). Maternity Leave, Early Maternal Employment and Child Health and
Development in the U.S. The Economic Journal, 115: F29-F27.; Srathearn, L., Mamun, A. A., Najmun, J. M., & O’Callaghan, M. J. (2009). Does Breastfeeding Protect Against Substantiated Abuse and Neglect? A 15-year cohort study. Pediatrics, 123: 483-493.; Chatterji, P., & Markowitz, S.
(2005). Does the Length of Maternity Leave Affect Maternal Health? Southern Economic Journal, 72(1): 16-41.; Klevens, J., Luo, F., Xu, L., & Latzman, N. E. (2016). Paid Family Leave’s Impact on Hospital Admissions for Pediatric Abusive Head Trauma. Injury Prevention.Duke Center for Child & Family Policy
Study: Snapshot of key findings
Paid family and medical leave insurance:
• Increases labor force participation and employee
retention.
• Improves the health of mothers and infants.
• Viewed by businesses as having had a positive or
noticeable effect.
• Potential cost savings from estimated impacts outweigh
administrative costs.
• Decreases infant mortality and nursing home usage.
Source: Gassman-Pines, Anna and Elizabeth Ananat, 2019. “Paid Family Leave in North Carolina: An Analyis of Costs and Benefits.” Duke Center for Child and Family Policy. Retrieved 6 August 2019 from: https://duke.app.box.com/s/9wti16byhdyyz6k99ri2yib3ttlprgl8Projected that a program offering twelve weeks leave with 80% wage
replacement would [51]:
save 26 infant lives in North Carolina each year – a 3 percent drop in
our state’s currently abysmal infant mortality rate!
keep 205 individuals out of nursing home care each year, cutting
costs by between $16.7 million and $18.6 million
Duke Center reduce the number of individuals needing public assistance through
the Temporary Assistance for Needy Families (TANF) program by
for Child & 956, saving $451,232 to $780,096 in North Carolina’s TANF costs
Family Policy annually;
provide meaningful support for families addressing a loved one’s
Study opioid or other substance abuse addiction.
Source: Gassman-Pines, Anna and Elizabeth Ananat, 2019. “Paid Family Leave in North Carolina: An Analyis of Costs and Benefits.” Duke Center for Child and Family Policy. Retrieved 6 August 2019 from: https://duke.app.box.com/s/9wti16byhdyyz6k99ri2yib3ttlprgl8 Paid leave portion of the Families First Coronavirus Response Act provided up to
10 weeks of emergency, expanded paid family leave care for a child whose
school or place of care is closed.
Challenges with it are exemptions, time span, sunset
Bureau of Labor and Statistics September jobs report found four times more
COVID-19 and women than men left employment. Specifically, 865,000 women dropped out of
the U.S. workforce, including 324,000 Latinas and 58,000 Black women, while
paid leave 216,000 men did the same.
Bipartisan Policy Center survey on motivating factors found:
Women with children are much more likely to have left work. Among
women with children under 2 years old, 42% have left work during the
coronavirus pandemic.
Two in five (41%) adults either are women who have left work or know a
woman that has left the workforce during the pandemic.
Women are twice as likely as men to say they left work for caregiving
responsibilities due to childcare provider or school closures
Impacts on children: increased poverty and family economic insecurity, increased
food and housing insecurity, loss of employer-sponsored health insurance,
potentially unsafe childcare situations
North Carolina had experienced declining women’s workforce participation prior
to the pandemic.
Source: BLS Employment Situation Summary 2020, October 2, 2020, https://www.bls.gov/news.release/archives/empsit_10022020.htm; BLS, September 2020 Employment Situation Summary, Table B-1: Employees on nonfarm payrolls by industry sector and selected industry
detail, available at https://www.bls.gov/news.release/empsit.t17.htm; “New Survey: Facing Caregiving Challenges, Women Leaving the Workforce at Unprecedented Rates,” Bipartisan Policy Center, October 28, 2020, https://bipartisanpolicy.org/blog/facing-caregiving-challenges/;
“Four Times More Women Than Men Dropped Out of the Labor Force in September,” National Women’s Law Center, Claire Ewing-Nelson, October 2020.; https://nwlc.org/wp-content/uploads/2020/10/september-jobs-fs1.pdfFamily Medical Leave Act (FMLA) passed in 1993 providing unpaid,
job-protected leave to workers meeting certain conditions
Federal
Movement on Federal Employee Paid Leave Act (FEPLA) passed in 2019 and
went into effect October 1,2020, provides 12 weeks of paid parental leave for
Paid Leave federal employees who would be eligible for the same amount of unpaid leave
under the Family and Medical Leave (FMLA) Act.
