"MEDICAL MARIJUANA": WHAT IS THE THERAPEUTIC VALUE? - John F. Kelly MGH Psychiatry Grand Rounds
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

“MEDICAL MARIJUANA”: WHAT IS THE THERAPEUTIC VALUE? John F. Kelly MGH Psychiatry Grand Rounds September 12, 2013

Outline • For what conditions might MJ/THC be beneficial? • What are the current THC-based treatment options? • What do we know from research how effective current THC-based and smoked MJ options are for commonly targeted medical conditions? • Anti-nausea(cancer/AIDS)/appetite (cancer) • Spasticity (multiple sclerosis) • Pain (neuropathy) • What are some of the risks associated with (smoked) “medical marijuana”? • What happens to MJ use rates in states that have implemented medical marijuana laws?

For which conditions might marijuana/THC
have a therapeutic benefit?
Up to 259 conditions including:
• Alzheimer’s disease • Glaucoma
• Anorexia • Migraines
• HIV/AIDS • Multiple Sclerosis
• Arthritis • Nausea
• Cachexia • Pain
• Cancer • Spasticity
• Crohn’s Disease • Wasting Syndrome
• Epilepsy
ProCon.org: http://medicalmarijuana.procon.org/view.resource.php?resourceID=000884
THC Administration & FDA Approved THC-
based medications
Approved
Compound Administration FDA Status Purposes
Locations
Dronabinol Oral capsule FDA-approved USA, Nausea & vomiting related
(Marinol) (1985) Germany to cancer chemotherapy
and wasting associated
with AIDS
Nabilone Oral capsule FDA-approved USA, Nausea & vomiting related
(Cesamet) (1985) Canada, to cancer chemotherapy
*Marketed in the UK, Mexico
US in 2006
Nabiximols Oromucosal Almost FDA- Canada, Multiple sclerosis
(Sativex) spray approved; UK, other spasticity, cancer pain,
late-stage European neuropathic pain
clinical trials countries
Marijuana Site Reclamation and Restoration Cost Analysis.” U.S. Department of Interior, National Park Service. December 9,
2010 (unpublished data). http://www.whitehouse.gov/ondcp/frequently-asked-questions-and-facts-about-marijuana#difference

Controlled studies evaluating the therapeutic effect of
THC by administration type
30
25
Number of studies
20
15
Smoked
10
Oral
5
Other (Oromucosal/Sublingual
0 Spray, IM, IV, Eye Drops)
Ben Amar, M. (2006). Cannabinoids in medicine: A review of their therapeutic potential. Journal of ethnopharmacology, 105(1), 1-
25.
Anti-nausea/emetic and appetite effects (Oral THC in cancer patients)

Anti-emetic effect
of oral THC vs.
standard treatment
• Sample: 73 patients with
neoplasms and
inadequately controlled
nausea and vomiting
• Design: Randomized,
double-blind, crossover
trial
• Intervention: Oral THC
vs. prochlorperazine
before and after
chemotherapy
• Follow-up: 3 randomly
assigned one-day courses
• Outcomes: Patient
preference in ameliorating
nausea & vomiting
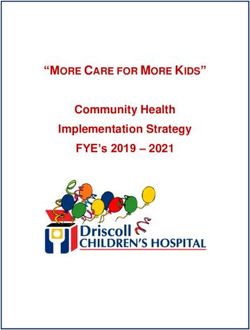
Effectiveness of THC
compared to Patient Preference for Anti-Emetic
prochlorperazine for Agent
treating nausea and
25 p=0.005
vomiting
THC
Prochlorperazine
20
Of the 25 who
No Preference
Number of patients
expressed
preference, 20
preferred THC to 15
prochlorperazin;
(degree of
preference for 10
either antiemetic
not dependent
on class of
emetic activity 5
related to
patient’s
chemotherapy); 0
increased Total Class A Class B Class C
appetite
Emetic Activity of Chemotherapeutic Agent
Sallan, S. E., Cronin, C., Zelen, M., & Zinberg, N. E. (1980). Antiemetics in patients receiving chemotherapy for cancer: a
randomized comparison of delta-9-tetrahydrocannabinol and prochlorperazine. New England Journal of Medicine, 302(3), 135-138.
