London Resilience Pandemic Influenza Response Plan - VERSION 5.0 JULY 2012 - NOT PROTECTIVELY MARKED
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below
NOT PROTECTIVELY MARKED London Resilience Partnership London Resilience Pandemic Influenza Response Plan VERSION 5.0 JULY 2012
NOT PROTECTIVELY MARKED
PAGE LEFT INTENTIONALLY BLANK
REGIONAL WN
FRAMEWORK
DRAFT
London Resilience Pandemic Influenza Response Plan 2 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
TABLE OF CONTENTS
Section One: Introduction ..................................................................................................................... 3
Aim of this document................................................................................................................... 3
Objectives of this document ........................................................................................................ 3
Audience ...................................................................................................................................... 3
Security Classification .................................................................................................................. 3
Queries......................................................................................................................................... 3
Section Two: Background ...................................................................................................................... 4
Influenza ...................................................................................................................................... 4
Pandemic Influenza ................ ......................................................................................................4
Avian Influenza ............................................................................................................................ 6
Influenza A/H1N1v (Swine influenza).............................................................................. ............6
Section Three: Planning Assumptions.................................................................................................... 8
UK Influenza Pandemic Preparedness Strategy 2011 ................................................................... 8
Planning and Response Phases ................................................................................................... 8
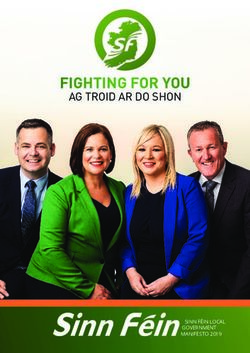
Table 1: WHO Pandemic Influenza Phases ................................................................................... 9
National Planning Assumptions.................................................................................................. 10
Responding to an Influenza pandemic
Staff absence
Additional Planning Assumptions ............................................................................................... 11
Deaths
Pharmaceutical Interventions
International travel and border restrictions
Isolation, quarantine and social distancing
Infection control, hygiene, facemasks
Public Gatherings
School closures
Mutual aid
Vulnerable People and Social Care ............................................................................................. 15
Section Four: Planning and Preparedness............................................................................................ 16
Business Continuity and Resilience Planning.............................................................................. 16
Multi-Agency Planning and Preparedness ................................................................................. 17
Table 4: Organisational Responsibilities in Planning and Preparedness ...................................... 19
Section Five: Early Response – Detect and Assess ............................................................................... 23
Rising Tide Emergency Response Escalation
Membership of the London Partnership during a Flu Pandemic
Influenza Pandemic Committee (Response)
Table 5: Organisational Responsibilities in the early response..................................... .......... .....26
Section Six: Pandemic Response – Treat and Escalate ........................................................................ .30
London Reporting and Co-ordination Arrangements ................................................................ 30
Cabinet Office Briefing Room (COBR) and Civil Contingencies Committee (CCC) ...................... 30
London Local Resilience Forum
Influenza Pandemic Committees (Response)
Table 6: Activation and Action Chart in WHO Phase 6.................................... ......... ..................32
Section Seven: Reports and Returns .................................................................................................... 39
Daily Schedule............................................................................. ........... ...................................39
London Resilience Pandemic Influenza Response Plan 3 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
Diagram 1: Information flows during an Influenza Pandemic .................................................... .40
Section Eight: Reconstitution and Recovery ........................................................................................ 41
Additional Waves and Reconstitution......................................................................................... 41
Central Government Actions in the Reconstitution Phase .......................................................... 41
Recovery .................................................................................................................................... 42
Central Government Actions in the Recovery Phase ................................................................... 42
London Local Resilience Forum Actions in the Recovery Phase ................................................. 42
Annexes ............................................................................................................................................. 43
Annex 1: Summary of Key Planning and Guidance Documents ....................................... 44
Annex 2: Guidance for Multi-Agency Influenza Pandemic Committees (IPC) in
London ............................................................................................................ 45
Annex 3: Pandemic Influenza Communication Strategy .................................................. 53
Annex 4: The Ethical Dimension ..................................................................................... 62
Annex 5: Membership of the London Local Resilience Forum........... .......... ....................64
Annex 6: Glossary of Abbreviations.......................................................................65
London Resilience Pandemic Influenza Response Plan 4 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
VERSION CONTROL
Version Date Change (owner)
1 May 2006 Version 1 agreed at the meeting of the London Regional Resilience
Forum (LRRF)
2 2007 Updated to reflect changes in command and control arrangements
and updated guidance and planning assumptions
3 2007 Took into consideration further guidance issued by the Department
of Health and Cabinet Office
4 March Incorporated recommendations following a national review of multi
2009 agency planning and was utilised in the 2009/10 pandemic
5 May 2012 Includes learning from the multi-agency debrief following the
2009/10 pandemic as well as the revised National Pandemic
Influenza Strategy. It also takes account of Government changes
effective from May 2010 including transition of the London
Resilience Team from the former Government Office for London to
the Greater London Authority, and significant changes to the NHS
landscape.
London Resilience Pandemic Influenza Response Plan 5 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
SECTION ONE – INTRODUCTION
AIM OF THIS DOCUMENT
1.1 The aim of this document is to provide the agencies that make up the London Resilience
Partnership with a strategic framework to support their integrated preparedness and
response to pandemic influenza.
1.2 Underlying this aim is the need to minimise, where possible, social and economic
disruption for the population of London in the event of an outbreak of pandemic
influenza.
OBJECTIVES OF THIS DOCUMENT
1.3 To summarise and collate the key plans and procedures which would be activated in the
event of an outbreak of pandemic influenza.
1.4 To give an overview of the response to ensure understanding within the London
Resilience Partnership.
