KOGI STATE FAMILY PLANNING COSTED IMPLEMENTATION PLAN - (2019 - 2021) Kogi State Ministry of Health, Nigeria - USAID
←
→
Page content transcription
If your browser does not render page correctly, please read the page content below

KOGI STATE FAMILY PLANNING
COSTED IMPLEMENTATION PLAN
(2019 - 2021)
Kogi State Ministry of Health, Nigeria
July 2018
Suggested citation: Kogi State Ministry of Health. 2018. Kogi State Family Planning Costed
Implementation Plan, 2019–2021.
Contact:
Kogi State Ministry of Health
PMB 1068
Olu-oworo Street
Lokoja, Nigeria
2
LIST OF CONTRIBUTORS
1. Dr. Ayo Olayemi SMOH
2. Dr. Francis Akpa SMOH
3. Abiodun Florence SMOH
4. Aledare Adekunle SMOH
5. Adaji Sunday SMOH
6. Mebanidu Ayo C. SMOH
7. Yunusa Momoh SMOH
8. Ajakaye Sabdat SMOH
9. Idoko Blessing SMOH
10. Braimoh Sule SMOH
11. Otitolaye Clement SMOH
12. Acheku Yusuf SMOH
13. Aturu Christaina M SMOH
14. Shaibu I. Adams SMOH
15. Ogundusi B. O SMOH
16. Comfort Agada Family Planning Advocacy Working Group (FPAWG)
17. Sanni Abubakar FPAWG
18. Mofi M. Usman FPAWG
19. Abaniwo C. Nathaniel FPAWG
20. Grace Ben Kato FPAWG
21. Henry Hellen FPAWG
22. Atabo Sarah Zonal Hospital ANKPA
23. Olorunyomi Modupe B. Hospital Management Board HQTRS
24. Wale Adeleye Balanced Advocacy BALSDA
25. Habeeb Salami Consultant
26. Oyewumi V. Ojo MB&P
27. Oni T.F MOF
28. Falusi A.T MWASD
29. Dr. Adetiloye Oniyire Jhpiego/MCSP
30. Dr. Chibugo Okoli Jhpiego/MCSP
31. Hannatu Abdullahi Jhpiego/MCSP
32. Dr. Gabriel Alobo Jhpiego/MCSP
33. Elizabeth Alalade Jhpiego/MCSP
34. Emmanuel Alabi Jhpiego/MCSP
35. Boladale Akin-Kolapo Jhpiego/MCSP
36. Susan Paul Jhpiego/MCSP
37. Alabi Grace Marie Stopes NIG
38. Iborida Jethro KSPHCDA
39. Odaudu Deborah KSPHCDA
3
TABLE OF CONTENTS
FOREWORD................................................................................................................................................................... 5
PREFACE......................................................................................................................................................................... 6
ACKNOWLEDGEMENTS........................................................................................................................................... 7
ACRONYMS.................................................................................................................................................................... 8
1. SECTION 1: INTRODUCTION
1.1. The Nigerian Context....................................................................................................................... 10
1.2. Kogi State Context....................................................................................................................... 11
1.3. Kogi State Family Planning Landscape................................................................................. 12
1.3.1. Service Delivery.................................................................................................. 13
1.3.2. Supplies and Commodities................................................................................ 15
1.3.3. Demand Generation............................................................................................ 16
1.3.4. Regulation and Policy........................................................................................ 17
1.3.5. Financing............................................................................................................... 17
1.3.6. Supervision, Monitoring and Coordination.................................................. 17
2. SECTION 2: INTEGRATED FAMILY PLANNING PLAN
2.1. Goal.............................................................................................................................................................. 20
2.2. Strategic Priorities............................................................................................................................... 20
2.3. Structure of the CIP.............................................................................................................................. 20
2.3.1. Demand Generation and Behaviour Change Communication................. 21
2.3.2. Service Delivery........................................................................................................... 22
2.3.3. Supplies and Commodities...................................................................................... 23
2.3.4. Policy & Regulation.................................................................................................... 24
2.3.5. Financing........................................................................................................................ 25
2.3.6. Supervision, Monitoring and Coordination..................................................... 26
3. SECTION 3: COSTING
3.1. Assumptions............................................................................................................................................ 28
3.2. Cost Summary......................................................................................................................................... 28
4. SECTION 4: PROJECTED METHOD MIX................................................................................................. 29
5. SECTION 5: THE PATH FORWARD
5.1. Resource Mobilization....................................................................................................................... 30
5.2. Ensuring Progress through Performance Management...................................................... 30
Annex A: Monitoring and Evaluation Summary Table................................................................................ 30
Annex B: Activity Matrix with Detailed Costing.......................................................................................... 34
References...................................................................................................................................................................... 45
4FOREWORD
The Government of Kogi State, in her plan to improve the State FP indicators and contribute to the
National commitment at the 2012 London Summit on Family Planning domesticated the Nigeria Family
Planning Blueprint (scale-up plan)
Kogi State has a contraceptive prevalence rate currently estimated at 11% percent for all married women
(NDHS 2013). However, only 8.5 percent of contraceptive users who are married women are using a
modern method (NDHS 2013). It is expected that the full implementation of the CIP would will take the
mCPR from its current 8.5% (NDHS 2013) to 20% by 2021 with a clear objective to provide a broad choice
of FP methods to users in order to meet their preferences and needs.
In view of the apparent challenges facing the State, 20% mCPR looks ambitious but achievable through
commitment and clear focus on 6 key strategic priority areas that includes: FP Demand Generation and
Behavior Change Communication, Staff and training, Partnership with Private sector in service delivery,
FP policy and financing, Monitoring and Coordination.
Therefore, I am confident that this CIP, if implemented, will meet the State’s ambition of attaining mCPR
of 20% by 2021 through increased availability and accessibility of FP information and services in the
State.
I wish to congratulate the State Ministry of Health, Health Regulatory Bodies, Professional Health
Associations, FP Implementing Partners, Civil Society Organizations and the Private Sector working in
Kogi State for their contributions towards the development of this very important document.
Dr. Saka Haruna Audu
Honourable Commissioner for Health
Kogi State
5PREFACE
The domestication of the National FP Blue Print led to the development of this three-year (2019-2021)
Family Planning (FP) costed implementation plan (CIP) for Kogi State. This is yet another significant
achievement being made by the State Government towards availability and access to high quality FP
services in the State.
