Mast cells can produce transforming growth factor β1 and promote tissue fibrosis during the development of Sj ogren's syndrome-related sialadenitis
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

Modern Rheumatology, 00, 2021, 1–9
DOI: https://doi.org/10.1093/mr/roab051
Advance access publication date: 2 September 2021
Original Article
Mast cells can produce transforming growth factor β1 and
promote tissue fibrosis during the development of
Sjögren’s syndrome-related sialadenitis
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab051/6363017 by guest on 06 November 2021
Shinjiro Kaiedaa,* , Kyoko Fujimotoa , Keita Todorokib , Yushi Abeb , Jingo Kusukawab ,
Tomoaki Hoshinoa and Hiroaki Idaa
a
Department of Medicine, Division of Respirology, Neurology and Rheumatology, Kurume University School of Medicine, Kurume, Japan
b
Dental and Oral Medical Center, Kurume University School of Medicine, Kurume, Japan
*Correspondence: Shinjiro Kaieda; kaieda@med.kurume-u.ac.jp; Department of Medicine, Division of Respirology, Neurology and Rheumatology, Kurume
University School of Medicine, 67 Asahi-machi, Kurume 830-0011, Japan.
ABSTRACT
Objectives: This study investigated the associations of mast cells with immune-mediated inflammation and fibrosis in patients with primary
Sjögren’s syndrome (pSS); it also explored the underlying pathophysiology of pSS-related sialadenitis.
Methods: Twenty-two patients with pSS and 10 patients with sicca (control individuals) underwent labial salivary gland biopsies. Sections were
subjected to staining and immunofluorescence analyses. HMC-1 human mast cells were cocultured with fibroblasts in vitro; fibroblasts were
also grown in HMC-1 conditioned medium. mRNA levels of collagen Type I (Col1a) and transforming growth factor (TGF)β1 were analysed in
cultured cells.
Results: Mast cell numbers in labial salivary glands were significantly greater in patients with pSS than in control individuals. In sali-
vary glands from patients with pSS, mast cell number was significantly correlated with fibrosis extent; moreover, mast cells were located
near fibrous tissue and expressed TGFβ1. Col1a and TGFβ1 mRNAs were upregulated in cocultured fibroblasts and HMC-1 cells, respec-
tively. Fibroblasts cultured in HMC-1 conditioned medium exhibited upregulation of Col1a mRNA; this was abrogated by TGFβ1 neutralizing
antibodies.
Conclusions: Mast cell numbers were elevated in patients with pSS-related sialadenitis; these cells were located near fibroblasts and expressed
TGFβ1. TGFβ1 could induce collagen synthesis in fibroblasts, which might contribute to fibrosis.
KEYWORDS: Fibrosis; mast cell; salivary gland; Sjögren’s syndrome; transforming growth factor β1
Introduction to pSS-related hyposalivation and xerostomia [9]. The grade
Primary Sjögren’s syndrome (pSS) occurs predominantly in of salivary gland tissue fibrosis is reportedly associated with
middle-aged women and is characterized by extensive lym- overall stimulated salivary flow [10]. It has been demon-
phocytic infiltration into exocrine glands and other organs, strated that aberrant upregulation of transforming growth
which causes dry mouth, dry eyes, and various extra- factor (TGF)β1 in the salivary glands of patients with pSS
glandular symptoms [1]. Various factors (e.g. genetic pre- contributes to the onset of fibrosis through mesenchymal
disposition) and environmental triggers (e.g. virus infection) changes in salivary gland epithelial cells [11]. No curative
are known to influence the development of pSS [2, 3]. Focal treatment has been established for the disease; current ther-
lymphocytic sialadenitis is a diagnostic criterion for pSS; it apy is limited to alleviation of symptoms. Recently, a T
consists of large numbers of activated T cells and B cells, cell-targeting biologic, abatacept, has been shown to enhance
together with specialized antigen-presenting cells such as saliva production, but not to reduce active gland destruction
monocytes/macrophages and dendritic cells [4, 5]. Fibrosis (characterized by lymphocytic infiltrate, tissue atrophy, and
is a common consequence of tissue damage and inflamma- fibrosis) in patients with pSS or secondary Sjögren’s syndrome
tion [6]. Fibrosis in the salivary glands has been noted as [12, 13]. Although the clinical utility of early abatacept inter-
a pathological element of the disease in patients with pSS; vention against sialadenitis has been suggested, its efficacy
this phenomenon is related to focal lymphocytic sialadeni- remains controversial. Newer treatments are needed to reverse
tis, which can be assessed by focus score, and is not solely inflammation and tissue damage, thereby maintaining salivary
attributable to age [7, 8]. A prior study indicated that the function in patients with pSS.
degree of CD4+ T-cell clonal expansion was positively cor- Mast cells contribute to a variety of allergic and non-
related with the proportion of salivary gland fibrosis and led allergic inflammatory diseases and autoimmune diseases
Received 1 March 2021; Accepted 29 July 2021
© Japan College of Rheumatology 2021. Published by Oxford University Press. All rights reserved.