1.5 To outline roles and responsibilities of agencies.
AUDIENCE
1.6 This document is intended for all agencies and organisations represented within the
London Resilience Partnership who would have a role to play in planning for and
responding to pandemic influenza.
SECURITY CLASSIFICATION
1.7 Once this document has been approved by the London Local Resilience Forum (LLRF) it
will not carry a protective marking and can therefore be shared with interested parties.
In order to make this document accessible to all those with an interest it can be found
on the internet at: www.londonprepared.gov.uk.
QUERIES
1.8 For any comments or queries concerning this document, please contact the London
Resilience Team on 0207 983 4000
London Resilience Pandemic Influenza Response Plan 6 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
SECTION TWO – BACKGROUND
INFLUENZA
2.1 Influenza is an acute infectious viral illness that spreads rapidly from person to person
when in close contact. It is characterised by the sudden onset of fever, chills, headache,
muscle pain, severe prostration and usually a cough – with or without a sore throat – or
other respiratory symptoms. The acute symptoms generally last about a week, although
a full recovery may take longer.
2.2 There are three types of influenza viruses – A, B and C:
Influenza A viruses cause most winter epidemics (and all pandemics) and affect a
wide range of animal species as well as humans. The natural reservoir for influenza
A viruses is wild aquatic shorebirds. Influenza A viruses have a propensity towards
adaptation and change – this is one factor that enables them to remain in
circulation year on year in slightly different form that can have widely differing
impacts on human populations.
Influenza B viruses only infect humans. They circulate most winters but generally
cause less severe illness and smaller outbreaks; their effect is most often seen in
children.
Influenza C viruses are amongst the many causes of the common cold.
2.3 Influenza is one of the most difficult infectious diseases to control because the virus
spreads easily via the respiratory route when an infected person talks, coughs or
sneezes. It also spreads through close contact or hand-to-face contact if hands are
contaminated.
2.4 The incubation period (from the time of infection to first symptoms) is in the range of
one to four days, typically two to three. People are generally considered to be infectious
whilst they are symptomatic and infectiousness mirrors symptom severity. People are
most infectious soon after they develop symptoms and are highly infectious for four to
five days from the onset of symptoms (longer in children and those who are immuno-
compromised).
2.5 The balance of evidence points to transmission by droplet and through direct and
indirect contact as the most important routes, however virus can also be spread through
infectious aerosolised particles, although the potential contribution of these (particularly
outside the healthcare setting) is unclear.
2.6 Transmission of the influenza virus can be reduced through the following actions:
Strict adherence to infection control practices, especially hand hygiene,
containment of respiratory secretions and the use of Personal Protective
Equipment (PPE)
Administrative controls such as separation or cohorting of patients with influenza
Instructing staff members with respiratory symptoms to stay at home and not
come in to work
Education of staff and general awareness raising of the need to regularly clean the
office environment.
London Resilience Pandemic Influenza Response Plan 7 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
PANDEMIC INFLUENZA
2.7 An influenza pandemic occurs when a novel influenza virus emerges against which the
human population has little or no immunity; global spread is thus considered inevitable.
A future pandemic could occur at any time. Intervals between the recent pandemics
have varied from 10 to 40 years with no recognisable pattern.
2.8 A future pandemic could originate anywhere in the world although South East Asia, the
Middle East and Africa are widely considered to be the most likely potential sources. The
virus could rapidly reach the UK and it could then take only one to two weeks until
sporadic cases and small clusters acting as initiators of local epidemics are occurring
across the whole country. The 2009/10 pandemic proved that the virus could reach the
UK more rapidly than this, but internal spread could be slower. The measures put in
place by regions (including London) where the first cases were reported, meant that
spread across the UK to major population centres was slower than this (see later).
2.9 As most people will have no immunity to the pandemic virus, infection and illness rates
may be higher than during seasonal influenza epidemics. Modelling based on previous
pandemics indicates that a substantial percentage of the world’s population could
require some form of medical care during a pandemic. Influenza poses a serious danger
for high-risk groups (such as the very young, the elderly and the chronically ill and some
disabled people). However, in previous pandemics hospitalization and deaths have also
occurred in healthy younger people.
2.10 The clinical attack rate of the illness will only become evident as person-to-person
transmission develops, but response plans should recognise the possibility of up to 50%
in a single wave pandemic. Up to 4% of those who are symptomatic may require hospital
admission if sufficient capacity were to be available.
2.11 Without intervention, and with no significant immunity in the population, historical
evidence suggests that one person infects about 1.4 to 1.8 people on average. This
number is likely to be higher in closed communities such as prisons, residential homes or
boarding schools.
2.12 All ages are likely to be affected but children and otherwise fit adults could be at
relatively greater risk as older people may have some residual immunity from possible
previous exposure to a similar virus earlier in their lifetime
2.13 Although the potential for age-specific differences in the clinical attack rate should be
noted, they are impossible to predict, and a uniform attack rate across all age groups is
assumed for planning purposes. More severe illness than seen with seasonal influenza is
possible in all population groups, rather than predominantly in high risk groups as with
seasonal influenza. A higher number of people than usual may develop severe
prostration and/or rapidly fatal viraemia, viral pneumonia or secondary complications. It
is not possible to predict these numbers in advance
2.14 Past pandemics have varied in scale, severity and consequence, although in general their
impact has been much greater than that of even the most severe winter ‘epidemic’.
