MEDICAL IMAGING LANDSCAPE REPORT - WHANGANUI AND MIDCENTRAL DISTRICT HEALTH BOARDS - MidCentral District ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

NOVEMBER 18, 2013
MEDICAL IMAGING LANDSCAPE REPORT
WHANGANUI AND MIDCENTRAL DISTRICT HEALTH BOARDS
27 March 2014 Medical Imaging Landscape Report Page 1 of 91
Document Control
Title: Medical Imaging Landscape Report Status: FINAL
Subtitle: Whanganui and MidCentral District Health Boards Rev Number:
Key Words: Publish Date: 14/11/2013
File Name: Landscape Report (18Nov13) FINAL Save Date: 27/03/2014
3:46:00 p.m.
27 March 2014 Medical Imaging Landscape Report Page 2 of 91CONTENTS 1 Executive Summary ......................................................................................................................... 6 2 The Role of Medical Imaging in The Health System ........................................................................ 7 3 DHB Funding Philosophies ............................................................................................................ 10 4 Regional Demographic Profile ....................................................................................................... 12 4.1 Projections ............................................................................................................................ 13 4.2 Equity of Access .................................................................................................................... 14 5 Modality Descriptions and Observations ...................................................................................... 15 5.1 Where Services are Provided ................................................................................................ 15 5.2 Breast Imaging ...................................................................................................................... 16 5.2.1 Modality Description..................................................................................................... 16 5.2.2 Key Issues ...................................................................................................................... 17 5.2.3 Potential Opportunites.................................................................................................. 17 5.3 MRI ........................................................................................................................................ 19 5.3.1 Modality Description..................................................................................................... 19 5.3.2 Key Issues ...................................................................................................................... 20 5.3.3 Potential Opportunites.................................................................................................. 22 5.4 CT .......................................................................................................................................... 23 5.4.1 Modality Description..................................................................................................... 23 5.4.2 Key Issues ...................................................................................................................... 24 5.4.3 Potential Opportunites.................................................................................................. 25 5.5 Ultrasound............................................................................................................................. 26 5.5.1 Modality Description..................................................................................................... 26 5.5.2 Key Issues ...................................................................................................................... 28 5.5.3 Potential Opportunites.................................................................................................. 29 5.6 Digital Subtraction Angiography (DSA).................................................................................. 30 5.6.1 Modality Description..................................................................................................... 30 5.6.2 Key Issues ...................................................................................................................... 32 5.6.3 Potential Opportunites.................................................................................................. 32 5.7 General X-Ray ........................................................................................................................ 34 5.7.1 Modality Description..................................................................................................... 34 5.7.2 Key Issues ...................................................................................................................... 34 5.7.3 potential opportunites .................................................................................................. 35 5.8 Nuclear Medicine and PET/CT ............................................................................................... 36 5.8.1 Modality Description..................................................................................................... 36 5.8.2 Key Issues ...................................................................................................................... 37 5.8.3 Potential Opportunites.................................................................................................. 37 5.9 Bone Densitometry ............................................................................................................... 38 5.9.1 Modality Description..................................................................................................... 38 5.9.2 Key Issues ...................................................................................................................... 38 5.9.3 Potential Opportunites.................................................................................................. 38 5.10 Medical Photography ............................................................................................................ 40 5.10.1 Modality Description..................................................................................................... 40 5.10.2 Key Issues ...................................................................................................................... 40 5.10.3 Potential Opportunites.................................................................................................. 41 5.11 Radiology Information System (RIS) / Picture Archiving & Communication System (PACS) . 42 5.11.1 Description .................................................................................................................... 42 5.11.2 Key Issues ...................................................................................................................... 42 5.11.3 Potential Opportunites.................................................................................................. 43 27 March 2014 Medical Imaging Landscape Report Page 3 of 91
6 Workforce Descriptions and Observations ................................................................................... 44 6.1 Radiologists ........................................................................................................................... 45 6.1.1 Description .................................................................................................................... 45 6.1.2 Key Issues ...................................................................................................................... 45 6.1.3 Potential Opportunites.................................................................................................. 46 6.2 Medical Radiation Technologists........................................................................................... 47 6.2.1 Description .................................................................................................................... 47 6.2.2 Key Issues ...................................................................................................................... 47 6.2.3 Potential Opportunites.................................................................................................. 49 6.3 Nursing .................................................................................................................................. 50 6.3.1 Description .................................................................................................................... 50 6.3.2 Key Issues ...................................................................................................................... 