For permissions, please e-mail: journals.permissions@oup.com
2 Kaieda et al.
(e.g. food allergy, inflammatory bowel disease, inflammatory Burlingame, CA, USA), as previously described [25]. To con-
arthritis, psoriasis, and systemic sclerosis) [14–16]. In the firm the presence of mast cells, after antigen retrieval in
context of pro-inflammatory and fibroblastic conditions, the accordance with the manufacturer’s protocol, sections were
numbers of mast cells have been shown to increase in joints stained with an anti-tryptase antibody (1:100 dilution, clone
with chronic arthritis inflammation and systemic sclerosis AA1; Medical & Biological Laboratories Co., Ltd., Nagoya,
fibroblastic lesions [17, 18]. Mast cells have been recognized Japan) or with control mouse immunoglobin G (IgG; Abcam,
as a cellular source of TGFβ or TGFβ1 in skin fibrob- Cambridge, MA, USA), followed by detection with a Vec-
lastic lesions exhibited by patients with systemic sclerosis, tastain ABC-horseradish peroxidase-alkaline phosphatase kit
bone marrow fibrosis, or idiopathic pulmonary lung fibro- and diaminobenzidine or horseradish peroxidase substrate.
sis [18–20]. Normal labial salivary glands primarily contain Sections were then counterstained with Gill’s II haematoxylin
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab051/6363017 by guest on 06 November 2021
connective tissue mast cells, which are in close contact with and mounted with Crystal/Mount or Cytoseal (Cat. No.
various resident cells (e.g. fibroblasts) [21]. Previous studies 08381-120; Polysciences, Warrington, PA, USA). Fibrotic
have indicated that mast cells may participate in pSS-related lesions in labial salivary glands were identified by Verhoeff–
sialadenitis, although the mechanisms by which mast cells van Gieson staining. The degree of fibrosis in minor labial
contribute to the development of sialadenitis remain unclear salivary glands was quantitatively graded in a blinded manner,
[21, 22]. Notably, a strong correlation has been reported as previously reported [22].
between the number of mast cells and degree of salivary tissue
fibrosis (rather than lymphoid infiltration); the roles of mast
cells in the pathogenesis of pSS have not yet been elucidated Immunofluorescence
[22]. Immunofluorescence analysis of paraffin-embedded sections
The objectives of this study were to determine the num- was performed to determine whether mast cells are located
bers of mast cells in minor salivary glands from patients with near fibroblasts in the salivary glands. Dual staining for
pSS and control individuals and to evaluate the associations of human mast cell tryptase and vimentin (a fibroblast cell
mast cells with immune-mediated inflammation and fibrosis in marker) was performed by using the Opal 4-color Manual
patients with pSS. Furthermore, we explored the mechanisms IHC kit (Cat. No. NEL810001KT; Perkin Elmer, Waltham,
by which salivary mast cells contribute to the pathophysiol- MA, USA), in accordance with the manufacturer’s instruc-
ogy of pSS-related sialadenitis; this facilitated investigation of tions. Following deparaffinization, the Blocking One (Cat.
the roles of TGFβ1 in fibrosis, as well as the source of TGFβ1 No.03953-95; nacalai tesque, Kyoto, Japan) was used for
in salivary glands. non-specific protein blocking. Sections were then incubated
overnight with anti-mast cell tryptase mouse monoclonal
antibodies (clone 10D11, 1:20 dilution) (Leica Biosystems
Inc., Buffalo Grove, IL, USA). Subsequently, sections were
Patients and methods washed using phosphate-buffered saline and labelled with
Patients Opal polymer HRP Ms + Rb for 10 minutes; detection was
Twenty-two patients with pSS and 10 patients with sicca performed using Opal Fluorophore Working solution (OPAL
(control individuals) were included in this study. All proce- 570). Sections were washed again, followed by dissociation
dures in this study were approved by the ethics committee and antigen retrieval in an autoclave at 121◦ C for 10 minutes.
of Kurume University (no. 17005) and adhered to the eth- Then, sections were washed and incubated overnight with
ical standards of the 1975 Declaration of Helsinki. Written anti-vimentin mouse monoclonal antibody (clone V9, 1:500
informed consent was obtained from all participants. All dilution) (Leica Biosystems Inc.). Finally, sections were
patients were diagnosed in accordance with the revised cri- washed and labelled with Opal polymer HRP Ms + Rb for
teria for the diagnosis of pSS, as defined by the American- 10 minutes; detection was performed using Opal Fluorophore
European Consensus Group [5]. Participants who failed to Working solution (OPAL 520). To determine whether mast
meet American-European Consensus Group criteria for pSS cells express TGFβ1 in labial salivary glands, sections were
(following salivary gland biopsy as described below), but incubated overnight with anti-human TGFβ1 (1:50 dilution)
had a complaint of dry mouth, were considered control (Peptide Institute, Osaka, Japan) and anti-human-mast cell
individuals. Stimulated saliva secretion was quantified in a tryptase monoclonal antibodies (1:10 dilution) (Leica Biosys-
standardized manner using the Saxon test [23]. tems Inc.); they were then labelled with Alexa Fluor 488 goat-
anti rabbit IgG (H + L) (Thermo Fisher Scientific K.K., Tokyo,
Japan) or Alexa Fluor 594 goat anti-mouse IgG (H + L)
Labial salivary gland biopsy (Thermo Fisher Scientific, Waltham, MA, USA). A confocal
Labial salivary gland biopsies were performed for all patients. microscope was used to analyse the results of fluorescence
Each specimen was obtained from the lower lip with par- staining.
ticipants under local anaesthesia. Specimens were graded by
focus scores in a blinded manner, as previously described [24].
Histomorphometric enumeration of
tryptase-positive mast cells in labial salivary glands
Immunohistochemical examination of labial Histomorphometric enumeration of mast cells was performed
salivary glands in a blinded manner, as previously reported [19, 26]. Briefly,
Formalin-fixed, paraffin-embedded sections (4 µm thick) of mast cells were enumerated by counting the numbers of
labial salivary glands were mounted on poly-L-lysine-coated tryptase-positive cells in deidentified labial salivary gland
glass slides. Immunohistochemical analyses were performed specimens; an eyepiece reticle was used to define an area of
by using the Vectastain ABC kit (Vector Laboratories, 0.04 mm2 . Five fields were counted in all samples.