Although little information is available on earlier pandemics, the three that occurred in
the 20th century are well documented. The worst (often referred to as ‘Spanish flu’)
occurred in 1918/19. It caused serious illness, an estimated 20–40 million deaths
worldwide (with peak mortality rates in people aged 20–45) and major disruption. Whilst
the pandemics in 1957 and 1968 (often referred to as Asian and Hong Kong flu
London Resilience Pandemic Influenza Response Plan 8 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
respectively) were much less severe, they also caused significant illness levels and an
estimated 1–4 million deaths between them. The 2009/10 pandemic is reported to have
caused around 18,500 confirmed deaths globally, however there is no published
estimate of the overall number of cases.
2.15 In addition to their potential to cause serious harm to human health, pandemics threaten
wider social and economic damage and disruption. Social disruption may be greatest
when rates of absenteeism impair essential services.
2.16 A pandemic may occur over one or more waves of around 15 weeks, each some weeks or
months apart of which the second or a subsequent wave could be more severe than the
first. Previous pandemics have had up to three waves that occurred over two years; the
2009/10 pandemic had two waves in the UK before the virus became one of the
circulating seasonal viruses.
AVIAN INFLUENZA
2.17 Avian influenza (‘bird flu’) is an infectious disease of birds caused by influenza A viruses.
It is spread between birds (and occasionally to humans) mainly through contact with
contaminated faeces but also via respiratory secretions or contaminated blood. Although
they do not readily infect species other than birds and pigs, scientists believe that
human-adapted avian viruses were the most likely origin of at least two of the last four
human influenza pandemics.
2.18 The highly pathogenic avian influenza A/H5N1 virus has caused concern for over a
decade, due to its highly contagious nature amongst domestic poultry species. Whilst
the virus has also infected humans, such infections have only been detected in a small
proportion of those who have been exposed to infected birds. To date, there has only
been limited evidence of person-to-person transmission and, even where that has
occurred; it has been with difficulty and has not been sustained.
2.19 A growing reservoir of infection in birds (for example the virus is recognised as being
endemic in Egypt, India, Bangladesh, Viet Nam, China, and Indonesia), combined with
transmission to more people over time, increases the opportunities for the A/H5N1 virus
either to adapt to give it greater affinity to humans or to exchange genes with a human
influenza virus to produce a completely novel virus capable of spreading easily between
people and causing a pandemic. However, the likelihood and time span required for such
mutations are not possible to predict.
2.20 Experts agree that A/H5N1 is not necessarily the most likely virus to develop pandemic
potential. However, due to the potential severity of a pandemic originating from an
A/H5N1 virus, this possibility cannot be discounted and the virus remains a key concern.
INFLUENZA A/H1N1V (SWINE INFLUENZA)
2.21 The world first became aware of cases caused by a novel influenza virus, influenza
A/H1N1v, at the end of April 2009. The World Health Organisation (WHO) raised the
global pandemic alert level from WHO Phase 3 to WHO Phase 5 over five days in late
April 2009. Phase 6 was declared by WHO on 11 June 2009 and signalled the start of
the first pandemic of the 21st century.
2.22 The first UK cases were reported in Scotland on 27 April 2009, and the first London case
on 30 April 2009. Initially the pandemic was managed through containment measures
such as treating cases and some school closures. As case numbers increased, this was
London Resilience Pandemic Influenza Response Plan 9 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
followed by outbreak management (limited prophylaxis and contact tracing) before the
UK entered the treatment phase (no prophylaxis or contact tracing).
2.23 Most people who contracted the swine flu virus were mildly affected and were treated
with antivirals, over the counter medicines, bed rest and fluids. However some cases
were more serious and required acute hospital care. There were less than 100 deaths as
a result of this virus recorded in London during the pandemic.
2.24 The majority of swine flu cases were in younger age groups than those usually affected
by seasonal flu. Pregnant women and morbidly obese people were unanticipated risk
groups. A number of cases and deaths were of people with no previously identified
underlying condition.
2.25 Cases in London peaked in July 2009. A second wave started in autumn 2009 and
peaked in November, coinciding with the usual winter pressures of cold weather and
seasonal illness. The 2010/11 winter season in the UK was dominated by the A/H1N1v
virus as part of the range of influenza viruses circulating that winter. It is likely to
continue to circulate and cause seasonal outbreaks until replaced by another dominant
strain.
London Resilience Pandemic Influenza Response Plan 10 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
SECTION THREE – PLANNING ASSUMPTIONS
UK INFLUENZA PANDEMIC PREPAREDNESS STRATEGY 2011
3.1 The 2007 DH guidance included significant detail on potential attack rates, fatality rates
and impact of a future pandemic on the UK. These were used to inform local and
regional planning; however the 2009/10 pandemic had characteristics that were very
different to those which had been modelled.
3.2 The 2011 National Strategy includes a number of key planning assumptions for
pandemic preparedness. These are fewer and less detailed than those which were
included in the 2007 Framework, reflecting the uncertainty about scale, severity and
development of any future pandemic.
3.3 The overall objectives of the UK’s approach to pandemic influenza preparedness are to:
minimise the potential health impact of a future influenza pandemic
minimise the potential impact of a pandemic on society and the economy
instil and maintain trust and confidence.
These are underpinned by three key principles: a precautionary approach, proportionality
and flexibility.
The precautionary approach refers to the fact that in the initial stages of a
pandemic it is unlikely to be possible to assess or predict with any accuracy the
severity or impact of the virus. Robust data from early UK cases will be essential in
informing and tailoring the UK response
As more information becomes available, a proportional response to the
pandemic can be ensured in accordance with whether the impact is perceived as
Low, Moderate or High impact
Flexibility was recognised as essential to the 2009/10 pandemic response. The
2009/10 pandemic highlighted the need for the UK to be able to act in response
to the national situation, rather than in line with pre-determined global structures.
Additionally, the response across the UK required significant local variability as the
impact waxed and waned across areas.