Families First Coronavirus Response Act (FFCRA) passed April
1, 2020 provides emergency paid sick leave and emergency paid family leave:
• current provisions exclude more than 106 million workers nationally and more
than 3.1 million NC workers, well more than half of our state’s workforce
• sunsets December 31, 2020 Paid Family Medical Leave Insurance programs exist in 9 states
and Washington, DC. Five states have implemented paid FMLI
programs(California, New Jersey, New York, Rhode Island, and
Washington State) with new programs coming online in
Massachusetts, Connecticut, DC, Oregon, and Colorado.
The ability to take PAID leave is key. Nearly half of those who were
Movement in FMLA-eligible and needed leave but didn’t take it cited lack of pay
as the reason.
the States on
Paid Leave
Source: “State Paid Family and Medical Leave Insurance Laws,” August 2019. National Partnership for Women and Families. https://www.nationalpartnership.org/our-work/resources/economic-justice/paid-leave/state-paid-family-leave-laws.pdf; Pew Research Center
(2017) Americans Widely Support Paid Family and Medical Leave But Differ Over Specific Policies.Growing North Carolina Support 20 local governments have approved paid parental or family leave policies for local government employees ranging from Charlotte and New Hanover County to Rolesville and Person County Executive Order 95 provided paid parental leave to state employees under Gov. Cooper’s purview, now also voluntarily covering Office of Administrative Hearings, Department of Agriculture and Consumer Services, Office of the Commissioner of Banks, Office of the Secretary of State, Office of the State Auditor, Office of the State Controller, Department of Public Instruction, Department of Justice and The Administrative Office of the Courts for a total of 59,000 employees UNC Board of Governors extended paid parental leave to 33,000 employees Paid leave is included in the NC Perinatal Health Strategic Plan, NC Perinatal System of Care Task Force recommendations, the Early Childhood Action Plan, the Pathways to Grade-Level Reading, the Essentials for Childhood Initiative, and the NC Council for Women recommendations as well as the agendas of the NC Families Care coalition and the Think Babies Alliance. Source: Executive Order 95: Providing Paid Parental Leave to Eligible State Employees https://governor.nc.gov/documents/executive-order-no-95-providing-paid-parental-leave-eligible-state-employees; “Paid Parental Leave Benefit Approved by UNC Board of Governors,” https://hr.unc.edu/paid-parental-leave-benefit-approved-by-board-of-governors/
Research on companies and states who’ve implemented paid
leave family and medical leave programs found paid leave
Impact on policies:
business
• Improve worker retention, which saves employers money
through reduced turnover costs
• Increase worker productivity
• Improve employee loyalty and morale
• Allow smaller businesses to compete with larger business for
talent
• Heightens American competitiveness in the global economy
• Can inspire entrepreneurship when small business start ups
can opt in
• Put dollars back into the local economy
• Reduces likelihood an employee will leave a job and require
public benefitsResearch on businesses in states who have
implemented these policies found:
• In RI, NY, and NJ, 61%, 64%, and 66%
(respectively) of employers are
supportive or very supportive of state
paid family and medical leave laws – and
this includes small employers.
Impact on
business • NY attitudes did not change significantly
after law came into effect – 63% were
supportive or very supportive in 2018 as
compared to 66% in 2016 and 2017.
• In California, approximately 90 percent
of firms surveyed said the law had either
a positive effect or no effect on
productivity, profit, morale, and costs.
Source: Leaves that Pay, Applebaum https://cepr.net/documents/publications/paid-family-leave-1-2011.pdf; The Business Impacts of Paid Leave: Insights from a Financial Analysis of Businesses Offering Paid Leave, Panorama and the American Sustainable Business
Council https://www.asbcouncil.org/sites/main/files/file-attachments/panorama_report_-_business_impacts_of_paid_leave.pdfs; Main Street Alliance 2018 report -https://d3n8a8pro7vhmx.cloudfront.net/mainstreetalliance/pages/716/attachments/original/1518636864/MSA_PFML_Report_-
_Phase_1_v3.pdf?1518636864Request to the Child Fatality Task Force Endorse passage of a bill creating a paid family and medical leave insurance program
Thank You!
Questions?
