LET'S MAKE ITCHING ANCIENT HISTORY - APRIL 20, 2021 | FREE VIRTUAL EVENT SCIENTIFIC PROCEEDINGS - Hill's Global ...
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

LET’S MAKE ITCHING
ANCIENT HISTORY
APRIL 20, 2021 | FREE VIRTUAL EVENT
SCIENTIFIC PROCEEDINGS
HillsGlobalSymposium.com
HGS_2021_Proceedings Book.indb 1 17/04/21 12:21 PM
HILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
CONTENTS
3 U
pdate on Human Atopic Dermatitis
(Donald Leung, USA)
5
Simplifying the Pruritic Dog
(Darren Berger, USA)
8
Getting the Most Out of the Teledermatology
Consultation
(Richard P. Usatine, USA)
11
Multimodal Treatment of Atopic Dermatitis – the Four
Most Important Concepts to Know
(Douglas J. DeBoer, USA)
14 H
ocus Pocus Veterinary Dermatology Curtain Lifted
and Myths Revealed
(Christina Restrepo, USA)
20
Nutritional Approach to Dogs With Atopic Dermatitis
(Dana Hutchinson, USA)
24
Using Psychology to Help Pet Parents Tackle Atopic
Dermatitis
(Thomas Webb, UK)
27
Let’s Make Itching Ancient History: Innovation in
Nutritional Management of Atopic Dermatitis and
Food Allergies in Dogs
(Jennifer M. MacLeay, USA)
31
Debunking Nutrition Myths for Allergic Pets
(Jennifer A. Larsen, USA)
(Julie A. Churchill, USA)
34
Canine Atopic Dermatitis: How to Use the Newest
Drugs in Clinical Practice?
(Wayne Rosenkrantz, USA)
38
More Than Crusty Skin Pics: Using Social Media in
Veterinary Dermatology
(Ashley Bourgeois, USA)
Click on any title to access the article
Editors:
Dr Maureen Revington BVSc, MSc, PhD
S Dru Forrester DVM, MS, DACVIM
Iveta Bečvářová DVM, MS, DACVN
The comments and opinions are those of the authors, and do not necessarily reflect the position or beliefs
of Hill’s Pet Nutrition, Inc or its employees. ISSN 1479 - 8999
HGS_2021_Proceedings Book.indb 2 17/04/21 12:21 PM
HILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
UPDATE ON HUMAN ATOPIC DERMATITIS
Donald Leung, MD, PhD
Edelstein Chair of Pediatric Allergy-Immunology
National Jewish Health
Denver, CO, USA
Atopic dermatitis (AD) is a highly pruritic chronic AD.12-14 These studies demonstrate that epidermal
inflammatory skin disorder affecting 10-25% of children profiles from AD with peanut allergy is associated with
worldwide and approximately 7% of adults.1 It often high TEWL values, particularly after skin tape stripping,
predates or is found in association with childhood high Type 2 immune activation, Staphylococcus
food allergy (FA), asthma, and allergic rhinitis.2 Recent aureus colonization, reduced filaggrin breakdown
studies have demonstrated that AD is associated products, and a reduced proportion of long-chained
with epidermal barrier dysfunction allowing tissue lipid products. Lamellar bilayer structural integrity is
penetration of allergens, irritants, and microbes, which highly organized in normal skin but very abnormal
elicit skin inflammation.3,4 Causes of the abnormal skin in electron micrographs of skin layers from AD with
barrier are complex and driven by a combination of peanut allergy. These observations are consistent
genetic variants, environmental triggers, immunologic with a defective skin barrier in patients with AD and
factors that affect gene expression, and the profile of peanut allergy, predisposing to epicutaneous allergen
proteins and lipids in the epidermis.5,6 Variability in sensitization.4 Interestingly, low filaggrin has also been
the occurrence of these factors likely accounts for the found in the skin of peanut-allergic patients (without
heterogeneity of AD onset, severity, and natural history AD) supporting the importance of targeting research
of this skin disease. Filaggrin (FLG) gene mutations, in and treatment even in nonlesional skin.15
particular, are the most profound single gene defects
Skin tape proteomics reveal evidence for lack of
identified in AD, but the most common cause of FLG
epidermal terminal differentiation in AD, particularly
deficiency stems from skin immune activation and
involving those patients who have associated food
environmental factors.
allergy.16 Although skin tape stripping only samples the
A major function of the epidermis is to protect the stratum corneum and upper granular layers of the skin,
host from potentially damaging environmental factors increased amounts of KRT5 and KRT14 amounts were
and reduction of transepidermal water loss (TEWL). observed in the skin of AD patients with food allergy
In infants, increased TEWL can be detected prior to as compared with AD only and healthy controls.17 This
the onset of clinical disease. The onset of AD has is unusual because KRT5 and KRT14 are predominantly
been linked to early colonization with Staphylococcus expressed by undifferentiated proliferating
aureus and expression of epidermal thymic stromal keratinocytes in the basal layer of the epidermis.
lymphopoietin (TSLP), even before the onset of clinical These observations suggest that the superficial layer
or lesional eczema.7-11 Epidermal injury by scratching, of skin in patients with AD FA+ is characterized by
allergens, microbes and irritants (such as detergents keratinocytes that hyperproliferate, impairing their
and pollution) lead to the release of epithelial cytokines ability to terminally differentiate, thus accounting for
such as thymic stromal lymphopoietin (TSLP) and the low filaggrin, lipid abnormalities, increased TEWL,
Interleukin (IL)-33, which play a pivotal role in driving and microbiome abnormalities that characterize AD
type 2 immune and inflammatory responses through skin in patients with food allergy.
the activation of dendritic cells, innate lymphoid (ILC)
Skin-gut interactions have now been demonstrated in
type 2 cells, and Th2 cells. Although cytokines such
experimental animals with eczema and food allergy.18
as Interferon (IFN)-g, IL-17, and IL-22 can modify the
The immune mechanisms linking the skin to the gut
course of allergic responses, type 2 cytokines such
were recently shown to have their origins in skin injury-
as IL-4, IL-13, TSLP, and IL-33 play a central role in the
induced release of IL-33 from keratinocytes, leading
development of allergic diseases.
to intestinal mast cell hyperplasia and food-induced
Using a minimally invasive skin tape sampling technique, anaphylaxis. Importantly, the systemic release of skin-
our research group has demonstrated that epidermal derived TSLP may contribute to high circulating IgE
profiling of lipids, proteins, and transcriptomes can be levels, which promote not only FA but also respiratory
used to identify endotypes underlying different AD allergy. AD pathobiology evolves from a complex
phenotypes, e.g. AD with peanut allergy versus AD interaction of epidermal barrier disruption, high type 2
without peanut allergy versus peanut allergy without immune response, and an imbalanced skin microbiota
3
HGS_2021_Proceedings Book.indb 3 17/04/21 12:21 PM
HILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
that promotes cutaneous barrier dysfunction. The emollients been optimized for skin barrier repair.