Mast cells produce transforming growth factor β1 and promote tissue fibrosis 3
Human mast cell line and fibroblast coculture U test. Spearman correlation coefficients were used to eval-
systems uate correlations between quantitative variables. Data were
The human mast cell line, HMC-1, was obtained from analysed using GraphPad Prism software version 4 (Graph-
J.H. Butterfield, M.D. (Mayo Clinic, Rochester, MN, USA). Pad Inc., La Jolla, CA, USA). Differences were considered
Human pulmonary fibroblasts were obtained from Promo statistically significant when p < .05.
Cell (Heidelberg, Germany). All cells were cultured in Dul-
becco’s modified Eagle Medium (Invitrogen, Carlsbad, CA,
USA) supplemented with 10% heat-inactivated foetal bovine Results
serum (Hyclone Laboratories, Inc., Logan, UT, USA), 2 mM Mast cell number increased in patients with
L-glutamine, 100 U/ml penicillin, 100 µg/ml streptomycin, pSS-related sialadenitis
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab051/6363017 by guest on 06 November 2021
50 µM 2-mercaptoethanol, and 0.1 mM non-essential amino Labial salivary gland biopsy samples from 22 patients with
acids (Invitrogen). Cultured fibroblasts between Passages 4 pSS and 10 control individuals were analysed by immunohis-
and 8 were used in experiments. For 1 week coculture exper- tochemistry to investigate the expression of tryptase-positive
iments with HMC-1 and fibroblasts, 2 × 104 fibroblasts were mast cells. The participants’ demographic and clinical char-
seeded in each well of a 24-well plate. Forty-eight hours later, acteristics are shown in Table 1. Notably, tryptase-positive
1 × 104 HMC-1 cells were added. HMC-1 cells were phys- mast cells were more evident in labial salivary gland samples
ically separated from fibroblasts during coculture by place- from patients with pSS (Figure 1(b)) than in samples from con-
ment of HMC-1 cells into the upper chamber of a Transwell trol individuals (Figure 1(a)). Consistent with the findings in
culture dish with a membrane that contained 0.2-µm pores a previous report, mast cells in labial salivary glands did not
(Nalge Nunc International, Roskilde, Denmark). Half of the show signs of extensive degranulation (Figure 1(b)) [29]. The
medium volume was changed at 3-day intervals, as previously number of mast cells in the labial salivary glands was signifi-
reported [27, 28]. cantly greater in patients with pSS than in control individuals
To establish HMC-1 conditioned medium, HMC-1 cells (p < .0001, Figure 1(c)).
were stimulated with or without recombinant interleukin (IL)-
33 and stem cell factor (SCF) (50 ng/ml; Peprotec, Rocky
Mast cells may contribute to reduced salivary
Hill, NJ, USA) for 24 h. HMC-1 cells were washed twice and
secretion and tissue fibrosis onset in SS
seeded into standard culture medium for additional 24 h. Sub-
sequently, HMC-1 cells were centrifuged at 900 RPM for Next, we examined whether mast cells were involved in sali-
7 minutes at 4◦ C; culture medium (i.e. HMC-1 conditioned vary dysfunction in patients with pSS or control individuals.
medium) was then harvested. To avoid cell contamination, There was a significant negative correlation between Saxon
HMC-1 conditioned medium was passed through a 0.22- test results and mast cell number (R = −0.6742, p = .006,
µm filter (Merck Millipore, Billerica, MA, USA); the absence Figure 2(a)) in patients with pSS. However, the correla-
of cell contamination was confirmed by using a haemocy- tion was not statistically significant in control individuals
tometer. Next, fibroblasts (2 × 104 per well) were seeded in (R = −0.012, p = .097, Figure 2(b)). These results suggested
24-well plates for 48 hours and cultured with standard culture
medium or HMC-1 conditioned medium. Diluted HMC-1
Table 1. Demographic and clinical characteristics of patients with pSS and
conditioned medium in standard culture medium (1:3 dilu- control individuals with Sicca syndrome.
tion) was also utilized. Anti TGFβ-1,2,3 monoclonal antibody
(clone 1D11.16.8, eBioscience, San Diego, CA, USA) or Sicca syndrome
control mouse IgG1 functional grade isotype control (eBio- pSS (n = 22) (n = 10)
science) was directly added to subconfluent fibroblast cultures Age, years, mean ± SD 53.29 ± 16.11 58.4 ± 16.4
with HMC-1 conditioned medium. Female, n (%) 16 (94%) 7 (70%)
Disease duration, 3.8 ± 6.3 –
mean years
Quantitative reverse transcriptase polymerase Lymphoid focus score 3.1 ± 0.1 0
chain reaction Raynaud’s phe- 4 (18%) 0
Total RNA was isolated from HMC-1 cells and fibroblasts nomenon, n (%)
Pulmonary involve- 2 (9%) 0
by using an RNeasy Mini kit (Qiagen, Hilden, Germany). ment
For follow-up RT-PCR assays, purified RNA was converted Anti-nuclear 13 (76%) 4 (40%)
to complementary DNA (cDNA) by means of a Quantitect antibodies, n (%)
reverse transcription kit (Qiagen). Reverse transcriptase poly- Anti-SSA/Ro52 16 (73 %) 2 (20%)
merase chain reaction (RT-PCR) was performed with SYBR antibodies, n (%)
Green Mastermix (Qiagen) using primers for human β-actin, Anti-SSB/La 7 (32%) 0
antibodies, n (%)
Col1a, and TGFβ1 (Qiagen) on an Mx3000p PCR machine
Anti-centromere 3 (14%) 0
(Stratagene, La Jolla, CA, USA). Relative expression lev- antibodies, n (%)
els were calculated using the comparative threshold cycle Serum IgG (g/l) 2.1 ± 0.7 1.2 ± 0.4
method [27]. Erythrocyte sed- 41 ± 21.8 21.2 ± 16
imentation rate
(mm/1 h)
Statistical analysis ESSDAI 4.6 ± 3.5 –
Results are presented as mean ± standard error of the mean. ESSDAI: European League Against Rheumatism Sjogren’s Syndrome Disease
Statistical analysis was performed using the Mann–Whitney Activity Index.4 Kaieda et al.