Appetite & Quality of
Life:
Efficacy of oral THC
vs. placebo
• Sample: 243 advanced
cancer patients
experiencing involuntary,
unexplained weight loss
• Design: Randomized,
placebo-controlled trial
• Intervention: Compared
3 conditions: Oral
cannabis extract (2.5mg
THC & 1mg CBD; similar
to nabiximols [Sativex])
vs. THC (2.5mg; similar
to dronabinol [Marinol])
vs. placebo
• Follow-up: 6-weeks
• Outcomes: Appetite
stimulation, Quality of LifeEfficacy of orally-administered cannabis extract for
appetite stimulation and quality of life for patients with
cancer
Strasser, F., Luftner, D., Possinger, K., Ernst, G., Ruhstaller, T., Meissner, W., ... & Cerny, T. (2006). Comparison of orally
administered cannabis extract and delta-9-tetrahydrocannabinol in treating patients with cancer-related anorexia-cachexia
syndrome: a multicenter, phase III, randomized, double-blind, placebo-controlled clinical trial from the Cannabis-In-Cachexia-
Study-Group.Journal of Clinical Oncology, 24(21), 3394-3400.• So, cancer pts may prefer THC-based medicine for anti- nausea, may stimulate appetite • Effects may be moderated by cancer stage and may not stimulate appetite among more advance cancer patients
Spasticity (oral spray THC in MS patients)
Safety and
efficacy of
nabiximols
• 3 randomized, placebo-
controlled, double-blind,
parallel-group studies
• n=666 (363 randomized
to nabiximols) patients
with MS and spasticity
• Outcome: spasticity
• Adverse events were
recorded
Wade, D. T., Collin, C., Stott, C., & Duncombe, P. (2010). Meta-analysis of the efficacy and safety of Sativex (nabiximols), on
spasticity in people with multiple sclerosis. Multiple Sclerosis, 16(6), 707-714.MS Spasticity:
Efficacy of
THC/CBD spray vs.
placebo
• Sample: 572 MS patients
with spasticity
• Design: Randomized,
placebo-controlled trial
• Intervention: Nabiximols
(2.7 mg THC + 2.5 mg
CBD) oromucosal spray
vs. placebo
• Follow-up: 12 weeks
• Outcome: Change in
spasticity from baselineEfficacy of oral spray nabiximols for MS patients with
spasticity
Novotna, A., Mares, J., Ratcliffe, S., Novakova, I., Vachova, M., Zapletalova, O., ... & Davies, P. (2011). A randomized,
double‐blind, placebo‐controlled, parallel‐group, enriched‐design study of nabiximols*(Sativex®), as add‐on therapy, in subjects
with refractory spasticity caused by multiple sclerosis. European Journal of Neurology, 18(9), 1122-1131.Spasticity (Smoked THC in MS patients)
MS Spasticity:
Efficacy of smoked
THC vs. placebo
• Sample: 30 MS patients
with spasticity
• Design: Randomized,
double-blind, placebo-
controlled crossover trial
• Intervention: 800mg 4%
THC cigarettes vs placebo
• Follow-up: 6 assessments
• Outcome: Change in
spasticityEfficacy of smoked THC for MS patients
with spasticity
Corey-Bloom, J., Wolfson, T., Gamst, A., Jin, S., Marcotte, T. D., Bentley, H., & Gouaux, B. (2012). Smoked cannabis for
spasticity in multiple sclerosis: a randomized, placebo-controlled trial. Canadian Medical Association Journal, 184(10), 1143-1150.Issues with blinding in medical marijuana RCTs
More than 50%
of studies are
considered at
high risk for
unblinding
The use of cannabis and rapidly acting cannabinoids pose considerable challenges
for blinding, as the psychoactive effects are expected to be quickly discernible to
study participants, particularly those who have been previous users of such products.