The unmet need for Family Planning in Kogi State is estimated at 21% while the total fertility rate is 4.2%,
and 89.5% of women of reproductive age are not using any contraceptive method (NDHS 2013).
Contraceptive use is low among adolescents and young adults, which has resulted in a high prevalence of
pregnancies, unsafe abortions and -related deaths, indicating a need to ensure strong FP access for young
and unmarried women.
In a bid to improve the poor FP indices, Kogi State Ministry of Health, with support from Maternal and
Child Survival Program (MCSP), being implemented by Jhpiego and other partners, and funding from
USAID, developed this FP CIP, which is a detailed roadmap for achieving a 20% mCPR goal by 2021. This
would improve maternal, newborn, adolescent and child Health in the State. This document specifies the
strategies towards achieving the laudable goal including the human, material and financial resources
needed.
It is our hope that this FP CIP will provide a veritable tool for evidence-based advocacy and broad-based
resource mobilization to all collaborating partners and agencies. We also call on the private sector to
invest in the various thematic areas identified in the document.
Pastor Kolawole J.F
Permanent Secretary, Ministry of Health
Kogi State
6ACKNOWLEDGEMENTS
The Kogi State Ministry of Health acknowledges with gratitude, the immense support of all those who
contributed to the development of this FP Costed Implementation Plan (CIP)
Foremost, our special gratitude goes to Maternal and Child Survival Program (MCSP) for financial and
technical support provided in the course of developing this document. This kind gesture is duly
acknowledged and heartily appreciated. We also acknowledge all the Implementing Partners, Civil Society
Organizations, Community Based Organizations (CBOs), Health Training Institutions, Professional
Associations and the Private Sector, who in no little means have contributed to ensuring the production
of this document through their technical support.
Finally, I want to acknowledge His Excellency, Alhaji Yahaya Bello, Executive Governor of Kogi State,
whose visionary leadership has set the pace in the health sector in Kogi State. To my Honourable
Commissioner for Health, I say very big thanks for granting approval and supporting the development of
this document.
Dr. A. Olayemi
Director of Public Health, SMOH
Kogi State
7ACRONYMS
ACOMIN Association of Civil Society On Malaria Immunization And Nutrition
ANC Antenatal care
BCC Behavioral Change Communication
BALSDA Balanced Stewardship Development Association
CHEW Community Health Extension Worker
CIP Costed Implementation Plan
CLMS Contraceptive Logistics Management System
CPR Contraceptive Prevalence Rate
DBC Demand Generation and Behavioral Change Communication
DPRS Department of Planning, Research and Statistics
HMIS Health Management Information System
HMB Hospital Management Board
KSMOH Kogi State Ministry of Health
KSPHCDA Kogi State Primary Health Care Development Agency
FGON Federal Government of Nigeria
FMOH Federal Ministry of Health
FP Family Planning
FPAWG Family Planning Advocacy Working Group
FPTWG Family Planning Technical working group
FP2020 Family Planning 2020
ICPD International Conference on Population and Development
IUD Intra Uterine Device
JCHEW Junior Community Health Extension Worker
LARC Long-Acting Reversible Contraceptive
LGA Local Government Area
LMIS Logistics Management and Information System
LMCU Logistic Management and Coordinating Unit
mCPR Modern Contraceptive Prevalence Rate
M&E Monitoring and Evaluation
MOF Ministry of Finance
MNCH Maternal, Newborn and Child health
MCSP Maternal and Child Survival Program
MSI Marie Stopes International
MWRA Married Women of Reproductive Age
NDHS Nigeria Demographic and Health Survey
NGN Nigerian Naira
PE Policy and Environment
PHC Primary Health Care
PPMV Private Patent Medicine Vendor
RH Reproductive Health
RIRF Requisition, Issue, and Report Form
8SC Supplies and Commodities
SD Service Delivery
SDG Sustainable Development Goals
SMC Supervision, Monitoring and Coordination
TWG Technical Working Group
UNFPA United Nations Population Fund
USAID United States Agency for International Development
WRA Women of Reproductive Age
9SECTION 1: INTRODUCTION
1.1. Nigerian Context
With an annual population growth of 3.2 percent and total fertility rate of 5.5, varying across States and
regions (NDHS, 2013)2, Nigeria stands at a risk of population growth that may dwarf her development
gains. Most projections place Nigeria as the third most populous country behind India and China by 2050.
In Nigeria, there are approximately 35 million women of reproductive age (WRA) 71.5% of whom are
married (MWRA). The NDHS (2013) puts the Contraceptive Prevalence Rate (CPR) among these women
at 15% and the modern CPR at 10%; and since then, relatively little progress has been made2. The goal of
the national CIP is to increase the CPR to 36% by 2018; this target was announced at the London Family
Planning Summit (2012)3. The realization of this goal to ensure 400, 000 infant and 700,000 child deaths
as well as 1.6 million unintended pregnancies averted. This goal was recently reviewed to achieving a
modern Contraceptive Prevalence Rate (mCPR) of 27 percent among all women by 2020.
All 36 States and the Federal Capital Territory (FCT) were expected to align themselves to this goal and
ensure that the required budgetary backing is put in place for adequate funding of FP services at the state
and (the 774) LGA levels.
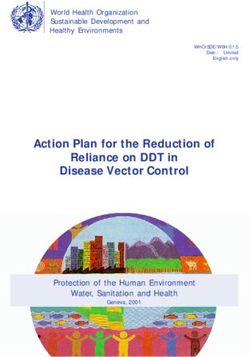
However, only 9.8 percent of these women are using modern FP methods. This national rate has largely
remained at this level since the late 1990s. The modern method mix predominantly (see Figure 1)
comprises condoms, pills and injectables. Over the 23-year period, contraceptive prevalence increased
from 6 percent in 1990 to 15 percent in 2013.
Fig 1: Married women using a contraceptive method, percent CPR
(Source: Nigeria Method Mix 1990–2013 2 )
101.2. Kogi State Context
Kogi is a state in the North-Central zone of Nigeria. It is popularly called the ‘confluence state’ because the
confluence of Rivers Niger and Benue occur there. The State was created on the 27th August 1991 from
the Eastern part of Kwara state and the Western part of Benue State. Its capital is Lokoja. There are three
major ethnic groups in Kogi, viz: Igala, Ebira, and Okun with other minorities like Bassa, Nge, Bassa Komo,
Nupe, Gbagi, Kakanda, Oworo, Ogori and Eggan.