development of noninvasive skin sampling techniques Indeed, a recent study demonstrated a trilipid cream
will allow early identification of abnormalities in the was more effective than a paraffin-based emollient in
skin barrier and facilitate early intervention in young reducing TEWL and serum IgE levels.20,21 Once immune
infants. activation is established, even in nonlesional AD, it is
important to effectively control cytokine actions with
These new skin sampling approaches may play an
proactive therapy. This may become possible with novel
important role in the identification of infants with early
pathogenesis-based topical and systemic therapies.
epidermal barrier dysfunction and facilitate the timely
Finally, The National Institute of Allergy and Infectious
introduction of novel therapies targeting infants who
Diseases (NIAID) Atopic Dermatitis Research Network
have skin barrier dysfunction, nonlesional immune
has studied a human skin commensal microbial therapy
activation, and microbial dysbiosis.19 Although there
to control Staphylococcus aureus colonization.22 Using
has been considerable controversy whether early
a multi-pronged approach to target the skin barrier
introduction of skin emollients can prevent AD and
dysfunction, microbial dysbiosis and underlying
food allergy, these studies have not targeted high-
skin inflammation in early infancy are likely to give
risk infants with pre-existing evidence for skin barrier
clinicians the best opportunity at controlling AD and its
dysfunction, many studies have not considered lack
associated atopic co-morbidities.
of adherence, nor have the ingredients of these skin
References 13. Berdyshev E, Goleva E, Bronova I, Dyjack N, Rios C, Jung J, Taylor
1. Leung DYM, Guttman-Yassky E. Deciphering the complexities of P, Jeong M, Hall CF, Richers BN, Norquest KA, Zheng T, Seibold M,
atopic dermatitis: shifting paradigms in treatment approaches. J Leung DY. Lipid abnormalities in atopic skin are driven by Type
Allergy Clin Immunol. 2014;134:769-79. PMCID: PMC4186710 2 cytokines. JCI Insight. 2018;3(4):e98006. PMCID: PMC5916244.
2. Davidson WF, Leung DYM, Beck LA, Berin CM, Boguniewicz M, 14. Leung DYM, Calatroni A, Zaramela LS, LeBeau PK, Dyjack N, Brar
Busse WW, Chatila TA, Geha RS, Gern JE, Guttman-Yassky E, Irvine K, David G, Johnson K, Leung S, Ramirez-Gama M, Liang B, Rios
AD, Kim BS, King HH, Lack G, Nadeau KC, Schwaninger J, Simpson C, Montgomery MT, Richers BN, Hall CF, Norquest KA, Jung J,
A, Simpson EL, Spergel JM, Togias A, Wahn U, Wood RA, Woodfolk Bronova I, Kreimer S, Talbot CC Jr, Crumrine D, Cole RN, Elias P,
JA, Ziegler SF, Plaut M. Report from the National Institute of Zengler K, Seibold MA, Berdyshev E, Goleva E. The nonlesional
Allergy and Infectious Diseases workshop on “Atopic dermatitis skin surface distinguishes atopic dermatitis with food allergy as
and the atopic march: Mechanisms and interventions.” J Allergy a unique endotype. Sci Transl Med. 2019;11(480):eaav2685. PMID:
Clin Immunol. 2019;143(3):894-913. PMCID: PMC6905466. 30787169
3. Walker MT, Green JE, Ferrie RP, Queener AM, Kaplan MH, Cook- 15. Berdyshev E, Goleva E, Bronova I, Bronoff AS, Hoffman BC,
Mills JM. Mechanism for initiation of food allergy: dependence on Ramirez-Gama MA, Garcia SL, Crumrine D, Elias PM, Cho CB, Leung
skin barrier mutations and environmental allergen costimulation. J DYM. Unique skin abnormality in patients with peanut allergy but
Allergy Clin Immunol 2018;141: 1711-25. no atopic dermatitis. J Allergy Clin Immunol. 2021;147(1):361-367.
4. Brough HA, Nadeau KC, Sindher SB, Alkotob SS, Chan S, e1. PMID: 32615171.
Bahnson H, Leung DYM, Lack G. Epicutaneous sensitization in 16. Goleva E, Calatroni A, LeBeau P, Berdyshev E, Taylor P, Kreimer
the development of food allergy: what is the evidence and how S, Cole RN, Leung DYM. Skin tape proteomics identifies
can this be prevented? Allergy. Apr 2020;75(9):2185–2205. PMID: pathways associated with transepidermal water loss and allergen
32249942 polysensitization in atopic dermatitis. J Allergy Clin Immunol.
5. Leung DYM, Berdyshev E, Goleva E. Cutaneous Barrier Dysfunction 2020;146(6):1367-1378. PMID: 32360271
in Allergic Diseases. J Allergy Clin Immunol. June 2020;145(6):1485- 17. Kim BE, Goleva E, Kim PS, Norquest K, Bronchick C, Taylor P,
1497. PMCID: PMC7291847 Leung DYM. Side-by-side comparison of skin biopsies and skin
6. Goleva E, Berdyshev E, Leung DY. Epithelial barrier repair and tape stripping highlights abnormal stratum corneum in atopic
prevention of allergy. J Clin Invest. 2019;129(4):1463-1474. PMCID: dermatitis. J Invest Dermatol. 2019;139(11):2387-2389.e1. PMCID:
PMC6436854 PMC6814531
7. Kelleher M, Dunn-Galvin A, Hourihane JO, Murray D, Campbell 18. Leyva-Castillo JM, Galand C, Kam C, Burton O, Guish M, Musser MA,
LE, McLean WH, et al. Skin barrier dysfunction measured by et al. Mechanical skin injury promotes food anaphylaxis by driving
transepidermal water loss at 2 days and 2 months predates intestinal mast cell expansion. Immunity 2019;50:1262-75.
and predicts atopic dermatitis at 1 year. J Allergy Clin Immunol 19. Lowe AJ, Leung DYM, Tang MLK, Su JC, Allen KJ. The skin as a
2015;135:930-5. target for prevention of the atopic march. Ann Allergy Asthma
8. Kelleher MM, Dunn-Galvin A, Gray C, Murray DM, Kiely M, Kenny Immunol. 2018;120(2);145-151. PMID: 29413338
L, et al. Skin barrier impairment at birth predicts food allergy at 2 20. Sindher S, Alkotob SS, Shojinaga MN, Brough HA, Bahnson HT,
years of age. J Allergy Clin Immunol 2016;137:1111-6. Chan S, Lack G, Leung DYM, Nadeau KC. Pilot study measuring
9. Kim J, Kim BE, Lee J, Han Y, Jun HY, Kim H, Choi J, Leung DYM, transepidermal water loss (TEWL) in children suggests trilipid
Ahn K. Epidermal thymic stromal lymphopoietin predicts the cream is more effective than a paraffin-based emollient. Allergy.
development of atopic dermatitis during infancy. J Allergy Clin 2020;75:2662–2708. PMID: 32176320.