50 6.3.3 Potential Opportunites.................................................................................................. 51 7 Indicative Financial Comparisons .................................................................................................. 52 8 Next Steps for the Development Plan ........................................................................................... 53 9 Appendices .................................................................................................................................... 54 9.1 Annual Plan Initiatives with a Medical Imaging Impact ........................................................ 54 9.2 Population Projections .......................................................................................................... 56 9.3 European or Other Population Projections ........................................................................... 58 9.4 Maori Population Projections ............................................................................................... 60 9.5 Asian Population Projections ................................................................................................ 62 9.6 Pacific Population Projections ............................................................................................... 62 9.7 Whanganui Access Equity ..................................................................................................... 63 9.8 Ministry of Health Funded PET CT Examinations .................................................................. 65 9.9 Imaging Services.................................................................................................................... 66 9.9.1 Hospital Based Services................................................................................................. 66 9.9.2 Patient Type – All Modalities......................................................................................... 69 9.9.3 Normal Hours Of Operation – All Modalities ................................................................ 71 9.9.4 Day Of Examination – All Modalities ............................................................................. 71 9.9.5 Hour Of Examination – Ct.............................................................................................. 73 9.9.6 Hour Of Examination – Us ............................................................................................. 76 9.9.7 Hour of examination – MRI ........................................................................................... 78 9.9.8 Out-Of-Hours Activity In Detail – Ct .............................................................................. 79 9.9.9 Out-Of-Hours Activity in Detail – Us ............................................................................. 80 9.9.10 Out-Of-Hours Activity in Detail – MRI ........................................................................... 81 9.9.11 DHB Provided Facilities ................................................................................................. 81 9.9.12 DHB Provided Current Equipment, Hours of Operation, Volumes and Staffing ........... 82 9.9.13 Private Provided Current Equipment, Hours of Operation, Volumes and Staffing ....... 88 27 March 2014 Medical Imaging Landscape Report Page 4 of 91
TABLES Table 1: Breast Imaging Future Developments .................................................................................... 18 Table 2: MRI Future Development ....................................................................................................... 22 Table 3: CT Future Development .......................................................................................................... 25 Table 4: Ultrasound Future Development ............................................................................................ 29 Table 5: Digital Subtraction Angiography (DSA) Future Development ................................................. 33 Table 6: General X-ray Future Development ........................................................................................ 35 Table 7: PET-CT Volumes ...................................................................................................................... 37 Table 8: Nuclear Medicine/PET-CT Future Developments ................................................................... 37 Table 9: Bone Densitometry Future Developments ............................................................................. 39 Table 10: RIS/PACS Future Developments ............................................................................................ 43 Table 11: Radiologist Future Developments ........................................................................................ 46 Table 12: MRT Future Developments ................................................................................................... 49 Table 13: Nursing Future Developments .............................................................................................. 51 Table 14: Services; DHB provided......................................................................................................... 87 Table 15: Privately provided services ................................................................................................... 91 FIGURES Figure 1: Location of Services............................................................................................................... 15 27 March 2014 Medical Imaging Landscape Report Page 5 of 91
1 EXECUTIVE SUMMARY
This is the second paper, in a series of three, to progress the 2012/13 Annual Plan centralAlliance
initiatives to review Medical Imaging services. The paper reflects work done to date with many
areas remaining work in progress. The next steps are to explore the key issues further, test current
assumptions and determine a final Plan to be endorsed by key stakeholders.
The final plan will define the need for imaging services for both DHB populations taking into
consideration not only current demand but also the inevitable impact of government targets and
strategies. It will identify opportunities to work differently as well as highlighting those areas to
consolidate, where it is important to strengthen rather than change current arrangements.
Opportunities for improvement include:
To provide better and faster services for referrers and patients
To ensure value for money from both current expenditure and future investment
To identify and fast track development opportunities
To think differently about and address historic problems
To contribute to future clinical strategies and facilities design
A focus on succession planning and workforce
To strengthen the public system as part of the centralAlliance and wider central region
Work on this plan runs in parallel with, and interfaces to, the Central Region Radiology project, the
Central Regional Information Services Plan (CRISP) and the Master Health Services Plan for
MidCentral DHB (MDHB).
In July 2013 a paper was presented to the Committees of both boards to provide a strategic context
for the presentation of more detailed papers in future meetings. That paper set the scene for the
project work underway to develop a plan for Medical Imaging Services. It outlined some key areas
of focus such as ultrasound access and the development of teleradiology services in Palmerston
North to address increasing out of hours demand for computed tomography (CT).
This paper outlines the landscape of service provision and access for both DHBs. The purpose of
this interim step, prior to a final plan, is to take the opportunity to more fully describe the current
state, and potential steps forward, and to seek feedback from the Committees on both these
aspects as they relate to future imaging services.
It is divided by modality area and identifies some potential opportunities for future development
shown at the end of each section. There are also separate sections, following the modality areas, to
describe the landscape for radiologists, MRTs and Nurses. The current operational performance of
both hospital departments is included and various comparisons between the two DHBs have been
completed.
The paper also highlights that further work is required to better understand and to gain agreement
on the clinical and strategic direction. Importantly further engagement with clinical staff is needed
to crystallise, and prioritise, the items before the final development plan is endorsed by the Project
Team. This paper will form the basis for these discussions in a series of clinical forums.