Kogi State is the most centrally located of all the states of the federation. It shares common boundaries
with 10 states namely Niger, Kwara, Nassarawa, and the Federal Capital Territory (to the north); Benue,
Enugu and Anambra (to the east); and Ondo, Ekiti and Edo (to the west).
The state is made up of 21 Local Government Areas (LGAs) as shown in Figure 2 and 239 wards with a
population figure of 3,314,043 from the 2006 population census. There are 50.5% male and 49.5% female
(Figures 3 and 4). As at 2007, it has a GDP per capita of $1,386 (C-GIDD) and is located on the West Africa
Time (WAT) time zone, which is equivalent to Coordinated Universal Time (UTC) plus 1 hour.
Figure 2: Map of Kogi State showing the 21 LGAs
Fig 3: Kogi State population by gender (Census 2006) Fig 4: Kogi State population by age groups (Census 2006)
91,833
49.50% 1,507,045
50.50%
Male 1,715,165
0-14 YRS
Female
15-63 YRS
65+ Years
111.3. Kogi State Family Planning Landscape
The family planning situation analysis painstakingly addresses important scopes of family planning
across public and private sectors. Accordingly, six critical components were looked into:
Service access and delivery
Supplies and commodities
Demand generation
Regulation and policy
Financing
Supervision, Monitoring, and Coordination
Fig 5: North Central Total Fertility Rate
7
6.1
6
5.4 5.4
5.2 5.1
5 4.5
4.2
4
3
2
1
0
FCT BENUE NIGER NASARAWA PLATEAU KWARA KOGI
Kogi State has a contraceptive prevalence rate currently estimated at 11% percent for all married women
in the state. However, only 8.5 percent of contraceptive users who are married women are using a modern
method. Married women using modern methods primarily rely on short-acting methods such as pills,
condoms, and injectables. Unmet needs for FP in the state is estimated at 21% while the total fertility rate
is 4.2. 89.5% of the women of reproductive age are not using any contraceptive method. Contraceptive
use is low among adolescents and young adults, which has resulted in a high prevalence of undesired
pregnancies, unsafe abortions and hence high abortion-related deaths, indicating a need to ensure strong
FP access for young, unmarried women.
12Fig 6: % of currently married women age 15-49 using any method of contraception
Source: NDHS 2013
45%
40%
35%
30%
25%
20%
15%
10%
5%
0%
FCT BENUE PLATEAU KOGI KWARA NIGER NASARAWA
Fig 7: Unmet needs for family planning by states in the North Central zone of Nigeria
Source: NDHS 2013
35%
30%
25%
20%
15%
10%
5%
0%
FCT NIGER PLATEAU NASARAWA BENUE KOGI KWARA
1.3.1 Service Delivery
Modern contraception is provided mainly at the public health facilities in the state. According to the
KSMOH Family Planning unit, the state has 1,073 facilities both primary and secondary with 247 facilities
offering at least a modern family planning method and counseling. Long term methods such as implants,
intrauterine devices (IUDs) are readily more accessible from public health facilities but the services are
under-utilized. Data on the distribution of contraceptive services from the private sector was unknown
as at the time of the situation analysis.
13Fig 8: Kogi State family planning uptake 2015-2017
Source: Kogi DHIS2
50000
45000
40000
35000
30000
2015
25000
2016
20000
2017
15000
10000
5000
0
New FP Acceptors Female FP injections IUCD Inserted Implant
Challenges facing service delivery in the state includes staff attrition due to reshuffling; distance of
facilities and the issue of insurgency in the state which has created fear, hence the service providers and
the clients are not willing to go to the facilities in the affected areas.
Table 1: Distribution of Health Personnel working in Kogi State
S/N Category Number
1 Doctors 198
2 Pharmacists 49
3 Nurses/midwives 1460
4 Community Health Officers (CHO & CHEW) 1262
6 Medical Laboratory Scientists 75
7 Physiotherapists 9
8 Radiographers 2
9 Pharmacy technicians 23
10 Laboratory technicians 47
11 Dental technologists 1
12 Dental technicians 10
13 Dental therapists 6
14 Health Records Officers 16
15 Health Record Technicians 55
16 Health Record Assistants 24
17 Pharmacy Assistants 147
18 Laboratory Assistants 66
19 Environmental Health Officers1 1200
Source: Kogi State SHDP
14The staff screening embarked upon by the state is yet to be completed while there has been an
employment exercise in the state in the last three months. Due to these, the actual number of health
workforce cannot be ascertained but the most recent information on numbers and density of health
workers available in the state is presented in Table 1.
The Task Shifting and Task Sharing Policy which allows CHEWs to provide LARCs to increase access to FP
for women in hard-to-reach areas is already domesticated by the state.
Staff skills and training: One of the triggers of the poor FP indices in the state is inadequate trained FP
providers, particularly for injectables and long-acting reversible contraceptives (LARCs). This may allow
providers bias to recommending certain methods (pills and injectables) over LARCs and this will limit
clients’ rights to free and informed choice. Even though, in an effort to increase modern FP methods,
Saving One Million Lives trained 90 health care workers including CHEWs in November 2017, the number
is grossly inadequate considering the population of the state. Apart from the Saving One Million Lives
program, MCSP and Marie Stopes,.
1.3.2 Supplies and Commodities
The Federal Government of Nigeria introduced the Free Contraceptive Policy in the public health sector
in April 2011 to eliminate the hitherto cost recovery arrangement that was used to finance delivery of
contraceptives from Central Contraceptives Warehouse in Lagos to the Service Delivery Points (SDPs),
otherwise known as Last Mile Distribution. With this, the Federal Government took up the responsibility
of procuring and supplying free family planning contraceptives to all states to facilitate constant
availability of contraceptives and prevent disruption of family planning services at all Service Delivery
Points (SDPs) nationwide.