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab051/6363017 by guest on 06 November 2021
Figure 1. Tryptase immunohistochemistry analysis of labial salivary glands from control individuals and patients with pSS. (a, b) Immunohistochemistry
with an anti-tryptase antibody revealed upregulation of mast cells in labial salivary glands from patients with pSS (b) compared with glands from control
individuals (a). Scale bar, 50 µm. (c) Numbers of tryptase-positive mast cells/mm2 in labial salivary gland tissue sections from patients with pSS and
control individuals. The number of mast cells was significantly greater in tissue from patients with pSS than in tissue from control individuals. Data are
shown as dot plots with mean ± standard error of the mean. Each dot represents a participant. ***p < .0001.
Figure 2. Relationships of tryptase-positive mast cell number with salivary function, fibrosis intensity, and local tissue inflammation in labial salivary
glands from patients with pSS. (a, b) A significant negative correlation was observed between Saxon test results and mast cell density in patients with
pSS, but not in control individuals. (c) There was no significant correlation between lymphoid infiltration intensity and mast cell number. (d) Mast cell
number and pathological fibrosis score were significantly correlated. Correlation coefficients and p-values are shown in each figure.Mast cells produce transforming growth factor β1 and promote tissue fibrosis 5
thus, we established in vitro cocultures of HMC-1 cells and
fibroblasts using an established Transwell system that prohib-
ited direct cell–cell contact and permitted separate analyses
of each cell type [27, 28]. Significant upregulation of Col1a
mRNA was observed in fibroblasts that had been cocultured
with HMC-1 cells for 7 days, compared with its expression in
fibroblast monocultures [Figure 4(a)]. Based on these results,
we hypothesized that mast-cell-derived soluble factors con-
tribute to fibroblast-mediated collagen synthesis and promote
tissue fibrosis in labial salivary glands during pSS-related
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab051/6363017 by guest on 06 November 2021
sialadenitis. To test our hypothesis, we generated HMC-1
conditioned medium for use in fibroblast cultures. HMC-1
cells have previously been reported to produce inflammatory
cytokines and chemokines upon treatment with recombinant
IL-33 and SCF [30]. In this study, fibroblasts were cul-
tured in HMC-1 conditioned medium or standard culture
medium for 24 h; Col1a mRNA expression was then eval-
Figure 3. Salivary gland mast cells are frequently in close proximity to uated by RT-PCR. As shown in Figure 4(b), the mRNA
fibroblastic regions in labial salivary glands from patients with pSS.
expression level of Col1a was significantly upregulated in
(a, b) Representative results of tryptase and Verhoeff–van Gieson
staining in serial sections of labial salivary glands from patients with pSS.
fibroblasts cultured in HMC-1 conditioned medium after IL-
Tryptase-positive mast cells (brown cells in a) are frequently in close 33/SCF stimulation, compared with fibroblasts in HMC-1
proximity to Verhoeff–van Gieson-stained fibroblastic lesions (b). Scale conditioned medium that had not been exposed to IL-33/SCF
bar, 100 µm. (c) Representative results of dual fluorescence stimulation and with fibroblasts in standard culture medium.
immunostaining for tryptase and vimentin in labial salivary glands from Col1a mRNA was upregulated in fibroblasts in an inverse pro-
patients with pSS. Single-staining images demonstrate tryptase-positive portion to the proportion of HMC-1 conditioned medium
mast cells (red cells) and vimentin-positive fibroblasts (green cells) in the
left and middle lower panels, respectively. Tryptase-positive mast cells
dilution in standard culture medium [Figure 4(c)]. These
were in close proximity to vimentin-positive fibroblasts in the merged results suggested that mast-cell-derived soluble factors pro-
image in the right lower panel. Nuclei were stained with mote fibroblast-mediated collagen synthesis.
4′ ,6-diamidino-2-phenylindole (DAPI) (blue). Scale bar, 100 µm.