While a number of opportunities have been raised, there are issues for some work streams that will
be a priority in the next financial year and will take precedence for the immediate term. These are:
Breast Imaging Services for Whanganui
The model of service for CT in Palmerston North
An urgent focus on the model of service for ultrasound for both DHBs
Radiologist and MRT capacity and capability for both DHBs
A focus on equity of access for both DHBs
27 March 2014 Medical Imaging Landscape Report Page 6 of 912 THE ROLE OF MEDICAL IMAGING IN THE HEALTH SYSTEM
The current health environment is characterised by Health Targets and Standards of Practice,
increasing regionalisation and new Models of Care. These measures are the basis of better
outcomes for patients and are reflected in the DHB’s Annual Plan. A review of both DHBs’ Annual
Plans has shown that effective and efficient access to imaging is a shared necessity. This access is a
key enabler, and also a key risk, in determining the likely success of many initiatives. Fifty Annual
Plan strategies are either entirely or partly reliant on the use of imaging. These strategies include
specific targets, such as for CT and MRI wait times, or wider goals such as improving cancer
pathways. Other areas relying on imaging services include plans to strengthen primary care
through GP access to diagnostics or supporting systemic improvement in patient flow through the
use of technology, such as RIS/PACS. A full list of Annual Plan strategies that have a Medical
Imaging component, are shown in section 10.1.
The Role of Medical Imaging
Medical Imaging is the technique and process used to create images of the human body for clinical
purposes, including the diagnoses of disease, in order to recommend treatment options for
patients. It serves the needs of referring clinicians and is influenced by developments in all areas of
medical practice. Similarly technological developments in medical imaging provide greater options
for clinical management that is incorporated in best practice pathways.
Due to resource constraints, imaging services in the public sector, need to prioritise patients with
different acuities ranging from acute ED trauma patients to routine GP referrals. The services are
funded from a range of sources including CWD discharges, ED attendances, and Community
Referred contracts, health insurers including ACC, maternity s88 payments, national screening
contracts, and private individuals. Services are delivered by both public and private providers.
One of the tensions to be managed is the need to minimise unnecessary examinations, in an
environment where the benefits and accessibility of information continues to improve. Global
issues affect both public and private medical imaging providers and addressing these is
fundamental for the healthcare system of the future. These challenges are:
Ensuring that there are the right services, in the right place to meet the needs of referrers.
Ensuring there are sufficient radiologists employed, and in training, to undertake not only
the viewing and reporting of images, but also to deliver and develop interventional services,
to foster special interest areas, to support training, participate in clinical rounds and
multidisciplinary meetings, and to be key decision makers in healthcare strategies and to
provide opportunities for positive engagement with referrers in both primary and secondary
care.
Ensuring that regional plans for implementing technology, maintaining equipment and
growing staff keep pace with the needs of the health sector.
Ensuring strong networks exist and are maintained between imaging services and referrers
so resources are used effectively and radiologists can actively guide best practice in using
imaging services.
Utilising technology to strengthen services in and out of hours.
Providing a compelling case for change for longstanding problems and thinking differently
about how services are resourced, delivered, and developed.
Providing a sustainable practice environment for ultrasound services that supports more
successful recruitment and retention of sonographers.
27 March 2014 Medical Imaging Landscape Report Page 7 of 91Whanganui DHB Annual Plan Whanganui DHB funds its Hospital Medical Imaging Department for all imaging required in the region. In turn the hospital based service provides a range of examinations and purchases from other suppliers those aspects they are unable to provide. This includes arrangements to access complex investigations such as interventional radiology, mammography and PET/CT and currently shorter term contracts to meet wait times, mostly in ultrasound. The largest outsourced arrangement is in the provision of a radiologist reporting service from Pacific Radiology in Wellington. This contract, for ongoing service provision and to support to the sole radiologist in Whanganui, ensures timely reporting and the availability of a broad range of examination types locally. The funding model strengthens the public sector which is critical in this small population. The DHB is relatively well placed to meet the initiatives of its Annual Plan with a well-functioning service for plain film, CT and MRI. General Practice has access to all modalities except MRI and while some pathways such as breast imaging have been fragmented, the DHB has implemented both short term and long term alternatives to manage inequities. The recently implemented RIS/PACS system has provided clinicians with improved access to information and improved internal data collection. As the initial implementation site of the regional RIS, this investment is expected to improve operational flexibility within the region’s radiology services in the future. However, ultrasound services are currently less than optimal, with the service unable to meet service needs due to staffing challenges. Contingencies are in place to support service delivery however these are temporary ad hoc arrangements requiring a number of patients to travel outside the region for this service. Acute arrangements are less than ideal due to inconsistency of options across the week. Addressing the service issues is now a priority and will be fast tracked through the development. MidCentral DHB The MDHB region is supported by four imaging providers, with the two largest being Palmerston North Hospital (PNH) and Broadway Radiology. The MDHB funding division purchases services from all providers. As a result the initiatives of the MDHB Annual Plan reflect the influence of all providers in the region. This disseminated model creates competition, offers choice and is responsive to progressing new strategies however there are inequities between providers and their readiness to participate in the market. PNH’s Medical Imaging Department has been constrained for many years due to lack of radiologist resources. Radiologists are central in the development of any imaging service and as a consequence shortages in this group have limited the development of other staffing groups, technologies and the ability of the service to play a role in new strategies. Notwithstanding these constraints MidCentral has developed a capability for interventional work that is greater than other similar sized facilities and has maintained a reputation for the quality of work undertaken. In 2013 radiologist staffing for the hospital has improved considerably as a result of active recruitment and improved retention over the past three years. There has been considerable investment over the past 18 months in replacement equipment, providing in many cases a step change in capability. Investment will be required if more radiologists are to be employed over historical levels, to support sustainable levels of staffing and in recognition of service growth and to move the PNH service forward. 27 March 2014 Medical Imaging Landscape Report Page 8 of 91