Immunol. 2016;137(4):1282-1285. PMID: 26879860 21. Sindher T, Alkotob S, Shojinaga MN, Hamilto R, Chan S, Cao S,
10. Kennedy EA, Connolly J, Hourihane JO, Fallon PG, McLean WHI, Bahnson T, Brough H, Lack G, Leung DYM, Nadeau K. Increases
Murray D, et al. Skin microbiome before development of atopic in plasma IgG4/IgE with trilipid versus paraffin/petrolatum-
dermatitis: early colonization with commensal staphylococci at based emollients for dry skin/eczema. Pediatr Allergy Immunol.
2 months is associated with a lower risk of atopic dermatitis at 1 2020;31(6):699-703. PMID: 32372469.
year. J Allergy Clin Immunol 2017;139:166-72. 22. Nakatsuji T, Hata TR, Tong Y, Cheng JY, Shafiq F, Butcher AM,
11. Meylan P, Lang C, Mermoud S, Johannsen A, Norrenberg S, Hohl Salem SS, Brinton SL, Rudman Spergel AK, Johnson K, Jepson B,
D, et al. Skin colonization by Staphylococcus aureus precedes the Calatroni A, David G, Ramirez-Gama M, Taylor P, Leung DYM, Gallo
clinical diagnosis of atopic dermatitis in infancy. J Invest Dermatol RL. Rational development of a human skin commensal microbe
2017;137:2497-504. for bacteriotherapy and use in a randomized clinical trial of atopic
dermatitis. Nature Medicine. 2021. (Article in Press).
12. Dyjack N, Goleva E, Rios C, Kim BE, Bin L, Taylor P, Bronchick C,
Hall CF, Richers BN, Seibold MA, Leung DYM. Minimally invasive
skin tape strip RNA sequencing identifies novel characteristics of
the type 2-high atopic dermatitis disease endotype. J Allergy Clin
Immunol. 2018;141(4):1298-1309. PMCID: PMC5892844.
4
HGS_2021_Proceedings Book.indb 4 17/04/21 12:21 PM
HILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
SIMPLIFYING THE PRURITIC DOG
Darren Berger, DVM, DACVD
Associate Professor
Iowa State University, IA, USA
Pet parents quickly seek veterinary care for their When presented with a pet whose main symptom
animals when they are pruritic. This is often the result is pruritus, a major consideration as to the potential
of perceived discomfort or suffering on their animal’s causes should be the patient’s signalment. Additional
part. It may also be the result of disruptions in the pet qualifying characteristics or historical insights that
parent’s quality of life such as disturbing their sleep may help narrow the differential causes are: (i) The
or their bond with their pet. Regardless of the source relationship between secondary infections and pruritus
of concern, pruritic pets are frequently a source of onset; (ii) Acute vs. chronic progression of the pruritus;
frustration for both the pet parent and veterinarian, as and (iii) Lesion location and distribution. The signalment
there is a lack of “traditional tests” that reliably provide is helpful from the standpoint of the patient’s age and
an accurate diagnosis for many causes of pruritic breed. When considering primary causes of pruritus
dermatoses.1 In many cases of pruritus, the diagnosis certain conditions should be considered more likely
is often made based on signalment, clinical suspicion, and should likewise alter the priority placed on various
and response to a therapeutic trial. This is what many diagnostics or therapeutic trials. In addition, different
of us refer to as “clinical practice”, but it many instances breeds have been shown to be overrepresented with
feels more like trial and error to the pet parent. As such, certain pruritic conditions or those that may predispose
it is important to educate the pet parent about the the patient to secondary infections which result in
possible causes and the process to relieving their pet’s pruritus. The author likes to break canine patients
discomfort. down into three groups based on age to help prioritize
potential differentials (Table 1).
TABLE 1.
Primary differentials for pruritic patients based on the age of the
patient at the time clinical signs started.
≤6 MONTHS OF AGE 6 MONTHS TO 4 YEARS OF AGE ≥ 5 YEARS OF AGE
Parasites Parasites Parasites
CAFR CAD CAD
CAD CAFR CAFR
Contact dermatitis Contact dermatitis Contact dermatitis
Hypothyroidism Endocrinopathies
Autoimmune or immune- Autoimmune or immune-
mediated conditions mediated conditions
Epitheliotropic lymphoma
CAFR – Cutaneous adverse food reaction; CAD – Canine atopic dermatitis
5
HGS_2021_Proceedings Book.indb 5 17/04/21 12:21 PM
HILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
Once the signalment has helped establish possible worsens. Contrary to this are disorders such as
underlying etiologies, other characteristics of the demodicosis or hypothyroidism where the patient is
patient’s pruritus should be used to help prioritize not typically pruritic until after the secondary infection
the differentials. Many pruritic patients will also has occurred. Likewise, whether the pruritus onset was
have secondary infections such as Staphylococcus acute and intense or chronic and progressive can also
pseudintermedius or Malassezia pachydermatis. These be telling. Parasitic conditions tend to have an acute
infections may directly cause the pet’s pruritus or and intense onset whereas canine atopy is a more
intensify the sensation. Regardless, establishing when chronic and progressive disorder. Finally, the location
they occur with respect to the onset of pruritus or and nature of associated skin lesions may be helpful. In
whether pruritus remains despite their elimination, the case of allergic dermatitis, thinned skin and haired
can be helpful in establishing the likely cause. This is regions (paws, pinnae, perianal, axilla, and inguinal
where the saying “an itch that rashes or a rash that regions) are normally affected. Alternatively, endocrine
itches” can provide valuable insight. Allergic conditions or autoimmune conditions tend to be symmetrical, with
tend to be pruritic disorders that get complicated the face and trunk more frequently affected.
by secondary infections and the patient’s situation
Once the differentials for the patient have been established and prioritized, the diagnosis
frequently relies on eliminating potential diagnoses through diagnostics and therapeutic trials.
The author prefers to work through differential lists in the following manner:
1. Is there a likelihood that the patient is pruritic for a non-allergic condition?
a. If so, perform appropriate skin scrapes, blood work, or biopsies
b. If not, move on to step 2
2. Are parasites present or highly suspected?
a.