Procurement of FP commodities is centrally carried out by the Federal Ministry of Health through the
United Nations Population Fund (UNFPA). The procurement is done with the funds contributed by the
Federal Government of Nigeria and development partners, including USAID, the UK Department for
International Development (DFID), and the Canadian International Development Agency (CIDA). This
indicates that Kogi State does not procure family planning commodities. The Ministry of Health has the
responsibility for family planning commodity management in the state which includes storing and
distribution to all service delivery points. The state receives supplies every 4 months and distributes to
the LGAs, while the LGA FP coordinators distribute bimonthly to the service delivery points.
The health facilities receive contraceptives in accordance with the consumption rate recorded quarterly
to avoid over stock. Commodity forecasting is done by both the State RH/Family Planning Coordinator
and LGA FP Program Officers using data from the various Service Delivery Points in the public health
sector only. These data include information on daily and monthly consumption pattern in absolute
number and methods. Specifically, at the SDP level, the Daily Consumption record, FP register, and
monthly summary are used for tracking and quantifying commodities while LGA RIRF forms and tally
cards and state RIRF are being used at the LGA and State levels respectively. Sometimes, the main
challenge to this exercise is either late submission of data or poor quality of data from SDPs. The state
witnessed stock out for 3 months in the year 2017 but such challenges have been addressed.
15One other key challenge to access of FP commodities in the State as identified in the course of the
development of this document was non-availability of consumables. There are unconfirmed reports that
clients are being charged out-of-pocket expenses to purchase consumables when the Federal Government
has a policy of free FP services at the public facilities. This challenge needs to be addressed to avoid it
being a major impediment for FP acceptors in the State. Also, funds are usually not available for last mile
distribution of the commodities to the health facilities. It is important for the state and LGAs to evolve a
cost effective and more sustainable contraceptives logistics management system to ensure regular
availability at SDPs.
1.3.3 Demand Generation and Behavior Change Communication
Currently, Kogi State does not have a Demand Generation/BCC Strategy and as such there is no structured
approach to demand creation activities for family planning. Focus Group Discussions and Indepth
interviews with different audience including law makers and senior public officials in Education, Women
Affairs, Finance Budget and Planning Ministries revealed high awareness of maternal mortality and
induced abortion among women and girls. However, most of the respondents could not give specific
statistics. In the same vein, teachers, students, women and men acknowledged high sexual activities and
induced abortion among adolescent girls, with all of them agreeing that access to and use of family
planning services among other solutions can significantly reduce incidences of unwanted pregnancy,
induced abortion and maternal mortality
The various focus group discussion sessions held with women, family planning clients (users), men and
young men and women revealed many sources through which they receive family planning information,
and these include health workers, radio and TV, friends and neighbours. Similarly, health workers (family
planning service providers) indicated ante natal and postnatal clinics and community outreach as the
avenue through which FP information is provided to women, girls and mothers generally. In addition,
some of the development partners that supported family planning programs and service delivery in the
state have at different times produced and distributed IEC materials in addition to supporting occasional
community and clinic-based outreach events to mobilise and provide services to women. However, at the
time of the situation analysis, FP messages are hardly aired on radio and TV; this is not unconnected with
the fact that there are few programs working on FP in the state, non-prioritization of FP by the state, and
the religious and cultural issues regarding FP in the state.
Despite high level of awareness of the benefits of family planning among the general population, demand
and uptake is still low and this might be due to misinformation, myths and misconceptions about family
planning. For women wanting to delay their next birth, the most common reason reported for not using
contraception was their inability to convince their spouses to allow them to accept modern FP method
and some mentioned their religion do not support FP. Additionally, some raised concerns about the side
effects of various methods available. It is therefore important for a shift in emphasis from
sensitisation/awareness creation to behaviour change interventions that have the capacity to neutralize
this negative information about family planning, reduce and or eliminate resistance from men and
generate demand for family planning not only among women but couples. The greater appreciation of
benefits of family planning in reducing maternal morbidity and mortality, eliminate risks of abortion that
women are exposed to and improve their quality of life will significantly influence their behaviour and
drive demand for FP services. In designing BCC/DG interventions, cognizance must be taken of media that
are accessible to women especially those living in rural areas.
161.3.4 Regulation and Policy
The Kogi State FP policy environment was sub-optimal. There are still challenges that range from lack of
a State specific FP policy, a state-specific FP strategic/operational plan; though its activities are currently
largely guided by national policies and guidelines that have either been domesticated or adopted. These
policies and guidelines include National Policy on Population for Sustainable Development (Revised
2014), National Policy for the provision of free contraceptives in public sector facilities (April 2011) and
National Policy on Task-Shifting and Task Sharing (2014). Others are The National LARC Strategy, the
Reproductive Health Commodity Strategy, the National Strategic Health Development Plan, the Maternal,
Newborn, and Child Health Strategy, National Reproductive Health Policy, Nigeria Family Planning
Blueprint (Scale-Up Plan 2014), National FP/RH Service Protocol, and National Guidelines on
Contraceptive Logistics Management System.
The State recently domesticated the Task Shifting Policy, which allows some modern FP tasks to be shifted
to CHEWs, and recently validated its State Strategic Plan 2017-2021. Translating these policies to
workable document that will be well funded in order to achieve an impactful and verifiable result requires
strong political interest and determination from the Government. Inadequate appropriation and non-
release of funds for family planning programs to over-dependence on few development partners in the
State are some of the challenges to achieving the full potentials of these policies and strategies for family
planning.
It is therefore expected that the State will leverage on these policies/strategies and make visible positive
changes in Maternal Mortality Rate reduction through the promotion of programs and actions that will
improve FP uptake in their States.
1.3.5 Financing
Family planning financing is the responsibility of the three tiers of government with each tier financing
different components. The Federal Government of Nigeria through the Federal Ministry of Health (FMOH)
procures and distributes contraceptives to the states, monitors its management and build capacity of FP
Focal Persons at state and LGA levels. The state on the other hand, ensures that commodities are
distributed to service delivery points through the LGAs, build capacity for service delivery, implement
demand creation activities and supervise and monitor. The LGAs coordinates service delivery at the SDPs,
conduct outreach and procure and supply consumables to SDPs within PHCs.
Although the state has been budgeting 5 Million Naira for FP in the last 4 years, the fund has never been
released. FP is majorly donor driven in the state. Saving One Million Lives trained 90 health care workers
including CHEWs in Nov 2017, Marie Stopes and MCSP have trained some health workers and conducted
several monitoring and evaluation activities but for FP services to be adequately financed, the need for
the government to release funding for FP cannot be over-emphasized.