The impact of new models of care, such as both the attendance and preparation for multidisciplinary meetings is also significant, with Radiologist capacity not simply a factor of the volumes of images reported. The role of this service within a more integrated health system, local and regionally, is changing. Good relationships, acknowledgement of interdependencies and agreement that strong suppliers in public and private are needed, and in fact complement each other, will provide certainty and confidence for the community in the health sector overall. Initiatives for primary care and implementing collaborative pathways are well supported by a philosophy to move imaging services to the community, making these easily accessible in a timeframe that facilitates better patient management outside of the hospital setting. The range of suppliers available to MDHB provides opportunities in this regard, which could be further enhanced by the development of community based publicly provided capacity, in a similar fashion to the community based Breast Imaging Service for example. The expected pace of the Faster Cancer Treatment programme is yet to fully appreciated, but will impact on CT services in the future. The current model of service for CT was discussed in the July update, with consideration being given to investment in teleradiology services and additional CT staff to better manage out of hours and weekend CT work. Ultrasound services continue to be constrained, mostly through a global shortage of public sector sonographers. Staffing in this area does fluctuate and PNH continues to train a number of sonographers each year; however a large private market does have an impact on retention. 27 March 2014 Medical Imaging Landscape Report Page 9 of 91
3 DHB FUNDING PHILOSOPHIES DHBs have a responsibility to fund access to community referred radiology services. There are differences between MidCentral DHB and Whanganui DHB in their funding approach. These differences are neither right nor wrong (and indeed there are significant variations between DHBs of all sizes and localities across the country). They are approaches that have evolved to meet the needs of the DHB’s primary care referrers given the capabilities that have existed over time in each DHB’s public and private provider markets. Primary Care Diagnostics Both DHBs support primary care having an increased responsibility for ordering diagnostics and acting on the reported results to maintain care for the patient in the community setting, if that is appropriate. This is now increasingly supported by greater standardisation, through the use of clinical pathways that require access to diagnostics, along with documentation of the patient history, and the clinical assessment to progress referral of the patient. These standardised clinical pathways are also now better supported by Primary Care information systems. This is reflected in the increasing use of the Map of Medicine, which can systematically guide the primary care clinician through the appropriate diagnosis and treatment decisions. The increased use of community referred diagnostics has also been enabled by the move to integrated family health centres (with a broader range of on-site diagnostic services; including x-ray and ultrasound) supporting the Better, Sooner, More Convenient approach. The two DHBs enable community referred radiology services in different ways. MidCentral has been influenced by the availability of a mature private provider market and in Whanganui by the relative lack of private providers and the need to retain sufficient volume within the hospital system to provide economy of scale. MidCentral DHB The Funding Division has, for a number of years, looked to support primary care to better exercise the decisions to order radiology diagnostics through giving it the responsibility for managing the availability, quality and appropriateness of radiology as a diagnostic tool. To this end the DHB has contracted the Central PHO to provide plain film x-ray and non-maternity ultrasound for the Otaki, Horowhenua and Tararua populations. The contract for this service has a number of quality requirements including that the PHO maintains an active radiology oversight committee chaired by a primary care referrer. The contract has a set number of Relative Value Units (RVUs) per locality and a price per RVU which in effect sets the community referred radiology budget within which the PHO is expected to operate. In effect the PHO (i.e. the primary care referrers) hold the budget. The PHO is able to have as few or as many radiology providers as appropriate to encourage services to be provided as locations convenient to each community. Limited contracts for specific purposes have been issued directly to the private providers for services such as Renal, Ultrasound DVT, CT colonoscopy, CT Heads and Transient Ischemic Attack (TIA) diagnostics. Palmerston North Hospital provides all other community referred radiology services including plain film x-ray. It is the DHBs intention to transition Feilding and Palmerston North to the same PHO contract once integrated family health centres are established in those locations. MidCentral has also demonstrated preparedness to contract radiology diagnostic services from private providers in situations where the hospital provider cannot provide the timeliness, volume or quality required. 27 March 2014 Medical Imaging Landscape Report Page 10 of 91
Whanganui DHB
Whanganui DHB provides community referred radiology for plain film x-ray, maternity, CT and MRI
services through the Wanganui Hospital Provider. There is no budget holding of volumes by the
PHO in this process. Private x-ray and ultrasound services are limited in Whanganui and are
probably not sustainable. This arrangement provides economies of scale as it allows for the
employment of additional staff to support out of hours rosters.
The contract for community referred radiology is included in the Service Level Agreement between
the WDHB Funder and Provider and is agreed annually. The Provider bears the risk of any over
delivery of volumes against this contract. Plain film x-rays, ultrasound, and CTs are all included in
this contract.
Funding for community referred MRI is specifically excluded, however historically access has been
given by the hospital provider to consultants to refer their patients from private for MRIs. The
value of this unfunded work is approximately $150K annually. Ideally the cost of private referred
MRI would be covered by health insurers and the DHB has initiated discussions to see how the
barriers to this occurring could be overcome. Currently, insurers do not reimburse for services
provided by public hospitals.