3.4 Pandemic preparedness and response will continue to be evidence based, based on
ethical principles, based on established practices and systems as far as possible, across
the whole of society, and coordinated at local, national and international levels.
PLANNING AND RESPONSE PHASES
3.5 The World Health Organisation (WHO) has identified six phases in the progression of an
influenza pandemic, from the first emergence of a novel influenza virus to a global
pandemic being declared (Table 1). The WHO’s global classification, based on the
overall international situation, is used internationally for planning purposes.
3.6 National, regional and local plans in the UK that were activated in response to the
2009/10 pandemic followed the WHO Phases, and also referred to a set of four UK Alert
Levels (no longer used) that further sub-divided WHO Phase 6. However, this did not
prove useful during the 2009/10 pandemic when transition between the WHO Phases
proved to be rapid and the UK was facing more severe challenges than other parts of the
world before WHO declared Phase 6.
London Resilience Pandemic Influenza Response Plan 11 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
Table 1: WHO Pandemic Influenza Phases
3.7 The 2011 UK Strategy recognises the need to disassociate the UK response from the
global WHO Phases and instead refers to five phases named: Detection, Assessment,
Evaluate, Treatment, Escalation and Recovery.
3.8 The phases are not numbered as they are not linear, may not follow in strict order, and it
is possible to move back and forth or jump phases. It should also be recognised that
there may not be a clear delineation between phases, particularly when considering
regional variation and comparisons.
3.9 Detection - this phase would commence either on the declaration of the current WHO
phase 4 or earlier on the basis of reliable intelligence or if an influenza-related ‘Public
Health Emergency of International Concern’ is declared by the WHO. The focus in this
stage would be intelligence gathering from countries already affected, enhanced
surveillance within the UK, developing diagnostics specific to the new virus, and
providing information and communications to the public and professionals. The indicator
for moving to the next stage would be the identification of the new influenza virus in
patients in the UK.
3.10 Assessment – the focus of this stage would be collection of detailed clinical and
epidemiological information on early cases on which to base early estimates of impact
and severity in the UK. Additionally it will focus on reducing the risk of transmission and
infection with the virus within the local community by actively finding cases, self
isolation of cases and suspected cases, treating cases/ suspected cases and using
antiviral prophylaxis for close/ vulnerable contacts, based on a risk assessment of the
possible impact of the disease. The indicator for moving from this stage would be
evidence of sustained community transmission of the virus, ie cases not linked to any
known or previously identified cases.
3.11 These two stages – Detection and Assessment – together form the initial response.
This may be relatively short and the phases may be combined depending on the speed
with which the virus spreads, or the severity with which individuals and communities are
affected. It will not be possible to halt the spread of a new pandemic influenza virus, and
it would be a waste of public health resources and capacity to attempt to do so.
3.12 Treatment - The focus of this phase would be treatment of individual cases and
population treatment via the NPFS (if necessary), enhancement of the health response
London Resilience Pandemic Influenza Response Plan 12 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
to deal with increasing numbers of cases, considering enhancing public health measures
to disrupt local transmission of the virus, such as localised school closures based on
public health risk assessment. Depending on the development of the pandemic, this time
should also be used to prepare for targeted vaccinations as the vaccine becomes
available. Arrangements will be activated to ensure that necessary detailed surveillance
activity continues in relation to samples of community cases, hospitalised cases and
deaths. When demands for services start to exceed the available capacity, additional
measures will need to be taken. This decision is likely to be made at a pan London or
local level as not all parts of the UK will be affected at the same time or to the same
degree of intensity.
3.13 Escalation – the focus of this stage would be escalation of surge management
arrangements in health and other sectors, prioritisation and triage of service delivery
with the aim to maintain essential services, resiliency measures, encompassing robust
contingency plans, and consideration of de-escalation of response if the situation is
judged to have improved sufficiently.
3.14 These two stages form the Treatment phase of the pandemic. Whilst escalation measures
may not be needed in mild pandemics, it would be prudent to prepare for the
implementation of the Escalation phase at an early stage of the Treatment phase, if not
before
3.15 Recovery – the focus of this stage would be normalisation of services, perhaps to a
new definition of what constitutes normal service; restoration of business as usual
services, including an element of catching-up with activity that may have been scaled-
down as part of the pandemic response e.g. re-schedule routine operations; post-
incident review of response, and sharing information on what went well, what could be
improved and lessons learnt; taking steps to address staff exhaustion; planning and
preparing for a resurgence of influenza, including activities carried out in the Detection
phase; continuing to consider targeted vaccination, when available; and preparing for
post-pandemic seasonal influenza. The indicator for this phase would be when influenza
activity is either significantly reduced compared to the peak or when the activity is
considered to be within acceptable parameters. An overview of how services’ capacities
are able to meet demand will also inform this decision.
NATIONAL PLANNING ASSUMPTIONS
3.15 The 2011 strategy planning assumptions are based on the Scientific Pandemic Influenza
Advisory Committee’s Modelling Sub-Group Summary (annex 1) (available at
www.dh.gov.uk/ab/SPI/DH_095904). Below find a summary on some relevant aspects :
Responding to an influenza pandemic
The UK will continue to maintain stockpiles and distribution arrangements for
antiviral medicines and antibiotics sufficient for a widespread and severe pandemic.
Health services should continue to prepare for up to 30% of symptomatic patients
requiring assessment and treatment in usual pathways of primary care (assuming the
majority of symptomatic cases do not require direct assistance from healthcare
professionals).
Between 1% and 4% of symptomatic patients will require hospital care, depending
on how severe the illness caused by the virus is.