Contact:
Beth Messersmith, Senior NC Campaign Director
MomsRising/ MamásConPoder
Beth@momsrising.org, 919-323-6179Endnote for Role of Paid Sick Days in Slowing COVID-19 Spread: Pichler, S, Wen K, Ziebarth, NR. COVID-19 emergency sick leave has helped flatten the curve in the United Sates. Health Aff, 2020, Oct 15., https://doi.org/10.1377/hlthaff.2020.00863 DeRigne L, Stoddard-Dare P, Quinn L. Workers without paid sick leave less likely to take time off for illness or injury compared to those with paid sick leave. Health Aff (Millwood). 2016;35(3):520–7. DeRigne L, Dare PS, Collins C, Quinn LM, Fuller K. Working US adults without paid sick leave report more worries about finances. J Soc Serv Res. 2019;45(4):570–81. Gilleskie DB. A dynamic stochastic model of medical care use and work absence. Econometrica. 1998;66(1):1–46.; Piper K, Youk A, James AE, Kumar S. Paid sick days and stay-at-home behavior for influenza. PLoS One. 2017 Feb2;12(2):e0170698 Rossin-Slater M, Ruhm CJ, Waldfogel J. The effects of California’s paid family leave program on mothers’ leave-taking and subsequent labor market outcomes. J Policy Anal Manage. 2013;32(2):224–45.; Callison K, Pesko MF. The effect of paid sick leave mandates on coverage, work absences, and presenteeism. J Hum Resour. Forthcoming 2020. Jacobs E. Evidence on the benefits of expanded access to family and medical leave. Statement of Elisabeth Jacobs, Senior Fellow, Urban Institute before the Subcommittee on Workforce Protections, Committee on Education and Labor, United States House of Representatives [Internet]. Washington (DC): Urban Institute; 2020 [cited 2020 May 14]. Available from: https://www.urban.org/sites/default/files/publication/101705/evidence_on_the_benefits_of_expanded_access_to_family_and_medical_leave_15.pdf Susser P, Ziebarth NR. Profiling the US sick leave landscape: presenteeism among females. Health Serv Res. 2016;51(6):2305–17.; Pichler S, Ziebarth NR. The pros and cons of sick pay schemes: Testing for contagious presenteeism and noncontagious absenteeism behavior. J Public Econ. 2017;156:14–33. Pichler S, Wen K, Ziebarth NR. Positive health externalities of mandating paid sick leave. J Policy Anal Manage; forthcoming.
Endnote for Improved Outcomes for Children slide: Heymann, Jody, Amy Raub, and Alison Earle. “Creating and Using New Data Sources to Analyze the Relationship Between Social Policy and Global Health: The Case of Maternal Leave.” Public Health Rep. 2011; 126(Suppl 3): 127–134. Retrieved August 7, 2016 from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC3150137/ Ruhm, Christopher J. “Parental leave and child health.” Journal of Health Economics, November 2000;19:931–960. Tanaka, Sakiko. “Parental leave and child health across OECD countries.” Economic Journal, January 2005;115:F7–F28. Burtle, Adam and Stephen Bezruchka. “Population Health and Paid Parental Leave: What the United States Can Learn from Two Decades of Research.” Department of Health Services, School of Public Health, University of Washington, June 2016. Retrieved August 7, 2016 from http://www.ncbi.nlm.nih.gov/pmc/articles/PMC4934583/#B8-healthcare-04-00030 Winegarden, C.R. and P.M. Bracy. “Demographic consequences of maternal-leave programs in industrial countries: Evidence from fixed-effects models.” Southern Economic Journal, 1995;61:1020–1035. Nandi, Arijit, Mohammad Hajizadeh, Sam Harper, Alissa Koski, Erin C. Strumpf, and Jody Heymann. “Increased Duration of Paid Maternity Leave Lowers Infant Mortality in Low- and Middle-Income Countries: A Quasi-Experimental Study.” PLoS Medicine, 2016;13:30. Gassman-Pines, Anna and Elizabeth Ananat, 2019. “Paid Family Leave in North Carolina: An Analyis of Costs and Benefits.” Duke Center for Child and Family Policy. Retrieved 6 August 2019 from: https://duke.app.box.com/s/9wti16byhdyyz6k99ri2yib3ttlprgl8 Tanaka, Sakiko. “Parental leave and child health across OECD countries.” Economic Journal, January 2005;115:F7–F28. Ruhm, Christopher J. “Parental leave and child health.” Journal of Health Economics, November 2000;19:931–960. Kamerman, Sheila B. “Parental Leave Policies: The Impact on Child Well- Being.” In Peter Moss and Margaret O’Brien, eds., International Review of Leave Policies and Related Research 2006, 16–21. London, UK: Department of Trade and Industry, 2006. Retrieved October 9, 2013 from www.berr.gov.uk. Baker, M. and K. Milligan, “Maternal employment, breastfeeding, and health: Evidence from maternity leave mandates.” Journal of Health Economics, 2008;27:871–887. Berger, Lawrence M., Jennifer Hill, and Jane Waldfogel. 