Lutge, E. E., Gray, A., & Siegfried, N. (2013). The medical use of cannabis for reducing morbidity and mortality in patients with
HIV/AIDS. status and date: New, published in, (4).Neuropathic Pain (Oral spray THC in diabetic patients)
Comparative effectiveness of pharmacological
treatments for pain
Nabixomols
(Sativex) least
effective for pain
reduction among
individuals with
diabetic peripheral
neuropathy
Snedecor, S. J., Sudharshan, L., Cappelleri, J. C., Sadosky, A., Mehta, S., & Botteman, M. (2013). Systematic Review and
Meta‐Analysis of Pharmacological Therapies for Painful Diabetic Peripheral Neuropathy. Pain Practice.Pain:
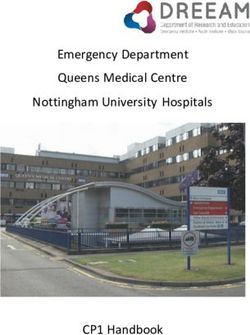
Efficacy of smoked
cannabis vs. placebo
• Sample: 23 adults with
neuropathic pain
• Design: Randomized,
placebo-controlled,
crossover trial
• Intervention: Four doses of
THC 0.0, 2.5, 6.0 or
9.4%THC administered
using a single-smoke
inhalation 3 times per day
• Follow-up: 8-weeks
• Outcome: Change in
average daily painEfficacy of smoked THC for chronic neuropathic pain
p = 0.023
8
7
6
Pain Score†
5
4
Average Daily Pain
Highest Daily Pain
3
Lowest Daily Pain
2
1
0
0.00% 2.50% 6.00% 9.40%
THC Potency
†Pain was scored on a scale from 0 (no pain) to 11 (worst possible pain)
Ware, M. A., Wang, T., Shapiro, S., Robinson, A., Ducruet, T., Huynh, T., ... & Collet, J. P. (2010). Smoked cannabis for chronic
neuropathic pain: a randomized controlled trial. Canadian Medical Association Journal, 182(14), E694-E701.Pain:
Efficacy of smoked
THC vs. placebo
• Sample: 55 patients with
HIV-associated sensory
neuropathy
• Design: Randomized,
double-blind, placebo-
controlled trial
• Intervention: 900 mg
3.56% THC cigarettes vs
placebo
• Follow-up: 3 weeks
• Outcome: Neuropathic
painEfficacy of THC for HIV-positive patients
with neuropathic pain
Significant benefit
in reducing pain
during active
treatment phase,
lasting up to 8
days after
stopping smoking
Abrams, D. I., Jay, C. A., Shade, S. B., Vizoso, H., Reda, H., Press, S., ... & Petersen, K. L. (2007). Cannabis in painful HIV-
associated sensory neuropathy A randomized placebo-controlled trial. Neurology, 68(7), 515-521.So, oral spray THC (Sativex) may help reduce spasticity in MS patients, but be unhelpful with chronic pain among diabetic pts with peripheral neuropathic pain Unclear whether smoked THC may help in this population Smoked THC may help reduce experience of chronic among certain clinical populations (e.g., HIV pts)
The controversy regarding medical marijuana 1. Health risks of smoked marijuana 2. Addictiveness of marijuana 3. Influence on youth drug use
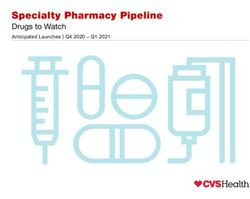
Health risks of FEV1/FVC ratio
Health risks of Cervix
smoked
Breast
marijuana
“There is very little
evidence that smoking Prostate
marijuana as a means of
Cancer Site
taking it represents a
significant health Melanoma
risk…there have been no Women
reported cases of lung Men
cancer or emphysema. I Lung
suspect that a day’s
breathing in any city with
poor air quality poses more Colorectal
of a threat than inhaling a
day’s dose – which for
many ailments is just a Tobacco-related
portion of a joint – of
marijuana.”