For deaths, the analysis remains that up to 2.5% of those with symptoms would die
as a result of influenza if no treatment proved effective. These figures might be
expected to be reduced by the impact of countermeasures but the effectiveness of
such mitigation is not certain. The combination of particularly high attack rates and a
severe disease is also relatively (but unquantifiably) improbable. Taking account of
London Resilience Pandemic Influenza Response Plan 13 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
this, and the practicality of different levels of response, when planning for excess
deaths, local planners should prepare to extend capacity on a precautionary but
reasonably practicable basis, and aim to cope with a population mortality rate of up
to 210,000 – 315,000 additional deaths, possibly over as little as a 15 week period
and perhaps half of these over three weeks at the height of the outbreak. More
extreme circumstances would require the local response to be combined with
facilitation or other support at a national level. In a less widespread and lower impact
influenza pandemic, the number of additional deaths would be lower.
Staff absence
Up to 50% of the workforce may require time off at some stage over the entire
period of the pandemic. In a widespread and severe pandemic, affecting 35%- 50%
of the population, this could be even higher as some with caring responsibilities will
need additional time off.
Staff absence should follow the pandemic profile. In a widespread and severe
pandemic, affecting 50% of the population, between 15% and 20% of staff may be
absent on any given day. These levels would be expected to remain similar for one to
three weeks and then decline.
Some small organisational units (5 to 15 staff) or small teams within larger
organisational units where staff work in close proximity are likely to suffer higher
percentages of staff absences. In a widespread and severe pandemic, affecting 50%
of the population, 30%-35% of staff in small organisations may be absent on any
given day.
Additional staff absences are likely to result from other illnesses, taking time off to
provide care for dependants, to look after children in the event of schools nurseries
closing, family bereavement, practical difficulties in getting to work and/or other
psychosocial impacts.
ADDITIONAL PLANNING ASSUMPTIONS
Deaths
3.16 An influenza pandemic may result in a large number of deaths throughout London. It is
possible (although unlikely) that a pandemic influenza virus could have a 50% clinical
attack rate and a 2.5% case fatality rate (the theoretical worst case scenario based on
previous pandemics). For London, this means planning for over 90,0001 excess deaths
over the full duration of the pandemic. As agreed by the London Local Resilience Forum,
Local Authorities have plans in place to meet the medium case scenario of approximately
36,000 deaths, which they can achieve within local resources and to existing standards .
In the event of deaths exceeding that range, London’s Local Authorities are likely to
require additional resources and guidance to cope with the additional demand,
particularly relating to the storage and disposal of such large numbers of bodies in a
consistent and acceptable manner.
3.17 The projected scale of excess deaths during a pandemic particularly at the upper end of
the planning assumptions is likely to present many challenges for local services. Planning
in both the local health community and Local Authorities will need to recognise the
requirement for sensitive and sympathetic management of potentially large numbers of
deaths.
3.18 The Home Office is the lead government department for policy on managing excess
1
Figure based on National Statistics 2007 mid-year population estimate of approximately 7,500,000 for London.
London Resilience Pandemic Influenza Response Plan 14 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
deaths and has published guidance on different ways of working to manage excess
deaths. This guidance can be located at
www.ukresilience.gov.uk/news/manage_deaths_guidance2.aspx
3.19 At the local level, responsibility for managing excess deaths lies with the Local Authority.
Local Authorities’ plans should be carefully coordinated with those of other Category 1
and 2 responders and private organisations.
3.20 At the pan London level, a London Excess Deaths Task and Finish Group was established
to develop a strategic, multi-agency London Excess Deaths Plan. The plan provides
guidance on different ways of working with respect to funeral services, burials and
cremations, coroners, death registration and mortuary capacity. Version 2 was published
in March 2010. Due to its protective nature, the plan is not publicly available. However
a local authority toolkit has been published and is available to all Category 1 and 2
responders, on request from LRT.
PHARMACEUTICAL INTERVENTIONS
3.20 A range of pharmaceutical interventions are available to prevent, treat and reduce the
consequences of pandemic influenza. These can be broadly categorised as vaccination
(pandemic specific and pre-pandemic), antiviral medication (treatment and prophylaxis)
and antibiotics.
3.21 Vaccines currently offered for protection against seasonal influenza are unlikely to
protect against a new or modified virus and it is impossible to develop a specific vaccine
until the pandemic influenza virus has been identified. While the Government has agreed
advance purchase agreements with manufacturers to produce pandemic specific vaccine,
it will nevertheless take up to six months for sufficient quantities to become available.
Therefore it is improbable that a vaccine will contribute to reducing the impact of an
initial wave of a pandemic. When developed, distribution of the vaccine will be
implemented following national guidance developed by the Department of Health.
3.22 Pre-pandemic vaccination with an influenza virus related but not specific to the
pandemic strain might offer some limited protection. Currently, there are very limited
stocks of an A/H5N1 vaccine purchased specifically for the protection of healthcare
workers that could be used in the event that a pandemic caused by this virus appears
imminent. Pre-pandemic vaccination of those most likely to spread the disease or suffer
complications could also help reduce hospitalisations and deaths in vulnerable groups.
Decisions on use would be made following assessments undertaken at the time of the
pandemic; however, response plans should consider arrangements for limited pre-
pandemic vaccination of targeted groups.
3.23 Antiviral medicines and other definitive pharmaceutical interventions are important
countermeasures, although they may be in limited supply. The UK has established
national stockpiles of oseltamivir (Tamiflu®) and zanamivir (Relenza®) that allow for the
treatment of all symptomatic patients at clinical rates of up to 50%.