Mast cells induce collagen synthesis in fibroblasts
through production of TGFβ1
that mast cells were involved in the reduction of salivary secre-
tion during sialadenitis associated with pSS. Furthermore, we Mast cells are reportedly a cellular source of TGFβ or TGFβ1
examined the association between the number of mast cells in systemic sclerosis, bone marrow fibrosis, and idiopathic
and lymphoid infiltration intensity, assessed by focus score. pulmonary lung fibrosis [18–20]. We examined the levels
There was no significant correlation between lymphoid infil- of transcripts for TGFβ1 in HMC-1 cells after 1 week of
tration intensity and mast cell density [R = 0.01545, p = .58, fibroblast coculture compared with HMC-1 monoculture. As
Figure 2(c)] in patients with pSS. The fibrosis of salivary demonstrated in Figure 5(a), significant elevation of TGFβ1
glands is a pathological element of pSS, which has been mRNA was observed in HMC-1 cells after 7 days of coculture
associated with reduced salivary flow [7]. A significant cor- with fibroblasts. Furthermore, HMC-1 cells stimulated with
relation was observed between the number of mast cells and recombinant IL-33 and SCF exhibited greater expression of
the degree of fibrosis in labial salivary glands obtained from TGFβ1 mRNA [Figure 5(b)]. Thus, we presumed that HMC-
patients with pSS [R = 0.5911, p = .0038, Figure 2(d)]. These 1-derived TGFβ1 could induce fibroblast-mediated collagen
results suggested that salivary resident mast cells could poten- synthesis. As demonstrated in Figure 5(c), fibroblasts cultured
tially contribute to the development of salivary tissue fibrosis, in HMC-1 conditioned medium exhibited significant upregu-
rather than the onset of lymphoid infiltration; this may lead lation of Col1a mRNA; treatment with neutralizing antibod-
to reduced salivary secretion. ies specific for TGFβ1 led to abrogation of this upregulation
effect [Figure 5(c)]. These results suggested that mast cells
induce collagen synthesis in fibroblasts through production of
Mast cells are frequently in close proximity to TGFβ1.
fibroblastic regions and fibroblasts
Histopathological analysis of serial sections demonstrated Salivary gland resident mast cells can produce
that tryptase-positive mast cells [brown cells in Figure 3(a)] TGFβ1
were often in close proximity to Verhoeff–van Gieson-stained
Finally, we examined whether salivary-gland-resident mast
fibrous tissue in labial salivary glands obtained from patients
cells could serve as a cellular source of TGFβ1 through dou-
with pSS [Figure 3(b)]. Furthermore, mast cells were located
ble immunofluorescence staining for tryptase and TGFβ1. As
near vimentin-positive fibroblasts [Figure 3(c)], with the
demonstrated in Figure 6, our in vitro findings were consistent
exception of focal lymphocyte accumulation in pSS-related
with in vivo staining results whereby tryptase-positive mast
sialadenitis, as in a previous report [21].
cells were found to express TGFβ1 (Figure 6, white arrows in
right lower panel). These results indicated that salivary-gland-
Mast cell-derived soluble factors promote resident mast cells produced TGFβ1, which contributed to
fibroblast-mediated type I collagen synthesis the development of tissue fibrosis by induction of fibroblast-
We hypothesized that mast cells contribute to the onset of mediated collagen synthesis during onset of pSS-related
tissue fibrosis by modulation of fibroblast immune function; sialadenitis.6 Kaieda et al.
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab051/6363017 by guest on 06 November 2021
Figure 4. Mast-cell-derived soluble factors induce type I collagen synthesis in fibroblasts. (a) Col1a mRNA expression in fibroblasts after coculture with
HMC-1 (coculture) or control monoculture for 7 days. (b) HMC-1 conditioned media were collected from HMC-1 cultures with or without IL-33/SCF
pretreatment and transferred into corresponding fibroblast cultures. Col1a mRNA expression levels were measured in fibroblasts cultured in HMC-1
conditioned medium, with or without IL-33/SCF pretreatment or after fibroblast monoculture, for 24 h. (c) Col1a mRNA expression levels were measured
in fibroblasts cultured in HMC-1 conditioned medium that had been diluted 1:3 in standard culture medium or after fibroblast monoculture. Data are
presented as the fold induction of Col1a mRNA expression after coculture or fibroblast monoculture using HMC-1 conditioned medium; triplicate wells
were examined in each culture condition. The expression of mRNA in fibroblasts grown in the monoculture condition was considered a fold induction of
1. Results are shown as mean ± standard error of the mean for data pooled from three (a, b) and two (c) independent experiments. *p < .05; **p < .01.
Discussion these two cell types [27, 28, 36]. A recent report demonstrated
In this study, we observed significantly greater numbers of that IL-33 expression was upregulated in labial salivary glands
mast cells in labial salivary gland samples in patients with in patients with pSS, which induced natural killer and natu-
pSS who exhibited sialadenitis, compared with control indi- ral killer T cells to produce interferon γ-perpetuating cellular
viduals. All human mast cells exhibit granules with abundant damage [38, 39]. Although the contributions of IL-33 to other
human tryptase-β bound to the proteoglycan matrix [31, 32]; immune cells (e.g. mast cells) during sialadenitis have not
no human has been identified who lacks mast cells, presum- been examined, IL-33 derived from labial salivary gland tis-
ably because their tryptase–serglycin proteoglycan complexes sue might contribute to mast cell accumulation in pSS-related
are essential for efficient control of bacterial and helminthic sialadenitis.
infections [33, 34]. Therefore, human tryptase-β can be used Our present results indicate that mast cells contribute to
as a relevant marker for salivary mast cells. The survival sialadenitis via induction of tissue fibrosis, rather than focal
of mast cells in peripheral tissue depends on signals from lymphoid inflammation. A previous investigation demon-
neighbouring cells; normal labial salivary glands primarily strated no significant correlation between lymphocytic infil-
contain connective tissue mast cells in close contact with tration and total mast cell number, whereas it found a
various resident cells (e.g. fibroblasts) [21]. Synovial-tissue- significant correlation between mast cell number and tis-
resident connective tissue mast cells are T-cell independent, sue fibrosis in labial salivary glands from patients with
while mucosal and connective tissue mast cells require mes- pSS [22]. Consistent with those findings, linear regres-
enchymal cell-membrane-bound c-kit ligand [26, 35, 36]. sion analysis revealed no significant positive correlation
In previous studies, salivary mast cells were found to be in between focus score and mast cell density. Accordingly,
proximity to fibroblasts, which implies that fibroblasts may active focal lymphocytic inflammation might not be accom-
support mast cell survival during sialadenitis [29]. Factors panied by salivary mast cell proliferation and altered
that regulate the accumulation of salivary mast cells have behaviour in pSS-related sialadenitis. Therefore, factors other
not been fully elucidated, but are presumably derived from than local lymphocytes (including activation of T and B
mesenchymal cells (e.g. fibroblasts). Among multiple fac- cells) may affect the behaviour of mast cells in sialadeni-
tors known to influence mast cell phenotype and behavior tis. An increase in mast cell number may be involved
in peripheral tissue, recent interest has focused on IL-33, in the development of chronic salivary tissue inflamma-
a pro- proinflammatory members of the IL-1 cytokine fam- tion triggered by lymphocytic sialadenitis and thus upreg-
ily [37]. IL-33 is expressed primarily by mesenchymal cells, ulation of salivary mast cells occurs after lymphocytic
such as fibroblasts; mast cells exhibit robust expression of aggregation.