As a provider, Whanganui DHB does not charge co-payments on any community radiology,
including ACC. However, co-payments are applied by private providers of radiology services.
In 2011/12 the WDHB Provider over-delivered against the community referred radiology contract,
which was increased at the beginning of the 2012/13 financial year. The Funder purchases relative
value units per modality as per the table below.
Contracted Actual
Community Referred Radiology RVUs 12/13 RVUs 12/13
Plain Film 9,200 12,188
CT 11,000 11,106
Ultrasound (excluding maternity) 3,700 3,272
Mammography 1,600 959
Other - Bone Density scans, Nuclear Med Scans, GP
referred interventional radiology and floroscopy 472 82
MRI - 4,156
25,972 31,763
Maternity Ultrasound 7,833 7,679
Whanganui DHB also purchases community radiology from MidCentral DHB through inter-district
flows. For the 2012/13 year this amounted to 1,941 RVUs with a funding value of $134,783.
Total DHB Public Funding Levels
Analysis of Whanganui‘s and MidCentral’s total funding of public and private providers shows that
Whanganui is funding at approximately $44,500 per 1,000 population while MidCentral is funding
at $72,500 per 1,000 population.
The differences may, in part, be explained by MidCentral’s provision of more complex examinations
and procedures. However the mature private market in MidCentral’s should also be considered in
order to get a complete view of the relative position of each DHB.
27 March 2014 Medical Imaging Landscape Report Page 11 of 914 REGIONAL DEMOGRAPHIC PROFILE
The current and future model of service for Medical Imaging, including predictions on issues of
access and supply, is significantly influenced by the profile of the populations the service is
designed to support. This section reviews the sources and correlation of current populations
counts (the census), the population projections and DHB Medical Imaging patient and examination
volumes. The data sources and analysis are shown in section 10.2.
The purpose of this analysis is to identify and understand any differences in access for particular
population groups (in the context of their relative health need) and provide a view on the likely
impact of population change generally. The analysis also considers the impact of ethnicity as a
proxy for health disparity and age as a proxy for likely health care intensity.
Statistics New Zealand publishes data sets to provide insight into the profile of the population of
each DHB, by DHB region and territorial authority. Census 2013 data is not yet available and
therefore 2006 data is used for this report. As this data is both outdated, and reported for the
territorial authorities within each DHB but not the DHB areas themselves, it is only a convenient
guide to the information, and is not to be considered absolutely correct.
The most recent census data is due for imminent release, and should be reviewed against the
indications considered in this section of the paper.
The latest population estimate for DHB boundaries shows that at 30 June 2012 Whanganui DHB’s
population was estimated to be 62,600 while MidCentral DHB’s population was estimated to be
169,300.
Given the correlations between health outcomes, age, family support, ethnicity and poverty the
following key factors will influence the Medical Imaging Landscape.
The residents of Whanganui DHB area, to a greater degree, and MidCentral to some degree,
have higher levels of socio-economic deprivation and higher percentages of the population
identified as Maori than the New Zealand average.
Whanganui DHB has significantly more people identified as Maori (23%) than New Zealand
overall (14%) and MidCentral DHB (17%). However MidCentral has the greater number of
Maori and both DHBs have similar number of Maori living in their rural areas.
More Whanganui males and females identified themselves as smokers (24% respectively)
compared to 20% and 18% for New Zealand males and females and 22% and 21% for
MidCentral.
Fewer Whanganui women aged 15 years and over had no children (21%) compared to New
Zealand over all (28%) and MidCentral women (27%).
More Whanganui and MidCentral women had 4 or more children (18% and 16%
respectively) than for New Zealand over all (13%).
More Whanganui and MidCentral people had no qualifications (30% and 27% respectively)
compared to New Zealand overall (22%).
79% of MidCentral people had personal incomes less than $50,000 for the year ended 31
March 2006 compared to 73% for New Zealand overall and 78% for Whanganui people.
More Whanganui and MidCentral people were on unemployment, sickness or domestic
purposes benefits than for New Zealand overall. 19% of Whanganui people were on NZ
Superannuation or veterans pensions compared to 14% for New Zealand overall and 17% for
MidCentral people.
27 March 2014 Medical Imaging Landscape Report Page 12 of 91 A similar number of people in New Zealand overall, MidCentral and Whanganui DHB areas
were identified as not being in the workforce (30-33%) and in full time employment (45-
48%).
Slightly more people in MidCentral and Whanganui were a couple with no children (42%
and 41% respectively) compared to New Zealand overall (40%) but more Whanganui
families identified as having a single parent (22%) than did MidCentral families (19%) and
New Zealand families overall (18%).
Slightly fewer Whanganui people were in a one family household (65%) compared to New
Zealand overall (68%) and MidCentral (67%) and more Whanganui people were in one-
person households (28%) compared to 25% in MidCentral and 23% in New Zealand overall.
4.1 PROJECTIONS
For WDHB the projected change over the period from 2006 to 2031 is a decrease to 89% of the
2006 census count. Significantly the 65+ age group change is 170% while the other age groups are
in the 73% to 78% range.