3.24 Arrangements to make antiviral treatment rapidly available to symptomatic individuals
are a critical part of the health response. This will be particularly important before a
specific pandemic vaccine is widely available. Higher clinical attack rates may require
prioritisation of use, but operational plans should initially aim to make antiviral
medicines available to all patients who have been symptomatic for less than 48 hours
from reporting symptoms indicative of influenza.
London Resilience Pandemic Influenza Response Plan 15 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
3.25 Antibiotics are an important pharmaceutical countermeasure to treat bacterial
pneumonia, which may be an important secondary complication of pandemic influenza.
The government has procured a stockpile of antibiotics for this purpose.
INTERNATIONAL TRAVEL AND BORDER RESTRICTIONS
3.38 The movement of people is a significant determinant of the speed of spread of
infectious diseases, and as a major destination and international travel hub, the UK is
particularly vulnerable. The possible health benefits that may accrue from international
travel restrictions or border closures need to be considered in the context of the
practicality, proportionality and potential effectiveness of imposing them, and balanced
against their wider social and economic consequences.
3.39 Modelling suggests that even a 99% restriction on travel into the UK immediately a
pandemic virus is identified could only be expected to delay the importation of the virus
by up to two months. Given the complexity of this issue, the Government will keep
under review the evidence on the benefits and disadvantages of the various approaches.
Any decision that is taken in relation to restricting travel will be taken at national level.
ISOLATION, QUARANTINE AND SOCIAL DISTANCING
3.40 Whilst it might be possible to isolate initial cases and quarantine their immediate
contacts, such an approach will become unsustainable after the first few hundred cases
and is unlikely to be particularly effective. However, spread across the UK was slowed by
the intensive containment measures (treatment, prophylaxis and contact tracing)
undertaken in London and the West Midlands at the start of the 2009/10 outbreak.
INFECTION CONTROL, HYGIENE, FACEMASKS
3.41 Applying basic infection control measures and encouraging compliance with public
health advice are likely to make an important contribution to the UK’s overall response.
Simple measures will help individuals to protect themselves and others.
These include:
staying at home when ill
covering the nose and mouth with a tissue when coughing or sneezing
disposing of dirty tissues promptly and carefully – bagging and binning them
washing hands frequently with soap and warm water to reduce the spread of the
virus from the hands to the face, or to other people, particularly after blowing the
nose or disposing of tissues
cleaning frequently touched hard surfaces (e.g. kitchen worktops, door handles)
regularly using normal cleaning products
avoiding crowded gatherings where possible, especially in enclosed spaces
if suffering with influenza symptoms, wearing a disposable face mask to protect
others should it become absolutely essential to go out (e.g. to go to hospital)
making sure that children follow this advice.
3.42 Although the perception that it may be beneficial to wear a face mask, especially in
London Resilience Pandemic Influenza Response Plan 16 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
public places, is widely held, there is little actual evidence of proportionate benefit from
widespread use. The Government will not therefore stockpile face masks for general use.
If individuals who are not symptomatic choose to purchase and wear face masks in
public places, they should be worn properly and disposed of safely to reduce infection
spread.
Although further clarification and guidance on the use of face masks may become
available in due course, the planning presumptions should be that anyone who is ill with
influenza-like symptoms will be advised to stay at home.
PUBLIC GATHERINGS
3.42 Large public gatherings or crowded events where people may be in close proximity are
an important indicator of ‘normality’ and can help maintain public morale during a
pandemic. Whilst close contact with others – especially in a crowded confined space –
accelerates the spread of an influenza virus, there is little direct evidence of the benefits
or effects of cancelling such gatherings or events. Individuals may benefit from reduced
exposure by not attending such events, but there would be very little benefit to the
overall community. Reduction in travel to such events may also reduce spread, although
the benefits of even major reductions in all travel are small.
PUBLIC TRANSPORT
3.43 Public transport within London will continue to operate, although services may be
rescheduled to ensure that a consistent minimal service is provided to communities
across London
SCHOOL CLOSURES
3.44 Influenza transmits readily wherever people are in close contact and is likely to spread
particularly rapidly in schools. As children are particularly unlikely to have any residual
immunity, they could be amongst the groups worst affected and can be ‘super
spreaders’.
3.45 The Government will take decisions on whether or not to advise closures on the basis of
an assessment of the emerging characteristics and impact as the pandemic develops.
The trigger for advice to close would be confirmation of initial cases in the area. The
decision to close schools would have an impact on not only the education of children,
but also services and businesses dependent on working parents.
3.46 Once the Government has issued advice, Local Authorities are responsible for
communicating this advice to school Head teachers2. The final decision rests with
schools and child care providers as to whether or not to close the school. Local
Authorities have a legal duty to provide education “at school or otherwise” for children
who for any reason may not for any period receive suitable education unless such
arrangements are made for them. Therefore, while it might not be possible to provide
the usual full service, Local Authorities must provide a reasonable level of education for
2
DfE will in future be responsible for issuing these messages to free schools and academies who do not report into
the LA education system
London Resilience Pandemic Influenza Response Plan 17 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
all children in their area if pupils are unable to attend school due to closure.
3.47 Once the pandemic virus is spreading freely in the community there is little public health
benefit of closing schools, and they would only be advised to do so for operational
reasons (insufficient teaching staff).
MUTUAL AID
3.48 For planning purposes, the assumptions should be that mutual aid from neighbouring
regions will not be available as the whole country will be affected. Limited mutual aid
within regions may be available and should be discussed locally.