2005. “Maternity Leave, Early Maternal Employment, and Child Health and Development in the U.S.” The Economic Journal 115 (February): F29-F47. Chuang, Chao-Hua, Pei-Jen Chang, Yi-Chun Chen, Wu-Shiun Hsieh, Baai-Shyun Hurng, Shio-Jean Jin, and Pau-Chung Chen. 2010. “Maternal return to work and breastfeeding: A population-based cohort study.” International Journal of Nursing Studies 47: 467-474. Lindberg, Laura. 1996. “Women’s decisions about breastfeeding and maternal employment.” Journal of Marriage and the Family 58 (1): pp. 239–51. Staehelin, Katharina, Paola Coda Bertea and Elisabeth Zemp Stutz. 2007. “Length of maternity leave and health of mother and child – a review.” International Journal of Public Health, 52: 202-20 Guendelman, Sylvia, Jessica L. Kosa, Michelle Pearl, Steve Graham, Julia Goodman, and Martin Kharrazi. 2009. “Juggling work and breastfeeding: effects of maternity leave and occupational effects of maternity leave and occupational characteristics. Pediatrics 123(1): e38-e46. Hawkins, Summer S., Lucy J. Griffiths, Carol Dezateux, and Catherine Law. 2007. “The impact of maternal employment on breastfeeding duration in the UK Millennium Cohort Study.” Public Health Nutrition 10(9): 891-896. Visness, Cynthia M., and Kathy I. Kennedy. 1997. “Maternal employment and breastfeeding: findings from the 1988 National Maternal and Infant Health Survey.” 87(6): 945-950. Appelbaum, Eileen and Ruth Milkman. 2011. Leaves That Pay: Employer and Worker Experiences with Paid Family Leave in California. Washington DC: Center for Economic and Policy Research. (accessed January 23, 2014). Tanaka, Sakiko. “Parental leave and child health across OECD countries,” Economic Journal, January 2005;115:F7–F28.; Stearns, J. “The effects of paid maternity leave: Evidence from Temporary Disability Insurance,” Journal of Health Economics. J. Health Econ. 2015;43:85– 102.
Endnote for Improved Outcomes for Children slide: Chen, Feng. 2020. “The Unintended Effects of California’s Paid Family Leave Program on Children's Birth Outcomes,” working paper. Van Niel, Maureen Sayres MD; Bhatia, Richa MD; Riano, Nicholas S. MAS; de Faria, Ludmila MD; Catapano-Friedman, Lisa MD; Ravven, Simha MD; Weissman, Barbara MD; Nzodom, Carine MD; Alexander, Amy MD; Budde, Kristin MD, MPH; Mangurian, Christina MD, MAS. 2020 "The Impact of Paid Maternity Leave on the Mental and Physical Health of Mothers and Children: A Review of the Literature and Policy Implications,"Harvard Review of Psychiatry: 3/4 2020 - Volume 28 - Issue 2 - p 113-126.
• Endorse passage of a kin care and safe days
bill that would guarantee all North Carolina
Committee workers the right to use their sick days
discussion and (whether paid or job-protected unpaid) to
determination care for a sick loved one, seek preventative
addressing carry- care, or deal with the physical, mental, or
over items Paid legal impacts of domestic violence, sexual
Family Leave assault, or stalking.
Insurance and Kin
Care and Safe Days • Endorse legislation addressing paid family
Leave for 2021 leave insurance in North Carolina.NC Department of Health and Human Services
Overview of Doula Landscape
Training, Scope of Practice and
Legislation
Tara Owens Shuler, M.Ed., LCCE, CD(DONA)
NC Division of Public Health
Women’s & Children’s Health Section
Women’s Health Branch
Perinatal Health Unit Manager
70Presentation Points
• Definition of a Doula
• Birth Outcomes with Doula Support
• Training Requirements
• Scope of Practice
• NC Doula Landscape
• States with Doula Legislation
• Doulas and COVID-19
71A Doula is….
• A trained non-clinical person who provides
• continuous physical, emotional and informational
support to a birthing person and their support
person.
• Support before, during and shortly after childbirth
to help her achieve the healthiest, most satisfying
experience possible.