If so, perform diagnostics to confirm their presence or establish an appropriate
preventative or therapeutic trial.
b. If not, or parasitic control is adequate move on to step 3
3. Is the patient’s pruritus seasonal?
a. Yes, then …
i. Has the potential for fleas been adequately addressed?
1. If not, institute integrated flea control
2. If flea control is appropriate, then the patient has atopic dermatitis
b. No, then…
i. Start a diet elimination trial
1. If the patient responds, then rechallenge with their prior or normal diet, if pruritus
recurs, reinstitute feeding with the therapeutic diet and if clinical signs resolve once
again, the diagnostic loop has been closed and a diagnosis of cutaneous adverse
food reaction has been established. Pruritus may recur as soon as hours or up to 1-2
weeks after reintroducing the pet’s normal diet. To help the pet parent establish a
diagnosis as quickly as possible reintroduction of the prior diet, treats, and chews
should be done as soon as possible.
2. If the patient fails to respond, the patient is most likely atopic or has concurrent
allergic conditions. Start specific or symptomatic therapy for canine atopic
dermatitis
The reason for this approach is that if a non-allergic condition is suspected, those most often
can be confirmed via blood work or biopsy with histopathology. This provides the pet parent
with a quick and definitive answer as to those differentials. This is in contrast to that of allergic
causes, where no single definitive test exists. Nowhere is this more evident than with canine atopic
dermatitis, which is a diagnosis of exclusion. In cases where a parasite or evidence of parasites
are found a definitive diagnosis can be made. However, in many cases of allergic dermatitis, the
differential is either confirmed or excluded by therapeutic trials.
6
HGS_2021_Proceedings Book.indb 6 17/04/21 12:21 PM
HILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
Flea allergy dermatitis should always be considered and lamb.4 There are three different concept diets to
a potential or concurrent diagnosis for any dog help avoid these offending allergens: novel or exotic
presenting with a history of pruritus. Acute or intense protein, hydrolyzed protein, or a home-cooked diet.
pruritus affecting the lumbosacral region, tail base, Just as there is no definitive commercial test for CAFR
or caudomedial thighs should raise suspicion along in dogs, there is also no definitive diet that is effective
with certain geographic regions where fleas can be 100% of the time. However, for the purpose of diet
a perennial problem. When fleas are suspected an elimination trials, there is currently no commercially
effective flea control program should be initiated. Many available over the counter diet that provides an
preventative products are available and effective for adequate substitute for a commercial therapeutic
this purpose. It is important to keep in mind the flea diet.5 Diet selection should ideally be based on patient
life cycle and your geographic region when considering history and dietary needs. A diet elimination trial should
how long a therapeutic trial should be implemented. last at least 8 weeks in canine patients to increase the
Regions in the Southeast United States, specifically likelihood of properly identifying a CAFR.6 Achieving
Florida, may need a more aggressive approach for this this length of time in some patients can be difficult and
differential and consider it a concurrent complicating a brief, tapering dose of glucocorticoids can be helpful
factor for any allergic condition compared to other during the initial phases of the diet elimination trials.7
regions in the U.S. In addition to fleas, other parasites
Canine atopic dermatitis is solely a clinical diagnosis. It
such as Sarcoptes scabiei and Cheyletiella spp. may
is a diagnosis of exclusion and in essence is proving a
also cause intense, acute pruritus in any age of patient.
negative which contributes to frustration surrounding
These mites on occasion can be difficult to recover
the condition. A diagnosis of canine atopic dermatitis
and when suspected may warrant a treatment trial.
can be made in patients with seasonal pruritus when
Many of the current flea preventatives are considered
fleas have been eliminated, or in non-seasonally
an effective treatment options for these and other
pruritic patients when all other allergic and non-
ectoparasties, and when utilized for a flea preventative
allergic conditions have been ruled out that directly
program, should be sufficient for ruling out these
or indirectly cause pruritus (predispose to secondary
potential pruritic causes.2
infections). Although allergy tests exist, they are poorly
Once parasites are eliminated as a potential cause, a named and they are not screening, diagnostic, or
cutaneous adverse food reaction should be considered. confirmatory in nature.8 No test is completely sensitive
Suspicion for a food allergen being the inciting or specific and clinically normal dogs may have positive
cause should increase if the patient has nonseasonal reactions, while clinically affected dogs can have
clinical signs, does not respond well to anti-pruritic negative results. Allergy tests as currently conducted
medications, has concurrent GI signs, or clinical signs in veterinary medicine should only be thought of and
began at a certain age for the patient. No one historical utilized as a “guide” for selection of allergens to be
clue is definitive or always indicative of a cutaneous included in allergen specific immunotherapy or the
adverse food reaction, but a combination of the basis for allergen avoidance measures. Two sets of
preceding historical clues should raise the clinician’s clinical criteria known as “Favrot’s criteria” have also
level of concern. Although much effort has been been developed to assist with the diagnosis of canine
directed toward the development of a diagnostic test to atopy. These sets of criteria should not be used as a
aid in the diagnosis of a CAFR, to date the single most sole diagnostic test as they are also not completely
effective diagnostic procedure to identify a CAFR in a specific or sensitive for the condition. However, when
patient remains a diet elimination trial with subsequent combined with a careful work-up as described above
provocation testing.3 The most commonly identified they can enhance a clinician’s diagnostic accuracy.
food allergens in dogs are beef, dairy, chicken, wheat
References 5. Olivry T, Mueller RS. Critically appraised topic on adverse food
1. Hensel P, Santoro D, Favrot C, et al. Canine atopic dermatitis: reactions of companion animals(5):discrepancies between
detailed guidelines for diagnosis and allergen identification. BMC ingredients and labeling in commercial pet foods. BMC Vet Res
Vet Res 2015;11:196. 2018;14:24.
2. Parasitic Skin Diseases. In: Coyner KS ed. Clinical Atlas of Canine 6. Olivry T, Mueller RS, Prélaud P. Criticallyappraised topic on adverse
and Feline Dermatology. 1st ed. Hoboken, NJ:Wiley-Blackwell, food reactions of companion animals(1):duration of elimination
2020; 111-130. diets. BMC Vet Res 2015;11:225.
3. Mueller RS, Olivry T. Critically appraised topic on adverse food 7. Favrot C, Bizikova P, Fischer N, et al. The usefulness of short-course
reactions of companion animals(4): Can we diagnose adverse food prednisolone during the initial phase of an elimination diet trial
reactions in dogs and cats with in vivo or in vitro tests. BMC Vet in dogs with food-induced atopic dermatitis. Vet Dermatol 2019;
Res 2017;13:275. 30:498-e149.