For MDHB the projected change over the period from 2006 to 2031 is an increase of18,250 people
or 112% of the 2006 census count. Significantly the 65+ age group change is 192% while the other
age groups are in the 94% to 105% range.
For WDHB the number of Maori will increase by 2021, for all ages, to 109% but that the 65+ group
show a change of 180%. Other age groups changes range between 102% and 111%.
While for MidCentral the change for all ages is 126% and 267% (1500 people) for the 65+ group.
The 40-64 group changes by 142% while ages below that approximately 115%.
By 2021 territorial authorities within the Whanganui DHB area will have, compared to the 2006
Census:
6,350 fewer people but 4,450 more in the 65+ age group
1,700 more people identifying as Maori of which 800 more will be aged 65+
Rural populations will decline
By 2021 territorial authorities within the MidCentral DHB area will have, compared to the 2006
Census:
11,900 more people of which 10,650 more will be 65+
Palmerston North City will have an additional 2,800 Asian and 1,900 Pacific Island people of
which 900 and 200 respectively will be 65+
While the total population changes are the single largest influence on capacity needed, the impact
of the aging population and the greater number of people aged 65+ is less certain. There are
various theories in respect to aging, health need and health resources. One view is that utilisation
of health resource is a constant no matter what age people live to, and that those who live longer
simply do so due to better health. The counter view is that as an aging population will be greater
users of health service due to our increased risks of age and the longer term effects of lifestyle
factors.
Specifically medical imaging market analysis (data from the major equipment suppliers) is
forecasting continued growth in developing countries driven by economic growth and population
aging but diminishing growth in developed countries due to budget constraints.
27 March 2014 Medical Imaging Landscape Report Page 13 of 914.2 EQUITY OF ACCESS As part of the review of the regional demographics a high level analysis of imaging techniques and access, relative to age and ethnicity, was undertaken. This work requires further expert interpretation before publication, however there is variability noted between Maori and non Maori population access to imaging that requires further explanation. An analysis of this area, with a view to considering where change may be required, will be completed for the final plan. 27 March 2014 Medical Imaging Landscape Report Page 14 of 91
5 MODALITY DESCRIPTIONS AND OBSERVATIONS
This section explores in greater detail the various modality areas. Each area is described with a focus on
how the area works and the differences between the various providers. Key linkages with major health
priorities are also described where relevant. Potential opportunities, originating from key issues, have been
developed through consultation and research and are noted for each area. These will form the basis upon
which final development steps to be agreed and presented. This section also highlights where further work
is required to better understand or to gain agreement on the clinical and strategic direction.
Further detail on these services (including service volume, equipment, staffing and hours) are included in
section 10, Hospital Based Services, page 65.
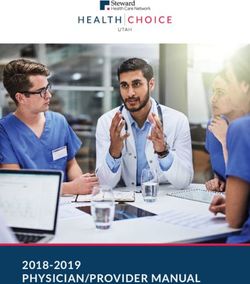
5.1 WHERE SERVICES ARE PROVIDED
The adjacent map of medical imaging service
locations shows that general x-ray services are
quite wide spread across the combined DHB
districts including facilities at both Turoa and
Whakapapa.
Fixed ultrasound services are provided in
Dannevirke, Palmerston North and Wanganui
with portable services provided in Levin and
Feilding.
Fluoroscopy, CT and MRI are provided in both
Wanganui and Palmerston North while
Angiography, Bone Densitometry, Nuclear
Medicine and Medical Photography services are
provided only in Palmerston North.
Mammography and screening are provided
from fixed locations in Palmerston North and
Wanganui with all the smaller centres covered
by the Mobile Breast Screening Service.
Numbers in the map colour code refer to the
number of service providers at each location.
FIGURE 1: LOCATION OF SERVICES
27 March 2014 Medical Imaging Landscape Report Page 15 of 915.2 BREAST IMAGING
5.2.1 MODALITY DESCRIPTION
Breast cancer is a significant health issue for New Zealand and is the leading cause of cancer death in non-
smoking New Zealand women. The incidence of both female and male breast cancer has increased in
recent years however reassuringly the mortality rate has reduced by 19% over the last decade. This
reduction is generally attributed to earlier detection and the greater use and effectiveness of adjuvant
treatment. The majority of breast cancers are detected through breast x-rays or mammograms.
There are three pathways for breast cancer diagnosis. These are:
1. Diagnosis via the BreastScreen Aotearoa programme
2. Diagnosis made in the private sector and referred to secondary or tertiary care or
3. Referral from primary care for breast symptoms or at risk mammography to secondary services,
either surgical or imaging
The BreastScreen Aotearoa programme, for women 45-69 years, is a diagnostic pathway for the detection
of breast cancer. The National Screening Unit (NSU), as part of the National Health Board, is responsible
for coordinating all population screening activities including BSA. The NSU contracts eight regional ‘Lead
Providers’ to deliver breast screening services nationally.
The Lead Provider for the Whanganui and MidCentral regions is MDHB. The providers have their own
unique brands with the service across the central North Island known as ‘BreastScreen Coast to Coast’ or
BSCC.