All sites
-- Lester Grinspoon, MD
Emeritus Professor of 0.0 0.5 1.0 1.5 2.0
Psychiatry RR of cancer incidence comparing MJ users to non-users
Harvard Medical School
Adjusting for sociodemographic factors, alcohol and tobacco use
Sidney, S., Quesenberry Jr, C. P., Friedman, G. D., & Tekawa, I. S. (1997). Marijuana use
and cancer incidence (California, United States). Cancer Causes & Control, 8(5), 722-728.40
% marijuana dependence (lifetime)
Addictiveness 35
of marijuana 30
25
“Adolescents, especially
troubled ones, and people
with psychiatric disorders 20
(including substance
abuse) appear more likely
than the general 15
population to become
dependent on marijuana… 10
Some controlled
substances that are
approved medications 5
produce dependence after
long-term use; this,
however, is a normal part 0
of patient management Ever users of Marijuana users Daily marijuana
and does not generally marijuana who start using in users
present undue risk to the their teens
patient”
Anthony, J.; Warner, L.A.; and Kessler, R.C. Comparative epidemiology of dependence on tobacco, alcohol, controlled
-- Institute of Medicine substances, and inhalants: Basic findings from the National Comorbidity Survey. Exp Clin Psychopharmacol 2:244–
268, 1994;
Hall, W.; and Degenhardt, L. Adverse health effects of non-medical cannabis use. Lancet 374:1383–1391, 2009;
Hall, W. The adverse health effects of cannabis use: What are they, and what are their implications for policy? Int J of
Drug Policy 20:458–466, 2009Health
(and societal) risks
of smoked
marijuana
20 drugs ranked by
overall harm along
16 criteria
Nutt, D. J., King, L. A., & Phillips, L. D. (2010). Drug harms in the UK: a multicriteria
decision analysis. The Lancet, 376(9752), 1558-1565.Influence on
youth drug use
“While it is not possible
with existing data to
determine conclusively
that state medical
marijuana laws caused
the documented declines
in adolescent marijuana
use, the overwhelming
downward trend strongly
suggests that the effect of
state medical marijuana
laws on teen marijuana
use has been either
neutral or positive,
discouraging youthful
experimentation with the
drug.”
-- Mitch Earlywine, SUNY
Albany;
Karen O’Keeffe, Marijuana
Policy Project
O’Keeffe & Earlywine (2011). Marijuana use by young people: The impact of state medical
marijuana laws. Marijuana Policy Project .Influence on
youth drug use
“By characterizing the use
of illegal drugs as quasi-
legal, state-sanctioned,
Saturday afternoon fun,
legalizers destabilize the
societal norm that drug
use is dangerous. They
undercut the goals of
stopping the initiation of
drug use to prevent
addiction.... Children
entering drug abuse
treatment routinely report
that they heard that 'pot is
medicine' and, therefore,
believed it to be good for
them.”
-- Andrea Barthwell
Former Deputy Director
White House Office of
National Drug Control
Policy (ONDCP)
Anderson, Hansen & Reesse (2012). Medical Marijuana laws and teen marijuana use.
University of Washington.
http://depts.washington.edu/phenom/docs/Anderson_Hansen_Rees_2012.pdf• THC confers therapeutic benefit
• FDA-approved medications addressing nausea in AIDS/cancer
• May not be as effective as other pharm. agents for chronic pain
• Some evidence of both oral THC-based meds and smoked MJ,
Conclusions relative to placebo, alleviating spasticity among MS patients
• Levels of THC and CBD (and other cannabinols) likely differ between
different batches of MJ used across studies, making generalizability
about potential benefit difficult; dosing regimen also differs/differs from
the way it may be smoked for medical reasons in the real world
• Lack of trials comparing smoked MJ to oral/spray THC for any ailment
• Thus, it is currently unclear whether the benefits of smoked MJ (net of
smoking-related risks) is greater than oral/other FDA-approved THC-
based medications, and for which specific medical conditions
• Physician recommendations for smoked MJ for any medical purpose
lacks clear systematic empirical basis
• Somewhat unclear also is the relationship between state medical MJ
implementation and its potential effect on changing
perceptions/attitudes and increasing MJ use, especially among
teens/young peopleYou can also read