the IL-33 receptor (ST2) [28]. We previously demonstrated Fibrosis, the result of excess collagen synthesis and depo-
that synovial fibroblasts induce mast cell granule maturation, sition, is a feature of many connective tissue diseases such
inflammatory cytokine production, and mast cell accumula- as systemic sclerosis [40]. A recent study indicated that sali-
tion in synovial tissues by inhibition of apoptosis via IL-33; vary gland fibrosis is a pathologic feature of pSS related to
in particular, we noted strong functional interactions between focal salivary gland inflammation, but is not solely causedMast cells produce transforming growth factor β1 and promote tissue fibrosis 7
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab051/6363017 by guest on 06 November 2021
Figure 5. Mast-cell-derived TGFβ1 induces fibroblast-mediated collagen synthesis. (a, b) RT-PCR was used to examine relative mRNA expression of
TGFβ1 in HMC-1 cells (1 × 106 /ml) after 1-week coculture of fibroblasts in the upper chamber and lower chambers, respectively, of a Transwell apparatus
(a) or after 24 h of stimulation with 50 ng/ml of recombinant human IL-33 and SCF (b). (c) Col1a mRNA expression levels were examined in fibroblasts
cultured in HMC-1 conditioned medium in the presence or absence of an anti-TGFβ1 antibody. Triplicate wells were examined. Results are shown as
mean ± standard error of the mean for data pooled from two independent experiments. *p < .05; **p < .01. N.S.: not significant (p > .05).
by ageing [7]. Although fibrosis is widely considered to be obtained from patients with SS; it also showed a signifi-
a progressive process, salivary gland fibrosis in pSS may cant correlation between neovascularization and the degree
not be progressive; no fibrotic progression was observed of tryptase-positive cell infiltration [42]. Additional studies
in longitudinal labial salivary gland biopsies that were col- are needed to explore the relationship between mast cells and
lected at a median of 4.5 years apart [41]. Salivary gland neovascularization.
tissue fibrosis remained unchanged over time, which sug- TGFβ1 is a key component in fibrosis; suppression of the
gests that chronic inflammation in pSS does not necessarily TGFβ1 isoform has been shown to considerably attenuate
lead to glandular tissue degeneration and replacement with fibrosis in a broad range of disease models, while enhanced
fibrosis. Because salivary gland tissue fibrosis is reportedly expression of TGFβ1 induces the onset of fibrosis [43]. Mast
associated with reduction of stimulated salivary flow, sup- cells are known to serve as a cellular source of TGFβ or
pression of fibrosis development in the early phase of the TGFβ1 in patients with systemic sclerosis, bone marrow
disease may offer new therapeutic avenues for patients with fibrosis, or idiopathic pulmonary fibrosis [18–20]. Impor-
pSS [10]. As demonstrated in Figure 4, conditioned medium tantly, we identified mast cells as a prominent cellular source
from activated HMC-1 cells induced fibroblast-mediated col- of TGFβ1 in the salivary glands; our in vitro findings empha-
lagen synthesis, similar to fibroblast coculture with HMC-1 size the potential contributions of mast cells to the onset
cells. These in vitro findings suggested a potential mast cell of tissue fibrosis by means of fibroblast-mediated collagen
contribution to labial salivary gland tissue fibrosis through synthesis. Because there is no established treatment to pre-
fibroblast-mediated induction of Type I collagen synthesis and vent salivary dysfunction in patients with pSS, therapeutic
impairment of salivary secretory function. Our results expand interventions to limit mast cell accumulation and suppress
the understanding of the integral relationship between mast TGFβ1 production could potentially attenuate labial salivary
cells and fibroblasts in labial salivary glands, which might pro- gland fibrosis and aid in the maintenance of salivary func-
mote fibrosis during sialadenitis. A previous study revealed tion. These observations imply a mechanism whereby salivary
that increased neovascularization is consistent with the sever- mast cells contribute to the onset of sialadenitis by inducing
ity of inflammatory lesions in labial salivary gland samples fibroblast-mediated collagen synthesis.8 Kaieda et al.
Tryptase TGFβ1
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab051/6363017 by guest on 06 November 2021
DAPI Merged
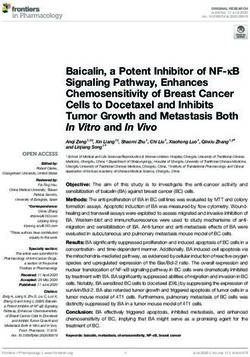
Figure 6. Salivary gland-resident mast cells could be a cellular source of TGFβ1 in labial salivary glands from patients with pSS. Representative images
of dual fluorescence immunostaining for mast cell tryptase (red) and TGFβ1 (green) in labial salivary glands from patients with pSS. Colocalization of
tryptase-positive mast cells and TGFβ1-positive cells was confirmed by dual fluorescence immunostaining. Double positive cells are indicated by white
arrows in the right lower panel. Nuclei were stained with DAPI (blue). Scale bar, 100 µm.