1.3.6 Supervision, Monitoring and Coordination
The Kogi State Ministry of Health and the Primary Health Care Development Agency (KSPHCDA) have
shared responsibility for family planning program management and coordination. While the Ministry is
responsible for overall coordination, policy, contraceptives supplies and logistics management, training,
supervision and strategic planning, the Agency on the other hand is responsible for overseeing service
delivery at the PHC level, monitoring and supervision of FP services at the PHC level, training and
17mentoring of service providers. In addition, the State Hospital Management Board oversees FP service
delivery at the secondary health care level while the tertiary health institution also plays similar role at
tertiary health care delivery level.
Fig 9: Family Planning Dataflow and Management
National (DHIS2)
Database administration and management
Performance review
Planning and decision making
State
LGA
Data quality assurance
Data quality assurance
Database administration
Data collection & entry
Data dissemination
Data dissemination
Evidence-based Planning &
Planning & improvement
decision making
Performance review
NGO facilities & others
Private clinics Data collection &
collation
Data collection &
Data use for
collation
planning &
Data use for planning &
SDPs (PHC)
decision making
Data collection & collation
Data use for planning &
decision making No FP data
No FP data
transmission
transmission
At the LGA level, there exists the reproductive health and family planning unit in the Primary Health Care
department. While the department is under the leadership of Director of Primary Health Care, the RH/FP
unit is under the leadership of a RH/FP Program Officer whose main responsibility is coordination of FP
programs and service delivery at the LGA level. Though there is no written job description for this office,
however, based on information obtained, roles and responsibilities should include projecting and
forecasting FP commodity requirements, collecting contraceptives from the State, supply of
contraceptives to SDPs, monitor and supervise service delivery, facilitate data transmission to the LGA
M&E unit and provide on the job training, mentor and coach providers. Others include support SDPs to
conduct outreach activities, put system in place for community participation in FP, financial planning
(budget) and management of FP resources, follow up to ensure release of budgeted fund, nominate health
workers for training in FP, document activities, undertake advocacy and facilitate availability of
consumables and managing input of the private health sector into FP.
18Ideally, the FP unit within the KSMOH should lead bimonthly supervisory meetings to assess the status of
FP service delivery in healthcare facilities but the non-availability of funds for this has been a bottleneck.
The study revealed that Saving One Million Lives program recently supports Bi-Monthly review and re-
supply of FP commodities to service delivery points. There is availability of FP Technical Working Group,
but their meetings and activities too have been hampered by lack of funds.
Both the Ministry and PHC Agency have responsibilities for monitoring and supervising the delivery of
family planning services, however, this is limited to facilities in the public health sector. At the LGA level,
the FP Program Officer performs this function focusing on SDPs. Feedback from the Program Officers
indicated that supervision and monitoring has not been a regular activity due to some challenges,
especially lack of fund and logistics support. Monitoring and supervisory visits when conducted were only
limited to facilities that have close proximity to either the State capital or Local Government
Headquarters. The state has established a data flow and management information system for family
planning. The system shows that FP service statistics are transmitted from the SDPs to the LGA and finally
to the national level (DHIS2). Specifically, at the facility level, there is a daily client register where all
clients are registered on daily basis and at the end of the month, it is summarized and transmitted to the
LGA Monitoring and Evaluation Officer who collates and forward to the state.
At the state level, the Monitoring and Evaluation Officer collates submissions from all LGAs and update
the State data base which is linked with the District Health Information System platform. While the state
has achieved 98% compliance in terms of the number of facilities reporting data, a major challenge is
quality of the data transmitted from health facilities and uploaded to the platform. This challenge is due
to high work load on the M&E Officers, inadequate capacity and lack of punitive measures for defaulters
and those that transmit poor quality data. A visit to a secondary facility providing FP services also
revealed that sometimes the daily register may not be available. At the time of the assessment, there was
no information on data reporting rate based on the number of SDPs providing FP services in the state. As
such the performance of SDPs in terms of timely and accurate data submission could not be determined.
Monitoring and coordination of FP activities is poor due to non-release of budgeted funds. In order to
accelerate FP improvement in the State, the ministry of health is expected to establish functional
platforms/forums for effective coordination of FP activities at the various levels and sectors (public,
private, and civil society). Though, only a few partners are working on FP in the State, there is a need for
a functional partner’s forum.
19SECTION 2: INTEGRATED FAMILY PLANNING PLAN
2.1. Goal
The overarching goal of the Kogi CIP is to increase women’s use of FP services (mCPR to increase from
8.5% to 20%) and contribute to the reduction of maternal mortality across the State by 2021.
2.2. Strategic Priorities
Reports of findings from the Kogi State FP Landscape identified key barriers to increasing contraceptive
prevalence in the State. Based on these findings, the CIP Development Task force outlined the following
strategic priorities as a means to highlight the critical activities needed to reach the target of 20% by 2021.
FP Demand Generation and behavioral Change Communication: Strengthening demand for a
full range of contraceptive methods and services by delivering targeted, accurate FP information
and addressing common FP myths and misconceptions.
Staff and training: Strengthening the capacity of healthcare workers to provide safe, high-quality
FP services, including counseling, provision and removal of long-acting reversible contraceptives.
Partnership with Private sector in service delivery: Increase coverage and access to high-
quality integrated FP services and commodities through the private sector, especially faith-based
organizations, private hospitals/clinics, pharmacies and PPMVs as appropriate for some methods.
FP policy and financing: To advocate for standard budget lines and timely release in State and
LGAs budgets to cover FP services, commodities, consumables, and distribution all the way to
the SDPs
Monitoring and Coordination: Increase coordination across the public, private, and civil society
sectors to maximize resources and supervision support to healthcare workers across the State.
2.3. Structure of the Costed Implementation Plan (CIP)
The CIP’s activities are structured around six thematic areas of the health system for family planning:
Demand Generation and behavioral Change Communication
Service Delivery
Supplies and Commodities
Policy and Environment
Financing
Supervision, Monitoring and Coordination
Across the six categories, several activities exist—some of which are further subdivided into sub-
activities, with descriptions for costing purposes. The full details of these activities and the cost of
implementation can be found in Annex B: Activity Matrix and Costing Details.