4. Mueller RS, Olivry T, Prélaud P. Critically appraised topic on adverse 8. DeBoer DJ, Hillier A. THe ACVD task force on canine atopic
food reactions of companion animals(2): common food allergen dermatitis (XV): Fundamental concepts in clinical diagnosis. Vet
sources in dogs and cats. BMC Vet Res 2016;12:9. Immunol Immunopathol 2001;81:271-276.
7
HGS_2021_Proceedings Book.indb 7 17/04/21 12:21 PM
HILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
GETTING THE MOST OUT OF THE
TELEDERMATOLOGY CONSULTATION
Richard P. Usatine, M.D.
Professor, Dermatology and Cutaneous Surgery
Professor, Family and Community Medicine
Founding Director, Skin Clinic, University Health System
University of Texas Health San Antonio, TX, USA
HOW TO PREPARE FOR TELEDERMATOLOGY VISITS • S ome viral infections such as mild to moderate zoster
To start doing teledermatology you need appropriate or herpes
hardware and software with a strong Internet or data • Monitoring chronic dermatology diagnoses that are
connection. The electronic health record (EHR) on currently under control
a good quality computer with a standard monitor By patient characteristics:
is the foundation. In medicine with human patients
the privacy considerations need to be HIPAA (Health • Y
oung adults and teenagers that are technology
Insurance Portability and Accountability Act) compliant. proficient
Communication for telehealth may be as simple as • Have access to high-quality Wi-Fi connections
a phone conversation or as complex as a discussion • Don’t need an interpreter
through a HIPAA compliant electronic portal from the • Follow-up patients well-known to the provider
EHR to a patient portal (e.g. Epic and MyChart).
Dermatology cases in which teledermatology is most
Software options for telehealth: challenging or least effective:
• Doximity By diagnosis:
• Zoom
• Skin cancer and precancer such as actinic keratoses
• Doxe.Me
• Skin cancer detection and total body exam
• Patient Portals in EHRs
• Systemic dermatologic disease in acute presentation
Examples of telemedicine built into EHRs:1 • Immunobullous disease in acute presentation
• AdvancedMD • Any dermatologic condition with plans for
• Allscripts intralesional injections
• Cerner • Rashes or any condition needing biopsies
• Epic • Conditions needing cryotherapy
• Salus • By patient characteristics:
• PrognoCIS • Any patient with limited technology literacy (often
Doximity app for phone, tablet and computer: You can older)
use your cell phone to call patients without revealing • Patients without smart phone or computer
your private number. When their phone rings, patients • Patients without Wi-Fi or good phone/data
see your office number (or any number you designate) connection
on their CallerID. For video conferencing, just dial the • Patients not knowing how to use their smart phone
patient’s number to start a video call. They are sent a for video connections
text message from a no-reply number (not your cell • Patients not using email and not able to send
number). With a few taps the patient and provider are photographs when needed electronically
connected.2
• Patients too shy for video conference
Dermatology cases in which teledermatology is most
What environment is best for teledermatology?
effective:
• A
quiet environment on both ends of the
By diagnosis:
communication
• Acne • Good lighting – avoid backlighting and dark rooms
• Psoriasis
• Atopic dermatitis
• Fungal infections that are classic
8
HGS_2021_Proceedings Book.indb 8 17/04/21 12:21 PM
HILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
How to establish rapport with the patient using video? During the physical exam, tips for best results:
• L ook at the phone or camera to establish eye contact • G ood lighting which is often indoors rather than
• Place patient’s image near your camera if patient is outdoors where there may be glare and shadows
on the monitor • Smart phone light or a flashlight can help examining
• Stay focused on patient the oral cavity
• Avoid distractions, disable other alerts, ringers, • A family member or friend can help point the phone
alarms or camera at the back or buttocks
• Advise patient when you are looking away at medical • Foot exam means removing shoes and socks
record or typing notes • Palpation can be done by the patient or parent if
• Dress professionally directions are given clearly
• Avoid eating during visit • Even a partial neurologic exam is possible with clear
• Understand that a patient may not want to reveal directions
a private area over a video connection even if they • A ruler or another common object such as a coin can
would feel comfortable with this in the office be placed near a lesion to give size
• Apologize if you are calling or connecting after the • Home dermoscopy is possible and may make sense
appointment time and don’t assume that the patient for patients at the highest risk of melanoma
has nothing else to do but to wait for you • There is a dermoscopy loan program available
• If you are calling or connecting early make sure the through Oregon Health Sciences University (OHSU)
patient is ready by asking their permission to proceed Tips for working with older adults:3
now vs calling back
• If the patient has decreased hearing, the patient may
• If there is no answer, leave a message that you or
wear a headset
someone from your office will call back so they know
that the phone number you are using is not spam or • Provider should use a good microphone or wear a
telemarketing headset
• Use office staff to help facilitate these connections • Position camera for patients to be able to see and
when using the patient portal of an EMR. Patients read your lips
may need coaching to figure out how to use the • Speak slowly and ask patient to teach-back to you
patient portal • Send written instructions electronically or by mail if
necessary
Steps to increase efficiency in teledermatology:
• U se office staff to schedule the telehealth visits and Pitfalls in teledermatology:
to schedule follow-ups • Patients who can’t navigate the technology
• Transmit prescriptions electronically including • Out of focus photos
controlled substances when necessary • Unhappy patients when the circumstances require an
• Transmit orders for labs and imaging electronically in-person visit – the rare patient becomes unhappy
when possible and inform patients how to get these stating they wasted their time – fortunately this is
tests done truly rare as patients are usually very grateful for the
• Do verbal health education but consider electronic teledermatology visit and understand that the next
information sheets/handouts when it is easy to send step is an in-person visit
an email or use the EMR for messaging. Benefits for patients:
How to maintain your own privacy while connecting • No travel needed
to patients: • No parking needed
• D on’t call or FaceTime from your personal cell phone • Avoiding contact with COVID-19
number unless you are prepared to receive messages • No problems finding the clinic
and phone calls from this patient in the future – in
• Less time due to no travel and no waiting room time
general it is best to avoid this situation –
• While waiting for a visit, chores and work can be
• Consider dialing *67 before the number, but this may
performed
result in the patient not picking up the phone call as
it looks like telemarketing. The app Doximity works • Helps patients with limited mobility and limited
to avoid this access to transportation
• If you are using a phone-based app such as Doximity, Risks for patients:
assign the office phone to the phone number that • Insurance may not cover the visit especially as the
they will see the call coming from pandemic becomes less severe
• Have an email address that you can use for patients • Procedures can’t be performed, so additional visits
to send photographs when needed as these photos are then needed
are often in better focus than video images
• Don’t text from your private phone or send emails
from your private email address
9
HGS_2021_Proceedings Book.indb 9 17/04/21 12:21 PM
HILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
Benefits for providers: divide - patients with less money and resources
• C an work from home or possibly a more relaxed office get help obtaining high-speed Internet and smart
phones/computers/tablets. (note that families often
• Less exposure to COVID-19
need this technology for online schooling and work
• Fewer no-shows - especially due to transportation at home for adults)
problems
• Continue public and private insurance coverage for
• Can do charts while listening to patients without telehealth.