We acknowledge some potential limitations of this study. could occur in the early stages of pSS, therapeutic intervention
First, the sample size limited our analysis of patient out- to prevent mast-cell-induced fibrosis should be investigated in
comes and reduced the strength of our conclusions. Sec- future studies.
ond, our in vitro experiments did not investigate whether
direct contact with mast cells and fibroblasts is neces-
sary to promote fibrosis. It is difficult to maintain HMC- Acknowledgements
1/fibroblast coculture involving cell–cell contact for sev-
eral days. Direct cell–cell contact of HMC-1 cells with We thank Ryan Chastain-Gross, Ph.D., from Edanz Group
fibroblasts in vitro may result in fibroblast overstimulation. (https://en-author-services.edanzgroup.com/ac) for editing a
Finally, because TGFβ1 is potent at low concentrations and draft of this manuscript and helping to draft the abstract.
exhibits unpredictable effects, we were unable to measure
this cytokine consistently in extended coculture or HMC-
1 conditioned medium experiments. Therefore, we repeated Conflict of interest
our studies in the presence of blocking antibodies against None declared.
TGFβ1.
In conclusion, the numbers of mast cells were elevated in
patients with pSS-related sialadenitis; these cells were located
near fibroblasts and served as a cellular source of TGFβ1. Funding
Notably, TGFβ1 could induce Type 1 collagen synthesis This work was supported by a Grant-in-Aid for Scientific
in fibroblasts, which might actively contribute to fibrosis. Research (C) (No. 19K08898: S.K.) from the Ministry of
Because tissue fibrosis leading to a reduction in salivary flow Education, Culture, Science, Sports, and Technology.Mast cells produce transforming growth factor β1 and promote tissue fibrosis 9
References [23] Kohler PF, Winter ME. A quantitative test for xerostomia. The
Saxon test, an oral equivalent of the Schirmer test. Arthritis Rheum
[1] Rischmueller M, Tieu J, Lester S. Primary Sjogren’s syndrome. Best
1985;28:1128–32.
Pract Res Clin Rheumatol 2016;30:189–220.
[24] Greenspan JS, Daniels TE, Talal N et al. The histopathology of Sjo-
[2] Nakamura H, Shimizu T, Kawakami A. Role of viral infec-
gren’s syndrome in labial salivary gland biopsies. Oral Surg Oral
tions in the pathogenesis of Sjogren’s syndrome: different char-
Med Oral Pathol 1974;37:217–29.
acteristics of Epstein-Barr virus and HTLV-1. J Clin Med 2020;
9:1459–84. [25] Shin K, Nigrovic PA, Crish J et al. Mast cells contribute to autoim-
[3] Ice JA, Li H, Adrianto I et al. Genetics of Sjogren’s syndrome in mune inflammatory arthritis via their tryptase/heparin complexes.
the genome-wide association era. J Autoimmun 2012;39:57–63. J Immunol 2009;182:647–56.
[4] Odani T, Chiorini JA. Targeting primary Sjogren’s syndrome. Mod [26] Shin K, Gurish MF, Friend DS et al. Lymphocyte-independent
Rheumatol 2019;29:70–86. connective tissue mast cells populate murine synovium. Arthritis
Downloaded from https://academic.oup.com/mr/advance-article/doi/10.1093/mr/roab051/6363017 by guest on 06 November 2021
[5] Vitali C, Bombardieri S, Jonsson R et al. Classification criteria for Rheum 2006;54:2863–71.
Sjogren’s syndrome: a revised version of the European criteria pro- [27] Kaieda S, Wang JX, Shnayder R et al. Interleukin-33 primes
posed by the American-European Consensus Group. Ann Rheum mast cells for activation by IgG immune complexes. PLoS One
Dis 2002;61:554–8. 2012;7:e47252.
[6] Wynn TA, Ramalingam TR. Mechanisms of fibrosis: therapeutic [28] Kaieda S, Shin K, Nigrovic PA et al. Synovial fibroblasts pro-
translation for fibrotic disease. Nat Med 2012;18:1028–40. mote the expression and granule accumulation of tryptase via
[7] Leehan KM, Pezant NP, Rasmussen A et al. Minor salivary gland interleukin-33 and its receptor ST-2 (IL1RL1). J Biol Chem
fibrosis in Sjogren’s syndrome is elevated, associated with focus 2010;285:21478–86.
score and not solely a consequence of aging. Clin Exp Rheumatol [29] Konttinen YT, Tuominen S, Segerberg-Konttinen M et al.
2018;36:80–8. Mast cells in the labial salivary glands of patients with
[8] Llamas-Gutierrez FJ, Reyes E, Martinez B et al. Histopathological Sjogren’s syndrome: a histochemical, immunohistochemical,
environment besides the focus score in Sjogren’s syndrome. Int J and electron microscopical study. Ann Rheum Dis 1990;49:
Rheum Dis 2014;17:898–903. 685–9.
[9] Joachims ML, Leehan KM, Lawrence C et al. Single-cell analysis [30] Silver MR, Margulis A, Wood N et al. IL-33 synergizes with IgE-
of glandular T cell receptors in Sjogren’s syndrome. JCI Insight dependent and IgE-independent agents to promote mast cell and
2016;1:e85609. basophil activation. Inflamm Res 2010;59:207–18.