72Doulas Support Encompasses
• Physical Support
• Positions for comfort and labor progression
• Comforting touch/counterpressure
• Emotional Support
• Reassurance and encouragement
• Assist in creating a relaxing and calm birth space
• Partner Support
• Assist partners in asking questions
• Giving tips for partner support
73Birth Outcomes with a Doula
• 2017 Cochrane Review
• 26 studies across 17 countries, involving > 15,000
women
• Findings:
• increased spontaneous vaginal birth,
• shorter duration of labor,
• decreased cesarean births,
• decreased instrumental vaginal birth,
• decreased use of any analgesia,
• decreased use of regional analgesia (epidural), and
• decreased negative feelings about childbirth experiences.
https://www.cochrane.org/CD003766/PREG_continuous-support-women-during-childbirth
74Support for Doula Services
• American College of Obstetrics and Gynecology (ACOG)
• Acknowledge the potential benefits of continuous labor
support
• Associated with improved maternal outcomes
• March of Dimes
• Statement to support increased access to doula care to
improve birth outcomes
• Advocates for payers to support reimbursement for services
https://www.marchofdimes.org/materials/Doulas%20and%20birth%20outcomes%20position%20statement%20final%20January%2030%20PM.pdf
https://www.acog.org/clinical/clinical-guidance/committee-opinion/articles/2019/02/approaches-to-limit-intervention-during-labor-and-birth
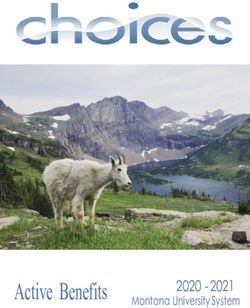
75Average Doula Training Requirements
National Black Doula Association
76Scope of Practice
• Accompanying the birthing person in labor,
• Providing emotional and physical support,
• Suggesting comfort measures,
• Providing support and suggestions to the partner,
• Explaining and discussing practices and procedures,
• Assisting their client in acquiring the knowledge
necessary to make informed decisions about their own
care, and
• Advising their client to check with their prenatal
provider if questions outside of their scope of practice.
77Outside of Scope of Practice
• Does not perform any clinical or medical tasks, such
as:
− taking blood pressure or temperature,
− fetal heart tone checks,
− vaginal examinations or
− postpartum clinical care.
• Doulas do not diagnose or treat in any modality.
78Doula is a Patient Advocate
• Advocates for the client's wishes as expressed in her birth
plan, in prenatal conversations, and intrapartum discussion.
• Encourages their client to ask questions of the care provider
and to express their preferences and concerns.
• Advocacy does not include speaking on behalf of the client
or making decisions for the client.
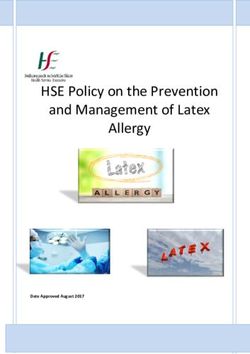
79Doula Distribution Across NC
Source: Chama Woydak, 7/25/18; Map created by Joan Colburn, MLIS MAHEC Library and Knowledge Services
8/16/2018
80No Statewide Organizational Oversight
• Doulas practice under a Code of Ethics set by
their respective certifying organization.
• No oversight body for doulas.
• No laws or regulations set forth for doulas in NC.
81Range of Doula Groups/Programs Across NC
• Volunteer programs through health care systems
• Community based volunteer programs
• Local health department contracts with local doulas
• Grant funded and/or agency funded doulas
• Doula program through health care systems
funded by patients
• Private doula businesses
82States with 3rd Party Reimbursement through Medicaid
State Summary
Oregon (HB3650) Doulas enroll through one of Oregon’s 15 Care Coordinated Organizations;
complete Traditional Health Worker Certification, register to get a NPI and enroll
2018 as Oregon Medicaid provider
Covers 2 prenatal and 2 postpartum visits, as well as continuous labor and birth
support. Medicaid reimbursement rate is $350 for this package
Minnesota Minnesota Health Care Programs (MHCP) covers doula services provided by
certified doulas for fee-for-service (FFS) members.
2013 Doula works under physician, CNM or NP.
Covered services include childbirth education and support services.
New Jersey (S1786) Provides Medicaid coverage for doulas, State plan amendment to cover birth
doulas as non licensed providers starting Jan 1, 2021
May 2019 Up to 8 home visits and continuous labor support, reimbursement rate $800
Indiana (SB416) Medicaid coverage for doula services. Provides that Medicaid pregnancy services
may include reimbursement for doula services.
*July 2019
Legislation did not include any funding.
https://www.mhtf.org/2020/01/08/expanding-access-to-doula-care/
83You can also read