appearing rude
• Can reach elderly and underserved patients Conclusions:
• T here are many benefits to telehealth for patients
Risk for providers:
and providers
• Insurance may not pay for the visit, especially phone • There are some pitfalls regarding limited technology
visits literacy and limited access to the hardware and
• Decreased satisfaction when procedures are needed Internet
and cannot be performed • Private and public support to improve technology
What can be done to make teledermatology more literacy and access to the hardware and the Internet
effective? can allow for innovations and growth of telehealth.
• P roviding avenues for patients to learn how to use
the technology needed.
• Federal and state support to overcome the digital
References 5. Clarke EL, Reichenberg JS, Ahmed AM, et al. The utility of
1. https://www.softwareadvice.com/telemedicine/#buyers-guide teledermatology in the evaluation of skin lesions. J Telemed
Telecare 2021:1357633X20987423. doi: 10.1177/1357633X20987423.
2. https://www.doximity.com/app
Epub ahead of print. PMID: 33461401.
3. Nieman CL, Oh ES. Connecting With Older Adults via Telemedicine
6. Cline A, Kim C, Deitz M, et al. Real-World Direct-to-Patient
[published online ahead of print, 2020 Aug 11]. Ann Intern Med.
Teledermatology in a Low-Income, Elderly Population. J Am
2020;10.7326/M20-1322.
Acad Dermatol 2021:S0190-9622(21)00187-0. doi: 10.1016/j.
Further reading jaad.2021.01.038. Epub ahead of print. PMID: 33476731.
1. Berman HS, Shi VY, Hsiao JL. Challenges of Teledermatology: 7. Conforti C, Lallas A, Argenziano G, et al. Impact of the COVID-19
Lessons Learned During COVID-19 Pandemic. Dermatol Online J Pandemic on Dermatology Practice Worldwide: Results of a Survey
2020;26:13030/qt7193305r. PMID: 33342172. Promoted by the International Dermoscopy Society (IDS). Dermatol
2. Hadeler EK, Beer J, Nouri K. Teledermatology: Improving Access or Pract Concept 2021;11:e2021153. doi: 10.5826/dpc.1101a153. PMID:
Widening Healthcare Disparities? J Drugs Dermatol 2020;19:1248. 33614221; PMCID: PMC787
doi: 10.36849/JDD.2020.5693. PMID: 33346507.
3. Cartron AM, Aldana PC, Khachemoune A. Pediatric teledermatology:
A review of the literature. Pediatr Dermatol 2021;38:39-44. doi:
10.1111/pde.14479. Epub 2020 Dec 9. PMID: 33295665.
4. Mizes A, Vainder C, Howerter SS, et al. Access to consultative
dermatologic care via physician-to-physician asynchronous
outpatient teledermatology. Am J Manag Care 2021 ;27:30-32. doi:
10.37765/ajmc.2021.88574. PMID: 33471459.
10
HGS_2021_Proceedings Book.indb 10 17/04/21 12:21 PMHILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
MULTIMODAL TREATMENT OF ATOPIC DERMATITIS:
THE FOUR MOST IMPORTANT CONCEPTS TO KNOW
Douglas J. DeBoer, DVM, DACVD
School of Veterinary Medicine
University of Wisconsin
Madison, WI, USA
A change in our thinking barrier to prevent infections where possible, as
Historically, management of atopic dermatitis (AD) opposed to recurring cycles of treatment
has been aimed at the end process of the disease, in • Modification of the immunologic response through
other words, focused on anti-inflammatory therapies. allergen immunotherapy
“Managing inflammation” has been the first goal
of therapy. This traditional approach was a rather • Controlling the primary factor in patient discomfort,
blunt instrument often consisting principally of oral that is, pruritus – and if possible, modifying the
corticosteroids, with antihistamines or fatty acids as neuro-immunologic ‘vicious cycles’ that contribute to
possible adjuncts. As our understanding grew, we chronicity
gained additional tools to manage the inflammation, for • Managing inflammation, where possible targeting the
example the oral and topical calcineurin inhibitors such therapy to treat specific signs such as scratching, or to
as ciclosporin; oclacitinib and lokivetmab to manage treat regionally with topical products.
pruritus; and effective topical corticosteroid products
that could manage inflammation with less systemic Foundation vs. accessory treatments
effect. We also gained a renewed understanding of We often say that every dog with AD has one key
the importance of treating secondary complications “foundation treatment” - one particular treatment that
such as bacterial and yeast infections. All of these provides the most efficacy for that patient, and the
approaches, even as they evolved, were still completely best client satisfaction. This treatment is often a drug
reactive – reacting to the inflammatory process, after it or biological, at least initially. Current treatments that
had already become well-established in the skin. fall into this group include corticosteroids, ciclosporin,
oclacitinib, lokivetmab, and allergen immunotherapy.
Our newer approach to long-term treatment of AD
The best foundation treatment DOES vary from patient
encompasses a broader, whole-patient view, stressing
to patient, and situation to situation. Things to think
a multifaceted protocol, based on a multifaceted
about when choosing and using foundation treatments
pathogenesis, and multifaceted clinical signs that are
include:
likely different in each patient. In addition, where possible
we now stress a proactive approach to treatment – in • Efficacy – of course. Each of the above foundation
other words, correcting the underlying pathogenesis treatments will probably work well for somewhere
of the disease where possible, preventing acute flares between 60-80% of dogs.1-4 However, it’s not the
where we can, and forestalling the development of same 60-80% for each treatment! Unfortunately,
chronic inflammatory changes in the skin that become at this point, there is no way to predict in advance
much more difficult to reverse. Important elements of which treatment will turn out to be the best one for
this new approach include: a particular dog. This implies that trial-and-error is
a necessary part of early treatment and clients must
• Elimination of allergens where possible (decreasing
understand this.
allergen load), targeting environmental, parasitic,
dietary, and microbial allergens • Administration and adherence – what does the owner
prefer; what is easy for them to do?
• Augmenting or repairing the epidermal barrier in an
attempt to limit percutaneous penetration of allergens •
Owner preferences; for example the biological
and irritants treatments may resonate more with some owners
than others.