202.3.1. Demand Generation And Behaviour Change Communication (DBC)
Objective: To ensure 100% of women of reproductive age, men and adolescent have accurate, clear, and
consistent messages on modern family planning methods by 2021.
Strategies Priorities Statement: FP Demand Generation, Communication and Behavior Change:
Addressing the cultural and religious belief, myths and misconceptions of men and women in
communities for full uptake of FP contraceptive methods targeting provision of accurate and consistent
information on family planning modern methods for Behavioral Change
Justification: According to NDHIS and ICF 2013, 60.6% of women have not heard or seen FP messages
on the radio or any other media source, representing a missed opportunity for programming. Therefore,
reaching all of these women, men and adolescents with accurate and consistent FP messages will certainly
improve the uptake of FP services particularly the modern methods in Kogi State.
Strategy: Dialogue, focus group discussion (FGD), compound meetings, house to house mobilization, Men
to Men engagement meetings, interpersonal communications, Head of households, using of folk tales and
drama to project the benefits and importance of FP. Involvement of community volunteers (town
announcers), community outreaches, engagement with TBAs, health educators and community engagers
towards promoting/better family planning uptake within their respective communities. These strategies
when fully engaged will definitely increase uptake of family planning services in the State.
Activities
DBC 1:1 Develop appropriate mass media programs/documentaries on Radio and TV stations to
inform/educate the people, develop articles/ write-ups for publications in the Newspaper and
also engage in Newspaper interviews/ Radio and TV discussions.
DBC 1:2 Development, production and distribution of IEC materials and Advocacy kits to the
grassroots. That is, Religious/Traditional leaders and opinion moulders.
DBC 1:3 Translation/Airing of jingles in 5 languages in Kogi State namely Yoruba, Igala, Ebira,
Nupe and Hausa.
DBC 2:1 Capacity building of Advocacy group members, Health educators - These people will in
turn train Community engagers, Traditional barbers, Community volunteers, CBOs, CSOs and
Health reporters from major media houses in the State on FP services.
DBC 2:2 Train and encourage Local/Traditional musician to promote FP with their music.
DBC 2.3 Facilitate 3-day cascading training to 239 (1 per ward) Community engagers.
DBC 3:1 Advocacy visit to the head of media houses: Director General Kogi State Radio
Broadcasting Corporation, Managing Director, The Graphic Newspapers, General Manager NTA
Lokoja, General Manager Prime FM Lokoja, Manager Grace FM, State Chairman Nigeria Union of
Journalists (NUJ), Education stakeholders, Security agencies and Religious/Traditional leaders to
key into Family Planning (FP).
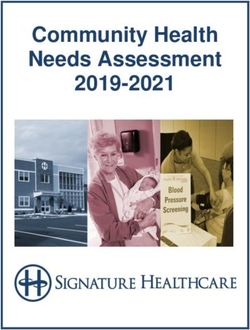
21Fig 8: Demand generation activity cost per year
Demand Generation Activity cost 7,000,000
6,000,000
5,000,000
4,000,000
per year
3,000,000
2,000,000
1,000,000
0
2019 2020 2021
DEMAND GENERATION 6,500,050 3,690,650 990,000
2.3.2. Service Delivery
Objective: Ensure that all health facilities (Public, Private and Faith based) in the State have at least one
skilled family planning service provider.
Priority Statement: Increase the capacity of health care workers to be able to render qualitative and
quantitative family planning services in the State.
Justification: Kogi State has 1073 health care facilities in the State with 247 health facilities offering FP
services. This means only 23% of health facilities in the State render family planning services. On the
other hand, there is staff attrition in the health sector with a lot of health care providers retiring without
replacement.
Strategy: Task shifting to the CHEWs and other health workers is necessary and this can be done by
increasing the capacity of CHEWs and other health workers to offer family planning services.
Activities
SD 1: Capacity Building for skilled Health Workers annually - (Nurses/Midwives and CHEWS.
SD 2: Quarterly Family Planning outreach to reduce unmet needs for Family Planning at the
community level.
SD 3: Purchase of operational vehicle for family planning activities
SD 4: Purchase of equipment (PP IUD Insertion kit, implants removal kits and pelvic model)
22Fig 10: Service delivery activity cost per year
70,000,000
Service Delivery Activity Cost Per
60,000,000
50,000,000
40,000,000
Year
30,000,000
20,000,000
10,000,000
0
2019 2020 2021
SERVICE DELIVERY 64,206,670 10,587,800 10,587,800
2.3.3. Supplies and Commodities
Key Objective: To strengthen the existing logistic management system for contraceptive supplies and
commodities in Kogi State to enhance contraceptive availability in all Health Facilities all year round.
Strategic Priority Statement
Last mile distribution: State Government/partners and other sources to support with funds for
last mile distribution of contraceptive commodities and supplies
Logistics management coordinating unit to develop and monitor last mile distribution to ensure
timeliness of commodities delivery.
Justification: Continuous availability of contraceptive commodities is key to promoting the uptake of
family planning in Kogi State. Stock out of contraceptive commodities in Health Facilities may discourage
family planning users from continuing family planning and intending family planning users from
commencing family planning. Hence, there is a need to strengthen the logistic management system.
Strategies: The strategy to ensure continuous availability of contraceptive commodities in all Health
Facilities is for the State Government to provide fund for:
Logistics management system of contraceptive commodities procured by the FMOH
Bimonthly data review, re-validation and resupply meeting of the State and LGA logistic
management coordinating which will help to generate requisition list to FMOH for replenishment
of commodities
Activities
SC 1: Strengthen the State logistics management system for FP commodity to make timely delivery of FP
commodities and last mile distribution easier.
Conduct bimonthly review and resupply meeting with LGA coordinators/SDPs.
23SC 2: Improve the quality of FP logistics data needed to make informed decision to ensure continuous
availability of FP commodities in all Health Facilities rendering Family planning services.
Re-training of Health workers and LGA team on FP logistics data tools.
Conduct bimonthly logistic FP data collection and collation meeting with LGA coordinator and
State technical officer.
Empower the State LMCU for data entry into the Navision tool.