VULNERABLE PEOPLE AND SOCIAL CARE
3.49 Vulnerable people are defined as those ‘that are less able to help themselves in the
circumstances of an emergency’. In the event of an influenza pandemic, these may
include; children, older people, mobility impaired, those mentally or cognitively function
impaired, the sensory impaired, individuals supported by health, LAs or the independent
sectors within the community, individuals cared for by relatives, prisoners and other
incarcerated populations (e.g. immigration removal centres (IRCs), police custody cells,
secure training centres), the homeless, pregnant women, minority language speakers,
tourists or the travelling community.
3.50 The process of identifying and managing vulnerable people should take place at the local
level. In London, multi-agency IPCs are responsible for putting in place arrangements for
sharing data on vulnerable people and ensuring that mechanisms are in place for
communicating, managing and supporting vulnerable people, including disabled people.
In particular, IPCs will need to produce estimates of the number and type of vulnerable
people within their area and consider their specific needs. IPCs will need to ensure that
they are able to deliver essential social services to vulnerable people during a flu
pandemic. See Annex 2 for guidance on the roles of IPCs.
3.51 Social care plays a daily role in partnership with the NHS by providing care to people in
the community. Social care resilience is essential in the response to an extended
duration or rising tide threat such as an influenza pandemic.
3.52 Social care is particularly important in working with the health response: in keeping
existing users safe in the community, reducing the impact on health of those who
become vulnerable due to the situation, and facilitating discharge into the community of
patients from the NHS services where this comes under pressure. It is essential that
health and social care services plan together for a pandemic in order that they respond
in concert.
3.53 Social care is provided by the public, private and third sector, serving client bases
ranging in size from individuals to large care homes. Due to its borough based
accountability, social care does not have the same command and control structure or
communications networks that exist in health care, which means a large scale
coordinated response needs to be designed in a different way. The local authority
Director of Adult Social Services is generally best placed to oversee social care
preparedness and response across the local area.
London Resilience Pandemic Influenza Response Plan 18 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
SECTION FOUR – PLANNING AND PREPAREDNESS
4.1 Even within a response plan such as this, it is prudent to reflect on planning and
preparedness measures that need to be undertaken in advance. This should take into
consideration the assumptions described in previous sections.
4.2 The 2009/10 pandemic illustrated that it is particularly important that planning is
flexible. The pandemic virus reached the UK some weeks before the pandemic was
officially declared, meaning that the planning required rapid adjustment and
consideration.
BUSINESS CONTINUITY AND RESILIENCE PLANNING
4.3 It is highly probable that the pandemic will consist of one or more waves, and once
established, its speed of spread will leave little time for contingency planning or
preparations.
4.4 Once efficient person-to-person transmission is established, preventing an influenza
pandemic is unlikely to be possible, as most people are likely to be exposed to the virus
at some stage during their normal activities. Those with influenza like symptoms should
minimise contact with others by remaining at home until the symptoms have resolved.
Those who are not symptomatic should continue normal activities for as long as
possible. By avoiding unnecessary close contact with others and routinely adopting high
standards of personal and respiratory hygiene, the likelihood of catching or spreading
influenza will be reduced.
4.5 The overall aim during a pandemic will be to encourage those who are well to carry on
with their daily lives normally for as long as possible, within the constraints imposed by
the pandemic. Although existing business continuity plans for other disruptive
challenges provide a good starting point for planning for an influenza pandemic, it must
be recognised that pandemic influenza presents a unique scenario in terms of prolonged
pressures through a reduced workforce and potentially increased workload.
Organisations are, therefore, expected to have business continuity and contingency
plans to ensure that critical services and outputs continue to be delivered throughout an
influenza pandemic.
4.6 It is the responsibility of all agencies that make up the London Resilience Partnership,
acting individually and collectively, to identify and plan for the full range of health and
non-health related impacts of pandemic influenza, including the implications for supply
chains.
4.7 Over the course of a pandemic, staff are likely to be absent from work for a combination
of reasons including personal illness, bereavement, fear of infection, the impact of public
health measures such as school closures and other factors such as transport difficulties.
All sectors should plan for such an eventuality which could last several months. Levels of
absence may vary due to the size and nature of a workplace, the kind of activity that
takes place there and the composition of the workplace.
4.8 Each organisation needs to estimate the level of staff absence and its potential impact
on its own activities. The level of staff absence will depend to some extent on the
composition of the workforce and the environments in which people work. In order to
derive estimates for the total numbers likely to be absent, employers should consider the
demographics of their work teams, including the percentage who have childcare or other
family care responsibilities, ‘normal’ absenteeism levels and options for home or remote
London Resilience Pandemic Influenza Response Plan 19 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
working. Due to the human resources implications of pandemic influenza, succession
planning will be a critical consideration in contingency planning.
4.9 Consultation and jointly conducted risk assessments by employers, staff and their trade
unions or representatives, combined with documented procedures during the planning
phase, can help ensure that employees are well educated and informed. Joint risk
assessments can also assist in identifying and exploring any subjective perceptions of
risk, the opportunities for more flexible working arrangements, and training
requirements to help cover staff absences. Identifying those staff with co-morbid
conditions or other factors that put them at higher risk may also allow proportionate
individual precautions.
4.10 Making temporary changes to working practices where possible – e.g. reducing close
face-to-face contact; providing physical barriers to transmission; enhancing cleaning
regimes; ensuring that the necessary protective equipment is available; having hand
washing, waste disposal and other hygiene facilities in place – and actively promoting
these and other similar measures - can help encourage and maintain attendance at work
during the response phase.
4.11 Advice on business continuity planning can be accessed from the UK Resilience website
at http://www.cabinetoffice.gov.uk/content/business-continuity. Tools such as the
Pandemic Influenza Checklist for Businesses highlight key questions to allow
organisations to undertake a gap analysis of their existing business continuity plans to
ensure robust resilience in the context of an influenza pandemic.