• Control of secondary infections when and as they
occur, and augmenting the epidermal antimicrobial • Adverse effect profile of each treatment.
11
HGS_2021_Proceedings Book.indb 11 17/04/21 12:21 PMHILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
• Safety, contraindications, and comorbidities for each • Nutritional considerations: beyond being a source of
treatment. EFA supplementation, modern “skin benefit” diets
often contain other ingredients that may enhance
• The “targetedness” of each treatment – see below for
barrier function and reduce inflammation, thereby
more about this!
adding to relief at least by reducing other medication
• Overall cost of the treatment – recognizing that this requirements. Evidence for efficacy of these diets
includes not only the cost of the treatment itself is limited at this point, but it does exist - both in
per year, but also recommended monitoring and re- cutaneous models and in clinical feeding trials.9-11
examination costs.
•
Don’t forget the ears! Atopic otitis externa is
With canine AD, one treatment alone typically does common as part of AD, and for some dogs is a major
not provide optimal relief. Along with finding the best manifestation of the disease. It may deserve specific
foundation treatment for each pet, adjunct treatments attention if present.
are enormously helpful for most dogs, both for
• Antihistamines: there is still virtually no evidence that
increasing efficacy and decreasing amounts of other
they are beneficial in AD that is of substantial severity,
medications that may be required. So – what works?
however, they are often tried as “add-ons” for patients
Here are some things to think about:
with mild disease.
• Parasite and infection control: many dogs with AD
The concept of targeting
will have concurrent flea sensitization. Thus, routine
prophylactic antiparasitic treatment is advised for Our recent understanding of the pathogenesis of
all canine AD patients. Very importantly, most dogs AD stresses that it is an immensely complex process
with AD are very susceptible to secondary infection involving many different cell types, inflammatory and
with both staphylococci and yeast organisms. immunologic processes, cytokines and chemokines,
Treatment must focus on not only initial elimination and other inflammatory mediators. In particular, many
of the infections, but prevention of future episodes of of these processes are orchestrated via networks of
infection. cytokines. Exactly which cells, processes, and mediators
are responsible for clinical signs and patient discomfort
• Topical treatment: bathing helps! Studies have shown likely varies by individual and by stage of disease.
that frequent (weekly to twice weekly) bathing with
any non-irritating, emollient shampoo can have a In parallel with this concept we must recognize that
limited antipruritic effect;4 it also washes away debris, foundation treatments vary greatly in how targeted
environmental allergens, and organisms from the skin. they are with respect to, for example, cytokine networks
In human AD, application of emollient preparations (Table 1). Corticosteroids are very untargeted, in that
to the skin is an important and basic element they affect production of many cytokines by many cell
of treatment, and unquestionably helps relieve types. This is why they work so well, but also why they
symptoms over time. Topical modification of barrier have adverse effects. Ciclosporin is more targeted, and
function is an active area of research in veterinary oclacitinib even more so. The most targeted treatment
medicine. Initial research has shown that application we have currently is lokivetmab, which affects only a
of topical lipid preparations can result in improvement single cytokine.
of the intercellular lipid lamellar structure and Putting these two concepts together: a dog with
composition and can be associated with limited relatively early, uncomplicated AD with minimal lesions
clinical improvement, though such improvement and mild to moderate pruritus may be simpler to address
typically takes months.5,6 than a dog with severe pruritus, longstanding disease,
• Essential fatty acid (EFA) supplementation – via diet secondary complications, and chronic skin changes. The
or otherwise: EFA supplements remain a cornerstone latter patient may have dozens of cytokines wreaking
of conservative management. Their effects may occur havoc. In this case, is it fair or reasonable to expect
through their weak anti-inflammatory actions, through that a very targeted therapy will be effective? It may
possible effects on epidermal barrier function, and be, or it may not be – and if it is not, the reason might
most importantly through their medication-sparing be that it is simply too targeted for that patient at that
effects.7,8 Because they are relatively inexpensive, safe, time. Moving up towards something LESS targeted may
and easily administered, many dermatologists advise provide a solution in this instance. Once the condition is
that, ideally, all atopic pets should receive enhanced better controlled, moving back down to more targeted
levels of EFA in their diet. Typically, daily doses in the treatments may provide long-term benefit with a better
range of 40-100 mg/kg of omega-3 anti-inflammatory adverse effect profile.
fatty acids, administered via supplement or as part of
the dietary formulation itself, are recommended to
achieve this benefit.
12
HGS_2021_Proceedings Book.indb 12 17/04/21 12:21 PMHILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
TABLE 1.
Extent of cytokine “targeting” of common foundation treatments in canine atopic dermatitis,
listed from least to most targeted.
TREATMENT TARGETED? COMMENTS
Reduce production of many cytokines at the DNA
Glucocorticoids Untargeted
transcriptional level
Blocks transcription of several cytokine genes in activated
Ciclosporin Somewhat targeted
T-lymphocytes, such as IL-2
Blocks cytokine receptor function mainly for interleukin-31;
Oclacitinib Somewhat targeted lesser effects on some other cytokines such as interleukins 2, 4,
6, and 13
Lokivetmab Completely targeted Binds and inactivates only interleukin-31
Short term plan, long term plan clinical remission. Fast-acting “foundation treatment”
Practice guidelines for treatment of AD4 stress that drugs are often the mainstay here. The “long term
one approach or set of therapies is appropriate for plan” is very different. It is intended to maintain clinical
short-term or immediate management of clinical flares, remission after it is induced. Elements of the “long term
and a second set is used in an attempt to gain longer- plan” are often accessory treatments like nutrition and
term control of the disease. Owners, especially, need topical measures, and they will take perhaps months
to understand this principle: “the therapy we use will to make a difference. Their effects will be more subtle,
change over time.” What we treat your dog with initially and will likely mostly manifest in better overall control
will differ from what we will recommend over the long with fewer relapses, along with less requirement for
term. The “short term plan” is designed to provide foundation treatment drugs.
immediate relief of the acute disease and induce
References
ote to the reader:
N 6. Popa I, Remoue N, Osta B, et al. The lipid alterations in the stratum
The International Committee on Allergic Diseases of Animals (ICADA) corneum of dogs with atopic dermatitis are alleviated by topical
regularly publishes expert panel reviews, updates, and practical application of a sphingolipid-containing emulsion. Clin Exp
guidelines for treating allergic diseases in dogs and cats. Many Dermatol. 2012;37:665-671.
helpful references can be accessed through the ICADA website at 7. Saevik BK, Bergvall K, Holm BR, et al. A randomized, controlled
www.icada.org. study to evaluate the steroid sparing effect of essential fatty acid
supplementation in the treatment of canine atopic dermatitis. Vet
1. Little PR, King VL, Davis KR, et al. A blinded, randomized Dermatol. 2004;15:137-145.
clinical trial comparing the efficacy and safety of oclacitinib and
8. Müller MR, Linek M, Löwenstein C, et al. Evaluation of cyclosporine-
ciclosporin for the control of atopic dermatitis in client-owned
sparing effects of polyunsaturated fatty acids in the treatment of
dogs. Vet Dermatol. 2015;26:23-30, e7-8.
canine atopic dermatitis. Vet J. 2016;210:77-81.