BSCC operates from a central hub in Amesbury St in Palmerston North. This site provides screening services
for the MidCentral region, and assessment services to facilitate diagnosis (further views, ultrasound and/or
biopsy) for those women found to have an abnormal screening mammogram. This site also administers the
programme and leads health promotion activity.
A mobile breast screening unit travels the region on a two yearly basis and there are nine mobile sites in
the region. These are in Otaki, Levin, Foxton, Dannevirke, Feilding, Marton, Gonville, Taihape and Ohakune.
The mobile unit is popular with women and is a key factor in providing remote and rural access to the
programme.
Screening mammograms are available year round at Progressive Medical Imaging, a private site in
Whanganui, which offers mammograms services only. Whanganui women with an abnormal screening
mammogram go to Palmerston North for further investigation and diagnosis.
Diagnostic breast imaging, in comparison to breast screening, is for those patients presenting with a
specific breast symptom or for those on a planned programme of follow up post breast cancer. These
patients, both male and female, are referred from both primary and secondary services.
A diagnostic work up or ‘triple assessment’ includes a mammogram, a targeted breast ultrasound and/or a
biopsy of a suspicious lesion.
MidCentral DHB
In Palmerston North the symptomatic and surveillance, or diagnostic mammograms are also taken in
Amesbury St, under the name of the MDHB Breast Imaging Service. Triple assessment is offered for all
symptomatic women and in the majority of cases this means one visit for women, and men, to complete a
diagnostic work up. This service has only recently combined with BSCC and the process continues to be
embedded. In addition, the introduction of a map of medicine pathway from General Practice to specialist
care, via the imaging service is planned for the next six months.
27 March 2014 Medical Imaging Landscape Report Page 16 of 91Whanganui DHB BSA is responsible for the delivery of a screening service for the women of the Whanganui region. The service provided for symptomatic women is the responsibility of the WDHB and is delivered via referrals to the Radiology Department. As the WDHB outsourcers mammography but provides ultrasounds this has led to a disjointed service for woman and extended waiting times between examinations. It also requires significant monitoring to ensure delays to diagnosis do not occur. Currently discussions are underway with Broadway Radiology to provide both mammography and ultrasound services in an attempt to reduce waiting times for symptomatic women. Streamlining of breast imaging to one event, and potentially one site, minimises the risk of unnecessary delays and will improve waiting times required by the national programme for faster cancer treatment. 5.2.2 KEY ISSUES Equipment The National Screening Unit requires all BreastScreen providers to have digital equipment by the end of 2013. This directive has instigated a nationwide upgrade of services and the implementation of a central national PACS for all BreastScreen images. The breast imaging service in Palmerston North has effectively completed a digital upgrade and aims to have this fully implemented by year end, with the delivery of a new digital mobile unit. For mammography services in Whanganui, both screening and diagnostic, the local provider is contracted until June 2014. This site is not digital and continues to assess the feasibility of whether it is financially viable to upgrade to a digital platform. Faster Cancer Treatment In October 2011, the Minister of Health outlined a programme of work to provide Faster Cancer Treatment with a focus on improving the quality of care. Key components of the programme include early recognition and reporting of symptoms and rapid access to investigations and treatment. Effective management of the diagnosis and treatment of breast cancer is long established internationally, and in New Zealand. Dedicated and well organised breast care teams are essential for the rapid assessment and diagnosis of breast problems including cancer. At a minimum, this includes a multidisciplinary team of surgeons, radiologists, pathologists, breast care/breast cancer nurses and medical radiation therapists with access to onsite mammography and ultrasound, preferably with stereotactic facilities and ready access to magnetic resonance imaging (MRI), nuclear medicine and computed tomography (CT) scanning. MidCentral has made a number of steps to improve breast services in the past two years and as a consequence is well placed with new equipment and a comprehensive model of care for breast diagnosis to meet the expectations of the Faster Cancer Treatment programme. 5.2.3 POTENTIAL OPPORTUNITES The current model of care for Whanganui does not meet the requirements of faster cancer treatment, and with the current technology being used, does not meet the national requirements for screening mammograms. A workshop, held in May 2013 with stakeholders across the breast pathway, proposed that there is one centralAlliance breast care service, subject to approval of a business case. If implemented, the service would be led from the Breast Imaging Service in Palmerston North, but with multiple sites delivering screening and diagnostic services (mammograms, biopsies and breast ultrasounds) across the region. Triple assessment models are traditionally offered on one physical site capitalising on the one location of equipment and specialist staff. This is extremely effective in metropolitan regions that densely populated and well served by public transport, yet relatively small geographically. 27 March 2014 Medical Imaging Landscape Report Page 17 of 91
In this region however, which is geographically large and sparsely populated, a single facility model would
create as many barriers as it would minimise. Challenges of geography and access to effective transport
does not preclude rural and provincial regions from enjoying the same level of clinical excellence
experienced in larger centres, but simply requires solutions that understand and meet the needs of the
population rather than the population trying to adapt to a one size fits all model.
The one service will operate with consistent imaging pathways for all aspects for breast imaging and
diagnosis, will arrange the annual imaging of women post breast cancer and provide overarching
governance and clinical leadership, in partnership with the surgical and oncology specialties in both
regions, for the ongoing care and management of breast disease.