[10] Bookman AA, Shen H, Cook RJ et al. Whole stimulated salivary [31] Miller JS, Moxley G, Schwartz LB. Cloning and characterization
flow: correlation with the pathology of inflammation and dam- of a second complementary DNA for human tryptase. J Clin Invest
age in minor salivary gland biopsy specimens from patients with 1990;86:864–70.
primary Sjogren’s syndrome but not patients with sicca. Arthritis [32] Vanderslice P, Ballinger SM, Tam EK et al. Human mast cell
Rheum 2011;63:2014–20. tryptase: multiple cDNAs and genes reveal a multigene ser-
[11] Sisto M, Lorusso L, Ingravallo G et al. The TGF-beta1 sig- ine protease family. Proc Natl Acad Sci U S A 1990;87:
naling pathway as an attractive target in the fibrosis patho- 3811–5.
genesis of Sjogren’s syndrome. Mediators Inflamm 2018;2018: [33] Shin K, Watts GF, Oettgen HC et al. Mouse mast cell tryptase
1965935. mMCP-6 is a critical link between adaptive and innate immunity
[12] Adler S, Korner M, Forger F et al. Evaluation of histologic, sero- in the chronic phase of Trichinella spiralis infection. J Immunol
logic, and clinical changes in response to abatacept treatment 2008;180:4885–91.
of primary Sjogren’s syndrome: a pilot study. Arthritis Care Res [34] Huang C, De Sanctis GT, O’Brien PJ et al. Evaluation of the
2013;65:1862–8. substrate specificity of human mast cell tryptase beta I and demon-
[13] Tsuboi H, Matsumoto I, Hagiwara S et al. Effectiveness of abata- stration of its importance in bacterial infections of the lung. J Biol
cept for patients with Sjogren’s syndrome associated with rheuma- Chem 2001;276:26276–84.
toid arthritis. An open label, multicenter, one-year, prospec- [35] Galli SJ, Tsai M, Wershil BK. The c-kit receptor, stem cell factor,
tive study: ROSE (Rheumatoid Arthritis with Orencia Trial and mast cells. What each is teaching us about the others. Am J
toward Sjogren’s syndrome Endocrinopathy) trial. Mod Rheuma- Pathol 1993;142:965–74.
tol 2016;26:891–9. [36] Wang JX, Kaieda S, Ameri S et al. IL-33/ST2 axis promotes
[14] Lyons DO, Pullen NA. Beyond IgE: alternative mast cell activation mast cell survival via BCLXL. Proc Natl Acad Sci U S A
across different disease states. Int J Mol Sci 2020;21:1498–513. 2014;111:10281–6.
[15] Costela-Ruiz VJ, Illescas-Montes R, Pavon-Martinez R et al. Role [37] Schmitz J, Owyang A, Oldham E et al. IL-33, an interleukin-
of mast cells in autoimmunity. Life Sci 2018;209:52–6. 1-like cytokine that signals via the IL-1 receptor-related protein
[16] Theoharides TC, Alysandratos KD, Angelidou A et al. Mast cells ST2 and induces T helper type 2-associated cytokines. Immunity
and inflammation. Biochim Biophys Acta 2012;1822:21–33. 2005;23:479–90.
[17] Crisp AJ, Chapman CM, Kirkham SE et al. Articular mastocytosis [38] Awada A, Nicaise C, Ena S et al. Potential involvement of the IL-
in rheumatoid arthritis. Arthritis Rheum 1984;27:845–51. 33-ST2 axis in the pathogenesis of primary Sjogren’s syndrome.
[18] Hugle T, Hogan V, White KE et al. Mast cells are a source of trans- Ann Rheum Dis 2014;73:1259–63.
forming growth factor beta in systemic sclerosis. Arthritis Rheum [39] Jung SM, Lee J, Baek SY et al. The Interleukin 33/ST2 axis in
2011;63:795–9. patients with primary Sjogren syndrome: expression in serum
[19] Nakayama S, Yokote T, Hiraoka N et al. Transforming growth and salivary glands, and the clinical association. J Rheumatol
factor beta- and interleukin 13-producing mast cells are associated 2015;42:264–71.
with fibrosis in bone marrow. Hum Pathol 2017;62:180–6. [40] Krieg T, Abraham D, Lafyatis R. Fibrosis in connective tissue dis-
[20] Shimbori C, Upagupta C, Bellaye PS et al. Mechanical stress- ease: the role of the myofibroblast and fibroblast-epithelial cell
induced mast cell degranulation activates TGF-beta1 signalling interactions. Arthritis Res Ther 2007;9:S4.
pathway in pulmonary fibrosis. Thorax 2019;74:455–65. [41] Kapsogeorgou EK, Christodoulou MI, Panagiotakos DB et al.
[21] Konttinen YT, Hietanen J, Virtanen I et al. Mast cell derangement Minor salivary gland inflammatory lesions in Sjogren syndrome:
in salivary glands in patients with Sjogren’s syndrome. Rheumatol do they evolve? J Rheumatol 2013;40:1566–71.
Int 2000;19:141–7. [42] Sisto M, Lisi S, Ingravallo G et al. Neovascularization is prominent
[22] Skopouli FN, Li L, Boumba D et al. Association of mast in the chronic inflammatory lesions of Sjogren’s syndrome. Int J
cells with fibrosis and fatty infiltration in the minor salivary Exp Pathol 2014;95:131–7.
glands of patients with Sjogren’s syndrome. Clin Exp Rheumatol [43] Gyorfi AH, Matei AE, Distler JHW. Targeting TGF-beta signaling
1998;16:63–5. for the treatment of fibrosis. Matrix Biol 2018;68–69:8–27.You can also read