2. Gadeyne C, Little P, King VL, et al. Efficacy of oclacitinib (Apoquel®)
9. Watson AL, Fray TR, Bailey J, et al. Dietary constituents are able
compared with prednisolone for the control of pruritus and clinical
to play a beneficial role in canine epidermal barrier function. Exp
signs associated with allergic dermatitis in client-owned dogs in
Dermatol. 2006;15:74-81.
Australia. Vet Dermatol. 2014;25:512-8, e86.
10. van Beeck FL, Watson A, Bos M, et al. The effect of long-term
3. Moyaert H, Van Brussel L, Borowski S, et al. A blinded, randomized
feeding of skin barrier-fortified diets on the owner-assessed
clinical trial evaluating the efficacy and safety of lokivetmab
incidence of atopic dermatitis symptoms in Labrador retrievers.
compared to ciclosporin in client-owned dogs with atopic
J Nutr Sci. 2015;4:e5.
dermatitis. Vet Dermatol. 2017;28:593-e145.
11. Witzel-Rollins A, Murphy M, Becvarova I, Werre SR, Cadiergues
4. Olivry T, DeBoer D, Favrot C, et al. Treatment of canine atopic
MC, Meyer H. Non-controlled, open-label clinical trial to assess
dermatitis: 2015 updated guidelines from the International
the effectiveness of a dietetic food on pruritus and dermatologic
Committee on Allergic Diseases of Animals (ICADA). BMC Vet Res.
scoring in atopic dogs. BMC Vet Res. 2019;15:220.
2015;11:210-221.
5. Marsella R, Segarra S, Ahrens K, et al. Topical treatment with
SPHINGOLIPIDS and GLYCOSAMINOGLYCANS for canine atopic
dermatitis. BMC Vet Res. 2020;16:92-97.
13
HGS_2021_Proceedings Book.indb 13 17/04/21 12:21 PMHILL’S GLOBAL SYMPOSIUM 2021 | PROCEEDINGS
HOCUS-POCUS VETERINARY DERMATOLOGY:
CURTAIN LIFTED AND MYTHS REVEALED!
Christina Restrepo, DVM, DACVD
Naples, FL, USA
Myth 1: Atopic Dermatitis (AD) and Cutaneous Elimination diet trials are required for patients with
Adverse Food Reactions (CAFR) are diagnosed by perennial pruritus and/or concurrent gastrointestinal
utilizing serum and saliva allergy tests. signs.1 Once a clinical diagnosis of canine AD is made,
The best and most accurate method of debunking allergy testing can be performed to identify potential
the above statement is to refer to the ample current causative allergens for allergen-specific immunotherapy
evidence-based veterinary literature. A sub-group (ASIT).1 Allergy testing can be performed by IDT and
of the International Committee for Allergic Diseases ASIS. Neither test is recommended as a screening test
in Animals (ICADA) developed, based on extensive and should only be used to confirm the clinical diagnosis
searches in online citation databases and abstracts from of canine AD.1 However, several factors may play a role
international meetings, a set of practical guidelines in the decision-making as to whether an allergy test
that can be used to assist practitioners in the diagnosis is necessary. Severe clinical signs, duration of clinical
of canine Atopic Dermatitis (AD).1 These guidelines signs for more than 3 months per year, insufficient
provide an overview of the diagnosis of canine AD that management with symptomatic therapy, side effects
involves three distinct, but complementary, approaches. with symptomatic drug therapy, and, most importantly
These are:1 in my opinion, a willing and financially committed
owner, justify in most cases, proceeding with allergy
1. Ruling out of other skin conditions with clinical signs testing and ASIT. Although IDT is considered the
that can resemble, or overlap with canine AD. preferred diagnostic method among dermatologists,
2. Detailed interpretation of the historical and clinical ASIS has several advantages over IDT, such as: minimal
features of the condition. The application of clinical patient risk (no sedation required), less traumatic (no
criteria known as “Favrot’s criteria.” repeated skin injections required), more convenient (no
hair clipping needed, less time-consuming), and lower
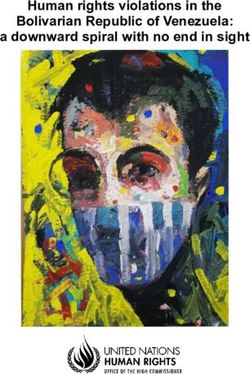
3. Assessment of skin reactivity by IntraDermal Testing risk of drugs interfering with test results (ie. concurrent
(IDT) (figure 1) or detection of IgE by Allergen- anti-inflammatory/antipruritic therapy). However, ASIS
Specific IgE Serology (ASIS) testing. only measures circulating allergen-specific IgE, does
Figure 1. Canine Intradermal Test not take into account other allergic pathways and often
shows positive reactions in non-allergic dogs.
IDT and ASIS are still lacking standardization and it is
suspected that false positive and false negative results
do occur. It is estimated that between 10 and 30% of
dogs with a clinically confirmed canine AD may show
a negative IDT.1 This high percentage of false negative
results can be due to several factors including improper
technique, too low test concentration of allergens, drug
interference, intrinsic host factors, incorrect selection
of allergens, IDT performed too long after (>60 days)
or during the peak allergy season, and presence of a
Use of any one of these approaches in isolatizon can condition called atopic-like dermatitis.1 Canine atopic-
result in misdiagnosis, so it is important not to rely like disease is clinically identical to canine AD, but IgE
on any of them as a sole diagnostic principle.1 ICADA response to environmental or other allergens cannot be
concluded that the diagnosis of canine AD is based on documented. Both testing methods are very different
meeting clinical criteria and ruling out other possible and not standardized, which inevitably results in
causes with similar clinical signs. Flea combing, skin poor correlation between both tests. Currently many
scraping and cytology should be performed, where companies are offering allergen-specific serology
necessary, as part of a thorough work-up (figure 2). testing, but a study showed test results do not agree
well between laboratories.1 Nonetheless the success
14
HGS_2021_Proceedings Book.indb 14 17/04/21 12:21 PMYou can also read