The one service model builds on an already well-established specialist team and through a function of
organic growth, rather than duplication; this team could expand to encompass the wider region.
This model is pre-existing in some circumstances with the BSCC programme operating at two fixed
screening sites and eight (8) mobile unit sites already. Diagnostic services in MidCentral already operate a
triple assessment approach and are planning to improve this model before the end of the year.
A future model would therefore consolidate what is currently available, enhance it where needed and
design any local variations, including the expansion of a site offering mammograms, ultrasound and
Radiologist services, in consultation with community and local health providers.
The model would include:
Eight mobile breast screening sites, as currently scheduled.
A lead site in Palmerston North from which all clinical activities would be managed. This site will
provide screening for the MidCentral region, BSA assessment services for both regions, reading of
mammograms for both regions, stereotactic biopsy and all administration including bookings.
A permanent outreach site in Whanganui offering screening mammograms and triple assessment of
diagnostic patients on a routine basis, with the opportunity for Whanganui clients to travel to
Palmerston North between pre planned sessions should they wish to, or if their clinical presentation
requires a swifter pathway to diagnosis.
Benefits of this model include:
Opportunities for improved communication and the development of effective relationships through a
multidisciplinary patient centred approach to care provision along the complete patient cancer
pathway.
Reduced anxiety for patients, family and whānau through increased trust in a more effective,
consistent and accessible system.
Better control and survival benefit for some cancer patients.
Effective use of specialist staff and equipment.
Dedicated breast nurses to act as a coordinator of care to facilitate the treatment pathway and to
provide guidance and support from symptoms to diagnosis through to follow-up.
Improved strategic decision making through consistent information, data collection and clinical
governance.
Value for money through reduced duplication and consolidation of skills and equipment in one
structure.
OPPORTUNTIES FOR FUTURE DEVELOPMENT
MDHB and WDHB to explore the development of an outreach dedicated breast imaging facility in
Whanganui, maintaining breast screening and diagnostic service provision locally in the region.
TABLE 1: BREAST IMAGING FUTURE DEVELOPMENTS
27 March 2014 Medical Imaging Landscape Report Page 18 of 915.3 MRI MRI is a rapidly growing and evolving medical imaging technology which is increasingly being requested by clinicians as the established standard for accurate and definitive diagnoses. There have been significant technological leaps forward which reduce examination times, improve image quality and the patient experience, particularly with the introduction of a wider bore. 5.3.1 MODALITY DESCRIPTION Two MRI scanners are located in the Whanganui and MidCentral region; one in Whanganui Hospital and one located on the Palmerston North Hospital campus, owned and operated by Broadway Radiology. Broadway Radiology provides all MRI services for MDHB via a fee for service contract. The service provided is well regarded however as demand grows increased volumes have created cost pressures for the hospital services. The Wanganui hospital has had MRI since December 1993. The current MRI scanner is a Siemens 1.5 Tesla unit, which is 9.5 years old and currently operating a 4 receiver channel system. Peripheral equipment includes an MR compatible automatic injector and pulseoxymeter (heart rate and oxygen saturation monitor). A planned upgrade in the near future will increase the number of receiver channels to 18. The Broadway Radiology MRI scanner in Palmerston North is a GE 1.5 Tesla unit, commissioned in October 1999 sited on the MDHB campus. About four years ago it was upgraded to an 8 channel system. Broadway Radiology MRI has access to full MRI compatible anaesthetic monitoring equipment. This anaesthetic monitoring equipment is owned by MDHB but is stored in the Broadway MRI scanner room. Broadway has an MRI compatible pulseoxymeter, but do not have an automatic injector. Consideration to technological improvements in three (3) tesla machines should also be considered when MRI machines are replaced. Wide bore technology has been developed, which enables obese patients to be scanned with greater ease. These patients are often not able to be scanned because they do not fit in the regular sized scanners. The wider bore also means a drop in the number of patients needing sedation to undergo scans, and has made scanning shoulders on even relatively normal sized patients much better tolerated from the patient’s perspective. Neither WDHB nor Broadway Radiology currently have wide bore magnets, and is something to be considered in futures years as part of the asset replacement cycle. Both scanners provide a similar range of examinations. These include musculoskeletal, neurological, abdominal and vascular imaging. The capabilities of the scanners are very comparable, with the only difference between them being that Broadway Radiology scanner has the equipment and software to perform Non Contrast Angiography, Breast MRI, Tempero-mandibular Joint MRI and MRI examinations under anaesthetic. Broadway Radiology also performs Spectroscopy of the brain, although this is seldom used. There is a good level of access to MRI in Whanganui. The MRI scanner is available 5-days per week between 08:00 and 16:00 on Mondays and Fridays, and 08:00 to 21:00 Tuesdays, Wednesdays and Thursdays. Access to outpatient and community referred MRI is being measured monthly and reported to the Ministry of Health via the Faster Access to Diagnostics Reporting. The following table shows access for these referral types in Whanganui. 27 March 2014 Medical Imaging Landscape Report Page 19 of 91
You can also read