Fig 10: Supplies and commodities activity cost per year
30,000,000
Supplies and Commodities Activity
25,000,000
20,000,000
Cost per Year
15,000,000
10,000,000
5,000,000
0
2019 2020 2021
Supplies &Commodities 25,048,200 25,048,200 19,720,800
2.3.4. Policy and Regulations
Objectives:
1. To ensure domestications of national policies before Dec 2021
2. To develop policies that will facilitate the integration of FP services to other MNCAH services.
Strategic Priority Statement: National Policies and regulations will be domesticated for use at the State
and Local Government Levels; Integration of FP services to other MNCAH services
Justification: In the light of improved knowledge in all aspects of Family planning, the State needs to use
evidence-based practice in all area of FP services.
The need to increase coverage of mCPR from 8.5% to 20% requires the integration of FP services in high
volume activities to extend reach to women of reproductive age.
Strategy:
1. Review, domesticate and disseminate existing National policies for the consumption of State and
LGA actors.
2. Integration of FP services into other MNCAH services.
Activities
PR 1.1 Review of existing National Family planning policies and regulations at all levels
PR 1.2: Dissemination of Policies and regulations to all stakeholders
24PR 1.3: Annual Review of Costed Implementation Plan
PR 1.4: End of CIP implementation review and preparation for next CIP
PR 1.5: End line Assessment
PR 2.1 Stakeholders meeting to develop strategy on Integration of family planning services into
other service delivery areas so as to increase FP uptake
PR 2.2 Quarterly FP TWG meetings
PR 2.3 Step down training to OICs in the 239 wards in Kogi State
PR 2.4 Quality Improvements /Integrated Supportive Supervision to the 21 LGAs in Kogi State
Fig 11: Policy and regulations activity cost per year
16,000,000
Policy and Regulations Activity Cost Per
14,000,000
12,000,000
10,000,000
Year
8,000,000
6,000,000
4,000,000
2,000,000
0
2019 2020 2021
Policy &Regulations 13,363,900 2,482,000 4,852,250
2.3.5. Financing
Objective: To get 100% budgetary provisions released for Family Planning Program through the budget
and planning/ ministry of Finance for effective implementation on yearly basis.
Strategic priorities Statement: State government directs all 21 local government areas through the
ministry of local government and chieftaincy to support and fund consumables at the local government
levels.
Justification: By 2021 adequate funding for capacity building, outreach to hard-to-reach areas, data
capturing, and mobility will increase facilities providing FP services from 247 presently to 847.
Strategy: Work with FPAWG to conduct advocacy visits to the Governor and follow up with the Hon
Commissioners for Health, budget and planning, Local Government and Chieftaincy Affairs, and
Finance to ensure timely release of fund for Family planning.
Mobilize resources from partners and private sector organizations.
Activities: Improve funding for family planning
25F1.1: Organize FP advocacy visit to Hon Commissioners for Health, budget and planning, Local
Government and Chieftaincy Affairs, to increase support and funding at the State and Local
government levels
F1.2: Advocate to Private business and enterprises for establishment of Public Private
Partnership (PPP) and charity organizations in support of family planning
F1.3: Build parliamentarian champions among the lawmaker who will support FP during budget
defense.
Fig 12: Financing Activity Cost Per Year
90,000
80,000
Financing Activity Cost Per Year
70,000
60,000
50,000
40,000
30,000
20,000
10,000
0
2019 2020 2021
FINANCING 85,050 85,050 85,050
2.3.6. Monitoring and Evaluation
Objective: Ensure periodic family planning data management through timely collection, collation,
analysis, reporting and usage at all levels of Healthcare service delivery in Kogi State by 2021
Strategic Statement: Develop M&E framework that will be responsible for Monitoring and Evaluation of
family planning services provision and data management
Justification: Routine data collection, collation, analysis, reporting and usage at all levels of Healthcare
service delivery is key. Tracking of Family Planning services to ensure its implementation is also critical.
Consequently, there is a need to strengthen M&E / HMIS activities at all levels.
Strategy
To develop an integrated M&E framework across the six thematic areas.
Tracking of routine data on FP services for collection, collation, analysis and report as feedback
to data users in the State.
26Activities:
SMC1: Printing of Family Planning monitoring tools: The Kogi State Ministry of Health shall print
the following tools for monitoring and supervision of FP activities in the State: Family Planning
Daily register, FP client cards, Review and resupply forms and FP scorecards.
SMC2: Bi-monthly Review/Resupply and Validation of FP data at the LGA level. (FP coordinators,
LMCU and M&E/HMIS): The State shall conduct Bi-monthly meeting of review/ resupply of
commodities and Validation of FP data at LGA level
SMC4: Quarterly coordination meeting of partners supporting FP and TWG: The State shall hold
quarterly coordination meeting of partners and Technical Working Group (TWG) and FP
Advocacy working group (FPAWG) at State level.
Fig 13: Monitoring & Evaluation Activity Cost Per Year
6,000,000
5,000,000
M & E Activity Cost Per Year
4,000,000
3,000,000
2,000,000
1,000,000
0
2019 2020 2021
M&E 5,262,650 5,262,650 5,262,650
27SECTION 3: COSTING
3.1. Assumptions
The approach used for the costing of this CIP builds upon similar costing processes adopted for the
National FP Blueprint and other state CIPs. The costs of each activity are based on the prevailing Kogi. In
addition, each activity’s costing inputs for both unit costs and quantities can be changed (e.g., the specific
input costs for producing a radio program, the number of programs to be produced, the cost of
broadcasting the program, the number of times it will be broadcast, and so on) if there is a need to revise
any elements in the future.
The projected method mix for 2021 was calculated using the 2013 NDHS estimated % use for each method
as a base. Unless otherwise noted, all unit costs (e.g., salaries, per diem rates, meeting rates, and so on)
are based on current costs as of July 2018.
Fig 14: Comparison of Cost per Thematic Areas per year
70,000,000
60,000,000
50,000,000
Cost in Millions
40,000,000
30,000,000
20,000,000
10,000,000
0
2019 2020 2021
Demand Generation 6,500,050 3,690,650 990,000
Service Delivery 64,206,670 10,587,800.00 10,587,800
Supplies &Commodities 25,048,200 25,048,200 19,720,800
Policy &Regulations 13,363,900 2,482,000 4,852,250
Financing 85,050 85,050 85,050
M &E 5,262,650 5,262,650 5,262,650
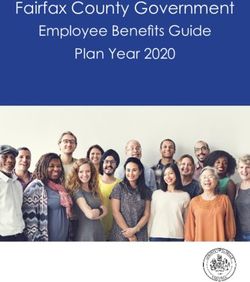
28SECTION 4: PROJECTED METHOD MIX
The CIP goal is that full implementation of the CIP activities will take the mCPR from its current 8.5%
(NDHS 2013) to 20% by 2021. The objective of the CIP is to provide a broad choice of FP methods to users
to meet their preferences and needs.