MULTI-AGENCY PLANNING AND PREPAREDNESS
4.12 It is likely that most, if not all, of the agencies that make up the London Resilience
Partnership will have established internal planning groups to lead on and coordinate
their organisation’s business continuity plans for pandemic influenza.
4.13 However, responding effectively during an influenza pandemic will also require the
combined efforts of the London Resilience Partnership to coordinate and establish
integrated multi-agency response plans.
4.14 A number of existing arrangements and organisational structures are in place to plan the
multi-agency response to pandemic influenza in the pre-pandemic phases.
London Local Resilience Forum (LLRF)
4.15 The role of the LLRF provides a senior level central focus for coordinated and effective
emergency planning in London, bringing together representatives from government, the
Mayor of London, London emergency services, the health sector in London, other key
public services and the business community. NHS London represents the local NHS
organisations (both category 1 and 2 responders). A full list of organisations that make
up the LLRF can be found in Annex 5.
4.16 The LLRF forms an overarching steering group and provides strategic guidance to
London’s emergency planning. The LLRF Chair is nominated by the Mayor of London
and the secretariat function is provided by the London Resilience Team (LRT).
4.17 During the preparedness phase pre-pandemic, the LLRF will meet on a regular basis to:
Assess the risk to London of pandemic influenza
London Resilience Pandemic Influenza Response Plan 20 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
Gather situation reports and updates at local and pan London level to guide
decision making, if applicable, and, where appropriate, communicate these via the
Government Liaison Team based in Department for Communities and Local
Government to central Government including the Department of Health and/or
Cabinet Office at a national level
Consider the establishment of a Business Continuity Group at the first meeting of
a London wide Pandemic Flu Coordinating Group.
Influenza Pandemic Committees (Planning)
4.18 IPCs (Planning) are based on local authority borough areas, and are the multi-agency
fora through which local planning, response and recovery are managed and co-
ordinated. They enable local service providers to establish a coherent approach with
each organisation knowing its role in relation to others.
4.19 IPCs (Planning) are made up of representatives from the local health community and
local authorities, and may also include borough police, fire brigade and voluntary sector
representatives.
4.20 The IPCs (Planning) are chaired by the Local Director of Public Health and convene
regularly to share information on the current state of preparedness, provide support,
make joint decisions, and develop local multi-agency plans.
4.21 For further guidance about IPCs (Planning) please see Annex 2.
London Resilience Pandemic Influenza Response Plan 21 of 69
Version 5, July 2012NOT PROTECTIVELY MARKED
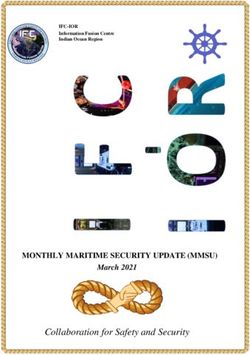
Table 4: Organisational Responsibilities in Planning and Preparedness
PLANNING & PREPAREDNESS
Organisation Lead Implementer Key Actions & Outputs
ALL ORGANISATIONS are Establish Pandemic Flu Lead to remain aware of international developments and
review emerging information and guidance.
expected to deliver the Monitor and evaluate risks and impacts for areas of responsibility.
following key actions and Identify and mitigate where possible critical vulnerabilities.
Undertake business continuity and resilience planning in the context of a
outputs at the specified pandemic flu scenario.
WHO Phase. Additional Ensure that planning is an integrated activity and that all plans are regularly
maintained and exercised.
organisation-specific Communicate plans with employees, contractors, and affiliated organisations.
activities for the relevant Participate in planning groups to discuss, plan and share best practice.
Use planning groups to consider adjustment of response strategies in respect of
WHO Phase are listed below. optimal practices.
Consolidate and test preparedness arrangements.
Familiarise themselves with overall UK Government advice on pandemic flu
planning.
All government departments Monitor and evaluate risks and impacts for areas of responsibility.
Inform and support contingency planning in areas of responsibility.
Produce up to date information, advice and guidance.
Monitor and review pandemic risk assessment.
Participate in cross-government official level committee to address
policy/preparedness issues.
Review/test communication links, preparedness and coordination arrangements.
Brief and convene Ministerial level committee if required
Department of Health - Lead government Establish national stockpiles of countermeasures to support response.
department
Maintain liaison with international health organisations.
Provide the information and guidance that other government departments,
organisations and agencies need to develop their own plans and responses.
Inform CCS, other Government Departments and NHS of any significant
developments.
Liaise with Defra and other relevant Government Departments over wider
implications of relevant avian /animal influenza incidents.
Provide information/briefings.
Consider need and options to support WHO/ international response.
Review options and development plans for a potential pandemic (or pre-
pandemic) vaccine with NIBSC and manufacturers.
Refine intervention strategies.
Review pharmaceutical and other supply needs.
Prepare information materials for future phases.
Provide the link between central government and the London partnership
London Government
Department for
Liaison Team Participate in planning groups to discuss, plan and share best practice across
Communities and related mechanisms, eg. LLRFs
Resilience and
Local Government Contribute to identification of policy gaps and to communication of new policy
Emergencies Division
advice
Mayor of London (or Chair London Local Resilience Forum (LLRF) - provide leadership and support
nominated for London Resilience Partnership.
representative)
Actions and outputs expected of all organisations, as above.
Greater London Undertake business continuity and resilience planning in the context of a
Authority pandemic flu scenario.
GLA Group Participate in groups to discuss, plan and share best practice
Have ongoing discussions with DH and NHS to address outstanding issues and
risks.
Test the GLA business continuity plan.
London Resilience Pandemic Influenza Response Plan 22 of 69
Version 5, July 2012You can also read