For purposes of costing and planning, a method mix projection was developed. Thus, these figures are
meant to be directional, not stand-alone targets. The 2021 method mix was estimated based on two core
assumptions:
Use of LARCs (i.e., IUDs and implants) will grow faster than in previous years due to increases in
trained healthcare providers and improved facilities.
Use of injectables will also grow faster than in previous years due to a policy change allowing
CHEWs to administer injections, and from experience indicating that injectables are typically a
preferred method.
Figure 15: Projected Method Mix Chart
100%
90%
80% LAM
70%
Male Condom
60%
Implants
50%
Injectables
40%
IUD
30%
Female Sterilization
20%
Pills
10%
0%
2019 2020 2021
29SECTION 5: THE PATH FORWARD
5.1. Resource Mobilization
Effective implementation of the CIP is key to improving the uptake of family planning in Kogi State. There
is a wide gap between the proposed cost and available resources, hence the need to explore other methods
in sourcing for fund using the CIP document as advocacy tool, while the budgeted and approved fund for
FP should be used for priority identified activities.
Complementing this, the Local Government, Partners and private sector organizations in the State should
be engaged to support FP so as to achieve CIP target. The Legislators will be engaged to stand for FP
budget when it is submitted for debate; SMOF will ensure those budgets approved are released on time
to SMOH for effective implementation of the CIP.
The State Ministry of Health with the support of the FPAWG will also do a mapping of possible areas of
funding for the CIP and come up with a resource mobilization strategy.
5.2. Ensuring Progress through Performance Management
The rationale for developing this plan is to fast-track impact and progress towards increasing the State
mCPR from 8.5% to 20% by 2021. This can only happen if the plans are promptly and effectively
translated into real programming and activity. The Kogi State CIP is an important instrument to set new
direction and measure progress towards accomplishing concrete milestones, outcomes, and impacts in
the State. Consequently, the acceptance of the performance management plan (Annex A) is recommended
for all stakeholders as a guiding tool towards progress.
This framework serves as an instrument that allows the State to track performance against stated goals.
It also allows national-level dashboard to aggregate the gains in country. Policymakers, advocacy experts,
donors, and ministry officials will have adequate template to document best practices. Furthermore,
progress can be communicated to the global level to facilitate learning and build advocacy and support.
The framework calls upon bi-monthly, quarterly or annual reporting of key indicators to measure output
or impact. The data source noted serves as a marker for the responsible data collection system. As a part
of the supervision, monitoring and coordination strategy in the CIP, KSMOH will lead coordination of this
data collection and request feedback, where necessary, from implementing partners.
30ANNEX A: MONITORING AND EVALUATION SUMMARY TABLE
# INDICATOR NO. INDICATORS INDICATOR TYPE DATA SOURCE LEVEL OF FREQUENCY
REPORTING
Impact NDHS/NARHS National/State ,
1. DEMAND GENERATION AND BEHAVIOUR CHANGE COMMUNICATION
1. DBC.1.1. No of Media documentaries produced and aired Output Program report State Weekly, quarterly
2. DBC1.2 Number of IEC advocacy tools and kits developed Output Program report State Annually
3. DBC 1.3 Number of Local languages/messages and FP logo developed Output Program report State Annually
4. DBC 2.1 No of Local/Traditional musician trained and encouraged to publicize Output Program report States Annually
information about FP
5. DBC 2.2 Local/Traditional musician Output Program report States Annually
6. DBC 2.3 No of Training of Trainers (TOT) Conducted Output Program report States Annually
7. DBC 3.1 No of Advocacy visits conducted Output Program report State Quarterly
2. SERVICE DELIVERY
1. SD1.1.1 Number of Nurses/Midwives trained. Output Program report State Annually
2. SD1.1.2 Number of CHEWs trained Output Program report State Annually
3 SD1.1.3 No of TWG trained on supportive supervision Output Program report State Annually
4. SD1.1.4 Number of post training follow up and supportive supervision conducted Output Program report State Quarterly
5. SD.2.1. Number of quarterly family planning outreaches conducted Output Program report State Quarterly
6. SD 2.2 Receipt of Vehicle purchased, picture, registration documents Output Program report State Annually
7. SD 2.3 Receipt of equipment purchased Output Program report State Annually
3. SUPPLIES AND COMMODITIES
1 1.1 No of bimonthly review and resupply meetings with LGA Output Program report State Quarterly
coordinators/SDPs conducted
312. 2.1. Number of trainings on logistics data management conducted Output Program report State Annually
3. 2.2. Number of reports of bimonthly collection and collation review meeting Output Program report State/National Bimonthly
conducted.
4. 2.3. Number of 3rd Party Logistics monitored for effective Last Mile Deliveries Output Program report State/National Bimonthly
4. POLICY AND REGULATION
1 PR.1.1 Copies of national policy and regulations reviewed Output Program report State Annually
2 PR.1.2 Report of dissemination of policies and regulations to all stakeholders Output Program report State Annually
3 PR 1.3 Annual review reports Output Program report State Annually
4 PR.1.4 Report of Implementation review Output Program report State Annually
5 PR.1.5 Report of Endline Assessment Output Evaluation report State Annually
6 PR 2.1 Quarterly FP TWG meeting Output Program report State Annually
7 PR 2.2 Meeting held on Strategy developed on integration of FP services in to other Output Program report State Annually
MNCH services
8 PR 2.3 Numbers of Officer in-Charge (OIC)s Trained on FP integration Output Program report State Annually
9 PR 2.4 Numbers of Quality Insurance (QI)/Integrated Supportive Supervision (ISS) Output Program report State Annually
carried out
5. FINANCING
1 F 1: 1 1 Numbers of Advocacy visits conducted Output Program report State Annually
2 F 2. 1 Numbers of Private organizations/Donors committed to fund FP in Kogi Output Program report State Annually
State
3 F 3.1 Numbers of Parliamentarians committed to support FP Output Program report State Annually
32You can also read